


Article Figures & Data
Figures
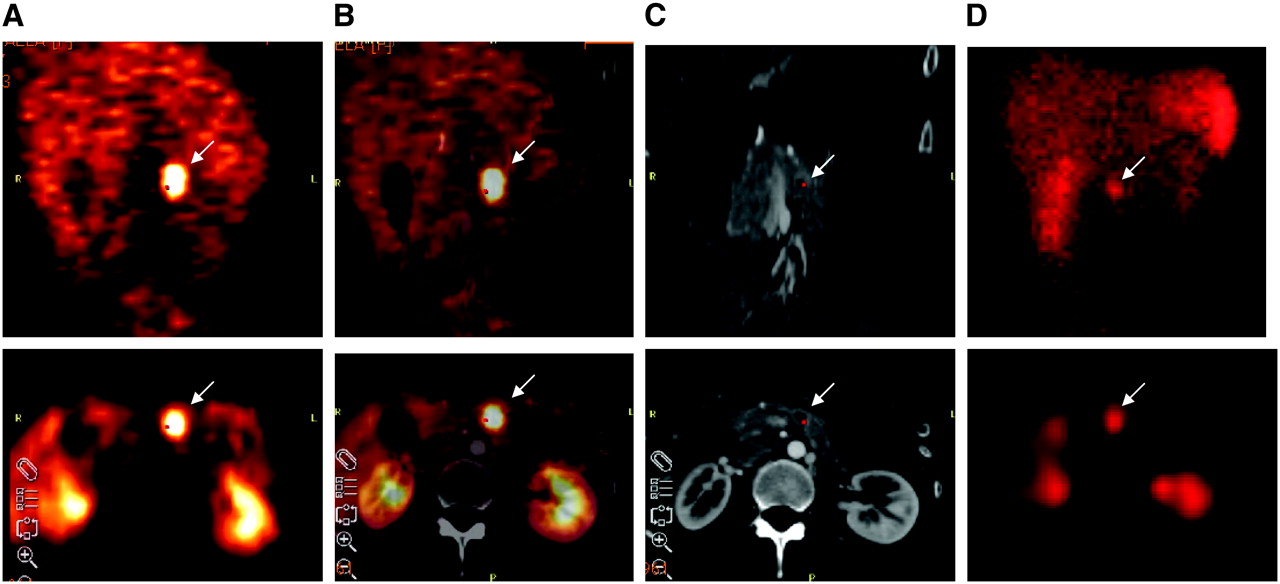
- FIGURE 1.
A 28-y-old female was referred for primary diagnosis of a NET because of elevated tumor markers in serum. PET (A) clearly depicted an abnormal focus in upper abdomen (arrow). This lesion could be delineated in the pancreas after image fusion with CT (B). There was also increased contrast medium enhancement in the margin when using helical CT (C). SPECT with 99mTc-HYNIC-TOC was also positive for this tumor in upper abdomen (D). This positive finding was confirmed by histopathology revealing a NET with 1 cm in diameter. (Top) Coronal views; (bottom) axial views.
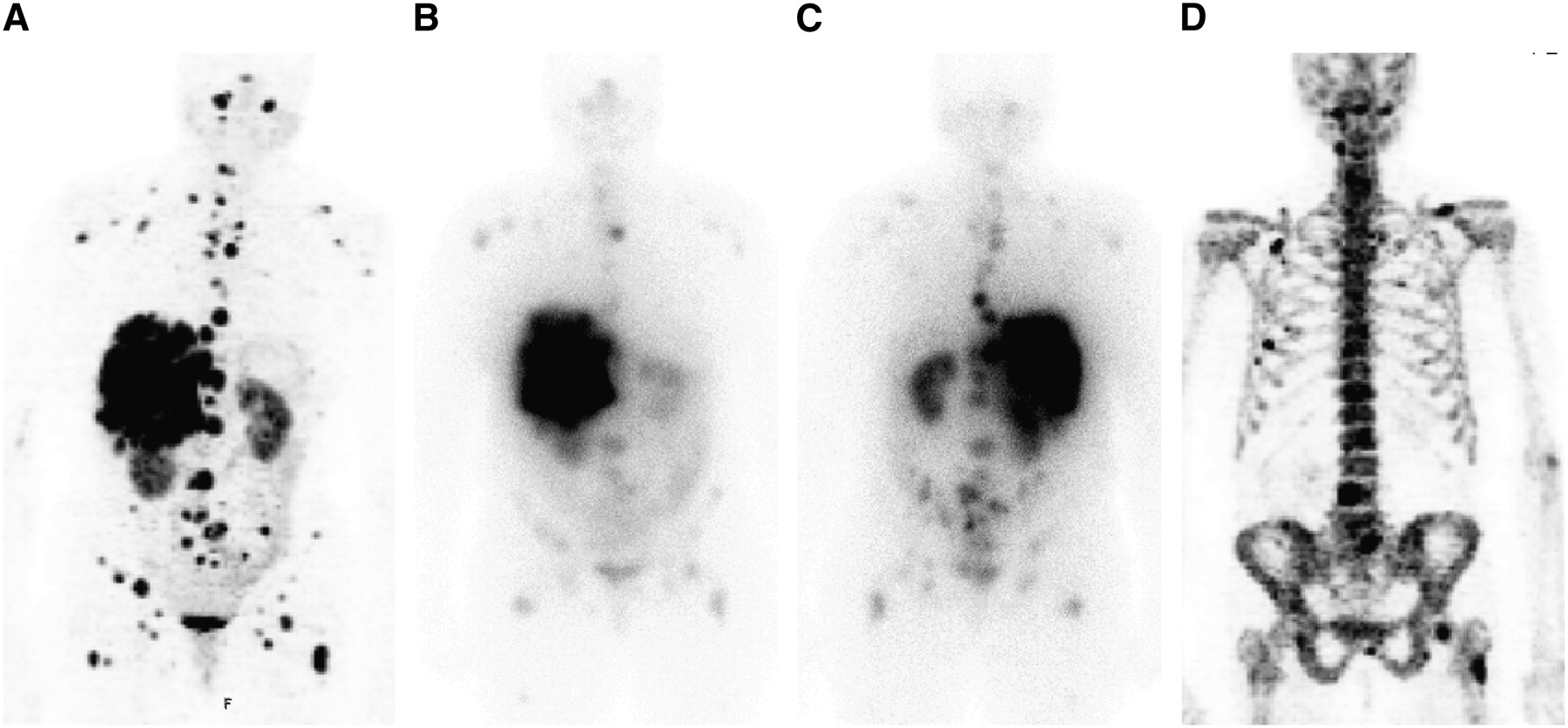
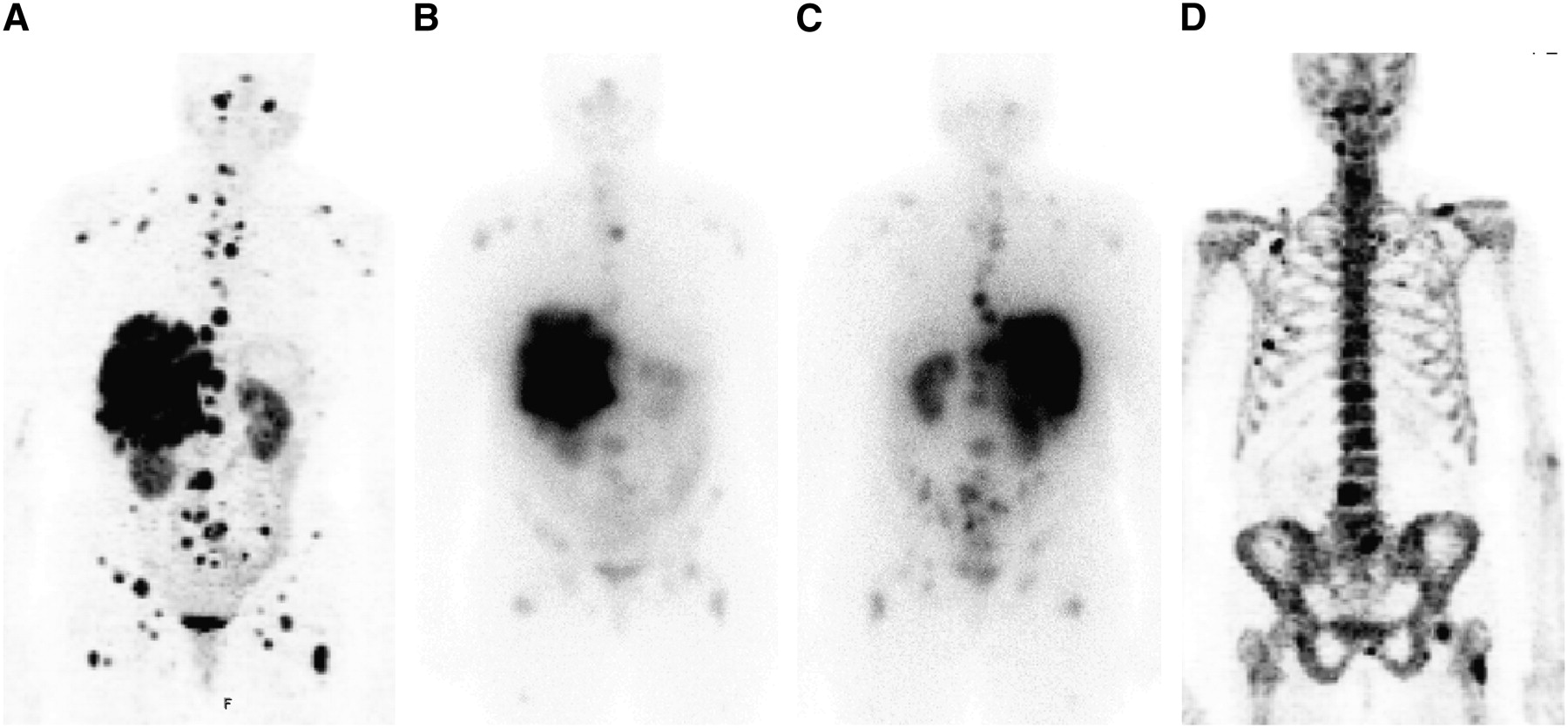
- FIGURE 2.
A 56-y-old woman with multiple liver and lymph node metastases was referred for restaging after surgery and chemotherapy. CT presented these tumor lesions; however, it was negative for bone lesions. Beside the visceral metastases, some additional osteoblastic and osteolytic bone metastases were clearly depicted with 68Ga-DOTA-TOC (A). Only some of these bone metastases were delineated by conventional scintigraphy (B, anterior view; C, posterior view). Osteoblastic bone lesions were confirmed by 18F-Na-fluoride PET (D). Retrospective CT analysis after image fusion revealed some of these bone metastases.
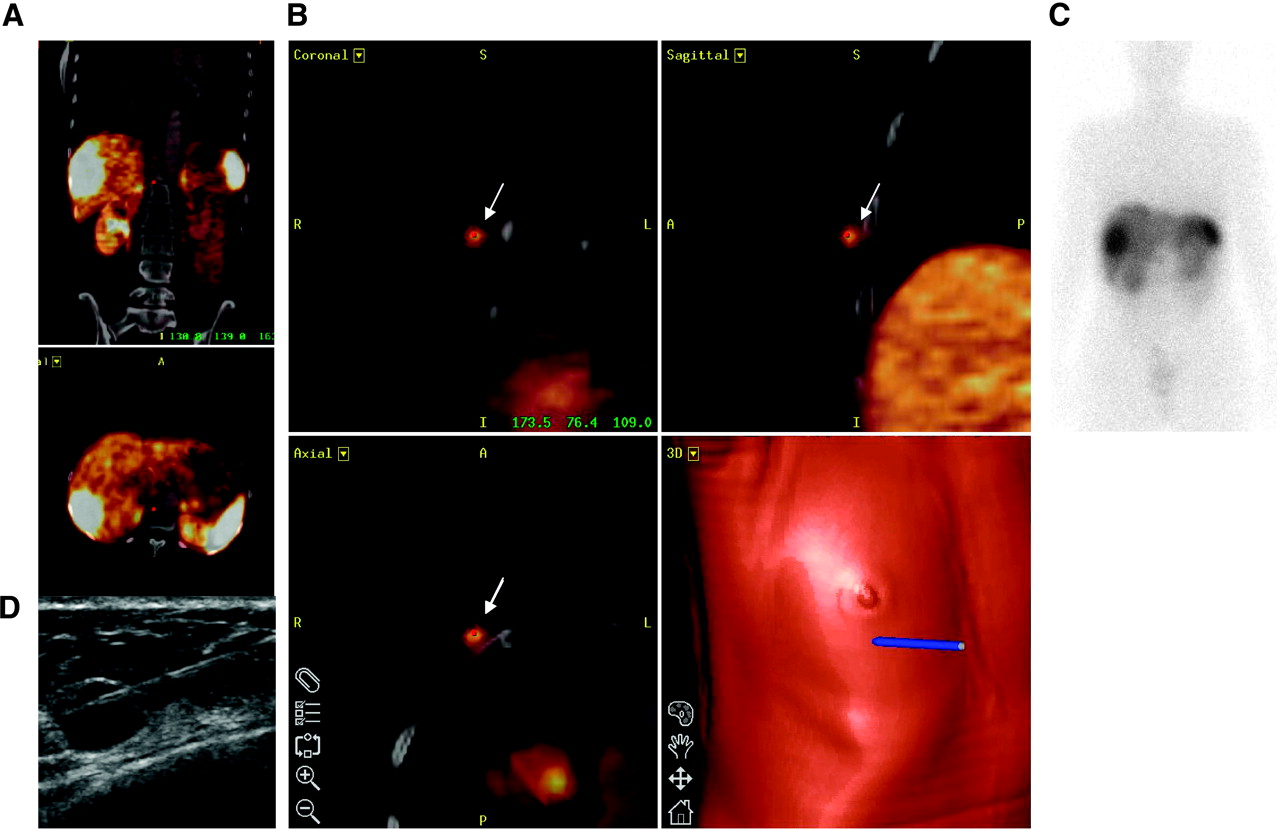
- FIGURE 3.
A 47-y-old female patient was referred for scanning after resection of a carcinoid of the ileum. Multiple liver metastases were known (A). Additionally, 68Ga-DOTA-TOC showed a small lesion in right breast (arrows) (B). This finding was initially not detected with CT or scintigraphy (C). Ultrasound-guided fine-needle biopsy confirmed a metastasis in soft tissue derived from the NET with 7- to 4-mm diameter (D). This tumor lesion and 3 liver metastases were consecutively surgically removed.
- FIGURE 4.
A 62-y-old male patient was investigated after resection of a small bowel carcinoid. 68Ga-DOTA-TOC PET displayed multiple small liver metastases (A). These liver lesions were negative with the other 2 modalities, CT and scintigraphy (B) including SPECT (C). Ultrasonography (D) and further follow-up controls confirmed these lesions. Diameters of metastases were in the range of 1 cm. Positive PET finding initiated treatment with [177Lu-DOTA0,Tyr3,Thr8]octreotide (177Lu-DOTA-TATE).


Tables
Patient no. Sex Age (y) Pathology Indication Clinical symptoms* Confirmation† 1 M 49 Paraganglioma Follow-up No Histology 2 F 57 Carcinoid of pancreas Follow-up No CT 3 F 47 Carcinoid of pancreas Follow-up Diarrhea CT 4 M 59 Carcinoid of pancreas Follow-up No CT 5 M 79 Carcinoid of pancreas Follow-up No CT 6 M 48 Carcinoid of pancreas Follow-up No CT 7 M 61 Broncogenic carcinoid Follow-up No CT, NaF 8 M 59 Small bowel carcinoid (gastrinoma) Staging Gastritis CT 9 M 62 Small bowel carcinoid Staging Flush CT, MRI 10 F 66 Small bowel carcinoid Staging Diarrhea CT 11 M 39 Elevation of CgA and NSE Detection No CT, MRI 12 F 28 Elevation of ACTH Detection Cushing Histology, CT 13 F 62 Carcinoid of pancreas Staging Flush Histology, CT 14 F 75 NET unknown primary Follow-up No CT 15 M 45 Carcinoid of pancreas Staging Diarrhea CT 16 F 50 NET unknown primary Follow-up No CT 17 F 70 Carcinoid of pancreas Follow-up Diarrhea CT 18 F 61 Elevation of CgA and NSE Detection No Histology 19 F 68 NET unknown primary (gastrinoma) Staging Flush CT 20 M 55 Small bowel carcinoid Follow-up No CT, MRI 21 F 40 NET of hypophysis Staging No MRI 22 M 61 NET unknown primary Staging No MRI, NaF 23 M 61 Carcinoid of pancreas Staging No CT 24 F 54 Carcinoid of pancreas Follow-up No CT 25 M 55 Carcinoid of pancreas (gastrinoma) Staging Gastritis CT 26 F 64 NET unknown primary Staging No CT 27 F 56 NET unknown primary Follow-up No CT, MRI 28 F 57 Hypoglycemia Detection NGP and CCR Histology 29 F 41 Carcinoid of pancreas Staging No CT 30 M 73 Elevation of CgA and NSE Detection Diarrhea MRI, histology 31 M 75 Hypoglycemia Detection NGP and CCR MRI 32 M 51 Carcinoid of stomach Staging No CT 33 F 58 NET unknown primary Follow-up Flush, diarrhea CT 34 M 63 Elevation of CgA and NSE Detection Diarrhea CT, MRI 35 M 62 Small bowel carcinoid Staging No CT 36 F 47 NET unknown primary Staging No CT, histology 37 F 28 Elevation of CgA and NSE Detection No Histology 38 F 41 Broncogenic carcinoid Follow-up No CT 39 M 51 Carcinoid of pancreas Staging Diarrhea CT 40 F 40 Elevation of CgA and NSE Detection No Histology 41 M 77 NET of prostate gland Staging No CT, NaF 42 M 54 Hypoglycemia Detection NGP and CCR CT, MRI 43 M 69 Carcinoid of stomach Staging No CT 44 M 64 Carcinoid of pancreas Staging No CT 45 M 84 Carcinoid of pancreas Staging Flush CT, MRI 46 M 74 NET unknown primary Staging No CT 47 M 74 Broncogenic carcinoid Staging No CT 48 F 43 Carcinoid of pancreas Staging No CT, MRI 49 M 56 Small bowel carcinoid Staging No CT 50 F 57 Small bowel carcinoid Staging No CT, NaF 51 F 58 Small bowel carcinoid Staging Flush CT 52 M 55 Elevation of CgA and NSE Detection No Histology 53 F 51 Elevation of gastrin Detection Gastritis CT, MRI, biopsy 54 M 62 Broncogenic carcinoid Follow-up No CT, MRI 55 M 40 Carcinoid of pancreas (VIPoma) Staging Diarrhea CT, NaF 56 F 67 Small bowel carcinoid Follow-up No CT 57 F 76 Carcinoid of stomach Staging Diarrhea CT, NaF 58 M 34 Carcinoid of pancreas Follow-up No CT, NaF 59 M 66 Small bowel carcinoid Staging No CT 60 M 64 Small bowel carcinoid Follow-up No CT 61 M 58 Small bowel carcinoid Follow-up Flush, diarrhea CT 62 M 59 Small bowel carcinoid Staging No CT 63 F 75 Small bowel carcinoid Staging No CT, MRI 64 M 47 Small bowel carcinoid Follow-up No CT 65 F 61 Broncogenic carcinoid Follow-up No CT, MRI 66 M 62 Small bowel carcinoid Staging No CT 67 M 35 Carcinoid of middle ear Follow-up No CT, MRI 68 M 65 Carcinoid of cecum Follow-up Flush CT 69 M 62 Small bowel carcinoid Follow-up Diarrhea CT 70 M 50 Small bowel carcinoid Staging No CT 71 F 78 Small bowel carcinoid Follow-up No CT, NaF 72 F 37 Hypoglycemia Detection NGP and CCR CT, MRI 73 M 73 Paraganglioma Follow-up No CT, MRI 74 M 79 Carcinoid of rectum Staging No CT 75 F 64 Carcinoid of stomach Follow-up No CT 76 F 66 Broncogenic carcinoid Follow-up No CT 77 F 60 Small bowel carcinoid Follow-up Diarrhea CT 78 M 67 Carcinoid of rectum Follow-up No CT 79 M 69 Paraganglioma Staging No MRI, histology 80 F 47 Small bowel carcinoid Follow-up No CT, MRI, histology 81 F 59 Carcinoid of pancreas Follow-up No CT, NaF 82 M 59 Carcinoid of pancreas Staging No CT, MRI, NaF 83 M 65 Small bowel carcinoid Follow-up No CT 84 M 54 Small bowel carcinoid Follow-up No CT Uptake Features of tracer accumulation Nonmalignant Linear, nonfocal limited intestinal uptake with moderate intensity Tracer uptake less intense than liver uptake Pancreatic head (PET): small sickle-shaped findings in right upper abdomen just below left liver lobe; diffuse nature of uptake Malignant Clearly demarked findings with higher tracer uptake compared with liver uptake Tracer accumulation in structures that did not take up tracer physiologically or was higher than background activity Pancreatic head: irregular or protrusive shape of finding; clear delineation from adjacent tissue with higher uptake than liver uptake Parameter 20 min 1 h 1 h 40 min Liver 6.2 ± 1.7 5.9 ± 2.1 5.5 ± 2.4 Background 0.8 ± 0.5 0.6 ± 0.4 0.6 ± 0.4 Tumor in liver 12.9 ± 4.9 14.6 ± 5.9 15.8 ± 6.9 Tumor in abdomen 9.0 ± 6.7 10.6 ± 7.5 11.6 ± 7.2 SUVbw is for selected tissue from 8 patients. SD gives interpatient variability.
PET SPECT CT Group n TP TN FP FN TP TN FP FN TP TN FP FN Detection 13 4 8 1 0 2 8 1 2 3 8 1 1 Staging 36 32 3 0 1 14 3 0 19 16 3 2 15 Follow-up 34 33 1 0 1 21 1 0 13 22 1 2 10 Overall 84 69 12 1 2 37 12 1 34 41 12 5 26 Parameter PET (%) SPECT (%) CT (%) Sensitivity 97 (69/71) 52 (37/71) 61 (41/67) Specificity 92 (12/13) 92 (12/13) 71 (12/17) Accuracy 96 (81/84) 58 (49/84) 63 (53/84) Number of patients is in parentheses.
Site PET SPECT CT Cranium 5 5 5 Neck/chest 35 30 31 Liver 56 46 56 Pancreas 23 21 19 Lymph nodes 90 68 87 Other 50 48 39 Bone 116 84 58 Overall 375 302 295 Other sites include, but are not mentioned, locations of tumor deposits—for example, peritoneal carcinosis.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- SNMMI Procedure Standard/EANM Practice Guideline for SSTR PET: Imaging Neuroendocrine Tumors
- Importance of PET with 68Ga-Labeled Somatostatin Analogs (perspective on "68Ga-DOTA-Tyr3-Octreotide PET in Neuroendocrine Tumors: Comparison with Somatostatin Receptor Scintigraphy and CT" J Nucl Med. 2007;48:508-518)
- Prognostic Value of 18F-FDG PET/CT in a Large Cohort of Patients with Advanced Metastatic Neuroendocrine Neoplasms Treated with Peptide Receptor Radionuclide Therapy
- Safety, tolerability and clinical implementation of 'ready-to-use 68gallium-DOTA0-Tyr3-octreotide (68Ga-DOTATOC) (SomaKIT TOC) for injection in patients diagnosed with gastroenteropancreatic neuroendocrine tumours (GEP-NETs)
- Improving Contrast and Detectability: Imaging with [55Co]Co-DOTATATE in Comparison with [64Cu]Cu-DOTATATE and [68Ga]Ga-DOTATATE
- 111In-Pentetreotide Scintigraphy Versus 68Ga-DOTATATE PET: Impact on Krenning Scores and Effect of Tumor Burden
- Multimodality imaging in carcinoid heart disease
- Twelve-Year Follow-up After Peptide Receptor Radionuclide Therapy
- CMKLR1-targeting peptide tracers for PET/MR imaging of breast cancer
- Safety, Biodistribution, and Radiation Dosimetry of 68Ga-OPS202 in Patients with Gastroenteropancreatic Neuroendocrine Tumors: A Prospective Phase I Imaging Study
- Sensitivity Comparison of 68Ga-OPS202 and 68Ga-DOTATOC PET/CT in Patients with Gastroenteropancreatic Neuroendocrine Tumors: A Prospective Phase II Imaging Study
- Current Concepts in 68Ga-DOTATATE Imaging of Neuroendocrine Neoplasms: Interpretation, Biodistribution, Dosimetry, and Molecular Strategies
- Somatostatin Receptor 2-Targeting Compounds
- 68Ga-DOTATOC Imaging of Neuroendocrine Tumors: A Systematic Review and Metaanalysis
- Localization of Unknown Primary Site with 68Ga-DOTATOC PET/CT in Patients with Metastatic Neuroendocrine Tumor
- Parametric Net Influx Rate Images of 68Ga-DOTATOC and 68Ga-DOTATATE: Quantitative Accuracy and Improved Image Contrast
- The Impact of Somatostatin Receptor-Directed PET/CT on the Management of Patients with Neuroendocrine Tumor: A Systematic Review and Meta-Analysis
- MIB-1 Index-Stratified Assessment of Dual-Tracer PET/CT with 68Ga-DOTATATE and 18F-FDG and Multimodality Anatomic Imaging in Metastatic Neuroendocrine Tumors of Unknown Primary in a PRRT Workup Setting
- Head-to-Head Comparison of 64Cu-DOTATATE and 68Ga-DOTATOC PET/CT: A Prospective Study of 59 Patients with Neuroendocrine Tumors
- 68Ga-DOTATATE PET/CT Interobserver Agreement for Neuroendocrine Tumor Assessment: Results of a Prospective Study on 50 Patients
- Comparison of the Impact of 68Ga-DOTATATE and 18F-FDG PET/CT on Clinical Management in Patients with Neuroendocrine Tumors
- 68Ga-DOTATOC PET/CT in Patients with Iodine- and 18F-FDG-Negative Differentiated Thyroid Carcinoma and Elevated Serum Thyroglobulin
- A Delphic consensus assessment: imaging and biomarkers in gastroenteropancreatic neuroendocrine tumor disease management
- Clinical Translation of a Click-Labeled 18F-Octreotate Radioligand for Imaging Neuroendocrine Tumors
- Safety and Efficacy of 68Ga-DOTATATE PET/CT for Diagnosis, Staging, and Treatment Management of Neuroendocrine Tumors
- Potential value of EUS in pancreatic surveillance of VHL patients
- Evaluation of the Efficacy of Targeted Imaging Agents
- Prospective Study of 68Ga-DOTATATE Positron Emission Tomography/Computed Tomography for Detecting Gastro-Entero-Pancreatic Neuroendocrine Tumors and Unknown Primary Sites
- Significance of a Single-Time-Point Somatostatin Receptor SPECT/Multiphase CT Protocol in the Diagnostic Work-up of Gastroenteropancreatic Neuroendocrine Neoplasms
- Appendiceal neuroendocrine neoplasms: diagnosis and management
- Prognostic Value of 68Ga-DOTANOC PET/CT SUVmax in Patients with Neuroendocrine Tumors of the Pancreas
- 64Cu-DOTATATE PET for Neuroendocrine Tumors: A Prospective Head-to-Head Comparison with 111In-DTPA-Octreotide in 112 Patients
- Increased 68Ga-DOTATATE Uptake in PET Imaging Discriminates Meningioma and Tumor-Free Tissue
- Can Complementary 68Ga-DOTATATE and 18F-FDG PET/CT Establish the Missing Link Between Histopathology and Therapeutic Approach in Gastroenteropancreatic Neuroendocrine Tumors?
- 68Ga-DOTATATE PET/CT, 99mTc-HYNIC-Octreotide SPECT/CT, and Whole-Body MR Imaging in Detection of Neuroendocrine Tumors: A Prospective Trial
- Preclinical Evaluation of a High-Affinity 18F-Trifluoroborate Octreotate Derivative for Somatostatin Receptor Imaging
- PET/MR in Oncology: Non-18F-FDG Tracers for Routine Applications
- Evaluating digestive neuroendocrine tumor progression and therapeutic responses in the era of targeted therapies: state of the art
- 18F-Fluorodihydroxyphenylalanine PET/CT in Patients with Neuroendocrine Tumors of Unknown Origin: Relation to Tumor Origin and Differentiation
- Promises of Cyclotron-Produced 44Sc as a Diagnostic Match for Trivalent {beta}--Emitters: In Vitro and In Vivo Study of a 44Sc-DOTA-Folate Conjugate
- Comparison of Response Evaluation in Patients with Gastroenteropancreatic and Thoracic Neuroendocrine Tumors After Treatment with [177Lu-DOTA0,Tyr3]Octreotate
- Comparison of 68Ga-DOTANOC and 68Ga-DOTATATE PET/CT Within Patients with Gastroenteropancreatic Neuroendocrine Tumors
- The Role of 68Ga-DOTATATE PET/CT in Suspected Neuroendocrine Tumors
- Tumor Response Assessment to Treatment with [177Lu-DOTA0,Tyr3]Octreotate in Patients with Gastroenteropancreatic and Bronchial Neuroendocrine Tumors: Differential Response of Bone Versus Soft-Tissue Lesions
- Unexpected Sensitivity of sst2 Antagonists to N-Terminal Radiometal Modifications
- A Man with Abdominal Pain: Enough Evidence for Surgery?
- Nuclear medicine imaging of neuroendocrine tumours
- Clinical PET of Neuroendocrine Tumors Using 64Cu-DOTATATE: First-in-Humans Study
- Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumours (NETs)
- 68Ga-DOTATOC Versus 68Ga-DOTATATE PET/CT in Functional Imaging of Neuroendocrine Tumors
- The SNM Practice Guideline for Somatostatin Receptor Scintigraphy 2.0
- Radiopeptide Imaging and Therapy in Europe
- Novel SDHD Gene Mutation (H102R) in a Patient With Metastatic Cervical Paraganglioma Effectively Treated by Peptide Receptor Radionuclide Therapy
- Treatment with Octreotide Does Not Reduce Tumor Uptake of 68Ga-DOTATATE as Measured by PET/CT in Patients with Neuroendocrine Tumors
- Nuclear medicine techniques for the imaging and treatment of neuroendocrine tumours
- 177Lu-DOTATATE Molecular Radiotherapy for Childhood Neuroblastoma
- Incidence of Increased 68Ga-DOTANOC Uptake in the Pancreatic Head in a Large Series of Extrapancreatic NET Patients Studied with Sequential PET/CT
- Somatostatin Receptors as Targets for Nuclear Medicine Imaging and Radionuclide Treatment
- 68Ga-DOTATOC PET/CT of Neuroendocrine Tumors: Spotlight on the CT Phases of a Triple-Phase Protocol
- Expression of somatostatin receptors, dopamine D2 receptors, noradrenaline transporters, and vesicular monoamine transporters in 52 pheochromocytomas and paragangliomas
- Diagnostics of Neuroendocrine Tumours
- Exendin-4-Based Radiopharmaceuticals for Glucagonlike Peptide-1 Receptor PET/CT and SPECT/CT
- The Role of 68Ga-DOTATATE PET in Patients with Neuroendocrine Tumors and Negative or Equivocal Findings on 111In-DTPA-Octreotide Scintigraphy
- 68Ga-DOTANOC PET/CT Clinical Impact in Patients with Neuroendocrine Tumors
- Somatostatin receptor-based imaging and therapy of gastroenteropancreatic neuroendocrine tumors
- Features of Carcinoid Heart Disease Identified by 2- and 3-Dimensional Echocardiography and Cardiac MRI
- A Comparison of 68Ga-DOTATATE and 18F-FDG PET/CT in Pulmonary Neuroendocrine Tumors
- 68Ga-DOTA-Tyr3-Octreotide PET for Assessing Response to Somatostatin-Receptor-Mediated Radionuclide Therapy
- Bone Metastases in Patients with Neuroendocrine Tumor: 68Ga-DOTA-Tyr3-Octreotide PET in Comparison to CT and Bone Scintigraphy
- 99mTc-HYNIC-TOC Scintigraphy Is Superior to 131I-MIBG Imaging in the Evaluation of Extraadrenal Pheochromocytoma
- The clinical value of [18F]fluoro-dihydroxyphenylalanine positron emission tomography in primary diagnosis, staging, and restaging of neuroendocrine tumors
- New Technologies for Human Cancer Imaging
- Tumor Receptor Imaging
- Utility of Radiolabeled Somatostatin Receptor Analogues for Staging/Restaging and Treatment of Somatostatin Receptor-Positive Pediatric Tumors
- Somatostatin Receptor Imaging in Patients with Neuroendocrine Tumors: Not Only SPECT?