


Abstract
This study aimed to assess the clinical impact of 68Ga-DOTATATE and 18F-FDG with respect to the management plan and to evaluate the prognostic value of both tracers. Methods: A total of 104 patients (55 male and 49 female; median age, 58 y; range, 20–90 y) with histologically proven neuroendocrine tumors (NETs) underwent both 68Ga-DOTATATE and 18F-FDG PET/CT. Twenty-eight patients (26.9%) had poorly differentiated tumors, and 76 (73.1%) had well-differentiated tumors. PET/CT results and SUVs were compared with prognostic factors such as histologic grade (G1, G2, or G3, for low-grade [well differentiated], intermediate-grade [moderately differentiated], and high-grade [poorly differentiated], respectively), chromogranin A, and proliferation index (Ki-67). Results: The 68Ga-DOTATATE and 18F-FDG PET/CT findings were discordant in 65 patients (62.5%) and concordant in 39 patients (37.5%). The results changed the therapeutic plan in 84 patients (80.8%). In 22 patients (21.1%), decision making was based on the 18F-FDG findings; in 32 (30.8%), on the findings with both radiotracers; and in 50 (48.1%), on the 68Ga-DOTATATE findings. The most frequent management decision based on 18F-FDG was initiation of chemotherapy (10 patients, 47.6%). The most common treatment decision due to 68Ga-DOTATATE was initiation of peptide receptor radionuclide therapy (14 patients, 27.4%). In 11 (39.2%) of 28 patients with poorly differentiated NETs, the management decision was based on only the 18F-FDG results. For 68Ga-DOTATATE, SUVmax was higher for G1 tumors and lower for G3 tumors (P = 0.012). However, no significant differences in 18F-FDG-derived SUVs were observed between different grades (P = 0.38). The Mann–Whitney test showed significant differences in 68Ga-DOTATATE SUVmax between tumors with a Ki-67 of less than 5% and tumors with a Ki-67 of more than 5% (P = 0.004), without significance differences in 18F-FDG SUVmax. Log-rank analysis showed statistically significant differences in survival for patients with bone metastasis versus soft-tissue or no metastasis for both 18F-FDG (P = 0.037) and 68Ga-DOTATATE (P = 0.047). Overall survival declined rapidly with increasing grade (P = 0.001), at an estimated 91 mo for G1, 59 mo for G2, and 48 mo for G3. Conclusion: 18F-FDG PET/CT had no clinical impact on G1 NETs and a moderate impact on G2 NETs. However, in poorly differentiated NETs, 18F-FDG PET/CT plays a significant clinical role in combination with 68Ga-DOTATATE. 68Ga DOTATATE SUVmax relates to grade and Ki-67 and can be used prognostically.
Neuroendocrine tumors (NETs) are a heterogeneous group of malignancies ranging from well-differentiated, slowly growing tumors to poorly differentiated neoplasms, which are aggressive and less frequent (1). Neuroendocrine cells have the ability to express several peptide receptors in high volumes, especially somatostatin receptors, which are heptahelical G-protein–coupled glycoprotein transmembrane receptors (2). In the past, evaluation of NETs was based mainly on somatostatin receptor scintigraphy and other conventional imaging methods such as ultrasound, CT, endoscopy, and MRI (3,4); however, after the advent of PET/CT systems, novel PET tracers have been developed and investigated, including biogenic amine precursors (e.g., 18F-dihydroxyphenylalanine), somatostatin analogs (68Ga-DOTA), and metabolic markers (18F-FDG) (3).
Three main DOTA-peptides (DOTATOC, DOTANOC, and DOTATATE) that specifically bind to somatostatin receptors overexpressed on the surface of NET cells, allowing visualization of NETs, have been used in the clinical setting for either NET diagnosis or peptide receptor radionuclide therapy (PRRT) (5,6). PET/CT with 68Ga-DOTA-peptides has been reported to present a higher sensitivity for the detection of well-differentiated, less aggressive NETs than CT or scintigraphy (7,8). On the other hand, 18F-FDG PET/CT is preferred for more aggressive, less differentiated NETs as there is emerging evidence that the presence of increased glucose in NETs highlights an increased propensity for invasion and metastasis, and an overall poorer prognosis (9). In fact, a strong association has recently been shown between higher 18F-FDG uptake and worse outcome even in patients with well-differentiated or low-grade tumors, with provision of prognostic information independently of the mitotic rate (9). Accordingly, 18F-FDG may retain an important role in managing patients with NETs because of its high prognostic value and its higher sensitivity in delineating disease extent, especially in aggressive and high-grade tumors (4).
Although the value of PET findings with both 68Ga-DOTA-peptides and 18F-FDG is therefore well established, the detection of additional sites of disease is not necessarily associated with alteration of therapeutic approach. The aims of this study were to evaluate and compare the clinical impact of 68Ga-DOTATATE and 18F-FDG PET/CT on the management plan in patients with NETs and to assess the prognostic value of SUVmax for both tracers.
MATERIALS AND METHODS
Patient Population
We retrospectively reviewed the findings for the first 104 patients (55 male and, 49 female; age range, 20–90 y; median, 58 y) with histologically proven NETs who underwent contemporaneous 68Ga-DOTATATE and 18F-FDG PET/CT at our institution between September 2006 and February 2014. The interval between the two studies ranged from 0 to 3 wk (median, 1 wk), which was considered sufficiently short given that NETs show relatively slow progression.
Each case of NET was classified as high, intermediate, or low grade according to the histology reports, based on recent consensus statements of the European Neuroendocrine Tumor Society, using mitotic index and Ki-67 index in staging of NETs along with immunohistochemistry (10) The study was approved by the institutional review board (study 15N10051), and all subjects gave written informed consent.
Image Acquisition
Images were acquired 1 h after injection of 370 MBq of 18F-FDG or 45–60 min after injection of 120–200 MBq of 68Ga-DOTATATE. No adverse effects were observed after the injection of 68Ga-DOTATATE or 18F-FDG. Imaging was performed using a dedicated Discovery ST PET/CT unit, with a 16-detector CT component (GE Healthcare); whole-body examinations (brain to midthigh) were performed with the patient supine. The CT exposure factors were 120 kVp and 80 mA in 0.8 s. Maintaining patient position, a whole-body PET emission scan was performed over an area identical to that covered by the CT scan. The PET acquisition was performed in 3 dimensions at 4 min per bed position, using a 9-slice overlap. The PET images were reconstructed using CT for attenuation correction. Transaxial PET data were reconstructed using ordered-subsets expectation maximization with 2 iterations and 21 subsets. The transaxial PET slice thickness was 3.27 mm, with an in-slice pixel size of 4.68 mm. The CT data were reconstructed to axial slices 3.75 and 2.5 mm thick using a soft-tissue algorithm.
Image Interpretation
The 68Ga-DOTATATE and 18F-FDG PET/CT images were interpreted in consensus by an experienced dedicated nuclear medicine physician and a dual-accredited radiologist/nuclear medicine physician. For the 68Ga-DOTATATE PET/CT studies, any area with an intensity greater than background that could not be identified as physiologic activity (pituitary gland, spleen, liver, adrenal glands, head of the pancreas, thyroid, and urinary tract) was considered to indicate tumor tissue (6). The 68Ga-DOTATATE scanning was performed after discontinuation of short-acting somatostatin analogs for 72 h and long-acting somatostatin analogs for 28 d. The findings of the two modalities were compared with each other and with the histologic findings. Furthermore, SUVmax was calculated by measuring the maximum concentration of the labeled tracer (kBq/mL) in the lesion divided by the decay-corrected injected activity (kBq) and normalized for body weight.
Clinical Impact
To evaluate the clinical impact of the PET/CT findings, the referring physicians were subsequently asked to provide information on how patients were managed and how the PET/CT results had influenced clinical decisions after retrieving all clinical data. The overall impact was evaluated patient by patient and was correlated with the histologic findings. To perform a survival analysis, the last date of survival and the last date of follow-up were recorded and the patients were censored regarding whether their cause of death was related to their disease.
Statistical Analysis
Metric data such as age were expressed as mean ± SD. One-way ANOVA was used to assess differences in SUVmax across grades for both 68Ga-DOTATATE and 18F-FDG. The Mann–Whitney test was used to assess for differences in SUVmax between a Ki-67 of less than 5% and a Ki-67 of more than 5%, as well as a Ki-67 threshold of 12%, for both 68Ga-DOTATATE and 18F-FDG. A P value of less than 0.05 was considered significant. Statistical analysis was performed with SPSS software (version 22.0; IBM).
The Spearman correlation coefficient was used to assess for a correlation between the SUVmax for either tracer and Ki-67. Kaplan–Meier survival analysis was performed to assess the prognostic value of the 68Ga-DOTATATE and 18F-FDG findings regarding overall survival. To assess whether different scan findings related to overall survival, the Kaplan–Meier product limit estimators were calculated and compared by log-rank tests. Specifically, it was tested whether soft-tissue and bone metastases will result in statistically significant differences in survival. Finally, the prognostic value of histologic grade and Ki-67 regarding survival was also evaluated.
RESULTS
The clinical and epidemiologic characteristics of the 104 patients are shown in Table 1.
Clinical and Epidemiologic Characteristics of the Patients
Discordant Findings
The 68Ga-DOTATATE and 18F-FDG PET/CT findings were discordant in 65 patients (62.5%) and concordant in 39 (37.5%). Discordant findings were observed in 25 patients (38.4%) with G1 NETs (low-grade: well differentiated), in 24 (36.9%) with G2 NETs (intermediate-grade: moderately differentiated), and in 16 (24.7%) with G3 NETs (high-grade: poorly differentiated) (P > 0.05). In only 1 (2.7%) of 36 patients with G1 tumors (Ki-67 ≤ 2) (P < 0.05) and 5 (12.5%) of 40 with G2 tumors (Ki-67 ≤ 12%) (P < 0.05) were the 18F-FDG findings more prominent than the 68Ga-DOTATATE findings. However, in all 6 of these patients the 18F-FDG–avid findings did not correlate with NET disease as shown either by biopsy or by follow-up imaging. The two patients with increased metabolic bowel activity underwent a subsequent colonoscopy that showed, in one case, large-bowel adenocarcinoma and, in the second, inflammatory changes. The remaining 4 patients had lung 18F-FDG–avid abnormalities, all of which were benign as confirmed on follow-up lung contrast-enhanced CT. In 2 patients in particular, there was a need for follow-up for 12 mo to confirm the inflammatory pathology.
Of the 25 patients with discordant results, 22 (88%) with G1 NETs had 68Ga-DOTATATE–positive findings (P < 0.05) and 9 (56%) of 16 with G3 NETs had 18F-FDG–positive findings (P < 0.05), confirming that 68Ga-DOTATATE is positive predominantly with a lower Ki-67 whereas 18F-FDG is positive with a higher Ki-67.
Clinical Impact
Considering all cases, the combination of 68Ga-DOTATATE and 18F-FDG PET/CT modified therapy in 84 patients (80.8%). The treatments before the PET/CT scans are listed in Table 2. In 22 patients (21.1%), the modification was based on 18F-FDG findings; in 32 (30.8%), on the findings with both radiotracers; and in 50 (48.1%), on the 68Ga-DOTATATE findings (Table 3). The most frequent management impact of only 18F-FDG findings was initiation or continuation of chemotherapy in 10 patients (47.6%), whereas the second most frequent was surgery in 5 patients (23.8%), followed by active surveillance. The most common treatment modification due to 68Ga-DOTATATE findings was initiation of PRRT in 14 patients (27.4%), followed by commencement of somatostatin analogs in 12 (23.5%). In general, there was a change of medical treatment in 40 patients (38.5%: confirmation of current treatment in 36 patients (34.6%), change in surgical planning in 15 (14.4%), and cancellation of surgery in 13 (12.5%).
Treatment Before 18F-FDG and 68Ga-DOTATATE PET/CT
Management Based on 18F-FDG and 68Ga-DOTATATE PET/CT Findings
Table 4 correlates grade with the PET/CT tracer that had the greatest clinical impact. In 11 of 28 patients (39.2%) with poorly differentiated NETs, the management decision was based on only the 18F-FDG results. In only 1 (2.7%) of 36 patients with G1 tumors (Ki-67 ≤ 2%) (P = 0.001) and 10 (12.5%) of 40 with G2 tumors (Ki-67 ≤ 12%) (P = 0.003) was the management changed because of the 18F-FDG results. There was no statistically significant correlation between the presence of chromogranin A in the histologic specimen and the results with either radiotracer (P = 0.69 for 68Ga-DOTATATE, P = 0.37 for 18F-FDG). Overall, 68Ga-DOTATATE was more likely to affect the final decision for tumors with a low Ki-67 expression, whereas 18F-FDG was better in tumors with a high Ki-67 expression, as demonstrated by Figure 1. Regarding the G2 group, we found that in patients with tumors with a Ki-67 of no more than 12%, 68Ga-DOTATATE made a greater contribution to clinical management than did 18F-FDG.
Correlation of Grade with 18F-FDG and 68Ga-DOTATATE PET/CT Findings
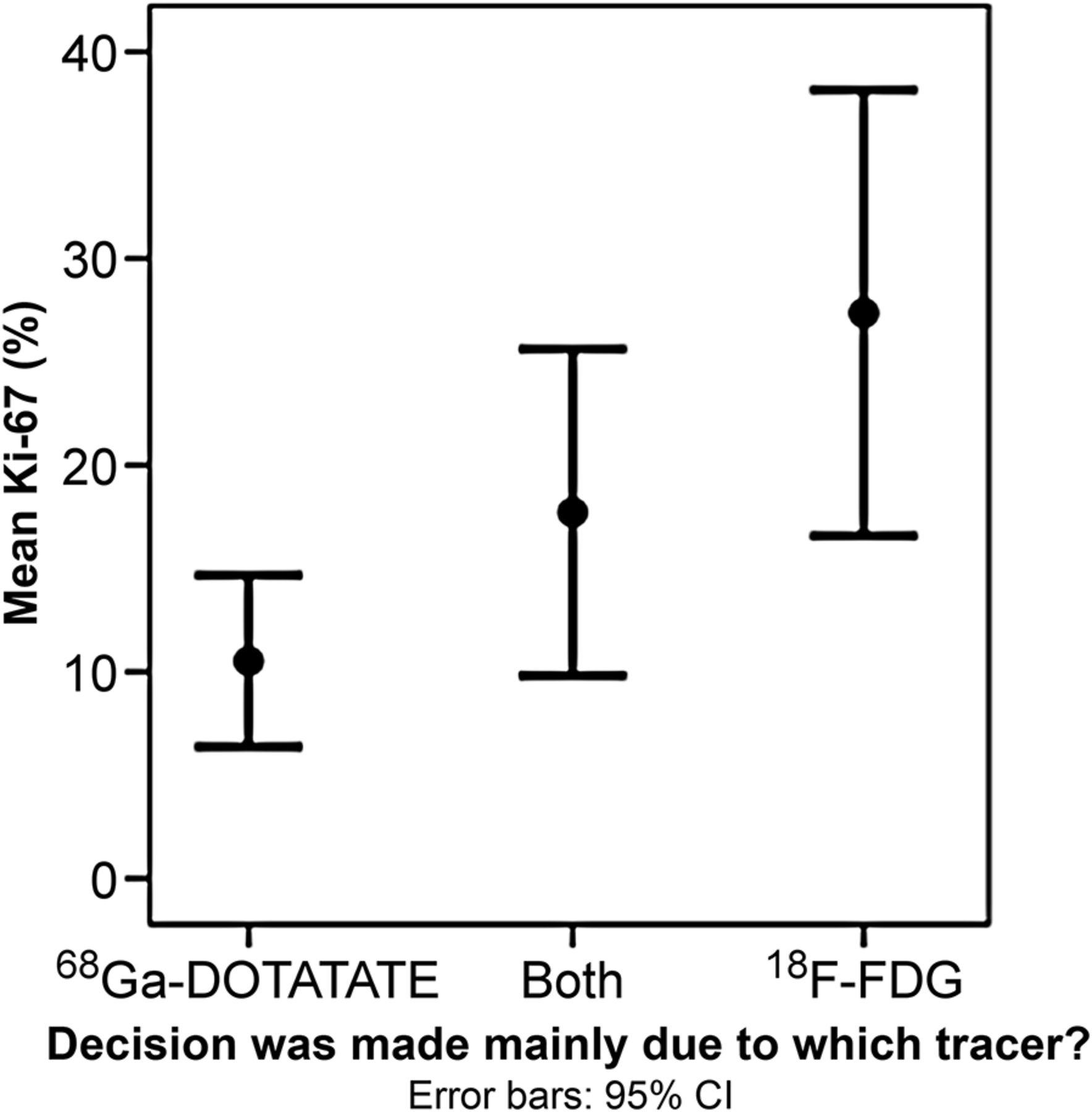
Correlation between mean Ki-67 of NETs and PET/CT tracer results on which clinical management decision was based.
Using Kaplan–Meier plots and log-rank comparisons, survival was found to decline rapidly with increasing grade (P = 0.001), with an estimated survival of 91 mo for G1, 59 mo for G2, and 48 mo for G3.
Using 1-way ANOVA, 68Ga-DOTATATE SUVmax was significantly higher for G1 tumors than for G3 (P = 0.012). However, no significant differences in 18F-FDG–derived SUVmax results between grades were detected (P = 0.38). As expected, there was a statistically significant negative correlation between Ki-67 and 68Ga-DOTATATE SUVmax (Spearman ρ = −0.374, P = 0.001). On the other hand, a significant positive correlation was noted between Ki-67 and 18F-FDG SUVmax (ρ = −0.345, P = 0.002). Further analysis showed significant differences in 68Ga-DOTATATE SUVmax between tumors with a Ki-67 of less than 5% and tumors with a Ki-67 of more than 5% (P = 0.004), whereas no significance difference in 18F-FDG SUVmax was detected using this cutoff. Interestingly, the Mann–Whitney test showed more statistically significant differences in SUVmax for tumors with a Ki-67 of 12% or less than for those with a Ki-67 of more than 12% (P = 0.002) for 68Ga-DOTATATE but not for 18F-FDG, indicating that tumors with a Ki-67 of more than 12% are more aggressive.
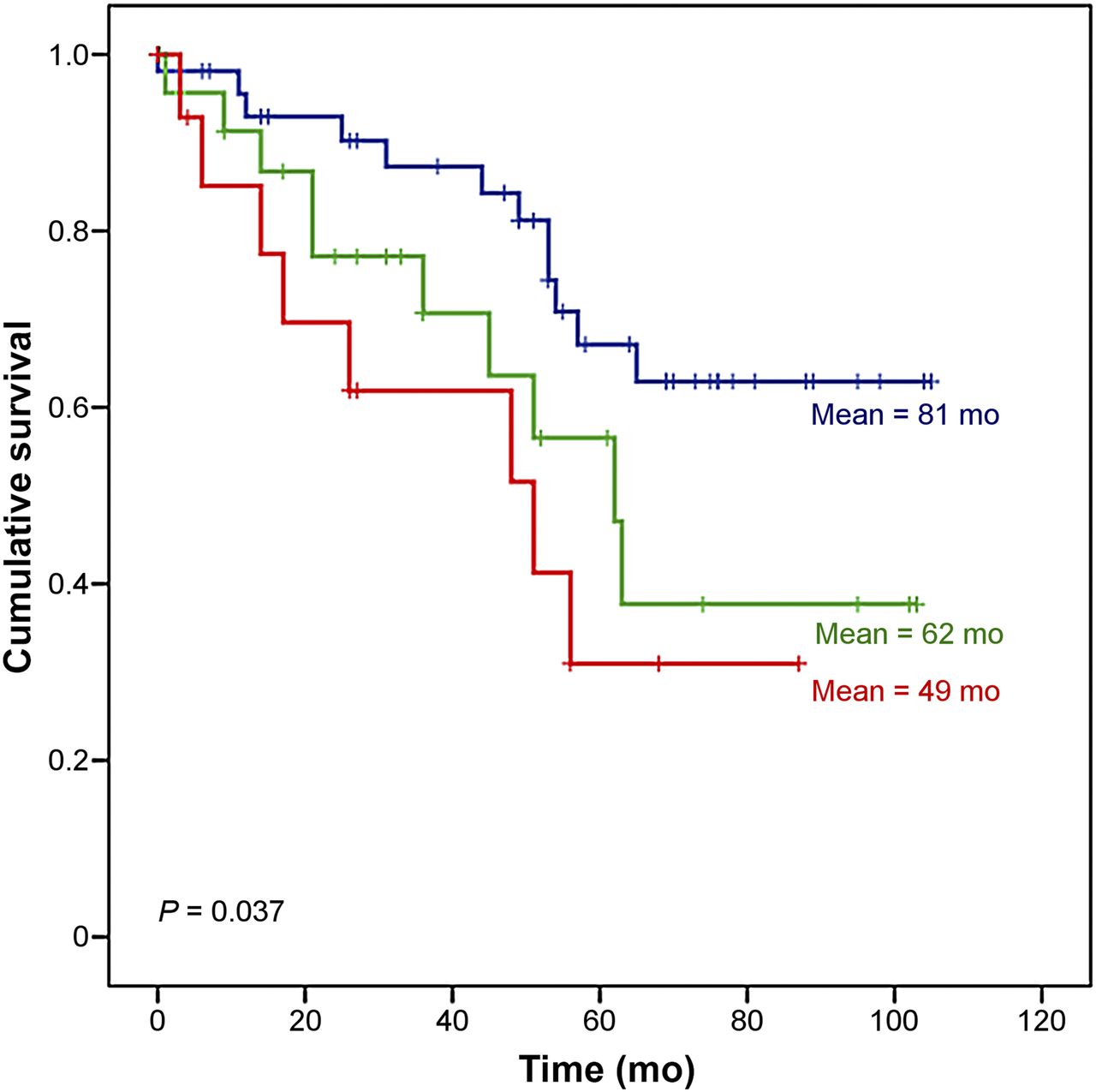
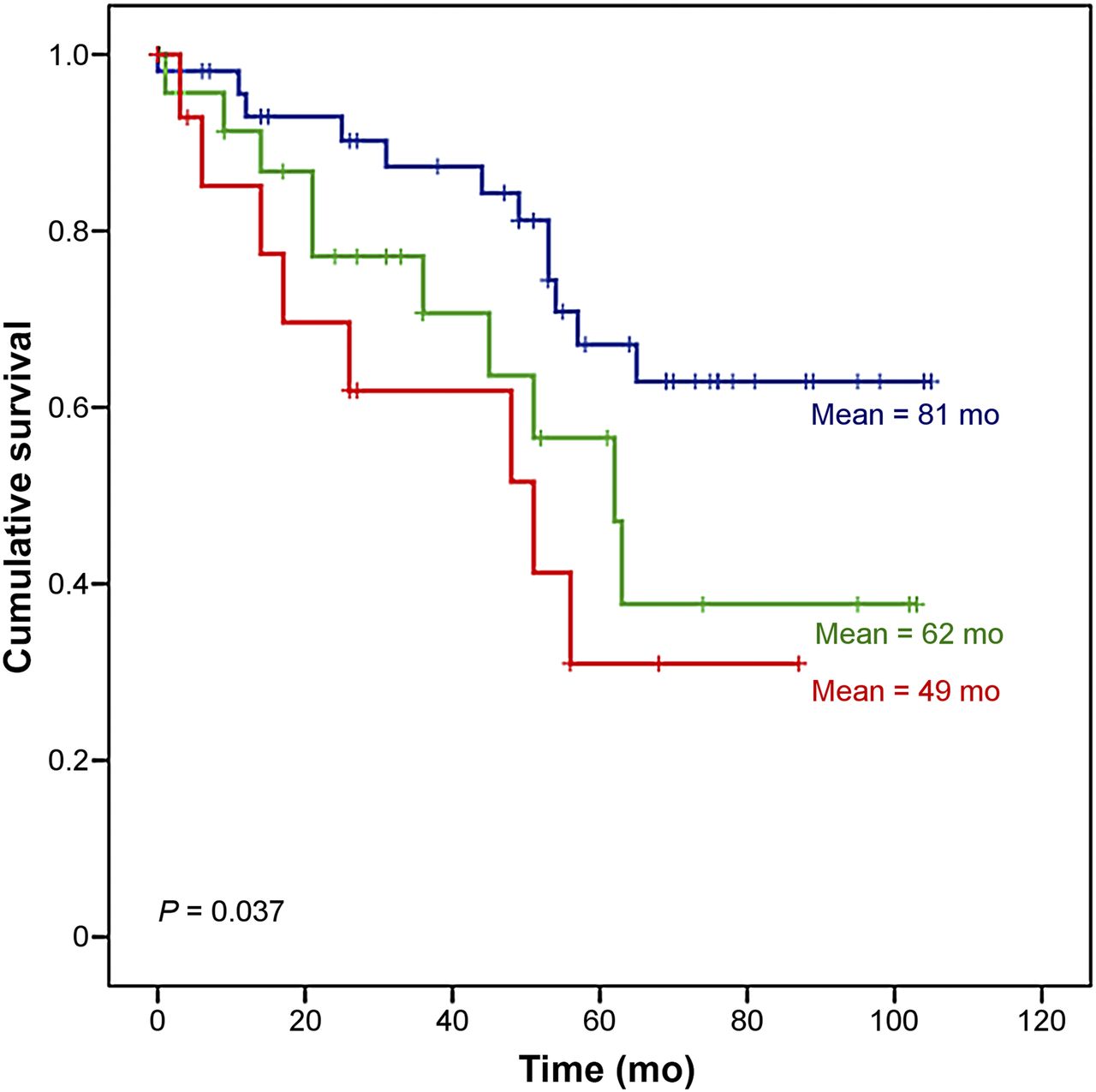
Using a grade of zero for no metastasis, 1 for soft-tissue metastasis, and 2 for bone metastasis, log-rank analysis showed statistically significant differences in survival for patients with bone metastasis versus soft-tissue or no metastasis (Figs. 2 and 3). This was true both for 18F-FDG scans (P = 0.037) and for 68Ga-DOTATATE scans (P = 0.047), with estimated survival significantly reduced in patients with bone metastasis (48 and 49 mo for 68Ga-DOTATATE and 18F-FDG, respectively) versus those with soft-tissue metastasis (74 and 62 mo) or no metastasis (80 and 81 mo).

Survival curves for patients with bone metastasis (red) vs. soft-tissue metastasis (green) or no metastasis (blue) detected using 68Ga-DOTATATE.
Survival curves for patients with bone metastasis (red) vs. soft-tissue metastasis (green) or no metastasis (blue) detected using 18F-FDG.
DISCUSSION
Imaging plays a crucial role in the diagnosis and management of NETs, because the initial diagnostic work-up and staging after histologic confirmation form the basis for the decision on whether to perform surgical resection or to initiate medical therapy. The small size of NETs makes it difficult for conventional anatomic imaging to visualize the primary tumor or its metastases, given that these modalities are unable to depict specific endocrine features; consequently, the diagnostic accuracy of functional imaging is significantly higher than that of conventional imaging (7,11–14).
18F-FDG PET/CT imaging has also been compared with 68Ga-DOTA peptide imaging in several studies, which have shown it to have variable sensitivity in detecting NETs (15–22). However, the presence of increased glucose in NETs highlights an increased propensity for invasion and metastasis, and 18F-FDG PET/CT accordingly has higher sensitivity in delineating disease extent, especially in aggressive and high-grade tumors (23). Detection of a higher number of lesions is nevertheless not always followed by a change in disease stage and, most importantly, does not always affect the therapeutic approach. Although several studies have demonstrated the clinical impact of 68Ga-DOTA peptides, few have compared the clinical impact of both PET tracers in NET patients (24–27).
To the best of our knowledge, our study is the first to determine the clinical impact of combined 68Ga-DOTATATE and 18F-FDG PET/CT in such a large, histologically proven NET population in correlation with grade. Most previous studies have compared the diagnostic accuracy of both radiotracers, with a relative lack of information regarding the influence on treatment approach.
Our study demonstrates that routine use of both 68Ga-DOTATATE and 18F-FDG PET/CT is not recommended for G1 NETs. In this NET subgroup, the clinical impact was influenced predominately by the 68Ga-DOTATATE study, which we suggest should be performed solely. In the G3 NET group the combination of both examinations is suggested, with emphasis on the 18F-FDG results in patients with higher Ki-67 values, reflecting a high level of glycolytic metabolism in high-risk patients with aggressive disease and poorer prognosis in whom chemotherapy is favorable (9). However, 68Ga-DOTATATE should also be considered in this subgroup, especially in the event of a relapse during a chemotherapy regimen, as the somatostatin receptor positivity makes PRRT a potential therapeutic option. Jamali et al. have reported that 18F-FDG–positive high-grade gastroenteropancreatic NET patients have benefited from PRRT (28). Nevertheless, this should be proven by a pre- and post-PRRT 68Ga-DOTA-peptide study to better delineate the tumor burden and further assess treatment response.
The current study demonstrates also that 18F-FDG PET/CT has a moderate clinical impact in G2 NETs. We propose that in NET patients with a Ki-67 of 12% or less, the use of 18F-FDG PET/CT should be limited and tailored to the individual patient, especially when suspicion of a second synchronous primary tumor is raised by an atypical disease distribution or when the patient had a previous neoplastic process. NETs with a Ki-67 of lower than 10% may tend to fall into the low-grade category, which may be why the patients in such cases have been reported to have a better prognosis (29).
Strosberg et al. have proposed chemotherapy as an earlier treatment option for tumors with a Ki-67 of higher than 10% after PRRT or somatostatin therapy; such tumors show higher 18F-FDG activity, reflecting their high proliferative capacity and aggressive behavior (30). Although the correlation between Ki-67 and prognostic information in NETs has been well proven, certain aspects of histologic staining, such as intratumoral heterogeneity, may rarely cause a false determination of grade, especially in the G2 category, in which the nearly flip-flop phenomenon of the dual tracers is more evident (31). Furthermore, the availability of new treatment regimens has emphasized the need for new prognostic and predictive biomarkers that can lead to better assessment of therapeutic response for individual patients (32). Tumor heterogeneity cannot be fully assessed by tumor biopsy, and this is an area in which combined dual-tracer PET/CT offers distinct advantages even though referring clinicians rely mainly on the histologic grading. In our population, there have been few patients with discordant findings between 68Ga-DOTATATE and 18F-FDG PET/CT studies, predominantly in the liver. Biopsy of the liver lesions in the same patients showed a mildly different Ki-67 value (>10% and <20%) for patients in the G2 category. In such cases, we considered as valid the higher Ki-67 value, taking into consideration the aggressiveness of metabolically active tumor.
The clinical impact of 68Ga-DOTANOC and 68Ga-DOTATATE has been well described previously. 68Ga-DOTA-peptide imaging has been shown to influence the management of more than half of patients, with a particular impact on initiation or continuation of PRRT or somatostatin analog medical therapy based on the demonstration of somatostatin receptor expression (24,33,34). Our results similarly show that 68Ga-DOTATATE affected the management plan in 48% of NET patients. Regarding 18F-FDG, Kayani et al., in a limited cohort, concluded that its use led to a change from PRRT to chemotherapy in 25% of patients with intermediate- or high-grade NETs (15). Our study demonstrated similar results, with 18F-FDG findings affecting 21% of patients, half of whom had G3 tumors (30).
Recent papers have investigated the value of 68Ga-DOTANOC SUVmax as a potential prognostic factor (35–37). We used a cutoff of 5% when relating Ki-67 to SUVmax based on the study of Panzuto et al. reporting that patients with a Ki-67 of more than 5% show more aggressive disease (37). Our data validated their findings, with significant differences in 68Ga-DOTATATE SUVmax according to whether the Ki-67 was above or below 5%. However, we found that there is a stronger association between aggressive tumor behavior and functional activity when a Ki-67 cutoff of 12 is implemented.
The study also showed that the SUVmax for 68Ga-DOTATATE is related to NET grade, another important prognostic marker. Interestingly, there was no relation between FDG SUVmax and grade. The only report with similar findings was by Sharma et al. in a limited population of NET patients with different primary sites (36). In their study, SUVmax for 68Ga-DOTANOC correlated with prognosis, whereas that for 18F-FDG did not. Several reports have indicated that 18F-FDG positivity is associated with a worse prognosis, although to our knowledge most of these studies did not specifically investigate the role of SUVmax (22,38). In our study, we found that metastases demonstrated by either tracer correlated with a shorter survival, with bone metastases correlating with the worst prognosis.
With regard to study limitations, the fact that only patients with histologically proven NETs were enrolled restricted the possibility of specificity measurement. A second limitation of the study is that it lacked histologic confirmation from two or more tumor sites in patients with discrepant findings between the two PET/CT tracers. However, it would be unethical and not feasible to have histologic confirmation of all the tumor-avid lesions.
CONCLUSION
18F-FDG PET/CT has no clinical impact on G1 NETs and a moderate impact on G2 NETs. In NETs with a Ki-67 index of 12% or less, use of 18F-FDG PET/CT should be limited and tailored to the individual patient. However, in poorly differentiated NETs, 18F-FDG PET/CT plays a significant clinical role in combination with 68Ga-DOTATATE. 68Ga-DOTATATE SUVmax is related to tumor grade, and Ki-67 and can be used prognostically.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 11, 2016.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 10, 2016.
- Accepted for publication June 30, 2016.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Castleman disease presenting as DOTATATE-positive retroperitoneal mass
- Dual Somatostatin Receptor/18F-FDG PET/CT Imaging in Patients with Well-Differentiated, Grade 2 and 3 Gastroenteropancreatic Neuroendocrine Tumors
- Prognostic Value of 18F-FDG PET/CT in a Large Cohort of Patients with Advanced Metastatic Neuroendocrine Neoplasms Treated with Peptide Receptor Radionuclide Therapy
- How I treat neuroendocrine tumours
- Phase I study of the 177Lu-DOTA0-Tyr3-Octreotate (lutathera) in combination with nivolumab in patients with neuroendocrine tumors of the lung
- Aetna and 68Ga-DOTATATE: A Sequel to "The Injustice of Being Judged by the Errors of Others" (1)
- Most of the Intended Management Changes After 68Ga-DOTATATE PET/CT Are Implemented
- Current Concepts in 68Ga-DOTATATE Imaging of Neuroendocrine Neoplasms: Interpretation, Biodistribution, Dosimetry, and Molecular Strategies