


Abstract
Radiolabeled somatostatin (sst) receptor agonists are integral to the diagnosis of gastroenteropancreatic neuroendocrine tumors (NETs), but detection rates, especially of liver metastases, remain limited even with PET/CT. 68Ga-OPS202 (68Ga-NODAGA-JR11; NODAGA = 1,4,7-triazacyclononane,1-glutaric acid-4,7-acetic acid and JR11 = Cpa-c(dCys-Aph(Hor)-dAph(Cbm)-Lys-Thr-Cys)-dTyr-NH2)), a novel radiolabeled sst receptor antagonist with a high affinity for the sst2 receptor, has the potential to perform better than sst receptor agonists. Here, we present the results of the phase II component of a phase I/II study that evaluated the sensitivity of 68Ga-OPS202, compared with the reference compound, 68Ga-DOTATOC (an sst receptor agonist), in PET imaging. Methods: Patients received a single 150-MBq intravenous injection of 68Ga-DOTATOC (15 μg of peptide) and 2 single 150-MBq intravenous injections of 68Ga-OPS202 (15 μg of peptide at visit 1 and 50 μg at visit 2). Whole-body PET/CT acquisitions were performed 1 h after injection on the same calibrated PET/CT scanner. Diagnostic efficacy measures were compared against contrast medium–enhanced CT or MRI as the gold standard. Two independent masked experts read the scans, and both outcomes were combined for analysis. Results: Twelve consecutive patients with low- or intermediate-grade gastroenteropancreatic NETs took part in this prospective study. Image contrast for matched malignant liver lesions was significantly higher for the 68Ga-OPS202 scans than for the 68Ga-DOTATOC scan: the median of the mean tumor-to-background SUVmax ratios were significantly higher for 15 and 50 μg of 68Ga-OPS202 (5.3 and 4.3, with interquartile ranges of 2.9–5.7 and 3.4–6.3 and P values of 0.004 and 0.008) than for 68Ga-DOTATOC (1.9, with an interquartile range of 1.4–2.9). The higher tumor-to-background ratio of 68Ga-OPS202 resulted not only in a higher detection rate of liver metastases but also in a significantly higher lesion-based overall sensitivity with the antagonist than with 68Ga-DOTATOC: 94% and 88% for 50 and 15 μg of 68Ga-OPS202, respectively, and 59% for 15 μg of 68Ga-DOTATOC (P < 0.001). Positive predictive values for 68Ga-OPS202 PET/CT and 68Ga-DOTATOC PET/CT were similar (∼98%). There were no significant differences in image contrast, sensitivity, or positive predictive values between the 2 68Ga-OPS202 peptide doses, indicating a high reproducibility. Conclusion: Preliminary diagnostic efficacy data from this phase II study indicate that 68Ga-OPS202 has high sensitivity for the detection of gastroenteropancreatic NETs. Further studies in larger patient populations are warranted.
See an invited perspective on this article on page 907.
Gastroenteropancreatic neuroendocrine tumors (NETs) are the most frequent neuroendocrine neoplasms, accounting for approximately two thirds of all neuroendocrine neoplasms.
Molecular imaging of NETs facilitates not only earlier diagnosis but often also detection of the primary tumor site, which is unknown in approximately 20%–30% of cases (1). Molecular imaging of NETs also aids in selection of the most appropriate therapy, thus improving outcomes (2). For many years, imaging with somatostatin (sst) receptor scintigraphy and SPECT has been central to the diagnostic work-up of patients with NETs (3). More recently, it has been shown that PET/CT scanning with 68Ga-labeled sst receptor agonists is superior to scanning with 111In- or 99mTc-labeled sst analogs (4). This difference reflects the greater sensitivity and spatial resolution of PET/CT, as well as the higher affinity of 68Ga radiopharmaceuticals for the sst subtype 2 (sst2) receptor (5,6). 68Ga production is also cost-effective, because portable 68Ge/68Ga generators are available, allowing access to radioisotopes without the need for an onsite cyclotron. Another advantage of PET/CT over SPECT/CT is that it better quantifies absolute tumor uptake. Although 68Ga-DOTATOC PET/CT has very high sensitivity versus conventional 111In-pentetreotide (OctreoScan; Mallinckrodt, Inc.), the detection rate of liver metastases and the overall sensitivity were lower for 68Ga-DOTATOC PET/CT than for hepatic-phase MRI in a lesion-based analysis (7,8). This lack of sensitivity is an issue when it comes to planning surgery and liver-directed therapies. Thus, there remains a clinical need for further improvement of sst receptor imaging in patients with NETs.
The introduction of 68Ga-labeled sst receptor antagonists has the potential to improve NET imaging, as more receptor binding sites are bound by sst receptor antagonists than by sst receptor agonists (9). The feasibility of using a radiolabeled antagonist (111In-DOTA-BASS) was demonstrated in patients with NETs (n = 4) or metastatic thyroid cancer (n = 1) (10). Indeed, compared with traditional 111In-pentetreotide scintigraphy, 111In-DOTA-BASS imaging was more sensitive. However, 111In-DOTA-BASS has a low affinity for the sst2 receptor, which is the most common sst receptor subtype expressed by NETs (11). Therefore, a series of radiolabeled sst receptor antagonists with higher affinity for the sst2 receptor was developed (12). Among them, we selected 68Ga-OPS202 (68Ga-NODAGA-JR11; NODAGA = 1,4,7-triazacyclononane,1-glutaric acid-4,7-acetic acid and JR11 = Cpa-c(dCys-Aph(Hor)-dAph(Cbm)-Lys-Thr-Cys)-dTyr-NH2)) as the radioligand of choice on the basis of its potential for imaging NETs (13). The corresponding therapeutic radiotracer, 177Lu-OPS201 (177Lu-DOTA-JR11), for a theranostic approach was associated with tumor doses that were 1.7- to 10.6-fold higher than those observed with the sst receptor agonist 177Lu-DOTATATE in 4 patients with metastasized NETs (14).
Our study of 68Ga-OPS202 in humans was designed to evaluate its safety, biodistribution, and dosimetry (phase I) and its preliminary diagnostic efficacy (phase II) in patients with gastroenteropancreatic NETs. The results of phase I of the study, which are summarized in an accompanying paper (15), show that there were no safety concerns with 68Ga-OPS202 and that the mean effective dose (±SD) was 3.6 ± 0.3 mSv/150 MBq. For the phase II component of the study, our hypothesis was that 68Ga-OPS202 would be a more sensitive agent than 68Ga-DOTATOC for diagnosis of gastroenteropancreatic NETs on PET/CT, with a high positive predictive value (PPV). The results presented in this article follow the Standards for Reporting Diagnostic Accuracy 2015 statement, which is shown in the supplemental material (supplemental materials are available at http://jnm.snmjournals.org).
MATERIALS AND METHODS
The methodology of the study (ClinicalTrials.gov identifier NCT02162446; EudraCT no. 2014-001881-88) is described in detail in the accompanying paper about phase I of the study (15). The institutional review board approved this study, and all subjects signed a written informed consent form in accordance with the Declaration of Helsinki.
Study Design and Patient Population
This was a prospective, open-label, microdosing phase I/II study. Consecutive patients with a histologically confirmed well-differentiated low- or intermediate-grade gastroenteropancreatic NET were included if they had positive results on a 68Ga-DOTATOC scan in the previous 6 mo. Patients were excluded if they had received NET-specific treatments between the 68Ga-DOTATOC scan and the start of the study, except for sst analogs, provided there was a sufficient washout period (28 d for long-acting somatostatin analogs and 2 d for short-acting somatostatin analogs). Potentially eligible patients were identified by the date of their last or planned 68Ga-DOTATOC scan in our clinic (between January and November 2014) and consultation of their medical records.
Synthesis and Radiolabeling
After elution from the 68Ge/68Ga generator, 68Ga was extracted using cation exchange. OPS202 and DOTATOC were labeled at 75°C and 95°C, respectively, within 400 s, followed by C18 solid-phase extraction to achieve purity of at least 95%. Greater detail can be found in the Materials and Methods section of the accompanying paper (15).
Imaging
The first administration of 68Ga-OPS202 (visit 1) was 15 μg/150 MBq ± 25% intravenously over no longer than 1 min (the actual mean administered amount of peptide was 14 ± 4 μg [range, 11–19 μg], and the actual mean administered activity was 161 ± 21 MBq [range, 125–189 MBq]). At 3–4 wk later, the patients received a second administration of 68Ga-OPS202 (visit 2). This second administration was 50 μg/150 MBq ± 25% (the actual mean administered amount of peptide was 50 ± 15 μg [range, 37–63 μg], and the actual mean administered activity was 172 ± 14 MBq [range, 141–192 MBq]). 68Ga-DOTATOC was administered up to 6 mo before 68Ga-OPS202 (15 ± 5 μg/161 ± 11 MBq). Except for diuretics, use of other medication on scan days was permitted.
Three-dimensional whole-body (head to subinguinal region) PET scans were obtained 1 h after injection of 68Ga-OPS202 and 68Ga-DOTATOC using the same PET/CT scanner for imaging with both tracers (Discovery STE; GE Healthcare). Calibration and quality assurance were performed according to the EARL (European Association of Nuclear Medicine Research Ltd.) procedure. Greater detail can be found in the Materials and Methods section of the accompanying paper (15).
At 3–9 mo after the end of the core trial, referring centers performed follow-up imaging using either contrast-enhanced triple-phase multidetector CT or 1.5- or 3-T MRI with a dedicated body array coil for signal reception. The pulse sequence requirements for MRI comprised, minimally, axial and coronal T2-weighted sequences and axial multiphasic T1-weighted gradient-echo sequences before and after administration of a gadolinium-based contrast agent. Additional, optional, pulse sequences included diffusion-weighted imaging and delayed T1-weighted imaging if a hepatobiliary contrast agent was used.
Image Analysis
Both 68Ga-OPS202 scans (15 and 50 μg) and the 68Ga-DOTATOC scan were reviewed by 2 independent, qualified readers, one of whom was on-site (a board-certified nuclear medicine physician from University Hospital Basel) and the other central (a board-certified radiologist and nuclear medicine physician). Both were masked to the patient, radiopharmaceutical, and peptide dose. A sequential locked-read methodology was used for image interpretation; that is, once scans had been reviewed and completed, readers were not permitted to reread them and modify their opinion. As an image-reading tool, Mint Lesion (Mint Medical GmbH), was used by both readers.
The diagnostic efficacy measure was the absolute number of malignant lesions detected. Two additional measures were part of an exploratory extension and not part of the original design: SUVmax for tumors and reference tissues, and mean tumor-to-background uptake ratio (SUVmax of tumor to SUVmax of reference tissue). The reference tissues were muscle, liver, and lymph nodes, as well as normal tissue near a suspected focus of uptake. For each of these measures, the results for the 68Ga-OPS202 PET/CT scans (15 and 50 μg) were compared with, as a reference, the results for the 68Ga-DOTATOC PET/CT scan, which is an accepted state-of-the-art imaging modality for gastroenteropancreatic NETs worldwide. SUVmax and tumor-to-background ratio were analyzed for matched lesions only (i.e., only lesions that were present not only on the 68Ga-DOTATOC scan but also on both 68Ga-OPS202 scans). In addition, the 68Ga-OPS202 scan at visit 1 was compared with the 68Ga-OPS202 scan at visit 2 to evaluate the reproducibility of tumor uptake, image contrast (tumor-to-background ratios), and sensitivity measurements.
Sensitivity and PPV
For sensitivity and PPV analyses, the scans for both 68Ga-OPS202 doses and for 68Ga-DOTATOC were compared with up to 9 mo of clinical and imaging follow-up after the end of the core trial by the central reader. As a standard of reference, multiple-phase abdominal CT, contrast-enhanced MRI of the liver, or, in one case, biopsy was used for comparison. Sensitivity and PPV analyses were part of an exploratory extension and not part of the original study design.
Statistical Analysis
It was planned to recruit 12 patients for this phase I/II study. This number was considered appropriate for an exploratory study and sufficient to address the study aim.
The nonparametric Wilcoxon signed-rank test was used to compare number of identified lesions, SUVmax for lesions and reference tissues, and tumor-to-background ratio between the reference 68Ga-DOTATOC scan and the visit 1 and 2 68Ga-OPS202 scans. Matched data from the on-site reader were used for the quantitative analysis of SUVs (median of the mean).
For the lesion-based sensitivity and PPV analyses, the outcomes from the on-site and central readers were considered to fit a mixed-effects logistic regression model. For exposure variables, it was assumed that the scan method was a fixed effect and the patient and reader were random effects. Three tests of superiority were performed, 68Ga-DOTATOC versus 15-μg 68Ga-OPS202, 68Ga-DOTATOC versus 50-μg 68Ga-OPS202, and 15-μg 68Ga-OPS202 versus 50-μg 68Ga-OPS202. To assess whether the results were robust, the outcomes of only the on-site reader were compared with the outcomes of both readers. Statistical testing was exploratory. The level of significance was set at 5%, and tests were 2-sided. Indeterminate and missing values were not replaced.
RESULTS
Patients
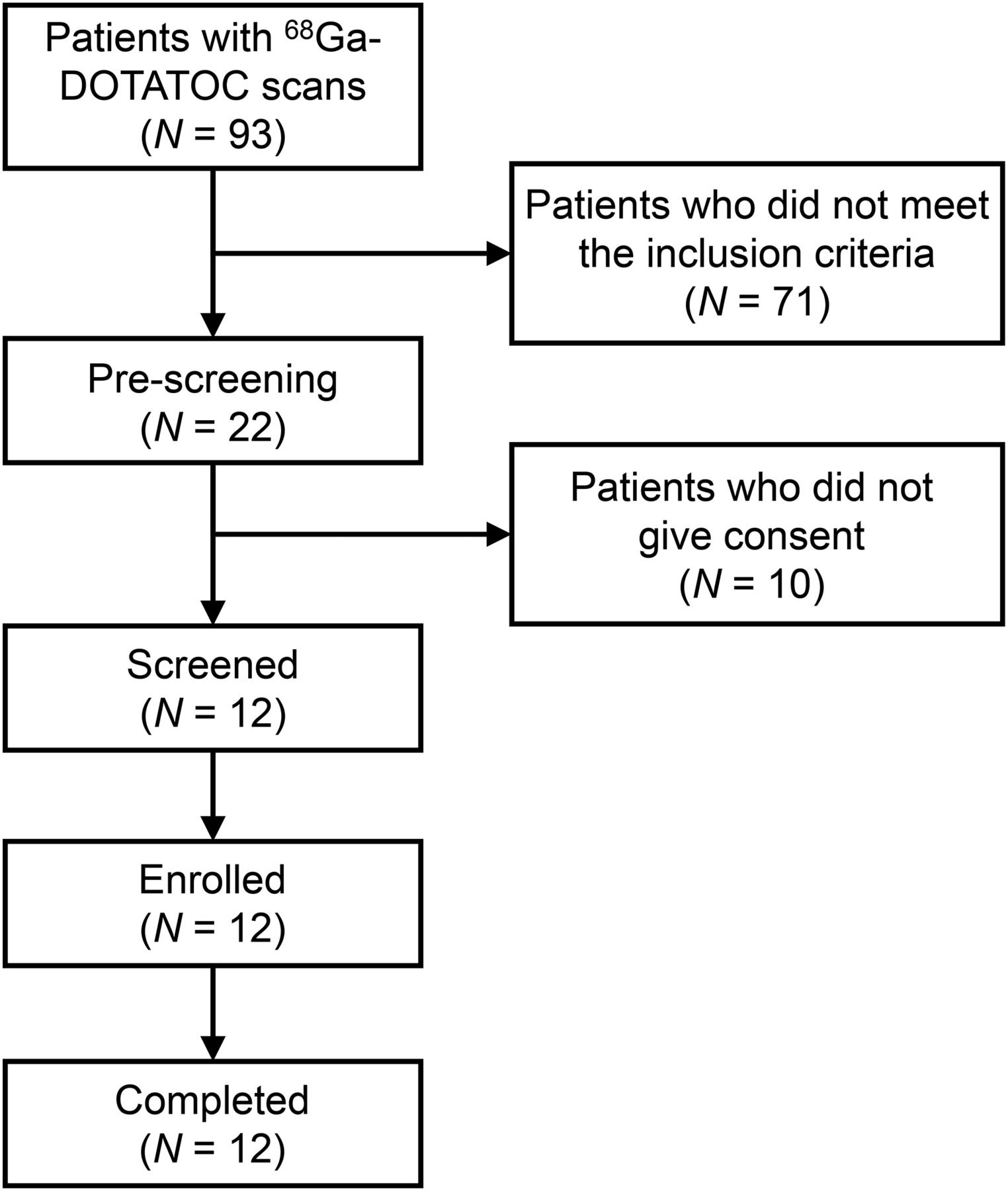
The study profile is given in Figure 1. Of the 12 patients screened, all 12 were enrolled; completed the phase I dosimetry, pharmacokinetic, and safety evaluation; and were included in this phase II diagnostic efficacy evaluation. Baseline demography and disease characteristics are summarized in Table 1. The median time between the 68Ga-DOTATOC scan and the first 68Ga-OPS202 scan (visit 1, 15 μg) was 34 d (interquartile range, 27.5–135 d). One patient underwent the 68Ga-DOTATOC scan 16 d after visit 1. Both the 68Ga-OPS202 and the 68Ga-DOTATOC scans revealed disease in 11 of 12 patients. Follow-up imaging confirmed that patient 11 was in complete remission. Patients did not receive any treatments between the 68Ga-DOTATOC and the 68Ga-OPS202 scans. Eleven adverse effects were reported in 6 patients after injection of 68Ga-OPS202, but none were severe, serious, or fatal. More information can be found in the accompanying paper (15).

Study profile.
Baseline Demography and Disease Characteristics
68Ga-OPS202 Versus 68Ga-DOTATOC
The total number of malignant lesions and liver lesions was significantly greater with 68Ga-OPS202 than with 68Ga-DOTATOC (Table 2). The scans did not significantly differ in the number of malignant lymph nodes found. Because only a few patients had lesions in other organs or tissues, statistical comparisons were not feasible.
Lesion-Based Comparison of 68Ga-OPS202 PET/CT Scans and 68Ga-DOTATOC PET/CT Scan
Image contrast (tumor-to-background ratio) for matched malignant liver lesions was significantly higher with 68Ga-OPS202 than with 68Ga-DOTATOC (Fig. 2; Table 3), mainly because of the significantly lower SUVmax of liver background (Figs. 3 and 4) in the 68Ga-OPS202 scans (Table 3). For matched malignant lymph nodes, there were no significant differences in the median of the mean tumor-to-background ratio between the 68Ga-OPS202 scans and the 68Ga-DOTATOC scan, regardless of the reference tissue.
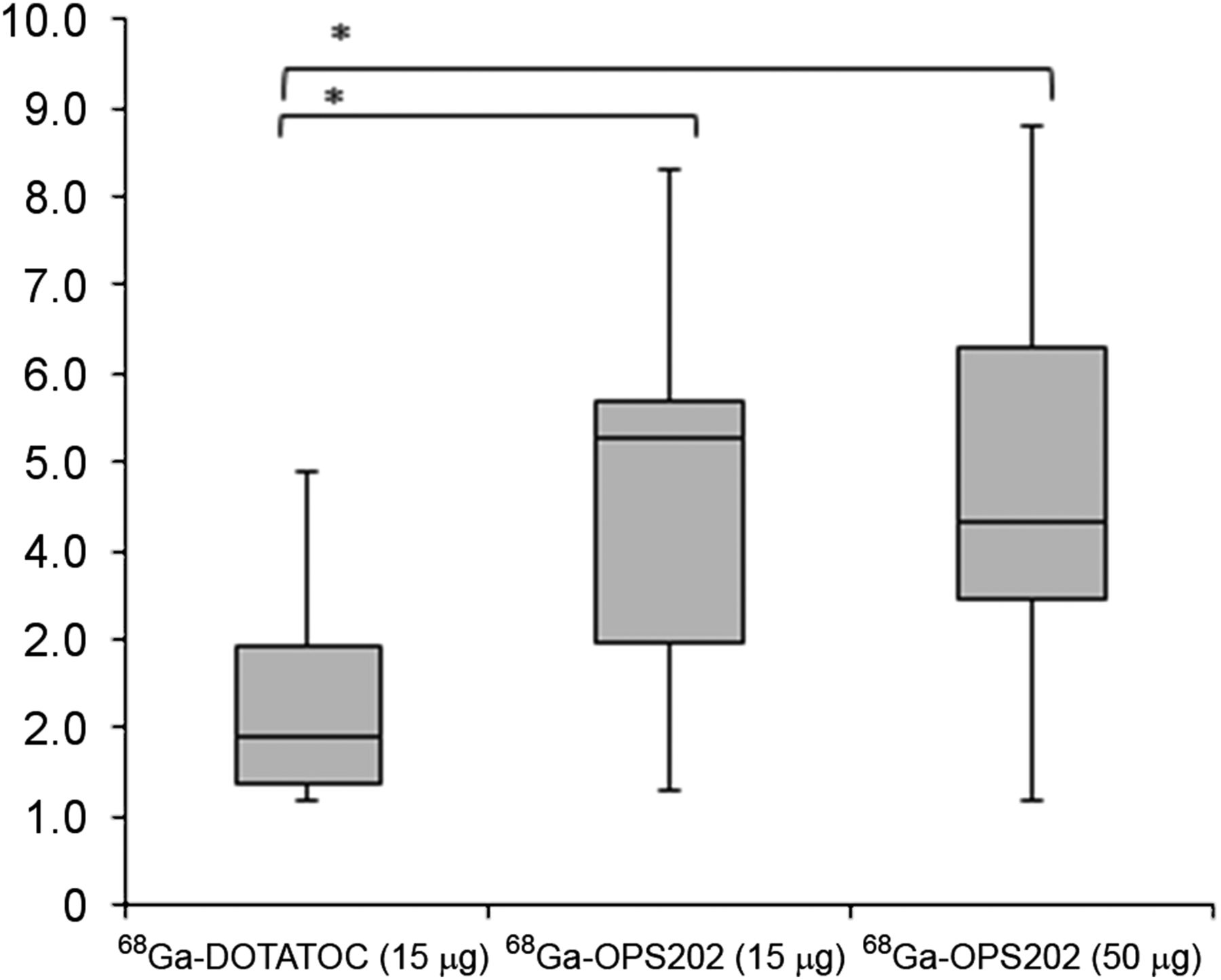
Box-and-whiskers plot representing tumor-to-background ratios of matched liver lesions (median of mean SUVmax ratios, first and third quartiles) for both 68Ga-OPS202 scans vs. the 68Ga-DOTATOC scan (on-site reader). Data in this figure were acquired as part of extension study and are not part of original study. *In comparison with 68Ga-DOTATOC, both 68Ga-OPS202 scans showed significant increase in tumor-to-liver ratio (P = 0.004 and 0.008), whereas no statistical difference was shown between the 2 OPS202 peptide amounts (P = 0.547).
Organ, Tumor, and Tumor-to-Background Uptake Ratios: 68Ga-OPS202 PET/CT Versus 68Ga-DOTATOC PET/CT in Matched Lesion Analysis by On-Site Reader
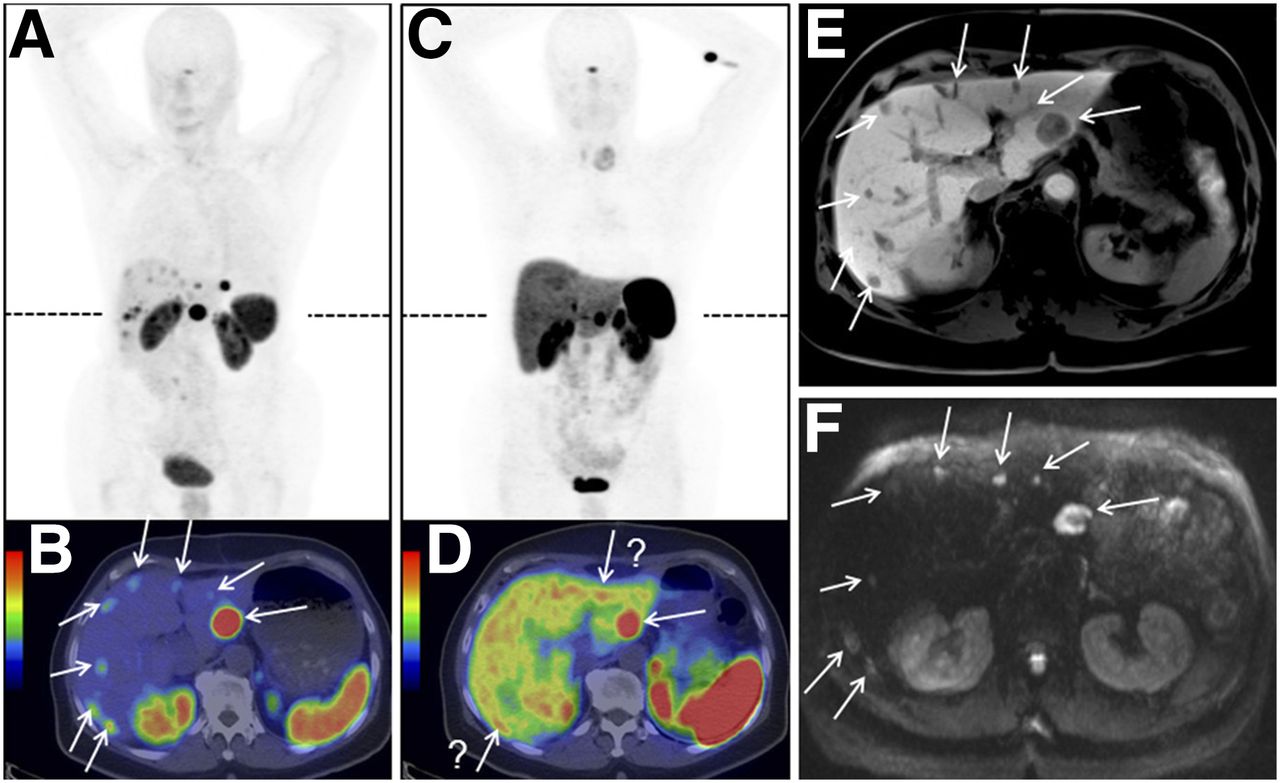
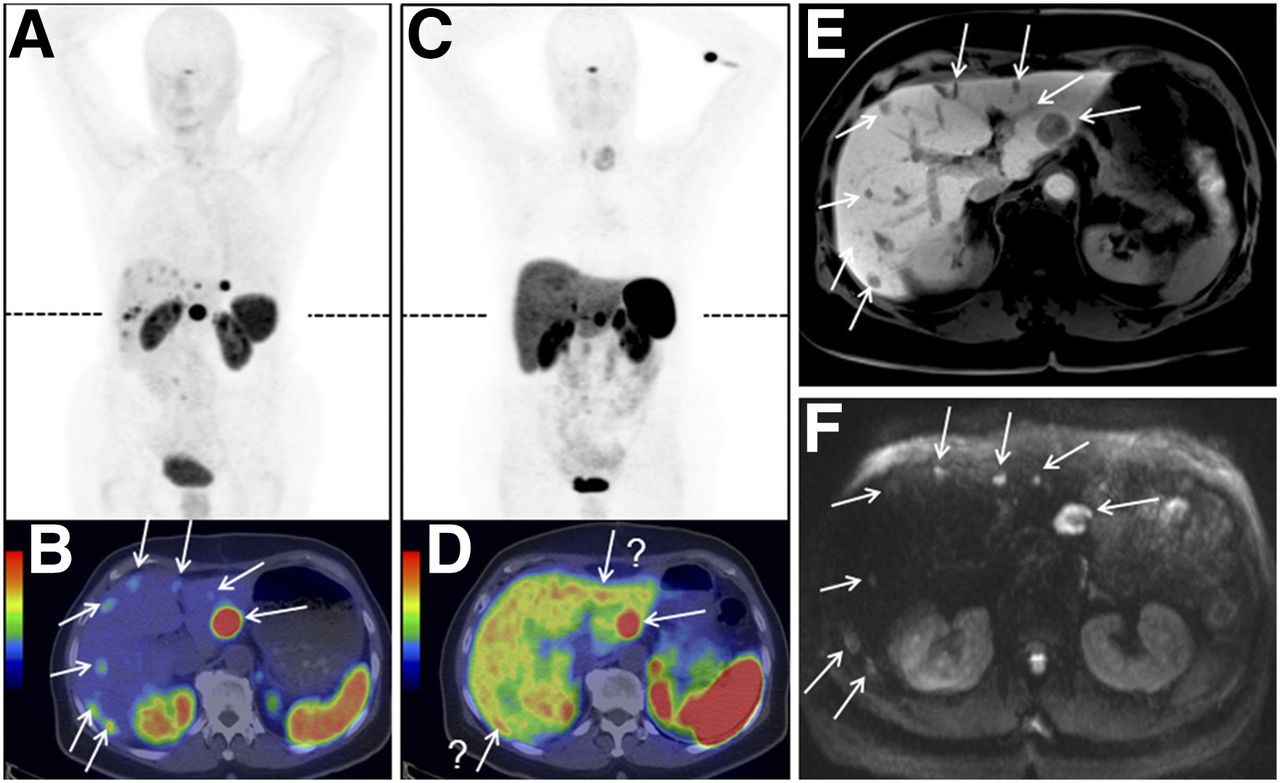
Images of patient 9, with ileal NET, showing bilobar liver metastases: 68Ga-OPS202 PET/CT (50 μg) (A and B), 68Ga-DOTATOC PET/CT (C and D), and MRI (E and F). Dashed lines in A and C show level of transaxial slices in B, D, E, and F. PET/CT studies were performed on same scanner within 2 mo of each other and were read using same gray scale (maximal-intensity projections, A and C) and color scale (transaxial fusion images, B and D). Findings were correlated with liver MRI performed 4 mo after 68Ga-OPS202 PET/CT, with delayed postcontrast acquisitions (E) and diffusion-weighted images (F) confirming additional metastases missed or questionable (arrow with question mark) on 68Ga-DOTATOC PET/CT. Importantly, background activity was lower in liver, intestine, and thyroid with 68Ga-OPS202 than with 68Ga-DOTATOC (e.g., for liver, mean SUVmax was 2.6 vs. 10.2). Repeated thyroidectomy for benign goiter failed to demonstrate malignancy of left thyroid nodule.

Images of patient 10, with ileal NET: 68Ga-OPS202 PET/CT (50 μg) (A and B), 68Ga-OPS202 PET/CT (15 μg) (C and D), 68Ga-DOTATOC PET/CT (15 μg) (E and F), and MRI (G and H). Dashed lines in A, C, and E show level of transaxial slices in B, D, F, G, and H. 68Ga-OPS202 scans were obtained 25 and 4 d after 68Ga-DOTATOC scan. Mean liver SUVmax was 4.6 and 4.7 for 15 and 50 μg of 68Ga-OPS202, respectively, and 5.6 for 68Ga-DOTATOC. Although 68Ga-DOTATOC and both 68Ga-OPS202 scans showed ileal primary, mesenteric malignant mass, and multiple liver metastases (black arrows), 68Ga-OPS202 scans detected significantly more liver metastases (white arrows). Head-to-head comparison with MRI performed 7 mo after 68Ga-OPS202 PET/CT confirmed that suggestive findings were true-positive only on 68Ga-OPS202 PET/CT (white arrows).
Sensitivity and PPV
Outcome analyses for both readers revealed a significantly higher lesion-based sensitivity for both 15 and 50 μg of 68Ga-OPS202 than for 68Ga-DOTATOC (P < 0.001 for both) (Table 4; Figs. 3 and 4). There was also a significant difference in sensitivity between 15 μg and 50 μg of 68Ga-OPS202 (P < 0.05), but this significance was not confirmed in the assessment of robustness (P = 0.76)—that is, if the analysis were done using on-site readings only. The PPVs for all 3 tested PET tracers were around 98%.
Lesion-Based Comparison of Sensitivity and PPV for 68Ga-OPS202 PET/CT and 68Ga-DOTATOC PET/CT in On-Site and Central Readings
DISCUSSION
To our knowledge, this was the first study to evaluate the diagnostic efficacy of a radiolabeled sst receptor antagonist, 68Ga-OPS202, for PET/CT imaging of gastroenteropancreatic NETs. Of key importance are the results compared with the reference sst receptor agonist PET/CT scan, which was conducted using 68Ga-DOTATOC. Multiple-phase CT of the abdomen and contrast-enhanced MRI of the liver were performed during follow-up. These are the most accurate methods for establishing the presence or absence of neuroendocrine liver metastases (3) and were chosen as the standards of reference. They show that 68Ga-OPS202 is more sensitive than 68Ga-DOTATOC (88%–94% vs. 59%), mainly because of a higher detection rate of metastases in the liver, the predominant site of metastasis in patients with gastroenteropancreatic NETs (16). This higher detection of liver metastases reflects the significantly lower uptake of 68Ga-OPS202 than of 68Ga-DOTATOC into normal liver tissue and therefore the higher image contrast. Sensitive detection of liver metastases is likely to have an impact on patient management, as the presence and extent of liver metastases are the most important prognostic factor (17). Unlike liver metastases, malignant lymph node lesions were not detected at a higher rate by 68Ga-OPS202 imaging, possibly because of the much smaller sample size for those lesions than of liver lesions.
Uptake into the normal pancreas and gastrointestinal tract was lower with 68Ga-OPS202 than with 68Ga-DOTATOC, leading to increased tumor-to-background ratios for the former and therefore suggesting that it may be more useful for detecting primary gastroenteropancreatic NETs. This ability, in turn, could have a positive impact on clinical management, because currently, the site of the primary tumor is unknown in approximately 20% of cases (1). Further studies are required to evaluate this aspect of diagnostic efficacy for 68Ga-OPS202 PET/CT; it was not possible in the current study because of the small patient population and therefore the low overall numbers of primary lesions.
68Ga-OPS202 is an antagonist with high affinity for the sst2 receptor (12) and shows more sst receptor binding sites than the agonists 68Ga-DOTATATE and 68Ga-DOTATOC (data not shown). Preclinical imaging studies comparing radiolabeled JR11 conjugates and 68Ga-DOTATATE (12) have shown that tumor uptake can be expected to be higher for 68Ga-OPS202 than for 68Ga-DOTATOC. In our clinical study, this was not the case. This unexpected finding might be explained by the short half-life of 68Ga (68 min), which does not allow scans to be acquired at later time points. Posttreatment scans with the therapeutic sister compound of 68Ga-OPS202—177Lu-OPS201 (177Lu-DOTA-JR11)—showed the highest tumor uptake between 3 and 24 h after injection of the radiotracer (Supplemental Fig. 1) (14). The sst receptor agonist 177Lu-DOTATATE showed a different behavior, with the highest tumor uptake at around 1 h after injection of the radiotracer (Supplemental Fig. 1).
Besides 68Ga-DOTATOC, there are other 68Ga-labeled sst receptor agonists for PET/CT imaging: 68Ga-DOTATATE and 68Ga-DOTANOC. Like 68Ga-OPS202, 68Ga-DOTATATE is an sst2 receptor–specific tracer, whereas 68Ga-DOTANOC targets the sst2, sst3, and sst5 receptor subtypes (18). The most commonly expressed sst receptor subtypes on gastroenteropancreatic NETs are sst2 and, to a lesser extent, sst1 and sst5 (11). The clinical use of 68Ga-DOTATATE and 68Ga-DOTANOC was compared in a crossover study on 18 patients with gastroenteropancreatic NETs (18). Uptake values (median SUVmax) for 68Ga-DOTATATE and 68Ga-DOTANOC in liver tumors were similar to those obtained for 68Ga-OPS202 in the current study, whereas uptake values for 68Ga-OPS202 in normal liver were lower, resulting in much better tumor-to-background ratios; the medians of the mean tumor-to-background ratios were 2.0 for about 30 μg of 68Ga-DOTATATE and 2.7 for about 30 μg of 68Ga-DOTANOC in that study (18), compared with 5.3 for 15 μg of 68Ga-OPS202, 4.3 for 50 μg of 68Ga-OPS202, and 1.9 for about 15 μg of 68Ga-DOTATOC in the present study. Although indirect comparisons with studies using other 68Ga-labeled sst analogs should be interpreted with caution, higher hepatic background levels have been consistently reported in the literature for 68Ga-labeled sst receptor agonists, compared with 68Ga-OPS202. In a study by Wild et al. (18), median SUVmax in the normal liver with approximately 30 μg of 68Ga-DOTATATE and approximately 30 μg of 68Ga-DOTANOC was 7.5 (interquartile range, 5.6–9.8) and 5.1 (interquartile range, 4.1–5.8), whereas in the current study, corresponding values with 15 μg of 68Ga-DOTATOC, 15 μg of 68Ga-OPS202, and 50 μg of 68Ga-OPS202 were 6.5, 3.4, and 2.7, with respective interquartile ranges of 4.8–8.9, 2.7–3.6, and 2.5–3.1. This is consistent with a study by Poeppel et al. (19), which compared 68Ga-DOTATATE and 68Ga-DOTATOC with a mean peptide amount of 6 μg (range, 2–13 μg) and failed to show any major difference between them. These findings add weight to our conclusion that, compared with sst receptor agonists, 68Ga-OPS202 has improved imaging contrast for liver metastases.
The results obtained for the 2 doses of the peptide component of 68Ga-OPS202 were generally consistent. There were no significant differences in the numbers of malignant liver or lymph node lesions detected per patient, the tumor or reference-tissue uptake values, or the tumor contrast values, indicating a high reproducibility for 68Ga-OPS202 PET/CT, which might be relevant for treatment-response evaluation and follow-up imaging. There were no safety issues identified with either dose (15), although the 3 adverse events (all grade 1) assessed as possibly related to the study drug were reported in 2 patients examined with the higher dose (50 μg). Because of the radioactive decay of 68Ge/68Ga generators, it is not practical to keep the ratio of radioactivity to mass dose constant (specific activity), but the results of the current study indicate that OPS202 doses of between 15 and 50 μg are efficient and well tolerated and provide high reproducibility.
One of the limitations of the study was the small patient population. A small number of patients is typical of early phase II studies. Although this affects the power of statistical comparisons, it does allow evaluation of general trends and provides important information for future studies. A notable point is that 3 of the 12 patients included in the study had more than 30 lesions. To avoid any possible bias, the number of lesions per patient was considered in the statistical analysis.
CONCLUSION
The preliminary diagnostic efficacy data from this phase II evaluation indicate that 68Ga-OPS202 has high sensitivity and reproducibility in the detection of gastroenteropancreatic NETs. These results, together with the safety profile from the phase I evaluation, suggest that 68Ga-OPS202 might be a valuable new radiopharmaceutical for staging, localization, treatment-response evaluation, and follow-up imaging of NETs. Further studies on larger patient populations are warranted.
DISCLOSURE
Hakim Bouterfa is a founder of OctreoPharm Sciences GmbH and a former employee of Ipsen; he now acts as a consultant for Ipsen. Jens Kaufmann is an employee of Ipsen. Medical writing support was funded by Ipsen. This study was sponsored in part by Ipsen. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank all the patients who participated in the trial, the OctreoPharm/Ipsen team, and the personnel of the Division of Radiopharmaceutical Chemistry and Nuclear Medicine at University Hospital Basel. We also thank Nicky French (Watermeadow Medical) for medical writing support.
Footnotes
Published online Nov. 30, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 25, 2017.
- Accepted for publication November 3, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- SSTR Antagonists as Theranostic Option in Merkel Cell Carcinoma
- 68Ga-SSO-120 PET for Initial Staging of Small Cell Lung Cancer Patients: A Single-Center Retrospective Study
- Head-to-Head Comparison of 68Ga-NODAGA-JR11 and 68Ga-DOTATATE PET/CT in Patients with Metastatic, Well-Differentiated Neuroendocrine Tumors: Interim Analysis of a Prospective Bicenter Study
- 18F-Labeled Somatostatin Analogs as PET Tracers for the Somatostatin Receptor: Ready for Clinical Use
- 18F-Labeled Somatostatin Analogs as PET Tracers for the Somatostatin Receptor: Ready for Clinical Use
- The Emergence of Somatostatin Antagonist-Based Theranostics: Paving the Road Toward Another Success?
- A Randomized, Factorial Phase II Study to Determine the Optimal Dosing Regimen for 68Ga-Satoreotide Trizoxetan as an Imaging Agent in Patients with Gastroenteropancreatic Neuroendocrine Tumors
- First-in-Humans Study of the SSTR Antagonist 177Lu-DOTA-LM3 for Peptide Receptor Radionuclide Therapy in Patients with Metastatic Neuroendocrine Neoplasms: Dosimetry, Safety, and Efficacy
- Somatostatin Receptor Imaging and Theranostics: Current Practice and Future Prospects
- A Prospective, Randomized, Double-Blind Study to Evaluate the Safety, Biodistribution, and Dosimetry of 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 in Patients with Well-Differentiated Neuroendocrine Tumors
- 177Lu-DOTA-EB-TATE, a Radiolabeled Analogue of Somatostatin Receptor Type 2, for the Imaging and Treatment of Thyroid Cancer
- Head-to-Head Comparison of 68Ga-DOTA-JR11 and 68Ga-DOTATATE PET/CT in Patients with Metastatic, Well-Differentiated Neuroendocrine Tumors: A Prospective Study
- Phase I Trial of Well-Differentiated Neuroendocrine Tumors (NETs) with Radiolabeled Somatostatin Antagonist 177Lu-Satoreotide Tetraxetan
- Future of Theranostics: An Outlook on Precision Oncology in Nuclear Medicine
- New Developments in Peptide Receptor Radionuclide Therapy
- Somatostatin Receptor Imaging of Neuroendocrine Tumors: From Agonists to Antagonists
- Safety, Biodistribution, and Radiation Dosimetry of 68Ga-OPS202 in Patients with Gastroenteropancreatic Neuroendocrine Tumors: A Prospective Phase I Imaging Study