


Abstract
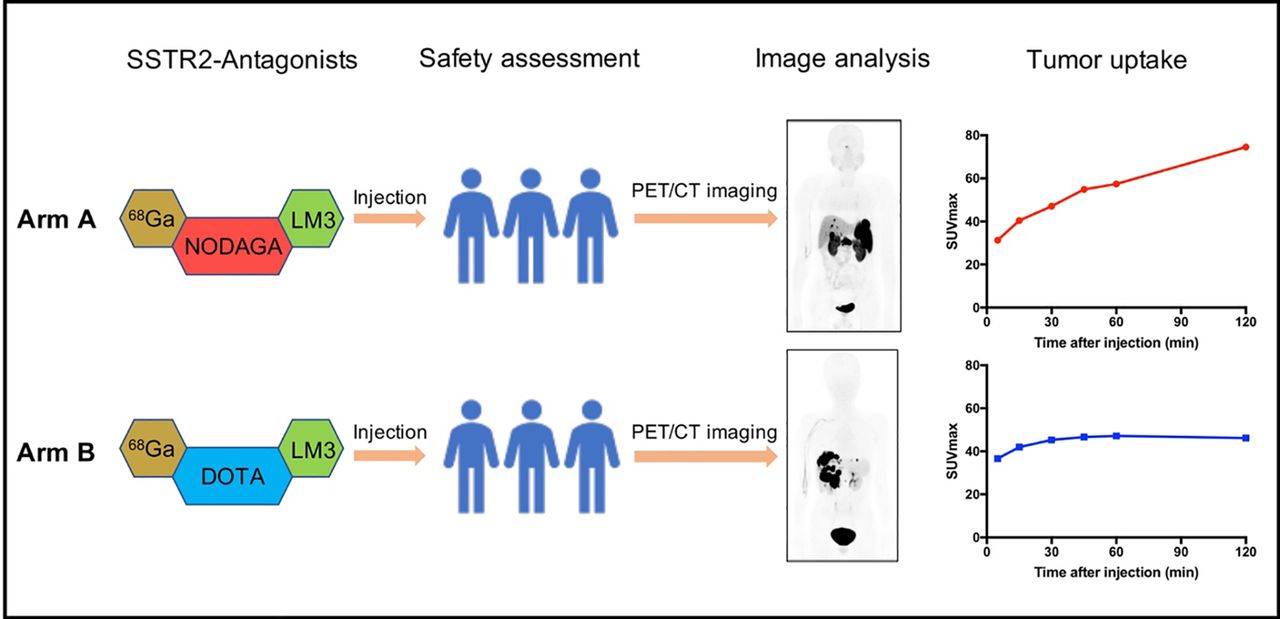
68Ga-NODAGA-LM3 (where LM3 is p-Cl-Phe-cyclo(d-Cys-Tyr-d-4-amino-Phe(carbamoyl)-Lys-Thr-Cys)d-Tyr-NH2) and 68Ga-DOTA-LM3 are somatostatin receptor subtype 2 (SSTR2)–specific antagonists used for PET/CT imaging. The purpose of this study was to evaluate the safety, biodistribution, and dosimetry of 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 in patients with well-differentiated neuroendocrine tumors. Methods: Patients were equally randomized into 2 arms, with arm A receiving 68Ga-NODAGA-LM3 and arm B receiving 68Ga-DOTA-LM3. Serial PET scans were acquired at 5, 15, 30, 45, 60, and 120 min after 68Ga-NODAGA-LM3 (200 MBq ± 11 MBq/40 μg of total peptide mass) or 68Ga-DOTA-LM3 (172 MBq ± 21 MBq/40 μg of total peptide mass) injection. The biodistribution in normal organs, tumor uptake, and safety were assessed. Radiation dosimetry was calculated using OLINDA/EXM (version 1.0). Results: Sixteen patients, 8 in each arm, were recruited in the study. Both tracers were well tolerated in most patients. Two patients in arm B had nausea (grade 2), and one of them had vomiting (grade 1). The PET images of the other 14 patients were further analyzed. Significantly lower organ uptake was observed in the pituitary, parotids, liver, spleen, pancreas, adrenal, stomach, small intestine, and kidneys with 68Ga-DOTA-LM3 than with 68Ga-NODAGA-LM3. In total, 38 lesions were analyzed, including 18 with 68Ga-NODAGA-LM3 and 20 with 68Ga-DOTA-LM3. Both tracers showed good tumor uptake and retention. With 68Ga-NODAGA-LM3, the tracer accumulation in tumor lesions increased by 138%, from an average SUVmax of 31.3 ± 19.7 at 5 min to 74.6 ± 56.3 at 2 h. With 68Ga-DOTA-LM3, the tumor uptake rapidly reached a high level at 5 min after injection, with an average SUVmax of 36.6 ± 23.6, and continued to increase to 45.3 ± 29.3 until 30 min after injection. The urinary bladder wall was the organ receiving the highest absorbed dose in both arms. The mean effective dose was 0.026 ± 0.003 mSv/MBq for 68Ga-NODAGA-LM3 and 0.025 ± 0.002 mSv/MBq for 68Ga-DOTA-LM3. Conclusion: Both 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 show favorable biodistribution, high tumor uptake, and good tumor retention, resulting in high image contrast. The dosimetric data are comparable to those for other 68Ga-labeled SSTR2 antagonists. Further studies are required to look into the potential antagonistic effects of 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3.
Neuroendocrine tumors (NETs) are a family of heterogeneous tumors featured by overexpression of somatostatin receptor (SSTR), especially SSTR subtype 2 (SSTR2), which could be a target for molecular imaging and radionuclide therapy. The role of radiolabeled somatostatin analogs such as TOC, TATE, and NOC in staging and restaging of NETs has been widely discussed (1). All these agents are SSTR agonists, which will be internalized into tumor cells after ligand–receptor interaction (2).
SSTR antagonists have emerged as another type of somatostatin analog, characterized by a low internalization rate and high tumor affinity (3–7). They bind to significantly more receptor sites than do agonists (4). Previous clinical studies have demonstrated higher sensitivity and better image contrast for 68Ga-NODAGA-JR11 than for 68Ga-DOTATOC (8). Data from our group suggested that 68Ga-DOTA-JR11 has better performance than 68Ga-DOTATATE in the detection of liver metastases (9). Nevertheless, 68Ga-DOTA-JR11 showed an overall lower tumor uptake than 68Ga-DOTATATE.
p-Cl-Phe-cyclo(d-Cys-Tyr-d-4-amino-Phe(carbamoyl)-Lys-Thr-Cys)d-Tyr-NH2 (LM3) is a novel SSTR antagonist developed by Fani et al. (10). It was coupled with different chelators (NODAGA, DOTA, and 1,4,8,11-tetraazabicyclo[6.6.2]hexadecane-4,11-diacetic acid) and radiometals (68Ga, 64Cu, and 177Lu). In vitro studies have shown 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 to have high SSTR2 affinities, with a 50% inhibitory concentration of 1.3 and 12.5 nmol/L, respectively (10). In animal models, both tracers showed good image contrast at 1 h after injection, and this contrast can be blocked by cold peptides. Zhang et al. reported a case with 68Ga-DOTATOC–negative high-grade liver metastases (11, 12). The patient was successfully imaged with 68Ga-NODAGA-LM3 PET/CT and subsequently treated with 177Lu-DOTA-LM3. Nearly complete remission was achieved after 3 cycles of intraarterial peptide receptor radionuclide therapy.
Given the promising preclinical results and preliminary clinical data, we designed this prospective, randomized, double-blind study to evaluate the safety, biodistribution, dosimetry (phase I), and diagnostic efficacy (phase II) of 68Ga-labeled LM3 in patients with well-differentiated NETs. Both 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 were investigated in this study, which was designed to have 2 parallel arms (arm A receiving 68Ga-NODAGA-LM3 and arm B receiving 68Ga-DOTA-LM3). The results of phase I are presented and discussed in this paper.
MATERIALS AND METHODS
Study Design
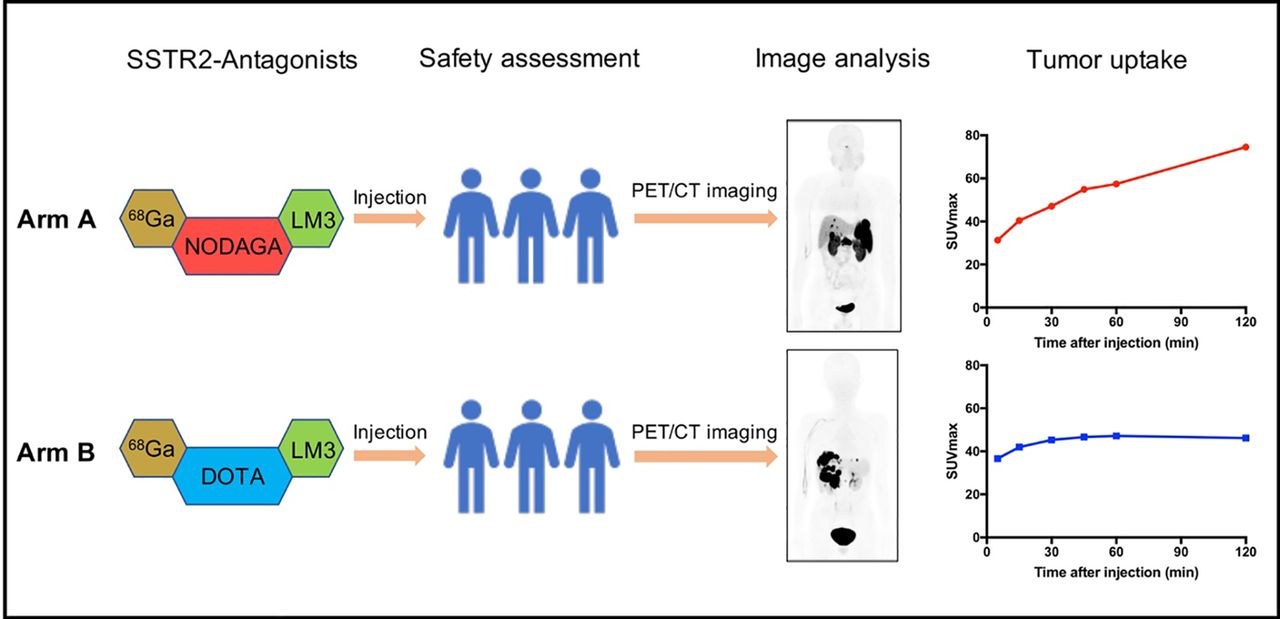
This study had a prospective, 2-armed, randomized, double-blind, phase I/II, single-center design (ClinicalTrials.gov identifier NCT04318561). It was approved by the institutional review board of Peking Union Medical College Hospital, and all patients gave written informed consent before study participation. The inclusion and exclusion criteria can be found in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org). The primary objectives of the phase I study were to determine the safety, biodistribution, and dosimetry of 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3. Sixteen patients with well-differentiated NETs were prospectively and consecutively recruited in this study (Fig. 1). The patients were equally randomized into 2 arms, and they were unaware of their arm.
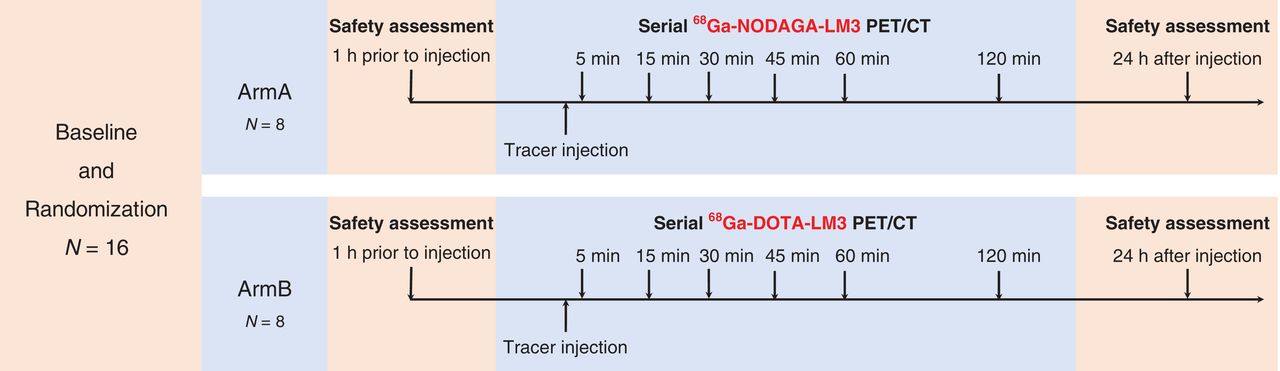
Diagram of study design. Sixteen patients were prospectively recruited in this study and equally randomized into 2 arms. In arm A, 8 patients underwent serial PET/CT scans at 5, 15, 30, 45, 60, and 120 min after 68Ga-NODAGA-LM3 injection. In arm B, 8 patients (anticipated) underwent serial PET/CT scans at 5, 15, 30, 45, 60, and 120 min after 68Ga-DOTA-LM3 injection. Two patients from arm B withdrew from study because of AEs.
Synthesis and Radiolabeling
Good-manufacturing-process–grade precursors, NODAGA-LM3 and DOTA-LM3, were supplied by CS Bio Co. The radiolabeling procedure was performed manually in a hot cell. Briefly, 68Ga was eluted from a 68Ge/68Ga generator (Eckert & Ziegler) using 5 mL of 0.1 M hydrochloric acid directly into a reaction vial containing 40 μg of precursor dissolved in sodium acetate buffer, for a final reaction mixture pH of 4. The mixture was heated to 100°C for 10 min to allow for radionuclide incorporation. After cooling to room temperature, the reaction mixture was diluted with 5 mL of water and then loaded onto an Oasis HLB light cartridge (preconditioned with 5 mL of ethanol and 5 mL of water) and washed with normal saline to remove unincorporated radionuclide. Finally, the product was eluted off the cartridge with 0.5 mL of 75% ethanol solution followed by 5 mL of normal saline through a Millipore filter (0.22 μm, 25 mm) into a sterile product vial. The radiochemical purity was more than 95%. The final product comprised 150–200 MBq of radiopharmaceutical, approximately 0.38 mL of ethanol, and approximately 40 μg of total peptide mass.
PET/CT Imaging
The study was performed on a time-of-flight PET/CT scanner (Polestar m660; SinoUnion Health Care Inc.). The patients received 68Ga-NODAGA-LM3 (200 MBq ± 11 MBq) or 68Ga-DOTA-LM3 (172 MBq ± 21 MBq) intravenously by a quick bolus injection (5 mL over 15 s). A low-dose CT scan (120 keV; 100 mAs; pitch, 1.3; 2.5-mm slice thickness; 0.5-s rotation time) from head to proximate thigh was obtained for anatomic localization and attenuation correction. Serial PET scans were acquired at 5, 15, 30, 45, 60, and 120 min after injection. The patients were required to lie still on the exam table during the first hour. Images were reconstructed using an ordered-subsets expectation maximization algorithm (2 iterations, 10 subsets, 192 × 192 matrix) and corrected for CT-based attenuation, dead time, random events, and scatter.
Safety Assessment
Heart rate, blood pressure, pulse oximetry, and 3-lead electrocardiography were recorded within 1 h before and at 24 h after LM3 injection. Clinical symptoms were monitored and graded according to the Common Terminology Criteria for Adverse Events (version 4.03).
Image Analysis
The 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 PET/CT images were anonymized and reviewed by an experienced nuclear medicine expert, masked to the medical history of the patients, on MIM software (MIM Software Inc.).
The physiologic uptake was evaluated in the following organs at all time points: pituitary gland, parotids, thyroids, lungs, blood pool, liver, spleen, pancreas (uncinate process), stomach, small intestine, kidneys, and adrenal glands. Regions of interest were drawn over these organs to exclude focal lesions, and the SUVmax (normalized to patients’ body weight) was recorded. In the case of bilateral organs such as the parotids, thyroids, lungs, and kidneys, the average SUVmax was calculated. For the adrenal glands, only the left adrenal gland was measured because uptake by the right adrenal gland could easily be influenced by adjacent liver uptake.
Any focal accumulations not explained by physiologic uptake were interpreted as focal lesions. Up to 4 lesions were chosen in each patient, including 2 hepatic lesions and 2 extrahepatic lesions. The lesion uptake was measured using SUVmax. Tumor-to-background ratio was quantified using blood pool, kidney, and liver as reference tissues.
Radiation Dosimetry
Whole-organ volumes of interest were manually drawn over the source organs, including spleen, liver, kidneys, pituitary glands, vertebral bodies L1–L5, and urinary bladder, at each time point. The non–decay-corrected activities at different time points were documented as percentage injected dosage and fitted with monoexponential curves. The area under the time–activity curve between time 0 and the first time point was calculated assuming a linear increase from 0 to the first measured activity. The area under the time–activity curve after the first time point was calculated by trapezoidal integration from the first time point to the last time point and extrapolation from the last data point using the fitted monoexponential function. For bone marrow, the residence time was derived using an image-based integration of the L1–L5 vertebrae, assuming L1–L5 have 12.3% of the whole-body bone marrow (13). Urinary bladder residence time was determined using the voiding bladder model implemented in OLINDA/EXM software, setting a 2-h bladder-voiding interval. The residence time in the remainder of the body was calculated as the maximum possible residence time (based on physical decay only) minus the sum of the residence time of all source organs. Absorbed dose for target organs and whole-body effective dose were determined with OLINDA/EXM software (version 1.0) using adult male models.
Statistical Analysis
Data were expressed as mean ± SD. The differences between 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 were evaluated using the Student t test (SPSS, version 22). Because of 2 dropouts in arm B, PET analyses were done for only 14 patients, whereas safety evaluations were done for all 16 patients. A P value of less than 0.05 was considered to indicate statistical significance.
RESULTS
Patients and Safety
Sixteen patients, 8 in each arm, were recruited in this phase. There were 2 dropouts due to adverse events (AEs) at 10–15 min after injection. The demographic and clinical characteristics are summarized in Table 1 (including the 2 dropouts).
Demographic and Clinical Characteristics of Patients
There was a mild decrease in blood pressure at 24 h after injection, compared with baseline (127.5/82.4 mm Hg vs. 133.6/86.3 mmHg, P < 0.05). No patients had symptoms related to hypotension after LM3 injection. No significant change in other vital signs or 3-lead electrocardiography was recorded.
There were 2 AEs (patients 3 and 8). Patient 3 was a 69-y-old man with functional pancreatic NET (grade 1 insulinoma; Ki-67 index, 2%; primary tumor resected) and multiple hepatic metastases. He had grade 2 nausea 10 min after tracer injection. Patient 8 was a 33-y-old woman also with functional pancreatic NET (grade 3 insulinoma; Ki-67 index, 30%) as well as multiple hepatic and lymph node metastases and a solitary bone metastasis. She had grade 2 nausea and grade 1 vomiting 15 min after tracer injection. The scans were discontinued after the AEs, and both patients withdrew from the study. The symptoms abated after a few hours without any intervention. Vital signs were stable during that period and also at 24 h after injection. Both patients were from arm B. No other AEs were reported.
Biodistribution in Normal Organs
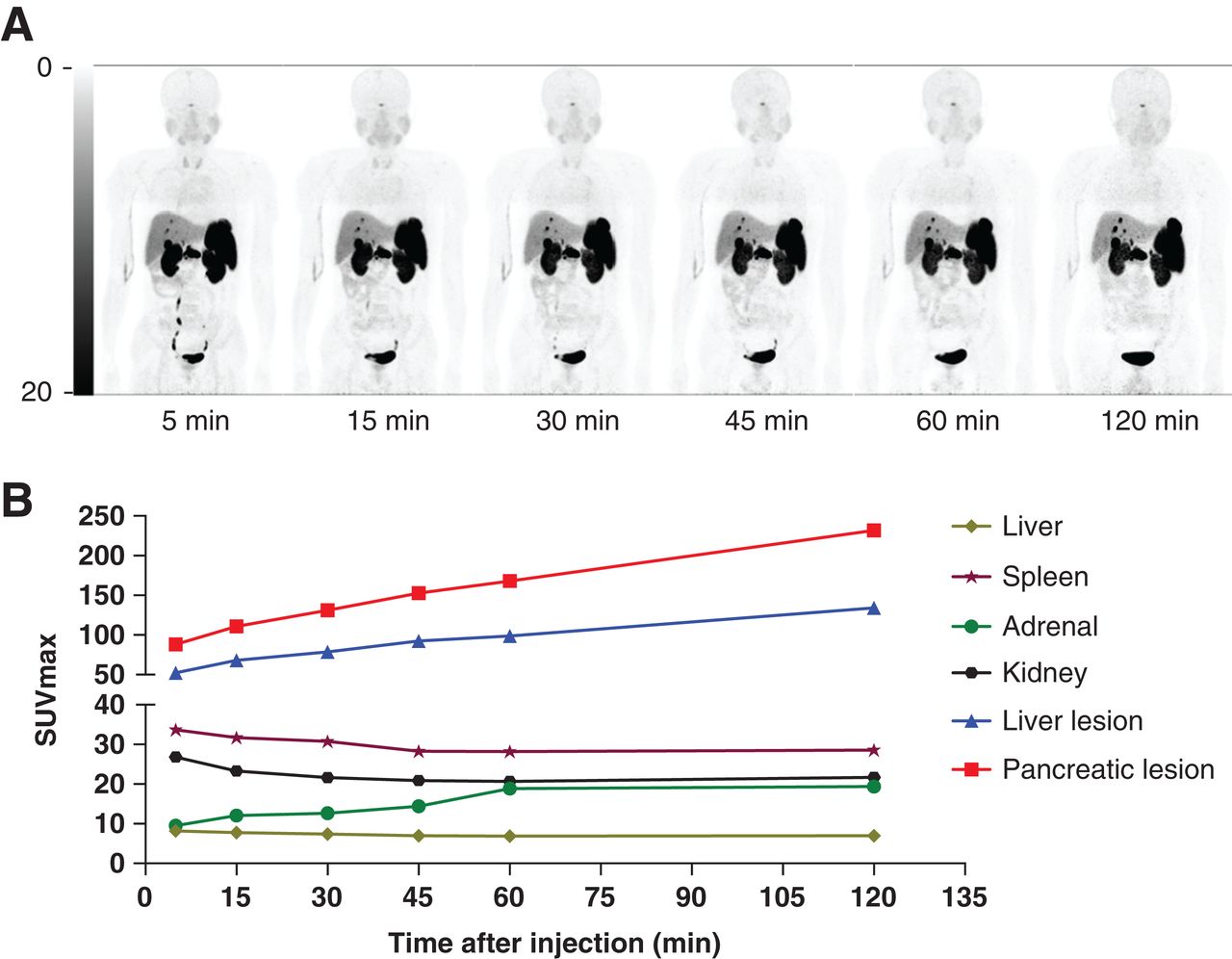
Figure 2 shows the biodistribution of 68Ga-NODAGA-LM3 at 5, 15, 30, 45, 60, and 120 min after injection in a patient with pancreatic NET. Figure 3 shows the biodistribution of 68Ga-DOTA-LM3 in another patient with pancreatic NET. Significantly lower organ uptake was observed in the pituitary, parotids, liver, spleen, pancreas, adrenal, stomach, small intestine, and kidneys with 68Ga-DOTA-LM3 than with 68Ga-NODAGA-LM3. The biodistribution in normal organs is summarized in Figure 4. The SUVmax at 1 h after injection is compared in Table 2.
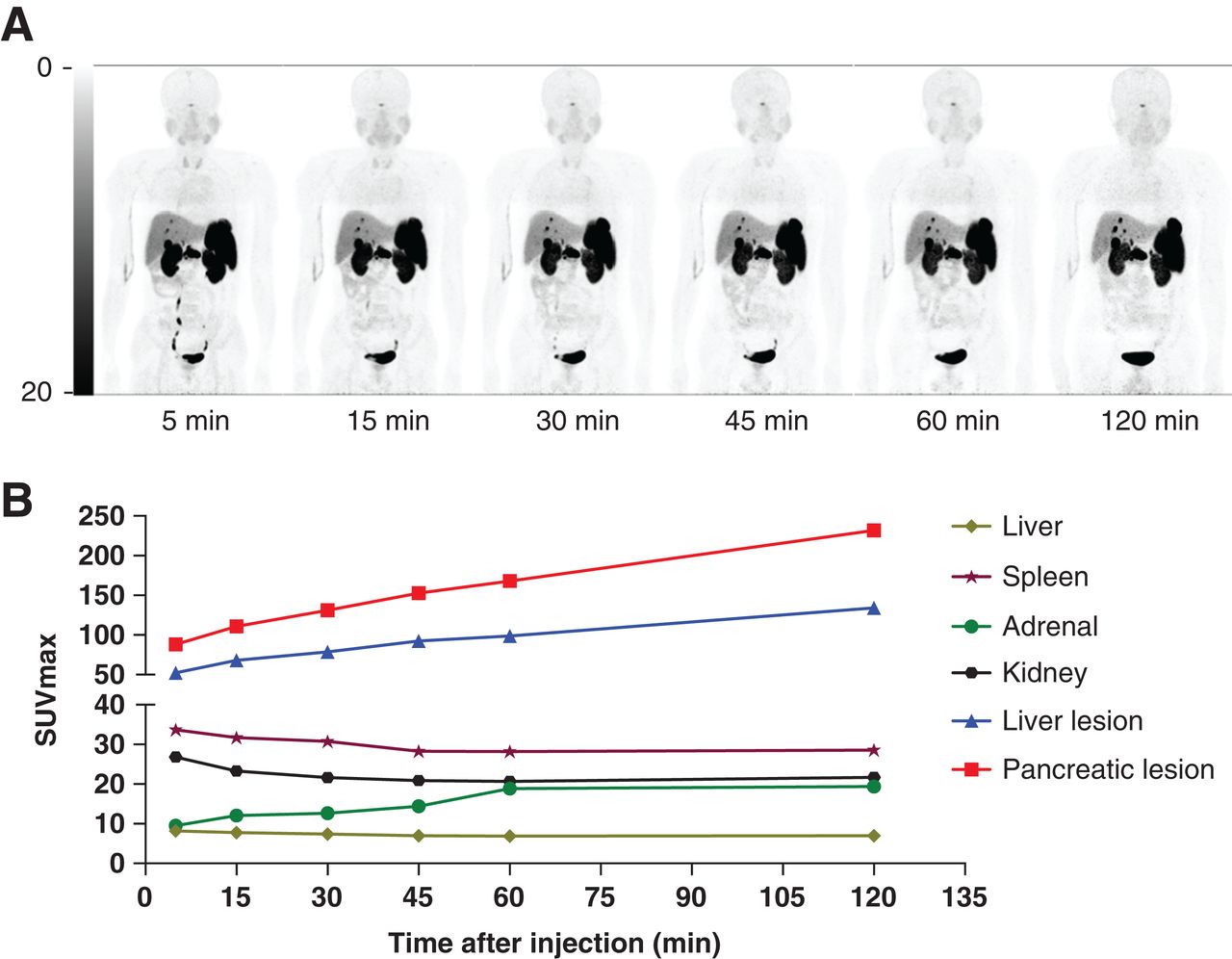
Patient 6 with grade 2 pancreatic NET as well as multiple hepatic and lymph node metastases. (A) Biodistribution of 68Ga-NODAGA-LM3 at 5, 15, 30, 45, 60, and 120 min after injection. Physiologic uptake could be visualized in SSTR-positive organs such as pituitary, adrenals, and spleen. Liver demonstrated moderate accumulation of 68Ga-NODAGA-LM3. (B) SUVmax–time curves showed excellent tumor retention in both pancreatic tumor and hepatic metastases.

Patient 12 with grade 1 pancreatic NET as well as multiple hepatic and lymph node metastases. (A) Biodistribution of 68Ga-DOTA-LM3 at 5, 15, 30, 45, 60, and 120 min after injection. No significant uptake is noted in any normal organs except for urinary tract. Spleen demonstrated only mild 68Ga-DOTA-LM3 accumulation. (B) SUVmax–time curves. SUVmax of normal organs remained at low level after 68Ga-DOTA-LM3 administration. Both primary and metastatic lesions showed good tracer accumulation, leading to high image contrast.
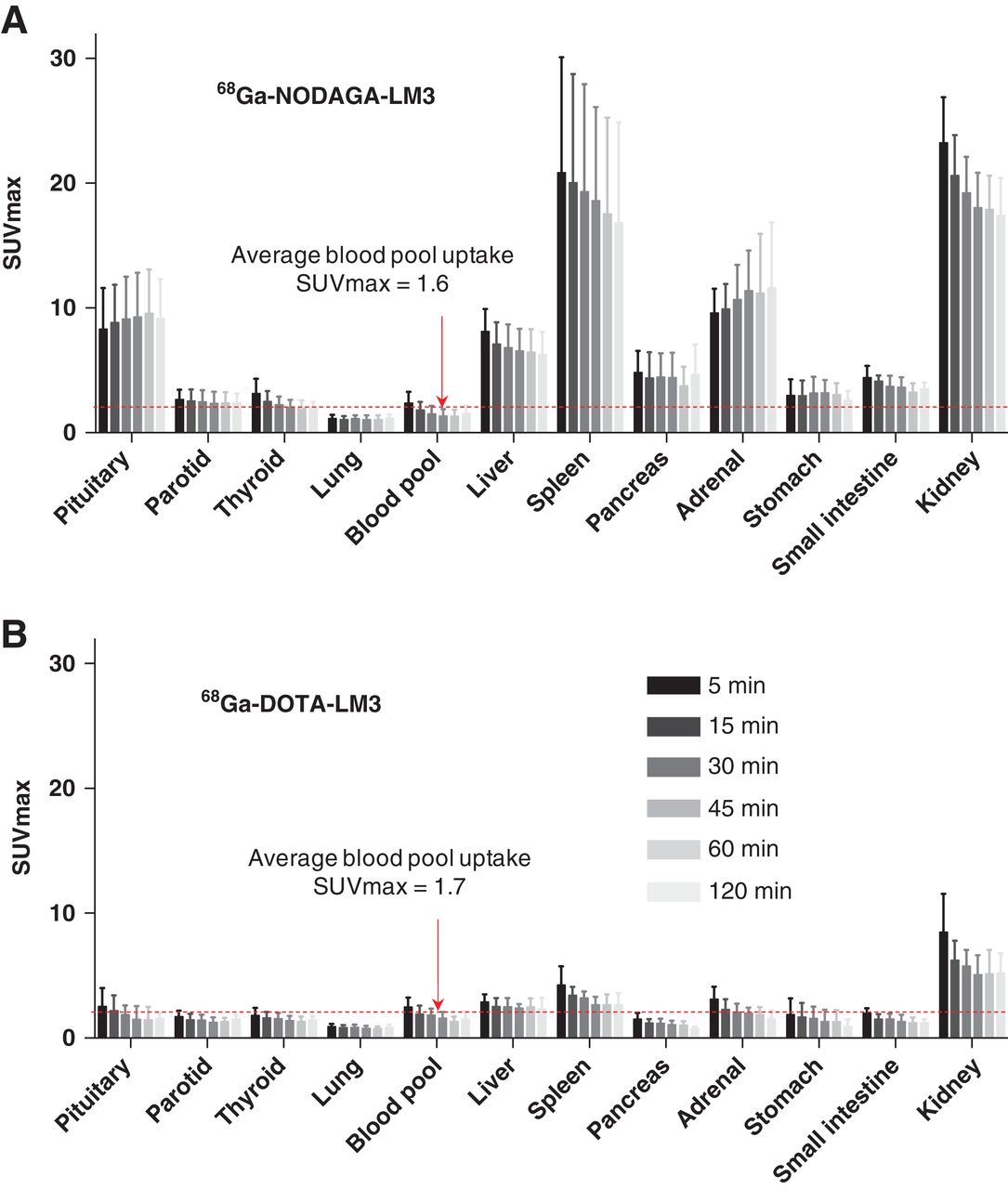
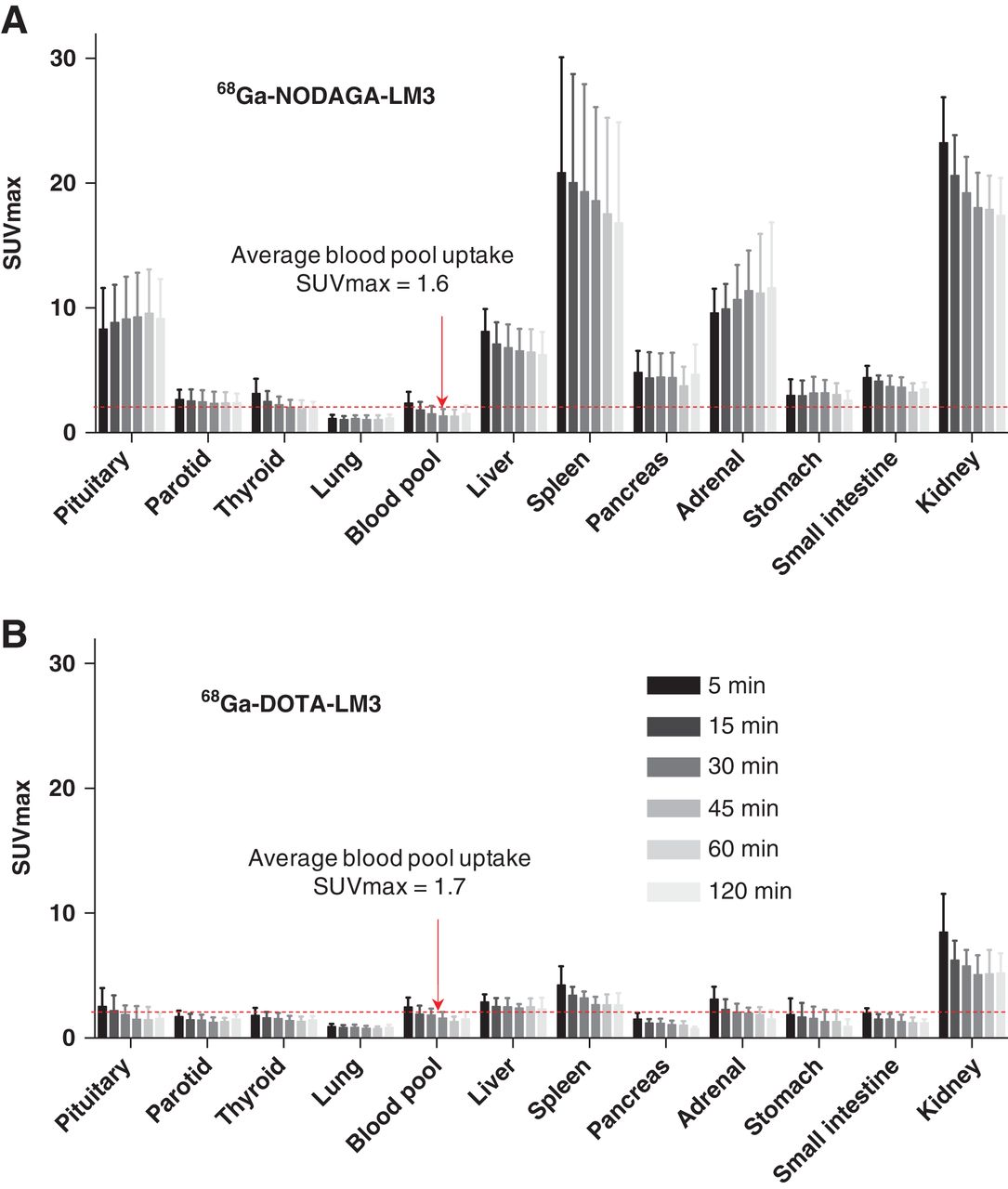
Biodistribution of 68Ga-NODAGA-LM3 (A) and 68Ga-DOTA-LM3 (B) in normal organs at 5, 15, 30, 45, 60, and 120 min after injection.
Uptake of Normal Organs at 1 Hour After Injection
Tumor Uptake
In total, 38 lesions were analyzed in 14 patients, including 18 lesions (13 hepatic, 2 pancreatic, 1 lymph node, 1 bone, and 1 stomach) with 68Ga-NODAGA-LM3 and 20 lesions (12 hepatic, 4 pancreatic, 2 lymph node, 1 bone, and 1 brain) with 68Ga-DOTA-LM3. With 68Ga-NODAGA-LM3, the tracer accumulation in tumor lesions increased by 138%, from an average SUVmax of 31.3 ± 19.7 at 5 min to 74.6 ± 56.3 at 2 h. With 68Ga-DOTA-LM3, the tumor uptake rapidly reached a high level at 5 min after injection, with an average SUVmax of 36.6 ± 23.6, and continued to increase to 45.3 ± 29.3 until 30 min after injection, remaining at a plateau thereafter. The SUVmax and tumor-to-background ratios are summarized in Figure 5 (data available in Supplemental Table 2). Because of the relatively lower kidney and liver background for 68Ga-DOTA-LM3, it showed a significantly higher tumor-to-kidney and tumor-to-liver ratios than did 68Ga-NODAGA-LM3 at all time points. There were no significant differences in SUVmax or tumor-to-background ratios between hepatic and extrahepatic lesions in either arm (P > 0.05).

SUVmax (A), tumor–to–blood-pool ratio (B), tumor-to-kidney ratio (C), and tumor-to-liver ratio (D) of 38 reference lesions, including 18 lesions with 68Ga-NODAGA-LM3 PET and 20 lesions with 68Ga-DOTA-LM3 PET. TBR = tumor-to-background ratio.
Radiation Dosimetry
The residence time of source organs and the absorbed dose of target organs are summarized in Tables 3 and 4, respectively. The urinary bladder wall received the highest radiation dose, 0.162 mGy/MBq for 68Ga-NODAGA-LM3 and 0.202 mGy/MBq for 68Ga-DOTA-LM3. Liver residence time and absorbed doses were higher in patients with than in patients without fulminant liver diseases (Supplemental Table 3). The effective dose was 0.026 ± 0.003 mSv/MBq for 68Ga-NODAGA-LM3 and 0.025 ± 0.002 mSv/MBq for 68Ga-DOTA-LM3.
Residence Time in Source Organs
Absorbed Doses to Target Organs and Effective Dose
DISCUSSION
The antagonists 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 show high SSTR2 affinities in both in vitro and in vivo preclinical studies. To our knowledge, this was the first clinical study to evaluate these 2 tracers in patients with NETs. The results show favorable biodistribution and dosimetry features, and both tracers were well tolerated in most patients.
One important finding of our study was the high tumor accumulation of 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3. Both tracers showed high tumor uptake; the highest SUVmax was up to 231.9 for 68Ga-NODAGA-LM3 and 126.9 for 68Ga-DOTA-LM3. The average SUVmax at 1 h after injection was 57.5 ± 39.4 for 68Ga-NODAGA-LM3 and 47.2 ± 32.6 for 68Ga-DOTA-LM3—values that are certainly comparable to those for SSTR agonists and other SSTR2 antagonists (8, 14–18). Furthermore, both tracers showed excellent tumor retention. Our data agree with the previous finding that radioantagonists show long tumor retention despite little internalization (6, 10). High tumor retention is a key feature for peptide receptor radionuclide therapy. Zhang et al. provided preliminary evidence of efficacy using 177Lu-DOTA-LM3 treatment in a patient with 68Ga-DOTATOC–negative liver metastases (11, 12). The patient was in nearly complete remission after 3 cycles of intraarterial peptide receptor radionuclide therapy, with a total of 20.4 GBq of 177Lu-DOTA-LM3. Our finding suggests that the antagonist LM3 may be another available peptide for peptide receptor radionuclide therapy in the future and that both 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 may be promising diagnostic companions.
The biodistribution of 68Ga-NODAGA-LM3 was similar to that of SSTR2 agonists, which show moderate or high uptake in SSTR2-positive organs (19). The highest organ SUVmax (except for the kidneys and urinary bladder) was observed in the spleen, followed by the adrenal and pituitary glands. 68Ga-DOTA-LM3, on the other hand, showed minimal uptake in almost all organs apart from the urinary tract. Only the liver and spleen showed slightly higher 68Ga-DOTA-LM3 accumulation than the blood pool, whereas all other organs showed either comparable or lower uptake. Interestingly, the differences in organ uptake between these 2 tracers were observed not only in SSTR2-positive organs, such as the pituitary, spleen, and adrenals, but also in the liver, reputed to be an SSTR2-negative organ. The lower background of 68Ga-DOTA-LM3 was further translated into significantly higher tumor-to-kidney and tumor-to-liver ratios. The reason for the differences in organ uptake is currently not well understood and requires further study. SSTR2 antagonists are sensitive to the chelator appended. With different chelators attached, a previous study has shown 68Ga-NODAGA-LM3 to have an SSTR2 affinity (1.3 nmol/L) 10-fold higher than that of 68Ga-DOTA-LM3 (12.5 nmol/L) (10). Our study suggests that the chelators not only affect tumor uptake and retention but also biodistribution in normal organs. It should be noted, however, that our data are partially in contrast to those published by Fani et al. (10). They found kidney uptake to be 65% higher for 68Ga-DOTA-LM3 than for 68Ga-NODAGA-LM3 (percentage injected dose per gram, 32.50 vs. 19.68) in animal models, whereas our study showed kidney uptake to be 72% lower for 68Ga-DOTA-LM3 than for 68Ga-NODAGA-LM3 (SUVmax, 5.1 vs. 17.9). The differences may result from different species and peptide amounts used.
The dosimetry data for 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 showed an effective dose slightly higher than, yet comparable to, that of other SSTR2 antagonists (0.024 mSv/MBq for 68Ga-NODAGA-JR11 and 0.022 mSv/MBq for 68Ga-DOTA-JR11) (18, 20). We also observed a higher liver dose for 68Ga-DOTA-LM3 despite a lower liver background. This finding is attributed mainly to dosimetry methodology. We used whole-organ volumes of interest to calculate the whole-organ activity (including disease activity). In our study, several patients (patient 1 in arm A, and patients 2, 7, and 16 in arm B) had fulminant hepatic metastases (Supplemental Fig. 1), which led to a much longer liver residence time and a much higher absorbed dose than in the other patients (Supplemental Table 3). These metastases explain the higher liver dose seen for 68Ga-DOTA-LM3 despite the lower liver background and are also responsible for the comparable effective dose between these 2 tracers despite faster washout of 68Ga-DOTA-LM3.
The administration of 68Ga-NODAGA-LM3 was well tolerated in all patients in arm A. However, 2 patients with functional pancreatic NET (insulinoma) in arm B reported AEs at 10–15 min after 68Ga-DOTA-LM3 injection. Both patients experienced nausea (grade 2), and one of them had vomiting (grade 1). These 2 AEs were considered to be related to the 68Ga-DOTA-LM3 injection. In a previous study investigating the safety of another antagonist, 68Ga-NODAGA-JR11 (68Ga-OPS202), no pharmacologic response to the radiopharmaceutical was reported (20). However, Krebs et al. reported potential SSTR2 antagonistic properties for 68Ga-DOTA-JR11 (18). In their study, 2 patients with functional NETs (the type of tumor was not specified) experienced symptoms such as flushing, hypotension (grade 3), nausea, and lightheadedness. Our study suggests that administration of an SSTR2 antagonist might trigger side effects such as nausea and vomiting. However, because so few patients were recruited, it is too early to tell whether these side effects were related to tumor functional status, antagonist peptides, or chelating agents. In fact, nausea and vomiting are common side effects of injecting somatostatin analogs. Patients with NETs, functional or nonfunctional, could have nausea and vomiting after administration of a therapeutic dose of octreotide acetate (Sandostatin; Novartis Pharmaceuticals Corp.). The AEs observed in our study may be related to the quick bolus administration. A slow bolus injection or infusion might help to relieve the symptom. Though the 2 patients with AEs in our study discontinued the scan because they were not able to lie still on the exam table for the first hour, the AEs were usually mild and would not affect an image acquisition at 60 min after injection.
Blood pressure was significantly lower at 24 h after injection than at baseline (127.5/82.4 mm Hg vs. 133.6/86.3 mm Hg, P < 0.05). However, this finding was not translated into any clinically relevant events. A blood pressure change is not a specific finding and may be influenced by many conditions, such as the patient’s emotional status, body temperature, exercise status, and caffeine consumption (21). Given the low peptide dose (40 μg) used in our study and the fast clearance of the radiopharmaceuticals (median biologic half-life of 5.18 h), the change in blood pressure at 24 h after injection was probably not related to antagonist injection.
Our study was limited by the small number of patients, which is typical for dosimetry evaluation of radiopharmaceuticals. Besides, neither blood nor urine samples were collected in our study. Blood and urine samples could allow us to search for metabolites. Lastly, the ideal comparison between 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 would be one conducted on the same group of patients. A further head-to-head comparison study is required.
CONCLUSION
Both 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 show a favorable biodistribution, high tumor uptake, and good tumor retention, resulting in high image contrast. The dosimetry data are comparable to those for other 68Ga-labeled SSTR2 antagonists. Further studies are required to look into the potential antagonistic effects of 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3.
DISCLOSURE
This work was sponsored in part by the CAMS Initiative for Innovative Medicine (2017-I2M-4-002 and 2018-I2M-3-001) and by the Nonprofit Central Research Institute Fund of the Chinese Academy of Medical Sciences (2019PT310026). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Do 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 show suitable biodistribution and dosimetry data in NET, and are they safe?
PERTINENT FINDINGS: Both 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 show a favorable biodistribution, high tumor uptake, and good tumor retention. Few AEs were reported using 68Ga-DOTA-LM3.
IMPLICATIONS FOR PATIENT CARE: Both 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 are promising in NET imaging.
ACKNOWLEDGMENTS
We thank Prof. Richard P. Baum for inspiring us on the LM3 project. We also thank all the patients who participated in this study, Yue Zhang (SinoUnion Healthcare Inc., China) for image acquisition, and Dr. Chengyan Dong (GE Healthcare, China) for critical proofreading and figure suggestions.
Footnotes
Published online February 12, 2021.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 6, 2020.
- Accepted for publication January 27, 2021.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}