


Abstract
111In-diethylenetriaminepentaacetic acid (DTPA)-octreotide scintigraphy is currently the nuclear medicine imaging modality of choice for identifying neuroendocrine tumors. However, there are cohorts of patients in whom scintigraphy findings are negative or equivocal. We evaluated the role of 68Ga-DOTATATE PET in a selected group of patients with negative or weakly positive findings on 111In-DTPA-octreotide scintigraphy to determine whether 68Ga-DOTATATE PET is able to detect additional disease and, if so, whether patient management is altered. Methods: Fifty-one patients with a histologically confirmed diagnosis of neuroendocrine tumors were included. Of the 51 patients, 35 who were negative and 16 equivocal for uptake on 111In-DTPA-octreotide scintigraphy underwent 68Ga-DOTATATE PET. Findings were compared using a region-by-region analysis. All findings were verified with CT or MRI. After 68Ga-DOTATATE PET, all cases were reviewed to determine whether the 68Ga-DOTATATE PET findings resulted in any alteration in management, in terms of suitability for peptide receptor therapy, somatostatin analogs, and surgery. Results: Of the 51 patients, 47 had evidence of disease on cross-sectional imaging or biochemically. 68Ga-DOTATATE PET was positive in 41 of these 47 patients (87.2%). No false-positive lesions were identified. 68Ga-DOTATATE PET detected 168 of the 226 lesions (74.3%) that were identified with cross-sectional imaging. 68Ga-DOTATATE PET identified significantly more lesions than 111In-DTPA-octreotide scintigraphy (P < 0.001). There was no correlation between 68Ga-DOTATATE uptake and histologic grade of neuroendocrine tumors. 68Ga-DOTATATE imaging changed management in 36 patients (70.6%), who were subsequently deemed suitable for peptide receptor–targeted therapy. Conclusion: In patients with negative or equivocal 111In-DTPA-octreotide findings, 68Ga-DOTATATE PET identifies additional lesions and may alter management in most cases.
- 68Ga-DOTATATE PET
- neuroendocrine tumor
- 111In-DTPA-octreotide scintigraphy
- peptide receptor therapy
- somatostatin analogs
Gastroenteropancreatic neuroendocrine tumors (NETs) are a heterogeneous group of relatively rare tumors. These tumors may arise from almost anywhere within the body but arise predominantly from the gastroenteropancreatic tract; they can metastasize to any organ (1). Somatostatin receptor (SSTR) overexpression in NETs has enabled development of imaging with scintigraphy using radiolabeled somatostatin analogs (2,3). To date, 5 SSTRs have been characterized, all of which are expressed in differing frequencies in NETs (4). SSTR-2 and -5 are expressed in 70%−90% of NETs (5). The most commonly used radiolabeled somatostatin analogs allow visualization and staging of carcinoid tumors expressing SSTR-2 and -5, though expression of other SSTR receptors can be identified with different analogs (6). The most commonly used radioligand is 111In-diethylenetriaminepentaacetic acid (DTPA)–octreotide, which is commercially available as 111In-pentetreotide. The expression of SSTRs in these tumors allows radionuclide therapy, subject to good uptake of somatostatin radiolabeled analogs. To date this expression has been assessed using 111In-DTPA-octreotide scintigraphy (7,8).
111In-DTPA-octreotide binds predominantly to SSTR-2–positive cells and emits γ-rays, which enable imaging of SSTR-2–positive NETs (9). The reported sensitivity of 111In-DTPA-octreotide scintigraphy varies from 67% to 100% (6,7,10,11) and differs according to the type of NET being visualized. There are limitations with this technique, and it has a restricted ability to identify lesions smaller than 1 cm and to obtain good spatial resolution, even when using SPECT (12).
In the last few years, studies using 68Ga-DOTATOC PET in NETs have shown promising results, with a higher rate of lesion identification than is achieved with conventional 111In-DTPA-octreotide scintigraphy (13–16). On the basis of availability at that time, in this study we used DOTATATE, an SSTR-2 analog (17), labeled with 68Ga, a positron emitter. 68Ga is produced from a 68Ge–68Ga generator and therefore is not dependent on a cyclotron. The automated labeling of this radiopharmaceutical done according to good laboratory practice under sterile conditions in an isolator takes approximately 60 min. The yield of 68Ga-DOTATATE is more than 98% with this method.
The study had 3 aims: first, to assess whether 68Ga-DOTATATE PET identifies SSTR-2–positive disease in NET patients with negative or weakly positive 111In-DTPA-octreotide findings; second, to establish whether there is any association between tumor grade and lesion identification using 68Ga-DOTATATE PET; and finally, to evaluate whether 68Ga-DOTATATE PET alters clinical management in patients with weak or negative 111In-DTPA-octreotide findings.
MATERIALS AND METHODS
Study Population
From November 2006 to March 2008, 312 patients underwent 111In-DTPA-octreotide scintigraphy. All were under prospective follow-up at the NET unit of Royal Free Hospital, London. Of these, 51 were referred for 68Ga-DOTATATE PET because of scintigraphy findings that were negative or showed only low-grade uptake of tracer (Krenning score, <2) (18). Briefly, the scale for the Krenning score is as follows: 0 = no abnormality, 1 = faint uptake in the tumor; 2 = clear uptake in the tumor but less than in the liver; 3 = uptake greater in the tumor than in the liver; 4 = uptake much greater in the tumor than in the liver (18). Long-acting somatostatin analogs were not stopped before imaging with PET or 111In-DTPA-octreotide scintigraphy.
We retrospectively reviewed the images and clinical data from the 51 patients (27 men and 24 women; age range, 18–80 y; median age, 55.5 y), who were imaged with 68Ga-DOTATATE PET/CT between January 2007 and April 2008. Forty-five patients underwent chest, abdomen, and pelvis CT; 2 underwent abdomen MRI; and 4 underwent chest, abdomen, and pelvis CT and additional MRI of the liver. All patients gave informed consent, in line with local medical ethical guidance.
The primary tumor origin was as follows: medullary thyroid, 2; thymic carcinoids, 2; paraganglioma, 2; hindgut, 2; bronchus, 2; pancreas, 13; midgut, 22. The remaining 6 patients had cancer of unknown primary origin (Table 1). All patients had a previous histologic diagnosis of NET based on World Health Organization criteria. All had undergone scanning with 111In-DTPA-octreotide within a median of 4 mo (range, 1–8 mo) of 68Ga-DOTATATE PET. Histologic findings were available in all cases, and tumor grade was classified as low, intermediate, or high, using the proposed criteria of the European Neuroendocrine Tumour Society for grading gastroenteropancreatic NETs (19,20). The classification was extended to include tumors of other sites and cancer of unknown primary origin.
Characteristics of Study Population
Image Acquisition
For 68Ga-DOTATATE PET, images were acquired 1 h after injection of 120–200 MBq of 68Ga-DOTATATE. No adverse effects were observed after the injection of 68Ga-DOTATATE. Imaging was performed using a dedicated GE Discovery LS PET/CT unit; whole-body examinations (mid brain to mid thigh) were performed with the patient supine.
CT was performed using the four 3.75-mm detectors, a pitch of 1.5, and a 5-mm collimation. The CT exposure factors for all examinations were 140 kVp and 80 mA in 0.8 s. With patient position maintained, a whole-body PET emission scan was performed covering an area identical to that covered by CT; scans were performed in 3-dimensional mode. All PET acquisitions were carried out in 3-dimensional mode (4 min per bed position), in an approximately 30-min scanning time. PET images were reconstructed using CT for attenuation correction. Transaxial emission images of 4.3 × 4.3 × 4.25 mm were reconstructed using ordered-subsets expectation maximization with 2 iterations and 28 subsets. The axial field of view was 148.75 mm, resulting in 35 slices per bed position.
For 111In-DTPA-octreotide SPECT, patients were injected with 200 MBq of 111In-pentetreotide IV (Covidien). Whole-body images were acquired at 24 h after injection on a dual-head γ-camera (Picker Prism; Phillips Medical Technology) using a medium-energy collimator. Patients were scanned with a camera speed of 7.2 cm/min and a matrix of 256 × 1,024. Photopeaks were set at 173 and 247 keV, with ±10% windows and no offset. SPECT abdominal images were obtained from the dome of the liver downward. An additional chest or pelvic SPECT study was performed if warranted by the appearance of the whole body or if abnormalities had been identified previously in other areas on cross-sectional imaging. Scan parameters were as follows: medium-energy collimator, 60 stops per head at 3° intervals, 25 s per stop, 64 × 64 matrix. The same energy window was used as with planar imaging. Images were processed and analyzed at a workstation using Odyssey software (Phillips Medical Technology). They were reconstructed using an iterative ordered-subsets expectation maximization program with 6 iterations and processed with a count-optimized Butterworth filter. Images were displayed as a full data set of orthogonal slices of 9-mm thickness. Images from 111In-DTPA-octreotide scintigraphy were reviewed by 2 nuclear medicine physicians.
The images from 68Ga-DOTATATE PET/CT were reported in consensus by an experienced dedicated nuclear medicine physician and a dual-accredited radiologist/nuclear medicine physician, who were unaware of the results of the previous 111In-DTPA-octreotide study. Areas of abnormal focal uptake were documented, with care taken to exclude sites of known physiologic activity on 68Ga-DOTATATE PET and 111In-DTPA-octreotide scintigraphy. These areas of abnormal uptake were compared with cross-sectional imaging to confirm the presence of lesions. The images from 111In-DTPA-octreotide scintigraphy were reported independently by an experienced nuclear medicine physician. If any discrepancies were present in the reports of the 2 examiners, the images were reviewed together and a consensus reached.
A 3-phase CT scan was obtained (unenhanced, arterial-phase enhancement at 30 s after injection, and venous-phase enhancement at 70 s after injection). The liver alone is scanned before contrast enhancement, the chest and liver are scanned in the arterial phase, and the whole abdomen and pelvis are scanned in the venous phase. All scans were acquired at 120 kVp and variable amperage, depending on body habitus. We used a Brilliance 64-slice scanner (Phillips Medical Systems, DMC GmbH) or a Lightspeed scanner (GE Healthcare). Scans were reconstructed at 3-mm (Brilliance) or 5-mm (Lightspeed) intervals. Intravenous contrast material was used: 100 mL of Omnipaque 300 (GE Healthcare) administered via a pump injector (E-Z-EM) at 3.5 mL/s.
The MRI scanner was a 1.5-T Achieva (Phillips Medical Systems). All scans were acquired using the Synergy Sense body coil. Slice thickness was 7 mm, with a 0.7-mm interspace and a 512 × 512 matrix. The contrast medium was Dotarem (Guerbet), 0.2 mL/kg, infused at 1.5 mL/s with a 20-mL saline flush via a cannula in an antecubital vein using a pump injector (Medrad).
Interpretation of Data
The number of lesions that could be identified clearly as single foci was determined for each patient. To enable a methodic and consistent approach to lesion identification, we created 3 categories of lesion sites: organs (lungs, breast, liver, pancreas, gastrointestinal tract, kidney, spleen, and pelvis/ovaries), nodal regions (thoracic, mesenteric, abdominal, and pelvic [excluding mesenteric]), and musculoskeletal system (vertebrae, bony thorax, bony pelvis, and limb bones). The same anatomic areas were imaged with 68Ga-DOTATATE PET and 111In-DTPA-octreotide scintigraphy to ensure relevant comparison of lesion detection. Because of confluence and inability to clearly delineate single liver lesions in some cases, liver metastases were classified as 1 organ metastasis, independent of the number of liver metastases present. Lymph nodes smaller than 1 cm on CT or MRI and showing marked avidity for 68Ga-DOTATATE and 111In-DTPA-octreotide were labeled as positive for disease.
The presence of lesions was confirmed by cross-sectional imaging of all patients with CT or MRI. Patients who underwent 68Ga-PET had PET/CT to confirm the location of disease. Plasma chromogranin A levels were available for all patients, and where appropriate, fasting gut hormone levels and urinary 5-hydroxyindoleacetic acid were also measured.
Statistical Analysis
Statistical analysis was performed using Prism (version 5.00; GraphPad Software) for Windows (Microsoft). Because the values generally were not normally distributed, nonparametric tests were used to compare marker levels between groups, that is, the Mann–Whitney U test (for 2 groups).
RESULTS
In total, 51 patients underwent 68Ga-DOTATATE PET and 111In-DTPA-octreotide scanning. Of these, 47 had evidence of disease on cross-sectional imaging; the 4 remaining patients had undergone previous curative surgical resection and were receiving surveillance imaging. In the 47 patients with evidence of disease, a total of 226 lesions were identified on cross-sectional imaging (including MRI, CT, and PET/CT). The number of patients with lesions from each anatomic site is listed in Table 2. Thirty-five patients were negative for uptake on 111In-DTPA-octreotide scintigraphy, whereas in the remaining 16 patients a total of 27 lesions were identified with a Krenning score of less than 2. 68Ga-DOTATATE PET identified disease in 41 of 47 patients (87.2%) and detected 168 (74.3%) of the 226 lesions identified on cross-sectional imaging. The number of lesions seen in each organ with each modality is listed in Table 3.
Total Number of Lesions Identified in Each Type of NET with the Different Modalities
Location of Lesions Identified by 111In-DTPA-Octreotide Scintigraphy, 68Ga-DOTATATE PET, and Cross-Sectional Imaging (CT ± MRI) in 47 Patients with Radiologic Evidence of Disease
Patient Analysis
Negative 111In-DTPA-Octreotide Findings
Among the 51 patients, 111In-DTPA-octreotide findings were negative, with no evidence of uptake (other than physiologic uptake) in 35 patients. In 3 of these 35 patients, no disease was identified on cross-sectional imaging and patients had normal chromogranin A and fasting gut hormone levels. The 3 patients with no evidence of disease on any modalities are considered to be disease-free currently; all of these patients had undergone previous surgical resection.
The remaining 32 patients had disease identified on cross-sectional imaging. Among these, 68Ga-DOTATATE findings were positive in 27 (Fig. 1). In total, 97 lesions were identified in the 27 patients with positive 68Ga-DOTATATE findings, whereas cross-sectional imaging identified 125 lesions in the 32 patients with disease.

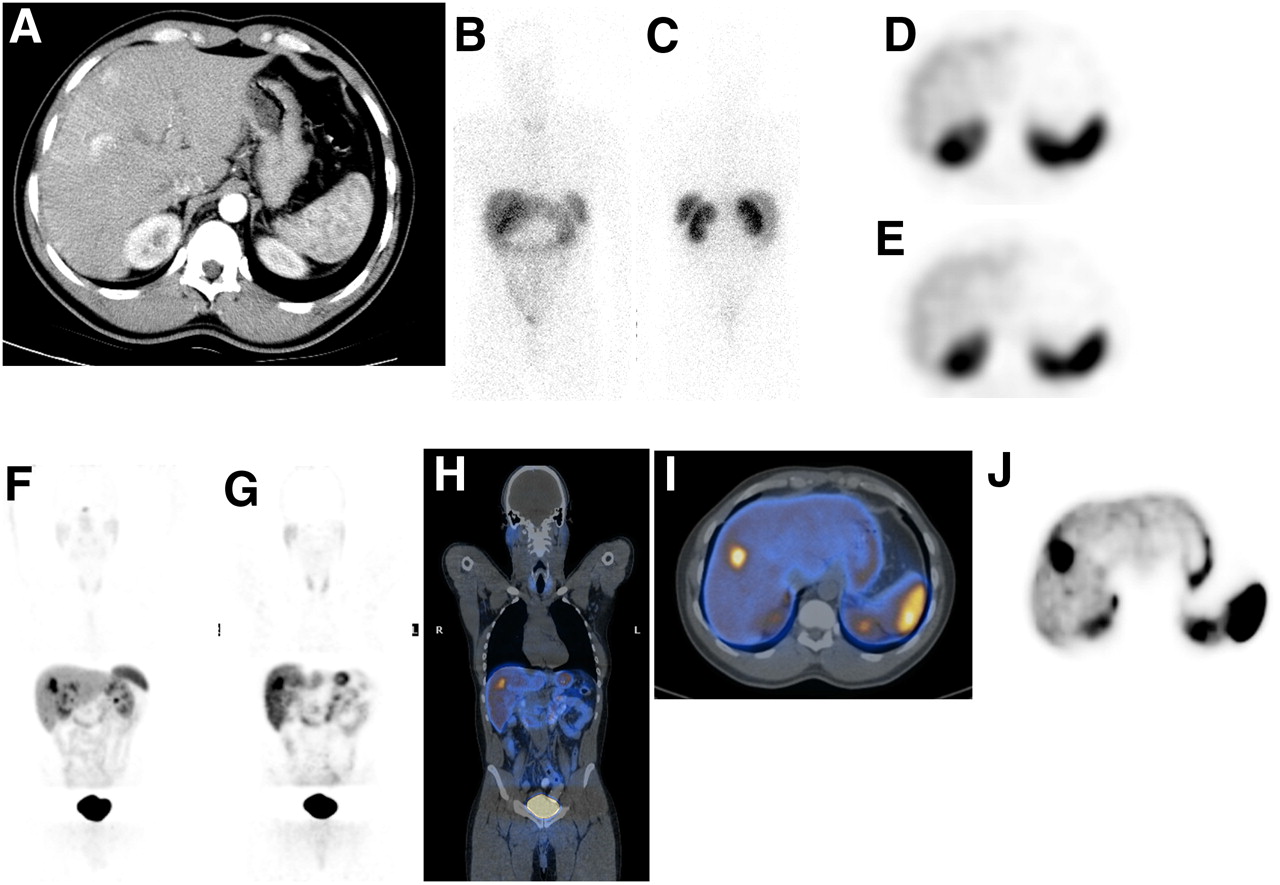
A 69-y-old man with low-grade metastatic midgut NET. (A) Arterial-phase CT shows multiple arterially enhancing and low-attenuation liver metastases. (B and C) Anterior and posterior whole-body 111In-DTPA-octreotide scintigraphy shows low-grade (Krenning score, 1) mesenteric metastases (arrow) but no liver metastases. (D and E) Axial 111In-DTPA-octreotide SPECT at level of spleen shows heterogeneous liver uptake with no discernable liver deposits. (F) Maximum-intensity-projection 68Ga-DOTATATE PET shows multiple deposits in liver and mesentery. (G) Coronal 68Ga-DOTATATE PET anterior to kidney shows multiple liver metastases. (H) 68Ga-DOTATATE PET/CT of G. (I) Axial 68Ga-DOTATATE PET/CT at level of spleen shows multiple liver metastases. (J) Axial 68Ga-DOTATATE PET at level of spleen shows multiple liver metastases.
Five patients who were negative for uptake on both 68Ga-DOTATATE PET and 111In-DOTA-octreotide scanning had evidence of disease on cross-sectional imaging. In these patients, 27 lesions were identified on CT ± MRI. These tumors were metastatic; the primary sites were ileal and pancreatic in 1 case each, whereas 3 were from unknown primaries. Two patients had functional syndromes (both carcinoid), and the remaining 3 had no syndromic features. Histologic results from these 5 patients showed 2 with low-grade tumors, 2 with intermediate-grade tumors, and 1 with a high-grade tumor.
Low-Grade or Faint Uptake on 111In-DTPA-Octreotide Scintigraphy
In 16 patients, there was some uptake on 111In-DTPA-octreotide scintigraphy; however, the uptake in the extrahepatic lesion was of low grade and notably less than that in the liver. Cross-sectional evidence of disease was identified in 15 of these patients. In 1 patient, 111In-DTPA-octreotide scintigraphy identified mediastinal and left-lung uptake of very low grade. This uptake was commented on in view of the fact that the patient had medullary thyroid cancer, which had previously been resected. Subsequently, there was no residual disease on cross-sectional imaging or uptake on 68Ga-DOTATATE PET, and plasma tumor markers plus chromogranin A were normal. This was the only false-positive result seen among all 51 patients. Uptake on 68Ga-DOTATATE PET was seen in 14 of the 16 patients with low-grade uptake on 111In-DTPA-octreotide. A total of 101 lesions were identified with cross-sectional imaging in the 15 patients with disease; of these, 71 (70.3%) were identified with 68Ga-DOTATATE PET.
68Ga-DOTATATE PET was false-negative in 1 case, which was an intermediate-grade nonfunctional pancreatic tumor. In this patient, 111In-DTPA-octreotide scintigraphy showed faint uptake in the region of the gallbladder and liver, corresponding to the site of liver metastases.
The sensitivity of 111In-DTPA-octreotide scintigraphy was not determined in view of the bias of the sample population. The specificity of 111In-DTPA-octreotide scintigraphy was 98%, because there was only 1 false-positive result. The sensitivity of 68Ga-DOTATATE PET was 87.2%, and the specificity was 100%.
Lesion Analysis
Evidence of NET disease was identified on cross-sectional imaging in 47 of the 51 patients in this study. A total of 226 lesions were identified with CT ± MRI, whereas 111In-DTPA-octreotide scintigraphy identified 27 lesions and 68Ga-DOTATATE PET identified 168 lesions. 68Ga-DOTATATE PET identified 74.3% of all lesions—significantly more than were identified by 111In-DTPA-octreotide scintigraphy (P < 0.001).
The locations of lesions (according to specific body region) identified by 68Ga-DOTATATE PET and by 111In-DTPA-octreotide scintigraphy were compared (Table 3). Because SPECT was performed only in the region of the chest and abdomen, skeletal metastases may not have been identified on planar imaging. Thirty-six bony lesions were identified by 68Ga-DOTATATE PET and CT ± MRI, of which 28 were in the rib cage or pelvis. Eight bony metastases were identified in the long bones (limbs). The smallest lesion detected on 68Ga-DOTATATE PET was a 6-mm node seen on CT.
68Ga-DOTATATE PET and Histology
Histologic findings were available for all patients. Table 4 shows the number of positive cases in patients with different grades of disease. The results for 111In-DTPA-octreotide are difficult to interpret in view of the patients selected. 68Ga-DOTATATE PET showed good lesion recognition with low-grade tumors. The sensitivity of 68Ga-DOTATATE PET decreased in the more aggressive and poorly differentiated tumors; however, this reduction did not reach significance.
Number of Positive 111In-DTPA-Octreotide Scintigraphy and 68Ga-DOTATATE PET Results in Patients with Different Histologic Grades of Disease
Positive 68Ga-DOTATATE Findings in Conjunction with Initially Negative CT Findings
In 2 cases, patients had undergone initial CT that had been reported as showing normal findings, though it is unclear whether bone windows were reviewed. One patient had normal biochemical markers and the other had raised chromogranin A levels. When these patients underwent 68Ga-DOTATATE PET/CT, the PET portion identified multiple bony metastases; these were found to correspond to sclerotic foci on CT when PET/CT images were reviewed.
Change in Clinical Management
To ascertain whether 68Ga-DOTATATE PET altered the clinical management in patients who had already undergone 111In-DTPA-octreotide scintigraphy, all case notes were reviewed. Changes in clinical management were classified as 1 of the following 4 categories: consideration of 90Y-DOTATATE radiotargeted therapy; suitability for commencement of somatostatin analogs; an alteration of disease stage; and consideration of surgical resection, where this was deemed possible.
Among the 51 patients, management was altered in 36 (70.6%) after 68Ga-DOTATATE PET. Of these 36, 20 were considered suitable for peptide receptor radiotargeted therapy with 90Y-DOTATATE because of the strength of tracer uptake on 68Ga-DOTATATE PET. A further 4 patients with negative results on both 68Ga-DOTATATE and 111In-DTPA-octreotide scanning were excluded from peptide receptor therapy with 90Y-DOTATATE. In 7 patients without functional symptoms but positive for uptake on 68Ga-DOTATATE PET, somatostatin analogs were commenced for their antiproliferative effects.
In 4 patients, surgery was regarded as a possible treatment option because of the presence of limited and resectable disease. In 3 patients, the disease was localized to the abdomen and pelvis, and in 1 patient, the disease was limited to the liver. In these patients, 68Ga-DOTATATE PET changed clinical management by confirming that the disease shown on cross-sectional PET had not been identified on 111In-DTPA-octreotide scintigraphy. Curative resections were performed in 2 patients, and there was no evidence of recurrence at 12 and 14 mo. Another patient underwent surgical debulking of more than 90% of the tumor load, and the remaining disease was stable at 6 mo after surgery. The fourth patient has, to date, been unwilling to undergo surgery and is considering other treatment options.
Finally, in 1 patient with no evidence of disease on CT or biochemically, low-grade uptake in the mediastinum and left lung was observed on the 111In-DTPA-octreotide scan. 68Ga-DOTATATE PET did not reveal any evidence of abnormal uptake, and the patient was regarded as disease-free. In this patient, 68Ga-DOTATATE PET confirmed cross-sectional imaging findings but altered management by finding no evidence of the uptake that had been seen on 111In-DTPA-octreotide scintigraphy.
DISCUSSION
To our knowledge, this study was the first to demonstrate that 68Ga-DOTATATE PET can identify disease in patients with NETs when conventional 111In-DTPA-octreotide findings are negative or show only faint uptake. Furthermore, 68Ga-DOTATATE PET changed the clinical management of 70% of the patients studied.
Although 68Ga-DOTATATE PET identified disease in patients with negative or weakly positive 111In-DTPA-octreotide findings, it did not map the full extent of disease. 68Ga-DOTATATE PET identified 74.3% of lesions documented by conventional cross-sectional imaging. There were individual cases in which some lesions were 68Ga-DOTATATE–avid whereas others were not. These cases illustrate the variable SSTR expression and heterogeneity of NETs, especially with intermediate- and high-grade tumors.
Inherently, PET has spatial resolution superior to that of conventional SPECT. Reubi et al have demonstrated that 68Ga-DOTATATE bound SSTR-2 and other SSTR subtypes with a considerably higher affinity than 111In-DTPA-octreotide (21). The higher affinity of 68Ga-DOTATATE for SSTR-2 may enable smaller lesions to be visualized on PET/CT. It is likely that whole-body SPECT would have identified more lesions, especially skeletal metastases, but whole-body SPECT is neither practical nor comfortable for patients. In areas where 111In-DTPA-octreotide SPECT and 68Ga-DOTATATE PET were performed, the number of lesions detected with PET was greater. It does not appear that lesion size is the only reason for increased lesion detection with 68Ga-DOTATATE PET, compared with 111In-DTPA-octreotide scintigraphy. As demonstrated in Figures 1 and 2, large lesions were identified on 68Ga-DOTATATE PET and not on 111In-DTPA-octreotide SPECT. The 111In-DTPA-octreotide scintigraphy protocol used in this study requires a total scanning time of 50 min to 1 h, which for many patients is the most that can be tolerated. The SPECT protocol in this study is similar to that recommended in other guidelines (22). The speed of whole-body planar images in this study (7.2 cm/min) is faster than that recommended in the SNM guidelines, which suggest a speed of approximately 3 cm/min. The faster image acquisition used in this study may lead to some 111In-DTPA-octreotide–avid lesions not being identified. A second limitation is the delay between 111In-DTPA-octreotide scintigraphy and 68Ga-DOTATATE PET (median time, 4 mo), since new lesions may have developed during the window between scans.
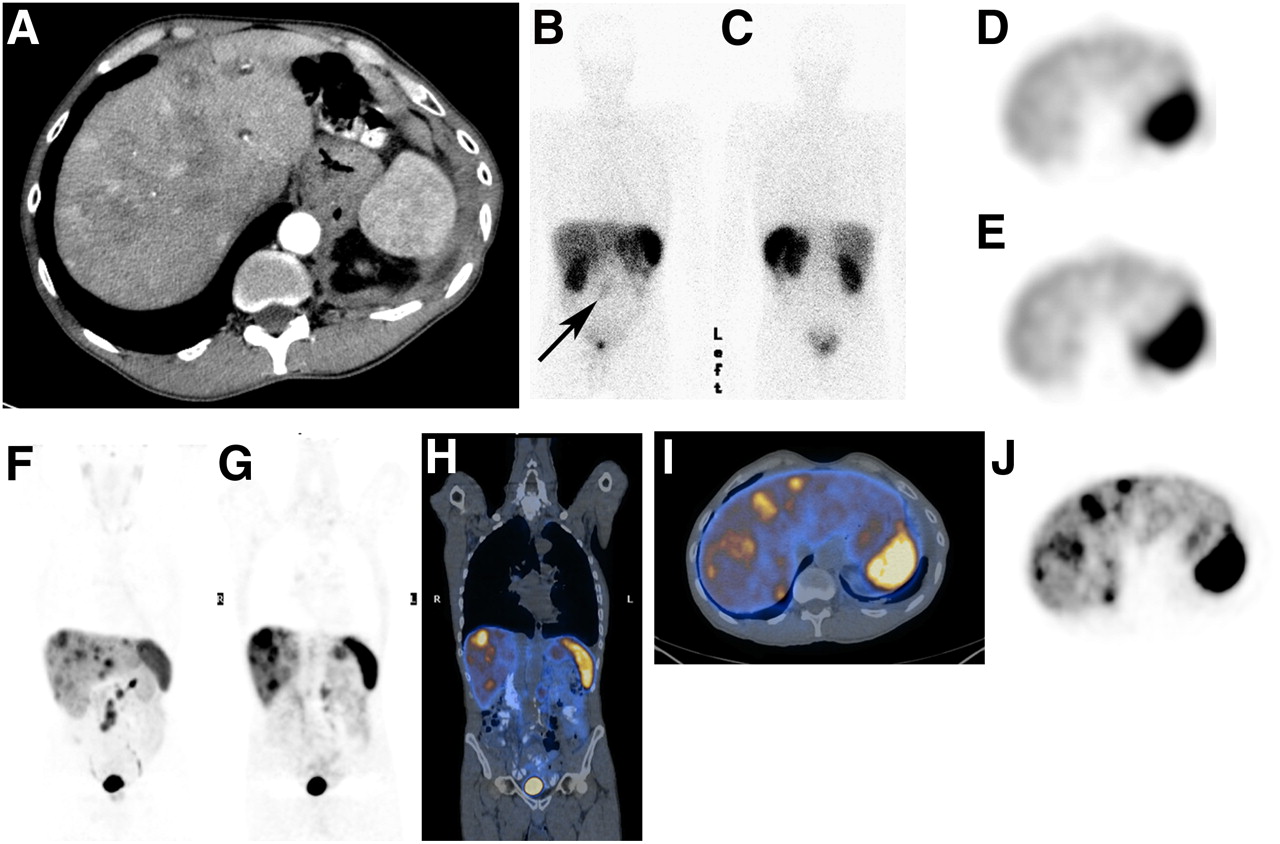
A 42-y-old man with intermediate-grade metastatic midgut NET. (A) Arterial-phase CT at level of splenic hilum shows 2 arterially enhancing liver metastases. (B and C) Anterior and posterior whole-body 111In-DTPA-octreotide scintigraphy shows physiologic uptake only. (D and E) Axial 111In-DTPA-octreotide SPECT at level of spleen shows no discernable liver lesions. (F) Maximum-intensity-projection 68Ga-DOTATATE PET shows liver metastases. (G) Coronal 68Ga-DOTATATE PET shows liver metastases. (H) 68Ga-DOTATATE PET/CT of G. (I) Axial 68Ga-DOTATATE PET/CT shows large metastatic liver deposit. (J) Axial 68Ga-DOTATATE PET shows large metastatic liver deposit.
Studies using 68Ga-DOTATOC PET have also shown higher sensitivity and specificity than 111In-DTPA-octreotide scintigraphy (23). A study by Buchmann et al. on 27 patients demonstrated an increase in lesion identification with PET, compared with 111In-DTPA-octreotide SPECT (13). Another study, by Gabriel et al., with a prospective design, compared 68Ga-DOTATOC PET and 111In-DTPA-octreotide SPECT in 84 patients and found that a significantly higher number of lesions were identified with 68Ga-DOTATOC PET (14).
The purpose of our study was not to directly compare the performance of 111In-DTPA-octreotide scintigraphy and 68Ga-DOTATATE PET but to assess the clinical utility of 68Ga-DOTATATE PET/CT in a specific subset with no uptake or low-grade uptake on 111In-DTPA octreotide scintigraphy. In these patients, we have clearly demonstrated that 68Ga-DOTATATE PET leads to changes in management. The role of 68Ga-DOTATATE PET seems to be similar to that of 111In-DTPA-octreotide scintigraphy, in that its main clinical uses are in localization of disease and assessment of suitability for treatment with somatostatin analogs and radiotargeted therapy.
In our study, 39% of patients were deemed suitable for radiotargeted therapy on the basis of 68Ga-DOTATATE PET findings. No difference in response to peptide receptor therapy was observed between patients who were positive on 68Ga-DOTATATE PET and negative on 111In-DTPA-octreotide scintigraphy, compared with patients who received such therapy on the basis of positive 111In-DTPA-octreotide findings. However, long-term follow-up data are required to confirm this finding.
There is evidence that somatostatin analogs have anti-tumor activity in patients with functional NETs (24). It is postulated that patients with nonfunctional NETs and negative 111In-DTPA-octreotide scintigraphy findings but positive 68Ga-DOTATATE PET findings may well benefit from somatostatin analog therapy.
At the time of primary staging, 68Ga-DOTATATE PET has an important role in the localization of disease, especially in patients who are negative on 111In-DTPA-octreotide imaging. From a surgical perspective, localization of the primary lesion, nodal involvement, and distant metastases is of the greatest importance. Our study has shown the clinical utility of 68Ga-DOTATATE PET in this setting, in that it provides accurate staging of disease.
SSTR expression decreases as the histologic grade of tumor increases, and high-grade tumors have limited SSTR expression (25). In this study, 68Ga-DOTATATE PET had similar sensitivities in identifying disease in low-, intermediate-, and high-grade tumors. For an accurate assessment of the role of 68Ga-DOTATATE PET and 111In-DTPA-octreotide in patients with low-, intermediate- or high-grade tumors, a study looking at unselected NET patients would be of benefit to evaluate the sensitivity, specificity, and accuracy of this tracer. Within the literature, there is evidence that 68Ga-DOTATATE PET is of limited value in patients with intermediate- and high-grade tumors and that 18F-FDG PET may be more suitable in these cases (17).
Other PET tracers have also undergone trials for imaging of NETs, including 11C-5-hydroxytryptophan and 18F-fluoro-l-3,4-dihydroxyphenylalanine. These have shown promising results, with higher detection rates than those achieved with 111In-DTPA-octreotide SPECT and CT (26). However, currently these substrates do not provide any therapeutic options, unlike somatostatin analogs, and therefore have limited clinical roles.
CONCLUSION
68Ga-DOTATATE PET detects 74% of lesions in a selected group of patients with negative or faint uptake (Krenning score, <2) on 111In-DTPA-octreotide scintigraphy and changes the clinical management in 70.6% of these patients
Acknowledgments
This work was undertaken at UCLH/UCL, which received a proportion of the funding from the NIHR Biomedical Research Centers funding scheme of the U.K. Department of Health and the KCL/UCL CCIC. One of the authors is funded by the ECMC at UCLH.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication May 20, 2009.
- Accepted for publication February 17, 2010.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diagnosing metastatic pheochromocytoma: Trick lies in attention to details!
- Safety, tolerability and clinical implementation of 'ready-to-use 68gallium-DOTA0-Tyr3-octreotide (68Ga-DOTATOC) (SomaKIT TOC) for injection in patients diagnosed with gastroenteropancreatic neuroendocrine tumours (GEP-NETs)
- Current Concepts in 68Ga-DOTATATE Imaging of Neuroendocrine Neoplasms: Interpretation, Biodistribution, Dosimetry, and Molecular Strategies
- Most of the Intended Management Changes After 68Ga-DOTATATE PET/CT Are Implemented
- Molecular radiotheranostics for neuroendocrine tumours
- Somatostatin Receptor 2-Targeting Compounds
- The Impact of Somatostatin Receptor-Directed PET/CT on the Management of Patients with Neuroendocrine Tumor: A Systematic Review and Meta-Analysis
- Head-to-Head Comparison of 64Cu-DOTATATE and 68Ga-DOTATOC PET/CT: A Prospective Study of 59 Patients with Neuroendocrine Tumors
- 68Ga-DOTATATE PET/CT Interobserver Agreement for Neuroendocrine Tumor Assessment: Results of a Prospective Study on 50 Patients
- 68Ga-DOTATATE Compared with 111In-DTPA-Octreotide and Conventional Imaging for Pulmonary and Gastroenteropancreatic Neuroendocrine Tumors: A Systematic Review and Meta-Analysis
- Safety and Efficacy of 68Ga-DOTATATE PET/CT for Diagnosis, Staging, and Treatment Management of Neuroendocrine Tumors
- Significance of a Single-Time-Point Somatostatin Receptor SPECT/Multiphase CT Protocol in the Diagnostic Work-up of Gastroenteropancreatic Neuroendocrine Neoplasms
- The Impact of 68Ga-DOTATATE PET/CT Imaging on Management of Patients with Neuroendocrine Tumors: Experience from a National Referral Center in the United Kingdom
- 64Cu-DOTATATE PET for Neuroendocrine Tumors: A Prospective Head-to-Head Comparison with 111In-DTPA-Octreotide in 112 Patients
- Impact of 68Ga-DOTATATE PET/CT on the Management of Neuroendocrine Tumors: The Referring Physician's Perspective
- 18F-Fluorodihydroxyphenylalanine PET/CT in Patients with Neuroendocrine Tumors of Unknown Origin: Relation to Tumor Origin and Differentiation
- Quantitative and Qualitative Intrapatient Comparison of 68Ga-DOTATOC and 68Ga-DOTATATE: Net Uptake Rate for Accurate Quantification
- 123I-BZA2 as a Melanin-Targeted Radiotracer for the Identification of Melanoma Metastases: Results and Perspectives of a Multicenter Phase III Clinical Trial
- Frequency and characterization of gastro-entero-pancreatic neuroendocrine tumor patients with high-grade of uptake at somatostatin receptor scintigraphy
- Comparison of 68Ga-DOTANOC and 68Ga-DOTATATE PET/CT Within Patients with Gastroenteropancreatic Neuroendocrine Tumors
- Unexpected Sensitivity of sst2 Antagonists to N-Terminal Radiometal Modifications
- Clinical PET of Neuroendocrine Tumors Using 64Cu-DOTATATE: First-in-Humans Study
- Radiopeptide Imaging and Therapy in Europe
- PET of Somatostatin Receptor-Positive Tumors Using 64Cu- and 68Ga-Somatostatin Antagonists: The Chelate Makes the Difference
- Therapeutic strategies for advanced neuroendocrine carcinomas of jejunum/ileum and pancreatic origin
- Imaging of Bilateral Neck Paragangliomas with 68Ga-DOTATATE Positron-Emission Tomography/CT