


Abstract
Somatostatin receptor (SSTR) imaging is widely used for guiding the management of neuroendocrine tumor (NET) patients. 68Ga-DOTATATE approval by the U.S. Food and Drug Administration has triggered widespread clinical interest in SSTR PET/CT throughout the United States. Here, we performed a systematic review and meta-analysis to evaluate the impact of SSTR PET/CT on the management of patients with NETs. Methods: A comprehensive literature search was performed using The National Center for Biotechnology Information PubMed online database, applying the following key words: “management” AND “PET” AND “neuroendocrine”. Fourteen of 190 studies were deemed suitable based on the following inclusion criteria: original research, cohort study, number of patients 10 or more, and reported change in management after SSTR PET/CT. Change in management across studies was determined by a random-effects model. Results: A total of 1,561 patients were included. Overall, change in management occurred in 44% (range, 16%–71%) of NET patients after SSTR PET/CT. In 4 of 14 studies, SSTR PET/CT was performed after an 111In-Octreotide scan. In this subgroup, additional information by SSTR PET/CT led to a change in management in 39% (range, 16%–71%) of patients. Seven of 14 studies differentiated between inter- and intramodality changes, with most changes being intermodality (77%; intramodality, 23%). Conclusion: The management was changed in more than one third of patients undergoing SSTR PET/CT even when performed after an 111In-Octreotide scan. Intermodality changes were 3 times more likely than intramodality changes, underlining the clinical impact of SSTR PET/CT.
Neuroendocrine tumors (NETs) emerge from neuroendocrine cells most frequently from the bronchopulmonary or gastrointestinal system (1). Each year an estimated 8,000 individuals are newly diagnosed with NET in the United States, and the annual incidence has increased 5-fold since 1973 (2).
Accurate initial evaluation and detection of recurrence is paramount for all malignancies, including NETs. Traditionally, the diagnostic workup involved morphologic imaging such CT, ultrasonography, or MRI. These resulted in limited detection rates due to a variety of factors such as small size, variable location, and low metabolic rates (3). It was later discovered that well-differentiated NETs express high levels of somatostatin receptor (SSTR), specifically subtype 2 (4). Therefore, in addition to conventional imaging, SSTR-targeted imaging could be applied to detect and functionally characterize NETs.
SSTR scintigraphy using 111In-DTPA-penteoctreotide (Octreoscan) was one of the first tracers developed to functionally image NETs. This probe binds with high affinity to SSTR, specifically subtypes 2 and 5 (5). Although considered a breakthrough at the time, Octreoscan suffered from limited image quality, limited spatial resolution, and prolonged imaging protocols (6). Over the past 2 decades, several chelator-conjugated somatostatin analogs were developed, among these DOTATATE, DOTANOC, and DOTATOC. These short amino acid–chelator conjugates demonstrated an affinity for SSTR superior to that of Octreoscan (7,8). DOTA agents can be labeled with 68Ga, a generator-eluted positron emitter that enables PET imaging and thus provides improved image quality and spatial resolution.
Several studies attest to the superior performance of 68Ga-labeled SSTR PET compared with Octreoscan (9–12). This was recognized recently by the U.S. Food and Drug Administration when it approved 68Ga-DOTATATE (NETSPOT®; Advanced Accelerator Applications) as an imaging agent for the detection of NETs.
Although the diagnostic performance of 68Ga-DOTATATE, 68Ga-DOTATOC, and 68Ga-DOTANOC has been reported in detail (11,13–17), the impact of SSTR PET/CT on patient management has not been reviewed systematically. The aim of this meta-analysis of published data was to determine the impact of SSTR PET/CT on the management of patients with NETs.
MATERIALS AND METHODS
Literature Search
A systematic literature search was performed using The National Center for Biotechnology Information PubMed online database. The following key words were used for selection of studies: “neuroendocrine” AND “PET” AND “management”. A full list of publications obtained with this search strategy is given in the supplemental material (available at http://jnm.snmjournals.org). Fourteen of 190 publications were deemed suitable based on the following inclusion criteria: original research, cohort study, reported change in management after somatostatin receptor imaging, and number of patients 10 or more.
Data Extraction
The following information was extracted from the 14 suitable studies: study type (prospective vs. retrospective), radioligand, sample size, change in management with type of management change (surgical vs. any) and intended versus implemented change, data acquisition method, responding entity, state of disease (primary staging vs. restaging), prior conventional imaging (if applicable), and response rates.
Additionally, treatment changes were extracted from selected studies if the prescan and postscan therapy recommendations were reported. Type of change was classified as inter- versus intramodality. An intermodality change was defined as change in the type of therapy (e.g., surgery to chemotherapy). An intramodality change was defined as change in dose/approach/technique within the suggested treatment modality (e.g., change in surgical strategy).
Statistical Analysis
Descriptive statistics such as mean and SD were used to summarize continuous variables, whereas count and percentage were used for categoric variables. The fixed-effects model approach may not provide proper inference for the dataset; so instead, we performed random-effects models for the overall impact on management for the 14 studies, as well as subgroup analysis with patients undergoing prior Octreoscan. The random-effects model estimates the magnitude of the heterogeneity, and assigns a greater variability to the estimate of overall change in management to account for this heterogeneity (18). Each study is weighted by the inverse of its variance (both for within-studies variance and between-studies variance). Consequently, individual study weights are more balanced, the impact of large trials decreases, and the confidence interval for the combined effect increases in width as compared with the fixed-effects model. Model diagnostics were performed to assess the forest plots with 95% confidence interval (CI). Tests for significance were 2-tailed, with a statistically significant P value threshold of 0.05. Statistical analyses were performed using R version 3.1.3.
RESULTS
Study Characteristics
On systematic review, 14 studies were included. Nine (64%) were retrospective and 5 (36%) were prospective. 68Ga-DOTATATE, 68Ga-DOTATOC, and 68Ga-DOTANOC were used in 8 (57%), 3 (21%), and 3 (21%) studies, respectively. A total of 1,561 participants (737 men, 824 women; mean age, 54 y; age range, 15–86 y) were included. The largest dataset, provided by Skoura et al., analyzed 728 patients retrospectively (19). The largest prospective study, by Sadowski et al. (20), included 130 patients. The remaining 12 studies included 53% of all patients (on average 4% per study). Characteristics of the included studies are presented in Table 1.
Characteristics of Included Trials
Impact on Management
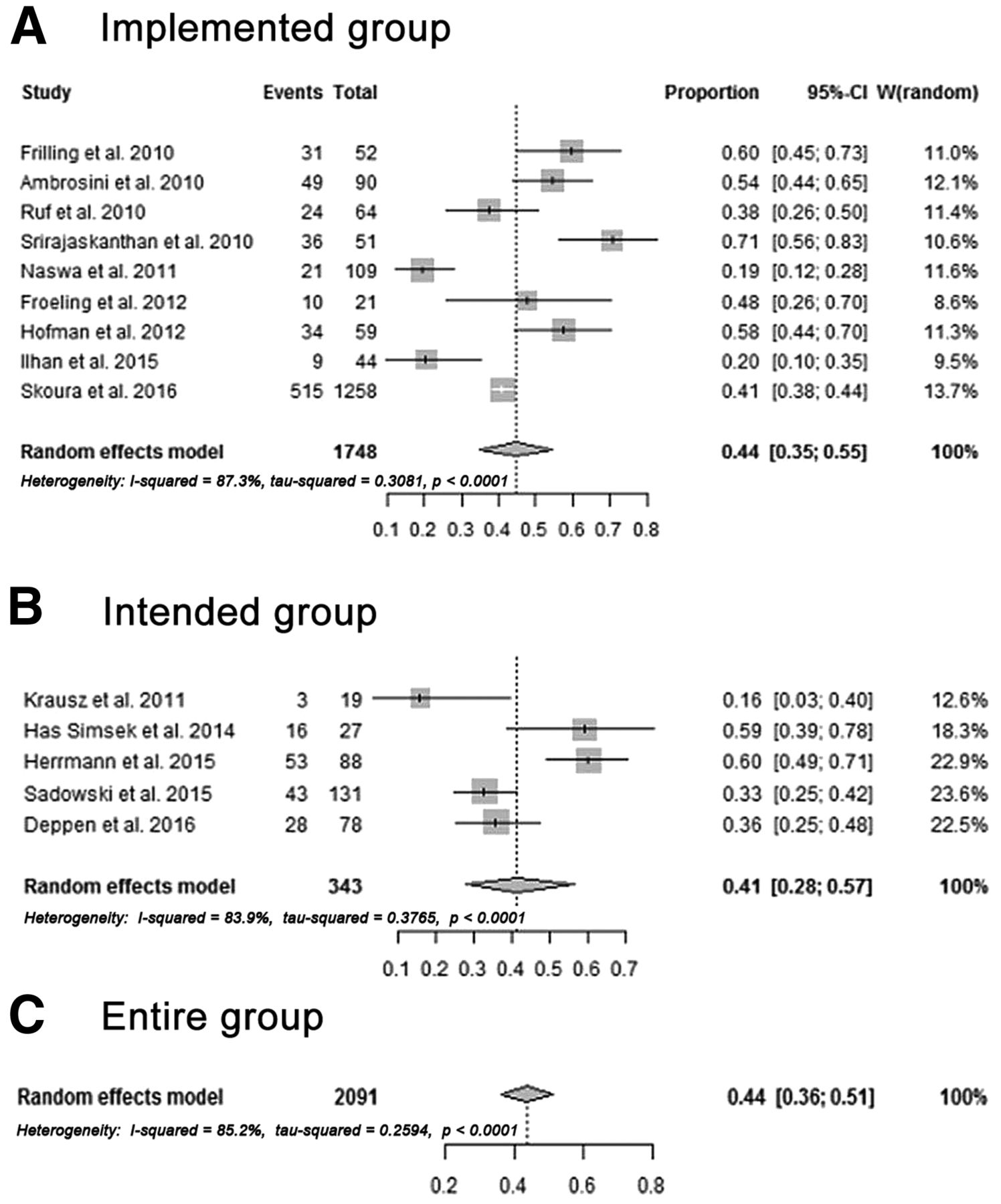
The impact on management for the 14 studies is illustrated in Figures 1A–1C. PET/CT findings resulted in management changes in 44% of the patients (95% CI, 36%–51%; range, 16%–71%; Table 1; Fig. 1C). Studies on implemented management (Fig. 1A, implemented group) reported change in 44% (95% CI, 35%–55%; range, 19%–71%), and studies on intended management (Fig. 1B, intended group) reported change in 41% (95% CI, 28%–57%; range, 16%–60%) of patients.
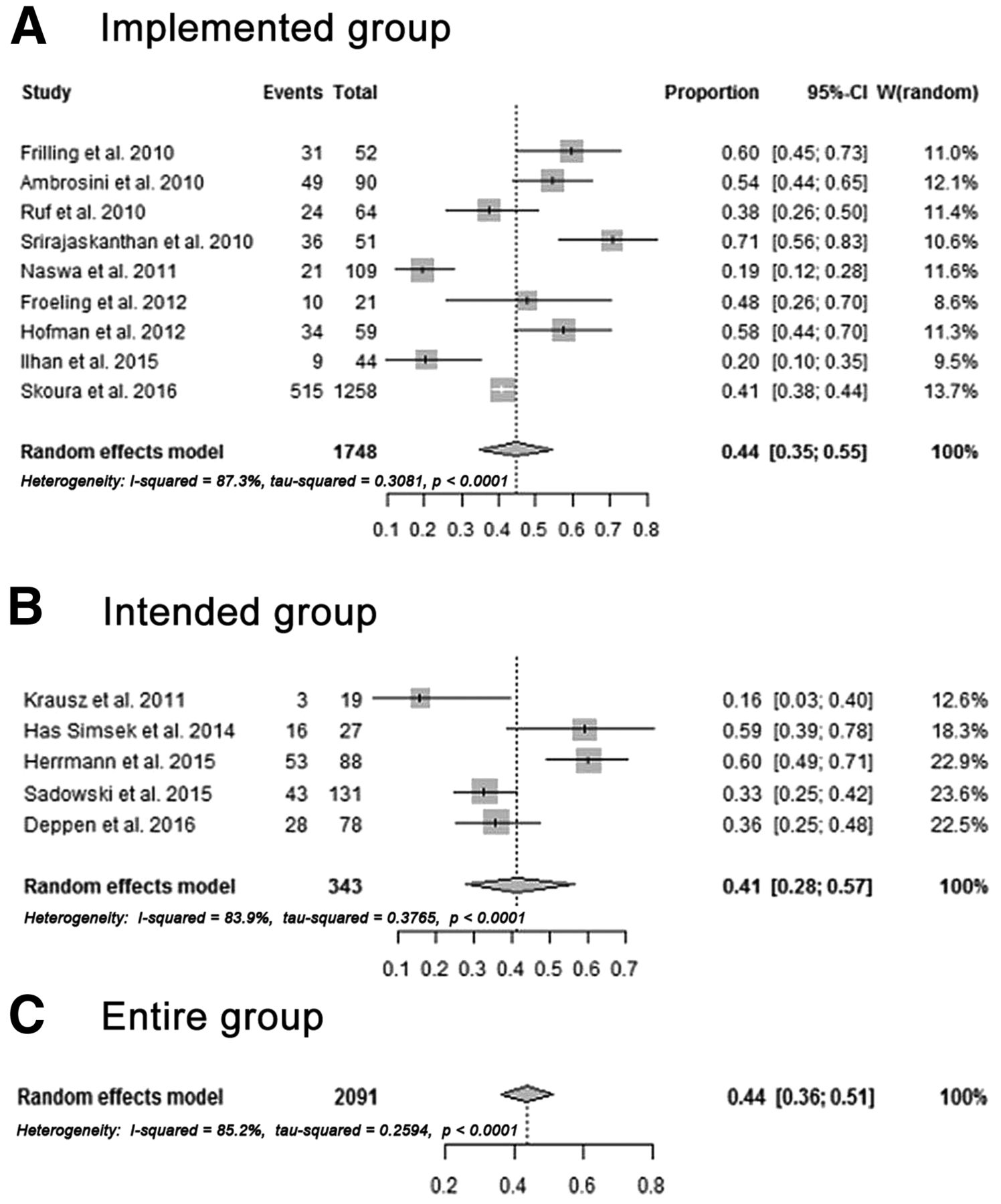
Analysis of change in management separated by implemented (A) and intended (B) changes and for all included studies (C).
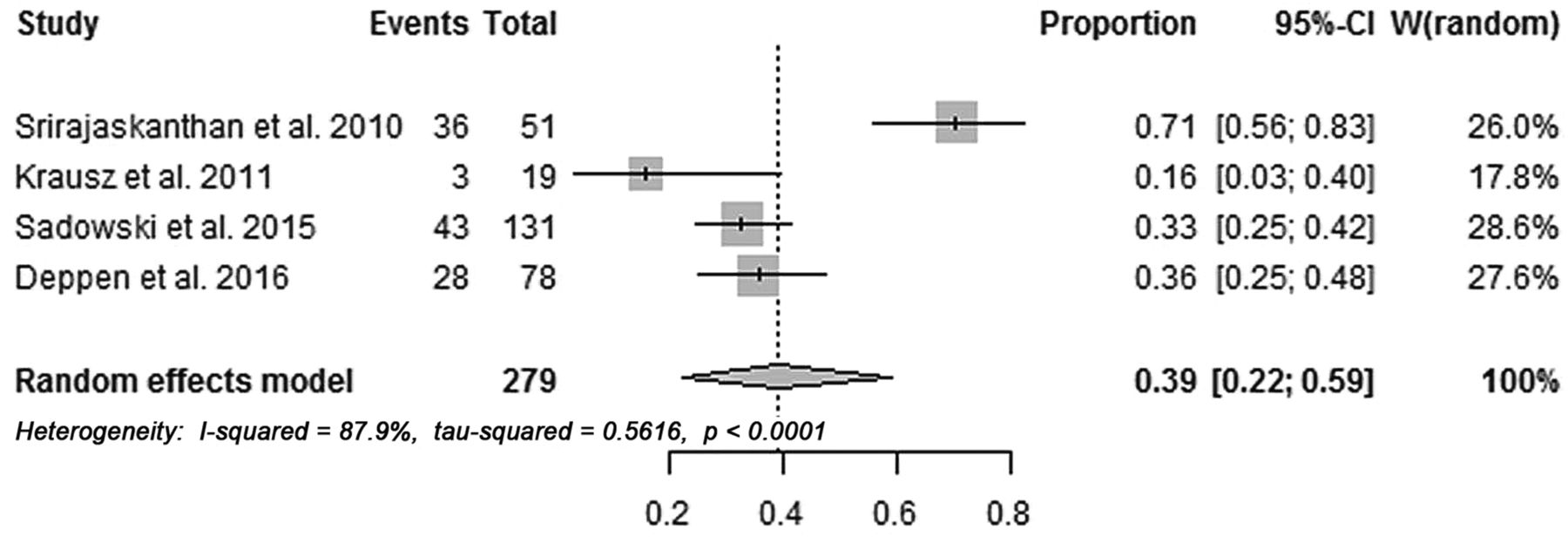
Four studies on 278 patients performed SSTR PET/CT in addition to previous Octreoscan (Table 2) (12,20–22). In this subgroup, an average of 39% of patients (95% CI, 0.22%–0.59%; range, 16%–71%) experienced change in treatment strategy (Fig. 2). Figure 3 demonstrates 68Ga-DOTATATE PET/CT findings in a patient who underwent a previous Octreoscan (23).
Change in Management in Patients with Prior Octreoscan

Subgroup analysis of patients who underwent Octreoscan before SSTR PET/CT.
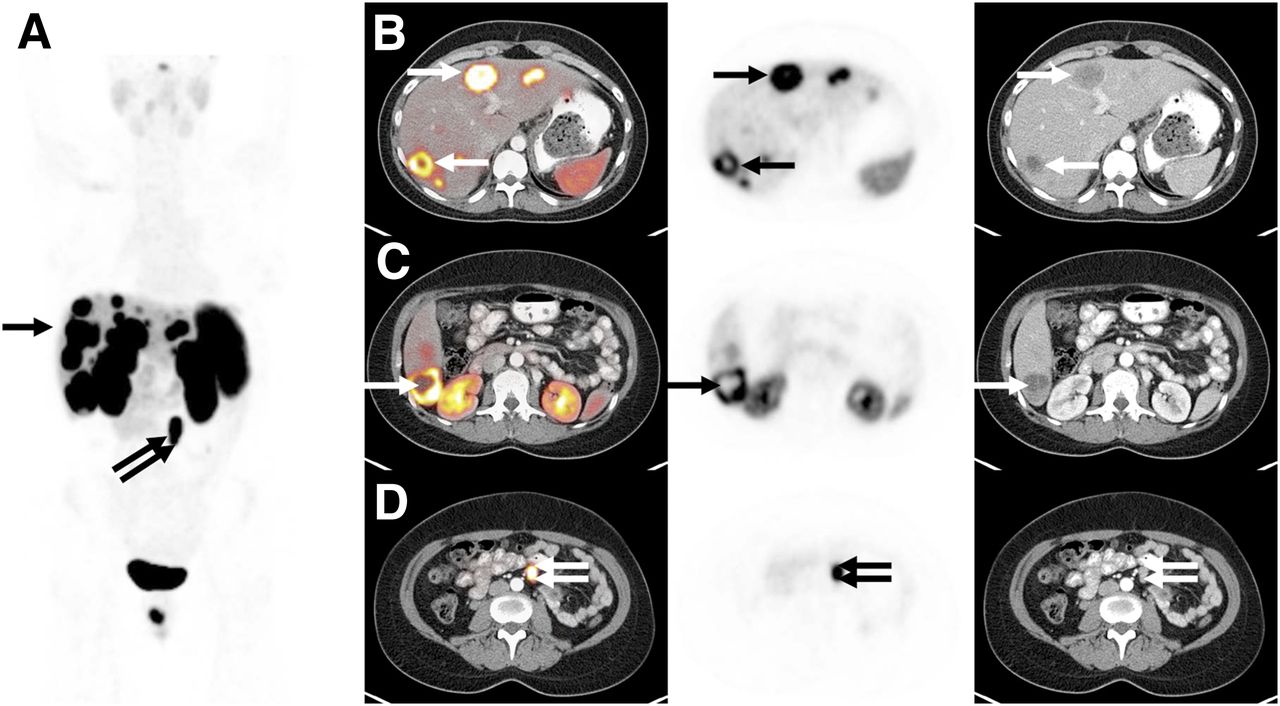
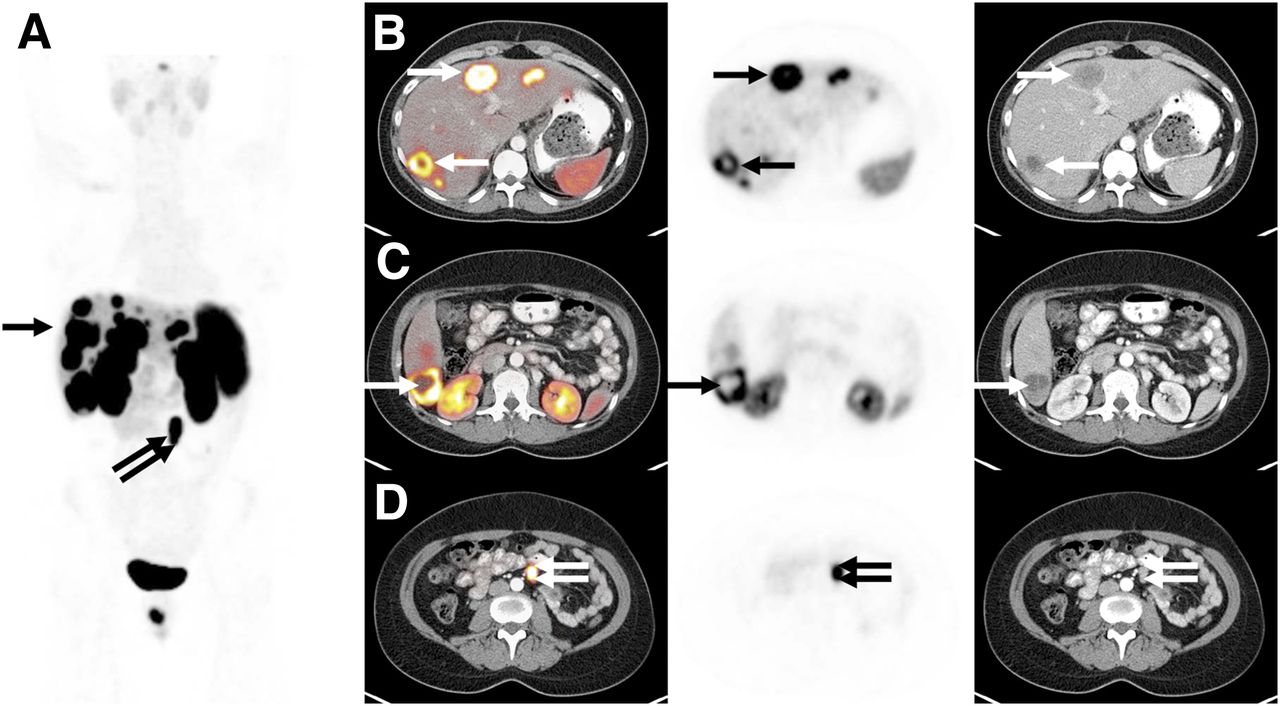
A 38-y-old female patient with metastatic NET of unknown primary. Octreoscan revealed SSTR-positive liver metastases. No extrahepatic disease was noted. Intended management was somatostatin-analog therapy. Maximum-intensity projection (A) and axial images of 68Ga-DOTATATE PET/CT performed 2 mo after Octreoscan are shown. PET/CT revealed numerous liver lesions (rows B and C) with intense tracer uptake (arrow). In addition, left mesenteric mass was discovered (row D, double arrow), which was later confirmed to be small bowel primary. Surgery for small bowel primary and initiation of somatostatin-analog therapy was implemented 2 mo after 68Ga-DOTATATE PET/CT scanning.
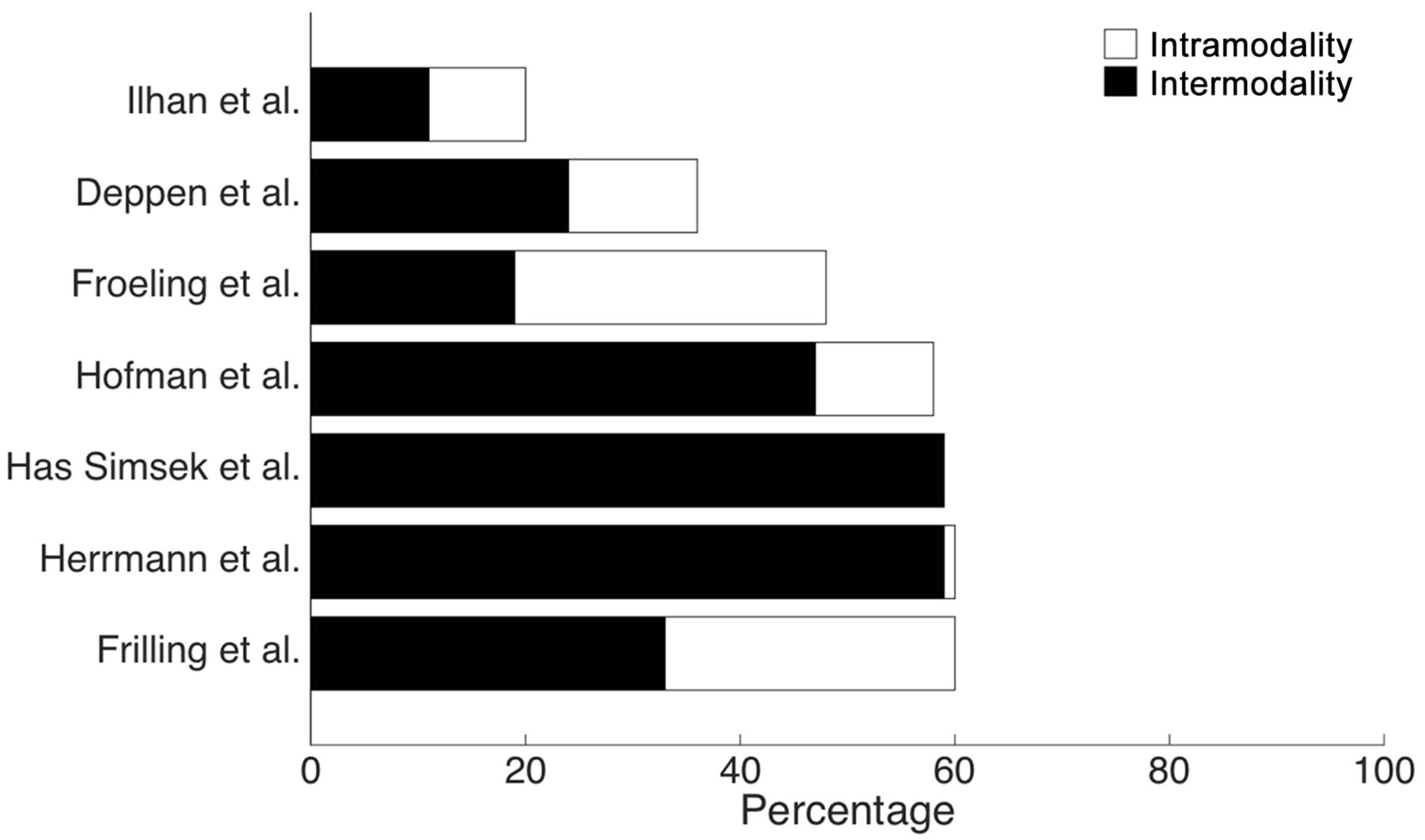
Type of management change (inter- vs. intramodality) was documented in 7 of 14 (50%) studies. Overall, intermodality changes (77%) occurred more than 3 times more frequently than intramodality changes (23%) (Fig. 4; Table 3).

Type of change was differentiated in 7 of 14 (50%) studies. Bars represent proportion of patients with any change in management, separated by subgroups with intermodality (black) vs. intramodality (white) change.
Intermodality Versus Intramodality Management Change
DISCUSSION
This article provides a systematic analysis of the impact of SSTR PET/CT on the management in patients with NETs. Management changes were seen in 44% of all patients. No significant difference in the rate of management change was seen among reports of intended (41%) versus implemented (44%) management change. Management was also changed in 39% of those patients who had undergone a previous Octreoscan. Finally, intermodality management changes occurred 3 times more frequently than intramodality changes.
The superior diagnostic performance of SSTR PET/CT as compared with Octreoscan has led to the recent U.S. Food and Drug Administration approval of 68Ga-DOTATATE as an imaging agent for NET. Three clinical studies were highlighted in the prescribing information of 68Ga-DOTATATE: 2 trials demonstrated high accuracy using histopathology or clinical follow-up for lesion verification (24,25), and 1 trial demonstrated safety and significant change in management in a head-to-head comparison with Octreoscan (22).
Impact on management is a prerequisite for acceptance of diagnostic tests by physicians and insurance companies. Centers for Medicare and Medicaid Services requested data on the impact of 18F-FDG PET/CT on clinical management to recommend reimbursement. This was evaluated in the National Oncologic PET Registry that enrolled thousands of patients and demonstrated intended management changes in around 40% of patients with a variety of cancers (26). Intermodality changes were 2 times more likely than intramodality changes (26). National Oncologic PET Registry findings led to wide coverage of 18F-FDG PET/CT by the Centers for Medicare and Medicaid Services. The degree of impact of 18F-FDG PET/CT is comparable to that of SSTR PET/CT regarding overall management changes (>40%); however, the rate of intermodality/major changes was higher for SSTR PET/CT (26).
The proportion of patients experiencing a change in management was similar in studies that reported intended (41%) versus implemented (44%) changes. This suggests that trials with intended endpoints do not suffer from low rates of implementation and underlines the validity of such endpoints. The additional value of SSTR PET/CT is robust and unaffected by previous SSTR scintigraphy. Thirty-nine percent of patients who had undergone a previous Octreoscan experienced treatment changes, highlighting the clinical impact of the more advanced PET/CT versus scintigraphy technology. Advantages also include the practicability of a 2-h PET/CT versus 2-d Octreoscan protocol, which was not analyzed by this meta-analysis.
Other limitations of this study should be noted: as with most meta-analyses, included articles were heterogeneous. Specifically, the definition of actual “change in management” varied from study to study. On the other hand, most of the included studies focused on implemented changes (9/14, 64%), and findings for the proportion of patients experiencing change in management were similar across all subgroups (average, 39%–44%). Skoura et al. (19) provided about half (728/1,561, 47%) of all the patients included in this study. Even though the change reported by Skoura et al. was well in range with results for the entire cohort, a random-effects model was used for analysis to avoid undue impact of this large trial.
CONCLUSION
Our systematic analysis demonstrates that PET/CT imaging using 68Ga-DOTATATE, 68Ga-DOTATOC, or 68Ga-DOTANOC is vital for patient management. Change occurred in similar magnitude when compared with the National Oncologic PET Registry multicenter trial resulting in 18F-FDG PET/CT reimbursement.
SSTR PET allows sensitive tumor detection. On the basis of its accuracy, SSTR PET/CT is the standard of care in Europe, incorporated into clinical guidelines, and recently received approval in the United States for the evaluation of NET. SSTR radioligands further serve as predictive biomarkers to confirm target receptor expression and identify patients suitable for 177Lu-DOTATATE peptide receptor radionuclide therapy, currently under expanded access. This systematic analysis demonstrates that accuracy translates into change in clinical management, underlining the importance of SSTR PET/CT implementation into the routine care of NET patients.
DISCLOSURE
This study was partially funded by the U.S. Department of Energy, Office of Science Award DE-SC0012353. Wolfgang P. Fendler received a scholarship from the German Research Foundation (Deutsche Forschungsgemeinschaft, DFG). Ken Herrmann and Wolfgang P. Fendler are consultants of Ipsen and have a research agreement with Advanced Accelerator Applications (AAA). No other potential conflict of interest relevant to this article was reported.
Footnotes
Guest Editor: Michael M. Graham, University of Iowa.
Published online Jan. 12, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 14, 2016.
- Accepted for publication December 5, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Role of Total-Body PET in Drug Development and Evaluation: Status and Outlook
- Identifying secondary findings in PET/CT reports in oncological cases: A quantifying study using automated Natural Language Processing
- Choice Is Good at Times: The Emergence of [64Cu]Cu-DOTATATE-Based Somatostatin Receptor Imaging in the Era of [68Ga]Ga-DOTATATE
- A Randomized, Factorial Phase II Study to Determine the Optimal Dosing Regimen for 68Ga-Satoreotide Trizoxetan as an Imaging Agent in Patients with Gastroenteropancreatic Neuroendocrine Tumors
- Mars Shot for Nuclear Medicine, Molecular Imaging, and Molecularly Targeted Radiopharmaceutical Therapy
- 64Cu-DOTATATE PET/CT for Imaging Patients with Known or Suspected Somatostatin Receptor-Positive Neuroendocrine Tumors: Results of the First U.S. Prospective, Reader-Masked Clinical Trial
- A Prospective Observational Study to Evaluate the Effects of Long-Acting Somatostatin Analogs on 68Ga-DOTATATE Uptake in Patients with Neuroendocrine Tumors
- 68Ga-FAPI PET/CT: Tracer Uptake in 28 Different Kinds of Cancer
- Safety, Pharmacokinetics, and Dosimetry of a Long-Acting Radiolabeled Somatostatin Analog 177Lu-DOTA-EB-TATE in Patients with Advanced Metastatic Neuroendocrine Tumors
- Aetna and 68Ga-DOTATATE: A Sequel to "The Injustice of Being Judged by the Errors of Others" (1)
- Appropriate Use Criteria for Somatostatin Receptor PET Imaging in Neuroendocrine Tumors
- Most of the Intended Management Changes After 68Ga-DOTATATE PET/CT Are Implemented