


Abstract
Radiolabeled somatostatin analog therapy has become an established treatment method for patients with well to moderately differentiated unresectable or metastatic neuroendocrine tumors (NETs). The most frequently used somatostatin analogs in clinical practice are octreotide and octreotate. However, both peptides showed suboptimal retention within tumors. The aim of this first-in-humans study is to explore the safety and dosimetry of a long-acting radiolabeled somatostatin analog, 177Lu-1, 4, 7, 10-tetra-azacyclododecane-1, 4, 7, 10-tetraacetic acid-Evans blue-octreotate (177Lu-DOTA-EB-TATE). Methods: Eight patients (6 men and 2 women; age range, 27–61 y) with advanced metastatic NETs were recruited. Five patients received a single dose, 0.35–0.70 GBq (9.5–18.9 mCi), of 177Lu-DOTA-EB-TATE and underwent serial whole-body planar and SPECT/CT scans at 2, 24, 72, 120, and 168 h after injection. The other 3 patients received intravenous injection of 0.28–0.41 GBq (7.5–11.1 mCi) of 177Lu-DOTATATE for the same imaging acquisition procedures at 1, 3, 4, 24, and 72 h after injection. The dosimetry was calculated using the OLINDA/EXM 1.1 software. Results: Administration of 177Lu-DOTA-EB-TATE was well tolerated, with no adverse symptoms being noticed or reported in any of the patients. Compared with 177Lu-DOTATATE, 177Lu-DOTA-EB-TATE showed extended circulation in the blood and achieved a 7.9-fold increase of tumor dose delivery. The total-body effective doses were 0.205 ± 0.161 mSv/MBq for 177Lu-DOTA-EB-TATE and 0.174 ± 0.072 mSv/MBq for 177Lu-DOTATATE. Significant dose delivery increases to the kidneys and bone marrow were also observed in patients receiving 177Lu-DOTA-EB-TATE compared with those receiving 177Lu-DOTATATE (3.2 and 18.2-fold, respectively). Conclusion: By introducing an albumin-binding moiety, 177Lu-DOTA-EB-TATE showed remarkably higher uptake and retention in NETs as well as significantly increased accumulation in the kidneys and red marrow. It has great potential to be used in peptide receptor radionuclide therapy for NETs with lower dose and less frequency of administration.
- peptide receptor radionuclide therapy (PRRT)
- somatostatin receptor (SSTR)
- neuroendocrine tumor (NET)
- Evans blue
- TATE
Because of the body-wide distribution of neuroendocrine cells, neuroendocrine tumors (NETs) are a heterogeneous group of neoplasms that can develop anywhere in the body (1). Although NETs are generally categorized as low-grade indolent tumors and other epithelial malignancies, they can be aggressive and resistant to therapy (2). Most NETs overexpress somatostatin receptors (SSTRs), so somatostatin analogs are recommended for unresectable and metastatic disease (3). However, the clinical efficacy is relatively limited (4,5).
For decades, diagnostic radioisotope-labeled somatostatin analogs have been intensively investigated for NET imaging (6). With therapeutic radioisotopes such as 90Y or 177Lu, peptide receptor radionuclide therapy (PRRT) has become an established treatment for patients with well to moderately differentiated unresectable or metastatic NETs and disease progression after first-line treatment (7). Several phase I and II clinical trials showed favorable results in NETs in general and even better results in patients with gastroenteropancreatic NETs and bronchial NETs, where as much as 30% objective response was observed (8). In a recently finished phase III clinical trial, a treatment with 177Lu-DOTATATE resulted in markedly longer progression-free survival and a significantly higher response rate than high-dose octreotide long-acting repeatable (LAR) among patients with advanced midgut NETs (9). The promising results from this trial led to the approval of Lutathera (177Lu-DOTATATE) by both the European Commission and the U.S. Food and Drug Administration for the treatment of gastroenteropancreatic NETs.
For PRRT, kidneys are usually the critical organs in terms of radiation toxicity due to nonspecific or specific accumulation of radiolabeled peptide, and maximum tolerated dose to kidney is in the range of 23–29 Gy (10–12). Renal irradiation is mainly caused by reabsorption of radiolabeled peptides in the proximal tubule. SSTR also plays a role in the total renal uptake of radiolabeled somatostatin analogs (13), because vasa recta, tubular cells of the cortex, and distal tubule cells express SSTR (14,15). The fast clearance of the peptide also affects the accumulation of radioactivity within the tumor, which means radiolabeled DOTATATE needs to be given by adding intravenous infusion dose and treatment cycles.
As the most abundant plasma protein, serum albumin has emerged as a versatile carrier for therapeutic agents (16,17). For example, a DOTA–folate conjugate with a low-molecular-weight albumin-binding entity 4-(p-iodophenyl)butyric acid has been designed to prolong its circulation in the blood, leading to improved tumor-to-kidney ratios (18). The same albumin-binding-entity–conjugated prostate-specific membrane antigen (PSMA) inhibitor also showed an increased circulation half-life and prostate tumor uptake, compared with the unmodified PSMA inhibitors (19,20). Recently, an Evans blue–based albumin-binding moiety was developed as a blood-pool imaging and lymphatic mapping agent (21–25) and also for modification of peptides, oligonucleotides, and chemotherapeutic drugs (26–28). We also developed a long-acting somatostatin analog (EB-TATE), with the aim to improve the pharmacokinetics and increase therapeutic efficacy (29). In a SSTR2-positive AR42J xenograft model, 90Y-DOTA-EB-TATE effectively accumulated in the tumor, resulting in complete regression of the tumors and full survival of the tumor-bearing mice with a single low dose of 3.7 MBq of 90Y-DOTA-EB-TATE (29).
Inspired by the promising preclinical results, we conducted a first-in-humans, first-in-class study to explore the safety, tolerability, and dosimetry and preliminary effects of administration of the study drug 177Lu-DOTA-EB-TATE in 5 patients with advanced metastatic NETs. For comparison, 177Lu-DOTA-TATE was evaluated in another 3 patients.
MATERIALS AND METHODS
Patient Recruitment
This is a noncontrolled, nonrandomized, nonblinded first-in-humans study, which was approved by the Institutional Review Board of Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College. This study was registered at clinicaltrials.gov (NCT03308682). All procedures were in accordance with the ethical standards of the institutional and national research committees and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. A total of 8 patients with metastatic SSTR-expressing NETs were enrolled at Peking Union Medical College Hospital, Beijing.
The inclusion criteria were adult patients with histologically confirmed, metastasized NETs; the tumors being unresectable; identified disease progression according to RECIST (version 1.1); confirmed SSTR expression on the target tumors; and at least one lesion with higher uptake than that of normal liver parenchyma on 68Ga-DOTATATE PET. The exclusion criteria were any of the following: serum creatinine level greater than 150 μM; baseline measured glomerular filtration rate of less than 50 mL/min/1.73 m2 determined by 99mTc-DTPA renal function examination; hemoglobin level of less than 8.0 g/dL; white-cell count less than 2.0 × 109/L; platelet count of less than 75 × 109/L; total bilirubin level of greater than 3 times the upper limit of the normal range and serum albumin level of less than 3.0 g/dL; cardiac insufficiency including carcinoid heart valve disease, severe allergy, or hypersensitivity to radiographic contrast material; claustrophobia; and pregnancy or breastfeeding.
PET Procedures
All patients underwent 68Ga-DOTATATE PET/CT scans using a Siemens Biograph 64 True Point system. The emission sequence was initiated at approximately 45 min after intravenous injection of 111–148 MBq (3–4 mCi) of 68Ga-DOTATATE. A Siemens MMWP workstation was used for postprocessing.
Radiopharmaceuticals
DOTA-EB-TATE was synthesized according to the procedure reported previously (29). Good-manufacturing-practices–certified, no-carrier-added 177Lu, in the form of 177LuCl3, was purchased from LuMark (IDB, Holland). The radiosynthesis was automated on an All-In-One synthesizer. The product (radiochemical purity > 98%) was dissolved in 0.9% saline and passed through a 0.22-μm filter to ensure sterility. The quality control was performed with thin-layer chromatography (BIOSCAN) with CH3OH:NH4OAc (v/v 1:1) as the developing solution.
SPECT/CT
No fasting, special diet, hydration, or other specific preparation was requested on the day of 177Lu-DOTA-EB-TATE or 177Lu-DOTATATE injection. Before the injection and 24 h later, safety data were collected, including physical examination and vital signs, electrocardiography parameters, blood count, biochemistry, and immunology. Any unusual or adverse clinical symptoms were recorded on the day of imaging and during the 3-mo follow-up. Safety data were also measured at 5 d and 1, 2, 4, and 8 wk after the tracer administration. Renal protection was performed using amino acid infusion to hydrate the patients. Before the amino acid infusion, tropisetron hydrochloride was applied to prevent nausea and vomiting. Amino acid infusion (2.5%; 25 g of arginine diluted in 1 L of normal saline) was started 1 h before administration of 177Lu-DOTA-EB-TATE or 177Lu-DOTATATE and maintained over 4 h.
Five patients underwent single-dose administration of 177Lu-DOTA-EB-TATE (0.35–0.70 GBq [9.5–18.9 mCi]), followed by serial whole-body planar and SPECT/CT scans at 2, 24, 72, 120, and 168 h after injection. Another 3 patients accepted intravenous injection of 0.28–0.41 GBq (7.5–11.1 mCi) of 177Lu-DOTA-TATE for the same imaging acquisition procedures at 1, 3, 4, 24, and 72 h after injection. All scans were obtained using a Precedence scanner (Philips Healthcare) with a medium-energy general-purpose collimator and a 20% energy window width centered symmetrically over the 208-keV photopeak of 177Lu.
The whole-body images were acquired with the camera configured for dual-head planar imaging with a 256 × 1,024 matrix at a scan speed of 10 cm/min. SPECT/CT scanning was performed after each whole-body scintigraphy, with each tomographic scan of 32 frames with a 40 sec exposure time per frame (21-min SPECT acquisition time) including all major organs after a low-dose CT scan.
SPECT reconstruction was performed using the system’s software on the clinical workstation. An iterative ordered-subset maximum-likelihood expectation maximization algorithm with 3 iterations and 8 subsets was used. Visual analysis was used to determine the general biodistribution and the temporal and intersubject stability. Regions of interest were drawn including the organs and NET lesions on the serial images.
Dosimetry Calculation
The dosimetry calculation was performed according to the European Association of Nuclear Medicine Dosimetry Guidance (30) and the procedure reported previously (23). A radioactive source with a well-determined 177Lu activity at a fixed position near the top of head on whole-body planar images was used to calculate dose concentration factor, and voxel-based activity concentration was converted to SUV in the volumes of interest. The decay uncorrected time–activity curve was generated based on the SUV of each organ. The SUVs were then converted to MBq/MBq on the basis of organ weight from the adult male phantom and the adult female phantom provided by the OLINDA/EXM (version 1.1; Vanderbilt University, USA) (31,32). The time-integrated activity coefficient of each organ was determined by fitting the data using a biphase exponential model provided by the software. The residence times of the urine bladder and NETs were calculated by the trapezoidal method using GraphPad Prism (version 4.0; GraphPad Software, Inc.). The void time was set as 60 min. The volume of left ventricle was set as 550 mL to calculate the residence of heart content. The ratio of activity mass concentrations for red marrow to blood was set as 0.32 to calculate dose delivery to bone marrow (33). The effective doses were calculated by entering the time-integrated activity coefficient for all source organs into OLINDA/EXM for either a 73.7 kg adult male or a 56.9 kg adult female. All the data were expressed as mean ± SD.
RESULTS
Safety Profile
All patient information is included in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org). With a mean injected dose of 0.632 ± 0.079 GBq (17.08 ± 2.14 mCi) of 177Lu-DOTA-EB-TATE or 0.28–0.41 GBq (7.5–11.1 mCi) of 177Lu-DOTA-TATE, no subjective side effects were experienced, and no adverse symptoms were noticed or reported. No clinically significant changes on physical examination, electrocardiography parameters, blood count, biochemistry, and immunology during the entire 7-d procedure and 3-mo follow-up in any of the patients were found.
Pharmacokinetics Profile
At 2 h after injection, 177Lu-DOTA-EB-TATE showed a relatively high level in the blood, as indicated by the strong signal in the heart region and major vessels (Fig. 1A). Among normal organs, liver, spleen, and kidneys showed moderate uptake of 177Lu-DOTA-EB-TATE. 177Lu-DOTATATE also showed moderate uptake in the liver, spleen, and kidneys, but no apparent uptake in the blood circulation was detected (Fig. 1B). Both agents showed negative brain uptake. On the basis of the quantitative data summarized in Table 1, 177Lu-DOTA-EB-TATE showed a much higher retention in the blood (SUV, 1.75 ± 0.58) than 177Lu-DOTATATE (SUV, 0.09 ± 0.03) at 24 h after injection (P < 0.01). The uptake of 177Lu-DOTA-EB-TATE in the lung, liver, kidneys, and muscle was also higher than those of 177Lu-DOTA-TATE. The uptake in the spleen was similar for the 2 agents.

(A) Representative whole-body anterior projection images of a 61-y-old male patient with NET liver metastases at 2, 24, 72, 120, and 168 h after intravenous administration of 177Lu-DOTA-EB-TATE. 177Lu-DOTA-EB-TATE cleared from blood pool over time and persistently accumulated in tumors. (B) Representative whole-body anterior projection images of a 49-y-old male patient with NET liver metastases at 1, 3, 4, 24, and 72 h after intravenous administration of 177Lu-DOTATATE. 177Lu-DOTATATE showed rapid renal clearance. Tumor uptake also gradually decreased along with time.
Biodistribution of 177Lu-DOTA-EB-TATE (SUV, n = 5) and 177Lu-DOTATATE (SUV, n = 3) in Patients with Advanced NETs
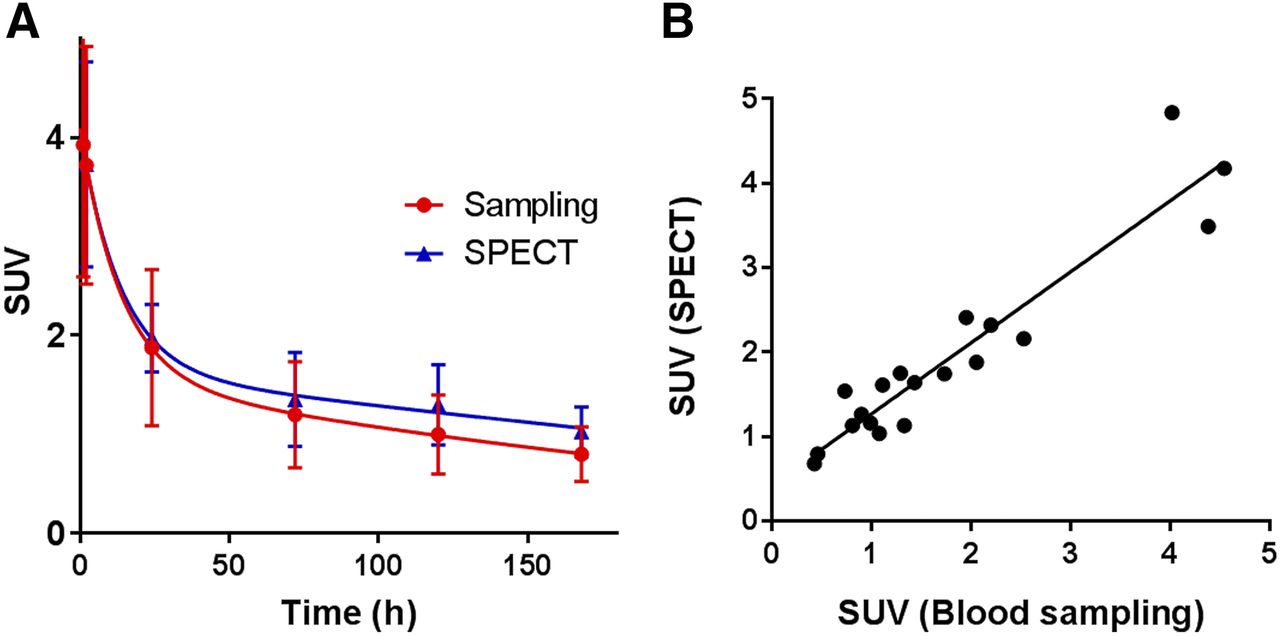
To confirm the accuracy of SPECT quantification, blood samples were collected from the patients at different time points after TATE injection, and radioactivity within the blood samples was quantified using a γ-counter. A positive and significant correlation between SPECT quantification and blood sampling was observed (R2 = 0.90, P < 0.0001, Fig. 2).
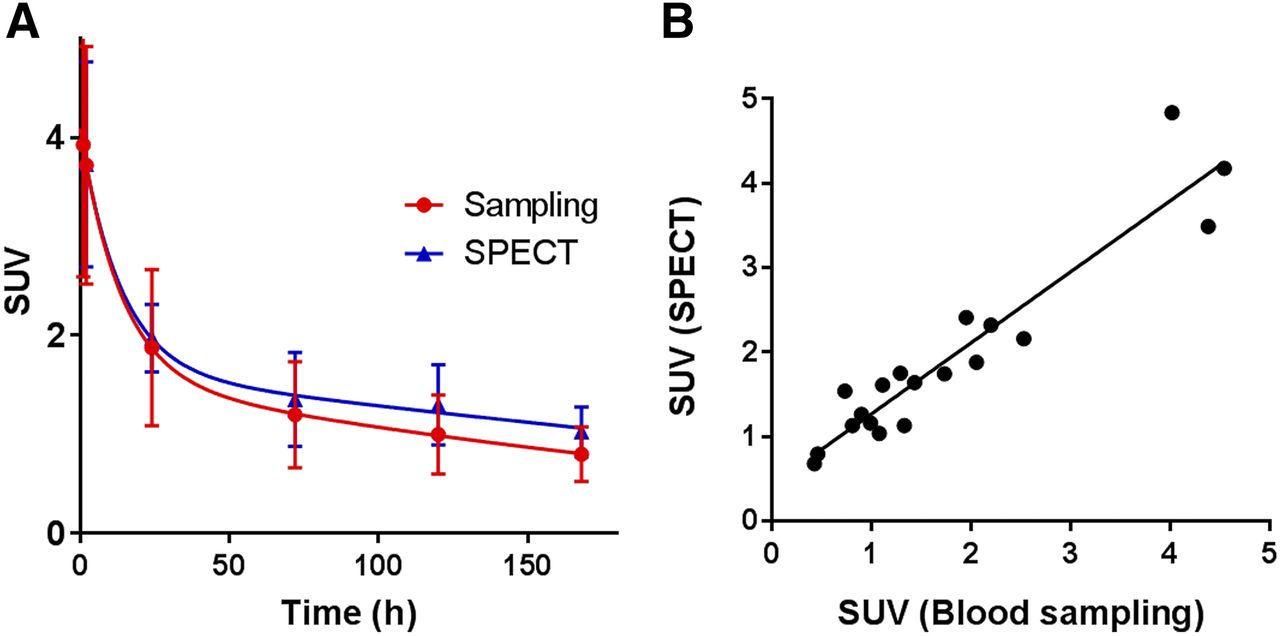
(A) Blood clearance of 177Lu-DOTA-EB-TATE quantified by SPECT and γ-counting of blood samples. (B) There is positive linear correlation between SPECT quantification and blood sampling (R2 = 0.90, P < 0.0001).
Normal Organ Dosimetry
On the basis of the quantification of SPECT images, dosimetry was calculated using OLINDA/EXM software (Table 2). As to the whole-body effective dose, there was no significant difference between 177Lu-DOTA-EB-TATE and 177Lu-DOTATATE (0.080 ± 0.05 vs. 0.069 ± 0.032 mSv/MBq, P > 0.05). The spleen was the organ that received the highest absorbed dose for both agents, with 1.45 ± 1.59 mSv/MBq for 177Lu-DOTA-EB-TATE and 1.77 ± 0.95 mSv/MBq for 177Lu-DOTATATE, respectively. 177Lu-DOTA-EB-TATE had a significantly higher effective dose in the kidneys than 177Lu-DOTATATE (1.15 ± 0.92 vs. 0.36 ± 0.07 mSv/MBq, P < 0.01). 177Lu-DOTA-EB-TATE also showed higher exposure to red bone marrow than 177Lu-DOTATATE (0.058 ± 0.014 vs. 0.0032 ± 0.0004 mSv/MBq, P < 0.01). 177Lu-DOTATATE showed higher exposure to pancreas and urinary bladder wall than 177Lu-DOTA-EB-TATE.
Estimated Effective Dose After Intravenous Administration of 177Lu-NOTA-EB-TATE (n = 5, 4 Men and 1 Woman) and 177Lu-DOTATATE (n = 3, 2 Men and 1 Woman)
Dose Delivery of 177Lu-DOTA-EB-TATE to NET Lesions
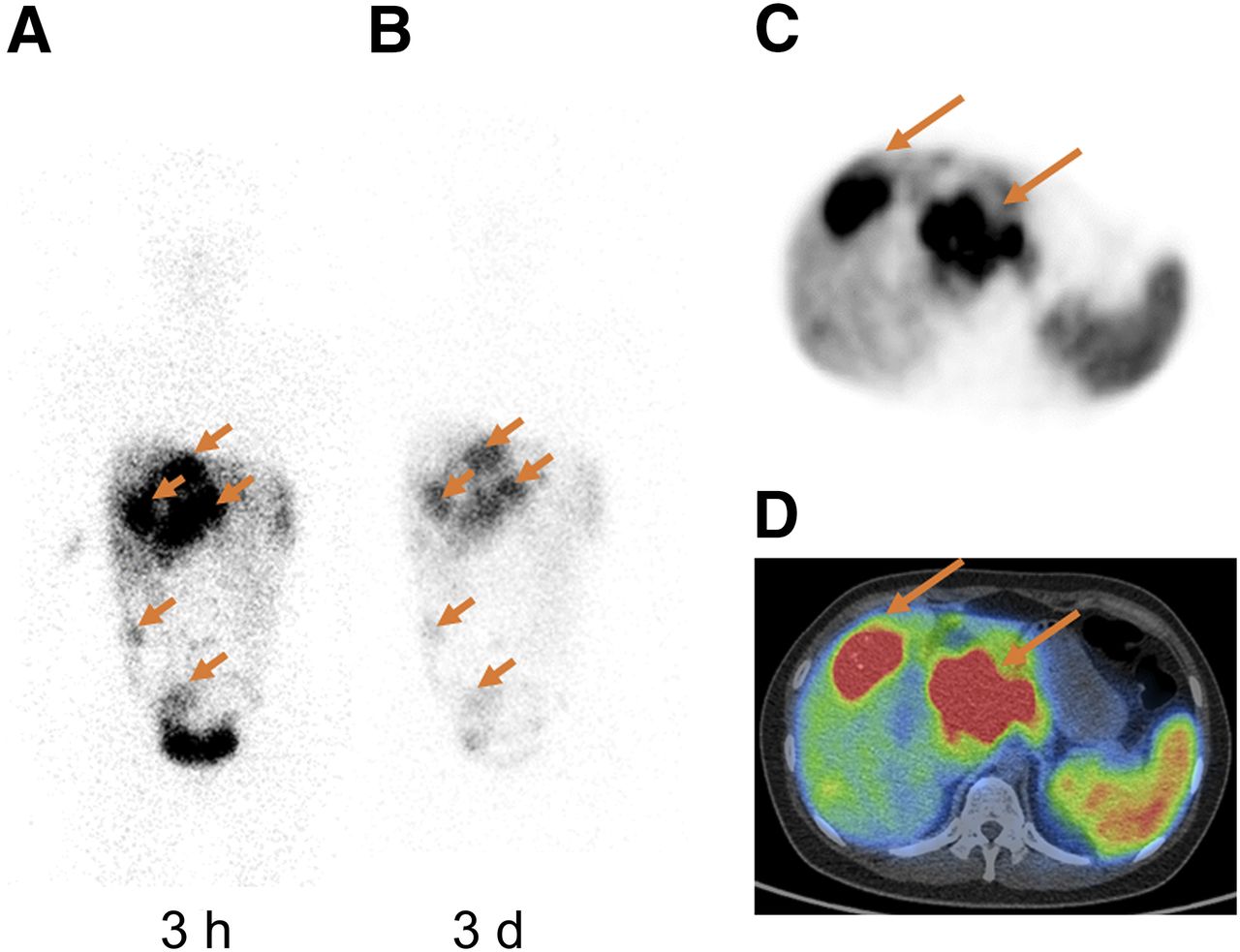
As shown in Figures 3 and 4, NET lesions were clearly identified with 68Ga-DOTATATE, with high local accumulation of radioactive signals at 45 min after injection. Most of the lesions seen by 68Ga-DOTATATE PET were also visualized on 177Lu-DOTA-EB-TATE and 177Lu-DOTATATE planar images and SPECT. It is worth noting that even at day 7, the NET lesions still showed high retention of radioactivity on 177Lu-DOTA-EB-TATE SPECT whereas the tumor uptake of 177Lu-DOTATATE decreased remarkably at 24 h after injection.
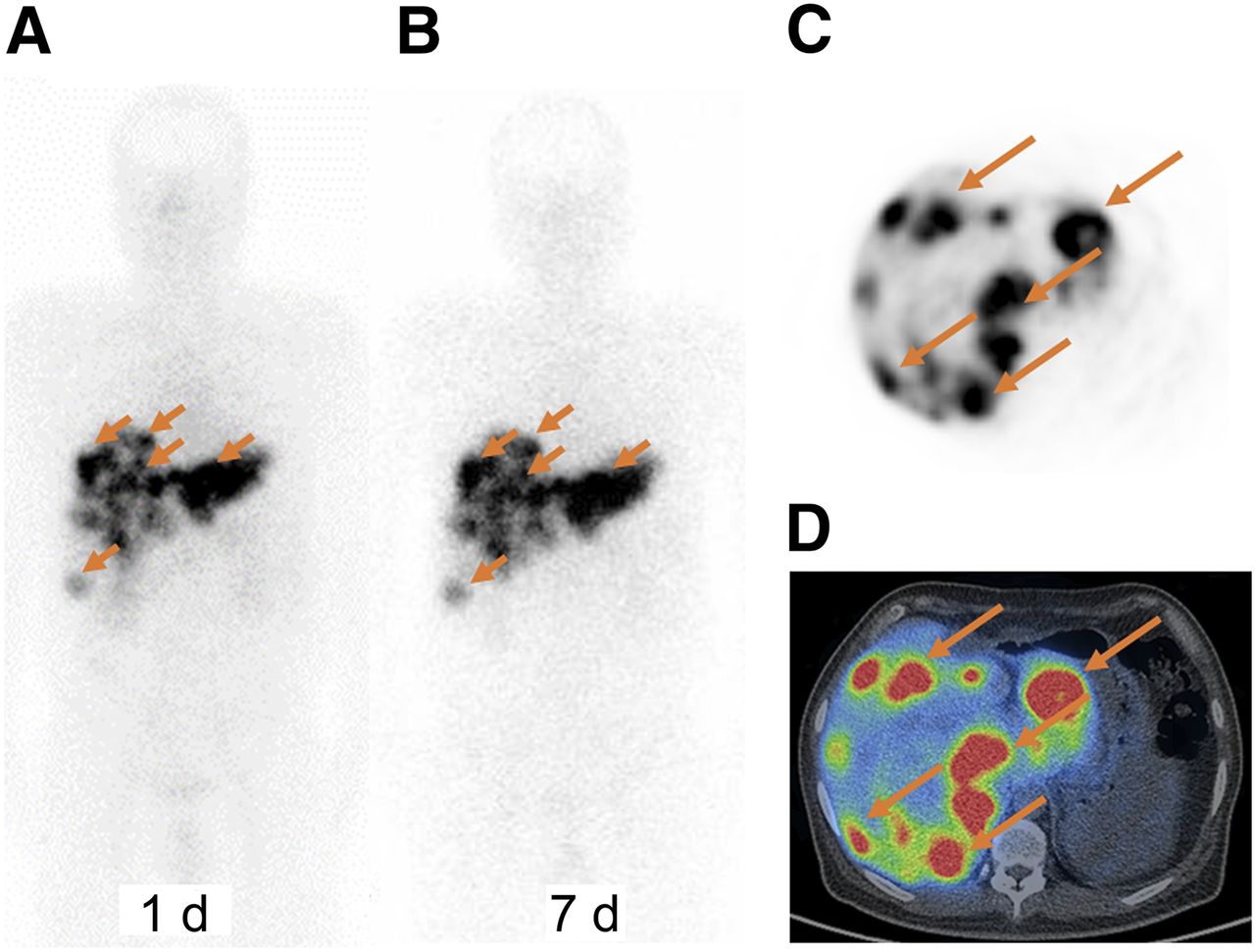
68Ga-DOTATATE PET/CT and 177Lu-DOTA-EB-TATE whole-body planar imaging and SPECT/CT of a 45-y-old male NET patient with multiple liver metastases. (A) Liver metastases identified by 68Ga-DOTATATE PET were clearly visualized on whole-body anteroposterior projection image at 1 d after administration of 177Lu-DOTA-EB-TATE. (B) Liver metastases were still clearly visualized on whole-body anteroposterior projection image at 7 d after administration of 177Lu-DOTA-EB-TATE. (C and D) Multiple liver metastases were shown on axial PET image (C) and PET/CT (D) at 45 min after intravenous injection of 68Ga-DOTATATE.

68Ga-DOTATATE PET/CT and 177Lu-DOTATATE whole-body planar imaging and SPECT/CT in a 27-y-old woman with advanced NET (G2). Multiple liver metastases were shown on whole-body anteroposterior projection images at 3 h (A) and 3 d (B) after administration of 177Lu-DOTATATE. Same liver metastases were shown on axial PET (C) and PET/CT (D) at 45 min after intravenous injection of 68Ga-DOTATATE.
In 5 patients with NET, a total 25 lesions were identified on 177Lu-DOTA-EB-TATE SPECT, including 1 primary lesion in the pancreas, 18 liver metastases, 5 lymph node metastases, and 1 pancreas metastasis. The average SUVs of these lesions were 9.91 ± 6.15, 14.91 ± 8.66, 22.28 ± 13.40, 22.46 ± 12.95, and 21.94 ± 11.63 at 2, 24, 72, 120, and 168 h after injection, respectively. In 3 patients with NET, a total of 37 lesions were identified on 177Lu-DOTATATE SPECT, including 1 lung metastasis, 21 liver metastases, 9 lymph node metastases, 4 bone metastases, and 2 pelvic metastases. The average SUVs of these lesions were 7.58 ± 5.07, 8.37 ± 5.63, 7.67 ± 5.34, 5.25 ± 3.19, and 3.86 ± 2.10 at 1, 3, 4, 24, and 72 h after injection, respectively. In patients receiving 177Lu-DOTA-EB-TATE, the average tumor SUV of 68Ga-DOTATATE PET was 12.37 ± 4.92, which was significantly lower than that in patients receiving 177Lu-DOTATATE (17.49 ± 7.02, P < 0.05).
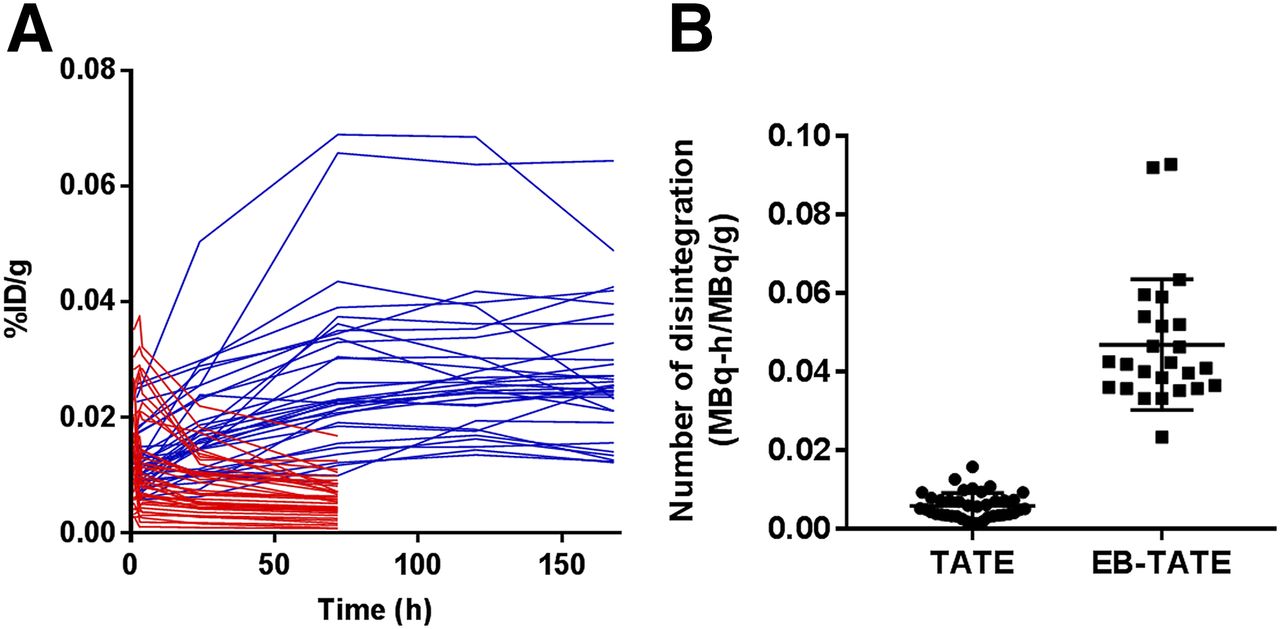
Tumor uptake of 177Lu-DOTATATE reached the peak at a very early time (3 h after injection) and decreased over time, whereas that of 177Lu-DOTA-EB-TATE kept increasing from 2 to 120 h and remained high between 120 and 168 h (Fig. 5A). Consequently, in patients receiving 177Lu-DOTA-EB-TATE, the number of disintegration of the 177Lu in the tumor region by mass average was 0.0469 ± 0.0167 MBq-h/MBq/g, which was about 7.9-fold higher than that in patients receiving 177Lu-DOTATATE (0.0059 ± 0.0033 MBq-h/MB/g, P < 0.01) (Fig. 5B). In both 177Lu-DOTA-EB-TATE and 177Lu-DOTATATE scans, the number of disintegration in NETs correlated well with the SUV determined by 68Ga-DOTATATE PET.

(A) Time–activity curves of NET lesions after administration of 177Lu-DOTA-EB-TATE (blue) and 177Lu-DOTATATE (red). (B) Number of disintegration of 177Lu within NET lesions from 177Lu-DOTA-EB-TATE and 177Lu-DOTATATE.
DISCUSSION
In this first-in-humans study, a recently developed long-lasting SSTR targeting agent (29), 177Lu-DOTA-EB-TATE, was applied in patients with advanced NETs. No subjective side effects were experienced, and no adverse symptoms were noticed or reported, indicating the safety of 177Lu-DOTA-EB-TATE.
Because of albumin binding, 177Lu-DOTA-EB-TATE showed a relatively long circulation half-life, with t1/2α around 9.47 h and t1/2β around 236 h (t1/2α = plasma/distribution half life; t1/2β = tissue/elimination half-life). Prolonged blood retention of 177Lu-DOTA-EB-TATE led to increased whole-body distribution over 177Lu-DOTATATE. Consequently, radiation exposure to red marrow from 177Lu-DOTA-EB-TATE reached 0.058 ± 0.014 mSv/MBq, which is 18.2-fold that of 177Lu-DOTATATE. It is well accepted that PRRT induces hematologic toxicity, usually resulting from bone marrow exposure to radioactivity. Indeed, subacute grade 3–4 hematologic toxicity was observed in 11% of the patients after PRRT with 177Lu-DOTATATE (34). A recent study revealed that the prevalence of persistent hematologic dysfunction after PRRT was 4% in 274 GEP NET patients receiving 177Lu-DOTATATE (35). On the basis of a generally accepted maximum absorbed dose of 2 Gy to the bone marrow (36), up to 33 GBq of 177Lu-DOTA-EB-TATE can be given to a patient. However, in view of the poor correlation between mean absorbed dose to the bone marrow and developed hematologic toxicity (8), the real therapy protocol has to be carefully planned. Plus, radiation exposure of the spleen may also affect the development of hematologic toxicity (37). Both 177Lu-DOTA-EB-TATE and 177Lu-DOTATATE showed high spleen accumulation, which may be explained by SSTR2 expression in this organ (13).
For PRRT, the maximum tolerated dose to kidneys is in the range of 23–29 Gy (10–12). Renal irradiation is mainly caused by reabsorption of radiolabeled peptides in the proximal tubule. SSTR also plays a role in the total renal uptake of radiolabeled somatostatin analogs (13), because endogenous expression of SSTR2s was found in vasa recta, tubular cells of the cortex, and distal tubule cells (14,15). Different from 177Lu-DOTATATE, which showed high dose rate within the early time period, 177Lu-DOTA-EB-TATE showed rather steady and extended kidney accumulation over time. Consequently, the absorbed dose in the kidneys for 177Lu-DOTA-EB-TATE was higher than that of 177Lu-DOTATATE. The retention of 177Lu- DOTA-EB-TATE in the kidneys is likely attributed to prolonged circulation, renal clearance, reabsorption in the proximal tubule, and SSTR2 expression. Because DOTA-EB-TATE has a much longer circulating time than DOTATATE, 2.5% l-arginine infusion may not show enough kidney protection. Other strategies may be needed to further reduce kidney retention of radiometal labeled DOTA-EB-TATE.
One limitation of this study is that the number of patients is rather small. A therapy study with more patients is necessary to compare 177Lu-DOTA-EB-TATE with 177Lu-DOTATATE with regard to therapeutic efficacy and potential toxicity. Moreover, all the recruited patients had been heavily treated, receiving various therapy regimens before undergoing DOTA-EB-TATE SPECT/CT. The dose calculation of normal organs may be affected by the high uptake in the tumors.
CONCLUSION
By introducing an albumin-binding moiety, 177Lu-DOTA-EB-TATE showed significantly higher NET uptake and retention over 177Lu-DOTATATE. This first-in-humans study demonstrates that 177Lu-DOTA-EB-TATE is safe and well tolerated in NET patients.
DISCLOSURE
This work was supported in part by the Intramural Research Program (IRP) of the National Institute of Biomedical Imaging and Bioengineering (NIBIB), National Institutes of Health (NIH), the Key Project on Inter Governmental International Scientific and Technological Innovation Cooperation in National Key Projects of Research and Development Plan (2016YFE0115400), National Natural Science Foundation of China projects (81701742, 81741142), and Beijing Municipal Natural Science Foundation (7161012). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Prof. Hongyan Ying (Oncology Department, PUMCH, CAMS & PUMC) for helpful regulatory advices, Dr. Yeqing Liu and Dr. Hongtao He (Philips Healthcare) for help in SPECT quantification, Dr. Hui Li (Department of Nuclear Medicine, PUMCH, CAMS & PUMC) for image acquisition, Dr. Xiaoping Hu (Beijing PET Technology Co., Ltd) and Dr. Dayong Huang (Tiansi Information Technology Co., Ltd.) for radiolabeling, and Dr. Jiahua Xu (GE Healthcare) for SPECT data analysis.
Footnotes
Published online Apr. 13, 2018.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 15, 2018.
- Accepted for publication March 26, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Landscape of Nuclear Medicine in China and Its Progress on Theranostics
- Efficacy of [67Cu]Cu-EB-TATE Theranostic Against Somatostatin Receptor Subtype-2-Positive Neuroendocrine Tumors
- A Single-Arm, Low-Dose, Prospective Study of 177Lu-EB-PSMA Radioligand Therapy in Patients with Metastatic Castration-Resistant Prostate Cancer
- Combined Targeted Radiopharmaceutical Therapy and Immune Checkpoint Blockade: From Preclinical Advances to the Clinic
- Albumin Binder-Conjugated Fibroblast Activation Protein Inhibitor Radiopharmaceuticals for Cancer Therapy
- 177Lu-DOTA-EB-TATE, a Radiolabeled Analogue of Somatostatin Receptor Type 2, for the Imaging and Treatment of Thyroid Cancer
- Peptide Receptor Radionuclide Therapy of Late-Stage Neuroendocrine Tumor Patients with Multiple Cycles of 177Lu-DOTA-EB-TATE
- Reply: Different Radionuclides in DOTA-EB-TATE Effect Different Uptake in Somatostatin Receptor-Positive HEK293 Cells
- Different Radionuclides in DOTA-EB-TATE Effect Different Uptake in Somatostatin Receptor-Positive HEK293 Cells
- Peptide Receptor Radionuclide Therapy in Grade 3 Neuroendocrine Neoplasms: Safety and Survival Analysis in 69 Patients
- New Developments in Peptide Receptor Radionuclide Therapy