


Abstract
To date, limited data are available concerning peptide receptor radionuclide therapy (PRRT) of grade 3 (G3) neuroendocrine neoplasms (NENs) with a Ki-67 proliferation index of greater than 20%. The purpose of this study was to analyze the long-term outcome, efficacy, and safety of PRRT in patients with somatostatin receptor (SSTR)–expressing G3 NENs. Methods: A total of 69 patients (41 men; age, 28–81 y) received PRRT with 177Lu- or 90Y-labeled somatostatin analogs (DOTATATE or DOTATOC). Twenty-two patients had radiosensitizing chemotherapy. Kaplan–Meier analysis was performed to calculate progression-free survival (PFS) and overall survival (OS), defined from the start of PRRT, including a subgroup analysis for patients with a Ki-67 index of less than or equal to 55% and a Ki-67 index of greater than 55%. Treatment response was evaluated according to RECIST 1.1 as well as molecular imaging criteria (European Organization for Research and Treatment of Cancer). Short- and long-term toxicity was documented (Common Terminology Criteria for Adverse Events, v 5.0) using a structured database (comprising >250 items per patient) and retrospectively analyzed. Results: Forty-six patients had pancreatic NENs, 11 had unknown primary cancer, 6 had midgut NENs, 3 had gastric NENs, and 3 had rectal NENs. The median follow-up was 94.3 mo. The median PFS was 9.6 mo, and the median OS was 19.9 mo. For G3 NENs with a Ki-67 index of less than or equal to 55% (n = 53), the median PFS was 11 mo and the median OS was 22 mo. Patients with a Ki-67 index of greater than 55% (n = 11) had a median PFS of 4 mo and a median OS of 7 mo. For patients with positive SSTR imaging but no 18F-FDG uptake, the median PFS was 24 mo and the median OS was 42 mo. A significant difference was found for both PFS and OS, with median PFS of 16 mo and 5 mo and median OS of 27 mo and 9 mo for an SUVmax of greater than 15.0 and an SUVmax of less than or equal to 15.0, respectively, on SSTR PET. In the group with 18F-FDG uptake scored as 3 or 4, the median PFS was 7.1 mo and the median OS was 17.2 mo. In the group with 18F-FDG uptake scored as 0–2, the median PFS was 24.3 mo and the median OS was 41.6 mo. PRRT was well tolerated by all patients; no grade 3 or grade 4 hematotoxicity occurred, and no clinically significant decline in renal function was observed. There was no hepatotoxicity. Conclusion: PRRT was tolerated well, without significant adverse effects, and was efficacious in G3 NENs; the clinical outcome was promising, especially in patients with a Ki-67 index of less than or equal to 55% and even in patients for whom chemotherapy had failed. Baseline 18F-FDG along with SSTR molecular imaging was useful for stratifying G3 NEN patients with high uptake on SSTR PET/CT and no or minor 18F-FDG avidity—a mismatch pattern that was associated with a better long-term prognosis.
Neuroendocrine neoplasms (NENs) are a heterogeneous group of neoplasms arising from diffuse neuroendocrine system cells (1). They are classified as grade 1 (G1), G2, and G3 according to the World Health Organization classification, which is based on mitotic activity and Ki-67 immunostaining, with a Ki-67 index of less than or equal to 2%, 3%–20%, and greater than 20%, respectively. High-grade (G3) NENs were previously referred to as neuroendocrine carcinomas, with an aggressive malignant character and poor prognosis; these were mainly treated with chemotherapy (2,3). However, substantial heterogeneity of high-grade NENs has been observed on the basis of clinical behavior, genetic profiling, and proliferation rate. According to the World Health Organization 2017 and European Neuroendocrine Tumor Society classifications, a new G3 NEN category for the distinction of well-differentiated G3 NENs from neuroendocrine carcinomas has been introduced. Recent genetic studies also reported that G3 NENs express p53 and rb1, which are usually negative in neuroendocrine tumors (NETs), providing a novel basis for prognostic and therapeutic stratification (4,5).
During the last decade, substantial progress has been made in the treatment of G1 and G2 NENs. On the other hand, systemic cytotoxic chemotherapy, typically using platinum compounds, is usually applied for highly malignant G3 neuroendocrine carcinomas.
NENs are characterized by a high level of expression of somatostatin receptors (SSTRs), allowing the use of radiolabeled somatostatin analogs for receptor-mediated imaging and peptide receptor radionuclide therapy (PRRT) with therapeutic radioisotopes such as 90Y or 177Lu; the latter has become an established treatment for patients with unresectable or metastatic, progressive, well-differentiated, SSTR-positive NETs (6–10). Recently, 177Lu-DOTATATE (Lutathera; Advanced Accelerator Applications) was approved by both the European Commission and the U.S. Food and Drug Administration for the treatment of metastatic, progressive, well-differentiated (G1/G2), SSTR-positive gastroenteropancreatic NETs in adults. However, data on PRRT in G3 NENs are very limited.
The aim of this study was to assess the safety and efficacy, in terms of survival analysis, of PRRT in patients who have SSTR-expressing G3 NENs with a Ki-67 proliferation index of greater than 20%. The prognosis of patients with distinctly different Ki-67 proliferation indices and baseline SSTR and 18F-FDG PET/CT imaging was also evaluated.
MATERIALS AND METHODS
Patients
Eligible patients were adults who had histopathologically confirmed metastatic G3 NENs (Ki-67 index, >20%) with a confirmed high level of SSTR expression—that is, tumor uptake greater than normal liver parenchyma uptake on 68Ga-SSTR PET imaging. Disease progression was documented within 3–6 mo before the start of PRRT.
From January 2003 to January 2017, data for a total of 69 patients who had G3 NENs (41 men and 28 women; age range, 28–81 y; mean age, 58.1 y [SD, 12.9 y]) and underwent PRRT were retrospectively reviewed. The study was approved by an internal review board, and written informed consent was obtained from each patient. The baseline demographics of the patients are shown in Tables 1 and 2.
Demographic and Baseline Clinical Characteristics of Patients With G3 NENs (n = 69)
Baseline Imaging of Patients with G3 NENs (n = 69)
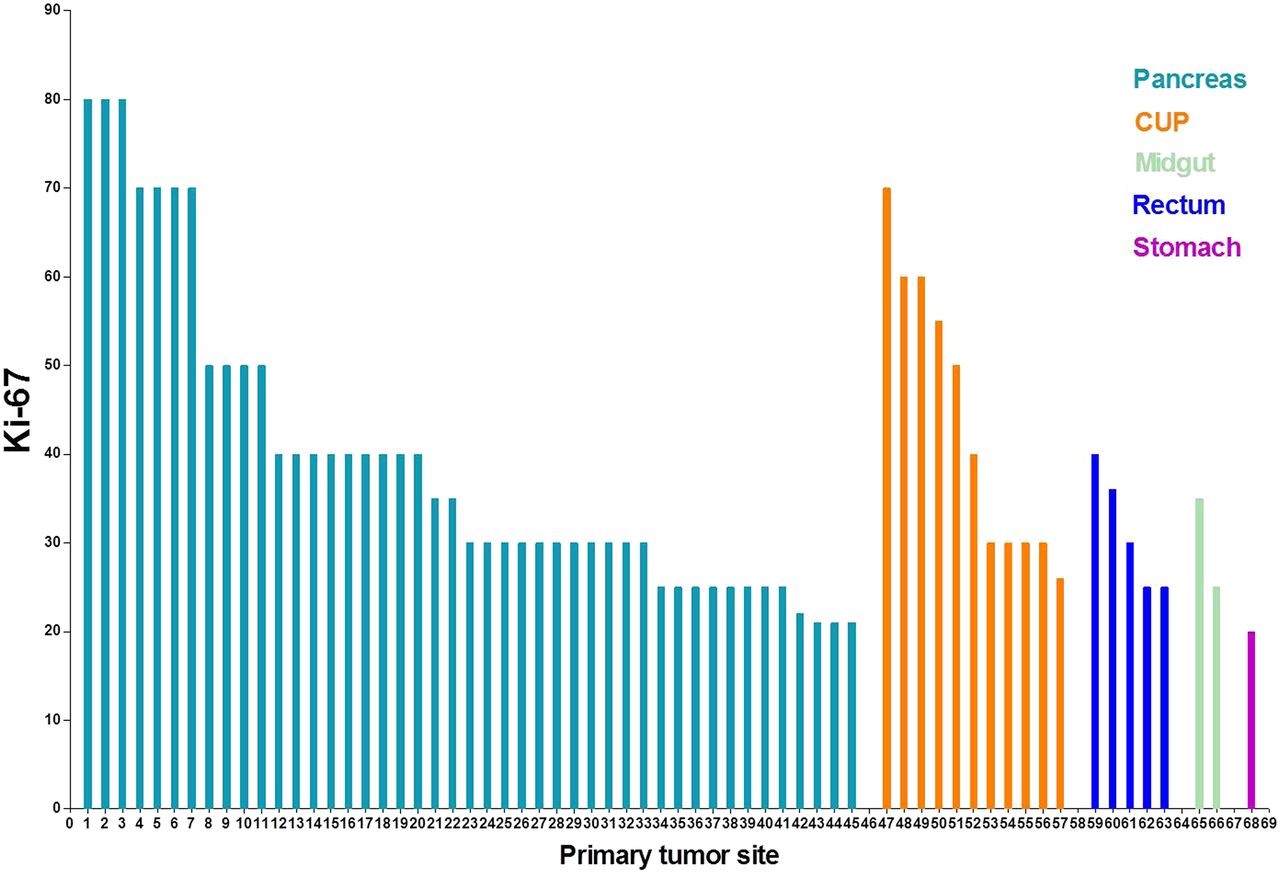
Forty-six patients (66.7%) had pancreatic NENs, and 11 (15.9%) had unknown primary cancer, whereas the primary tumor was present in the midgut in 6 patients, in the stomach in 3 patients, and in the rectum in 3 patients. Of the 69 patients, 53 (76.8%) had a Ki-67 index of less than or equal to 55% and 11 (15.9%) had a Ki-67 index of less than or equal to 55%; for 5 patients (7.2%), the Ki-67 was unknown at the initial assessment and no samples could be obtained for reanalysis. The Ki-67 index for each patient according to the primary tumor site is shown in Figure 1.
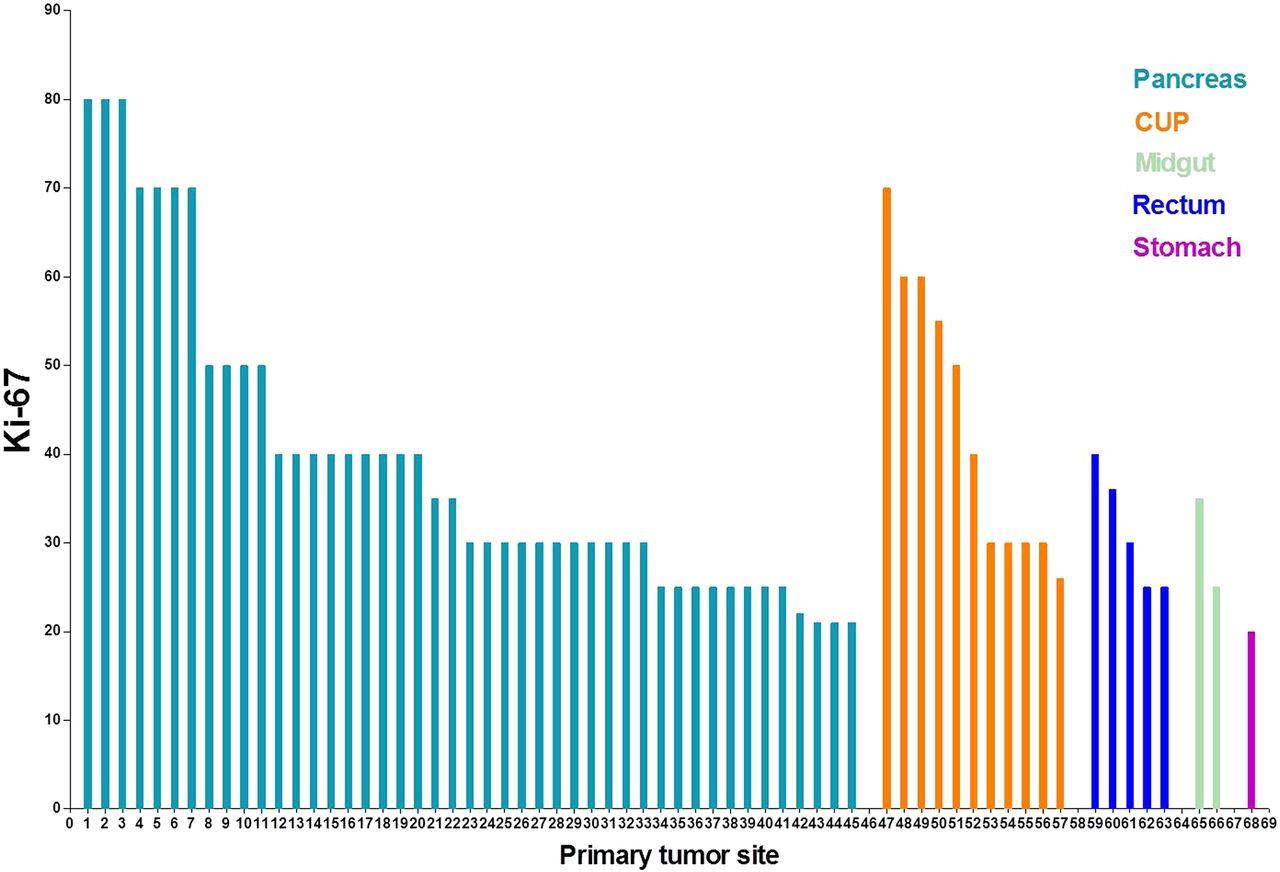
Ki-67 proliferation index for G3 NEN patients according to primary tumor site. CUP = unknown primary cancer.
PRRT was applied as the first-line treatment in 8 patients (11.6%), as the second-line treatment in 25 patients (36.2%), and as the third-line therapy in 28 patients (40.6%). The time span (mean ± SD) between biopsy for the assessment of Ki-67 and the first treatment cycle was 27.1 ± 36.8 mo. Treatment parameters and the number of PRRT cycles are shown in Table 3. The median administered activity for 177Lu PRRT per cycle was 4.5 ± 13.2 GBq (range, 2.5–9.5 GBq). The median administered activity for 90Y PRRT per cycle was 3.2 ± 1.0 GBq (range, 1.3–4.8 GBq). The maximum cumulative administered activity was 38.0 GBq.
Treatment Cycles and Cumulative Administered Radioactivity for PRRT with 177Lu, 90Y, and Both Radionuclides (n = 69)
Radiopharmaceutical Preparation
The DOTA-conjugated somatostatin analogs DOTATOC, DOTANOC, and DOTATATE were labeled with 68Ga, 177Lu, and 90Y, respectively, in our institutional radiopharmacy according to good manufacturing practices regulations. The radionuclide 68Ga was obtained in-house from a 68Ge/68Ga generator. A highly efficient NaCl-based 68Ga labeling procedure has been developed in our hospital (11,12). 177Lu and 90Y were obtained from different manufacturers. The labeling of DOTA-conjugated peptides with 177Lu and 90Y was performed as previously described (13). High-performance liquid chromatography was used for quality control. The radiochemical purity was always greater than 99%.
Treatment Regimen
Nephroprotection was performed by amino acid infusion (1,600 mL of 5% lysine HCl and 10% l-arginine HCl) (14). In patients with impaired renal function (glomerular filtration rate, <60 mL/min) and for the application of 90Y, 4% Gelofusine (B. Braun Melsungen AG) was infused according to patients’ weights for additional nephroprotection. The infusion was started at least 30 min before administration of the radiotherapeutic compound and continued for 4 h thereafter. The radiopharmaceutical was coadministered over 10–15 min using a second infusion pump system. The activity to administer was individually chosen on the basis of the Bad Berka Score (15)—that is, the uptake in tumor lesions, as shown by 68Ga-SSTR PET/CT (performed before each treatment cycle), renal function, hematologic reserve, liver involvement, extrahepatic tumor burden, Ki-67 index, tumor grade, 18F-FDG PET/CT status, tumor dynamics (doubling time, new lesions), weight loss, time since first diagnosis, functional activity of the tumor, previous treatments, and general status of the patient (Karnofsky Performance Scale) (16–18). The decision to use 90Y or 177Lu depended on the tumor mass, renal and hematologic function, previous therapy (especially chemotherapy), SUV, and other factors, as described by the Bad Berka Score (15,19–21). Both radionuclides were used in subsets of patients sequentially or in combination on the same day (tandem PRRT) (15). The interval between the treatment cycles was 10–12 wk. Depending on general and hematologic status as well as tolerability, 22 patients with high uptake on 18F-FDG PET/CT underwent peptide receptor chemoradionuclide therapy—that is, PRRT in combination with a low dose of capecitabine (1,500 mg/m2/d in 2 daily divided doses) for 2 wk starting from the day of PRRT. Additionally, temozolomide was administered in 4 of 22 patients (5).
Safety
Laboratory parameters (erythrocytes, hemoglobin, platelets, leukocytes, creatinine, blood urea nitrogen, serum glutamic oxalo-acetic transaminase, serum glutamate pyruvate transaminase, bilirubin, serum alkaline phosphatase, thyroid-stimulating hormone, gamma-glutamyl transpeptidase, and respective tumor markers) were evaluated before each cycle and at restaging. Renal function was monitored by the tubular extraction rate using 99mTc-mercaptoacetyltriglycine renography; in addition, the glomerular filtration rate was determined using 99mTc-diethylenetriaminepentaacetic acid in patients with elevated serum creatinine levels. Treatment-related adverse events were graded according to the Common Terminology Criteria for Adverse Events (CTCAE, v 5.0).
Restaging was performed with SSTR PET/CT every 3–4 mo after PRRT. In case of stable disease or remission (complete or partial), restaging was performed with SSTR PET/CT every 6 mo until disease progression was evident on imaging. SSTR PET/CT and 18F-FDG PET/CT were performed until January 2014 with a Siemens Biograph Duo and since then with a Siemens Biograph mCT Flow 64. SUVmax were obtained by drawing circular regions of interest, which were automatically adapted (40% isocontour) to a 3-dimensional volume of interest using commercial software provided by the vendor. Contrast-enhanced CT (spiral CT using a Biograph mCT Flow 64) was acquired after the intravenous administration of 60–100 mL of nonionic iodinated contrast agent. Images were evaluated by 2 experienced nuclear medicine specialists. MRI was performed in selected cases (allergy to iodinated contrast agent or poor detectability of liver metastases on CT scan), and an abdominal ultrasound was obtained at each visit. PRRT was resumed if progression occurred after a therapy interval of more than 6 mo (so-called next “treatment phase” of PRRT).
Response Assessment
The treatment response was assessed on CT or MR images according to RECIST 1.1 (22). Imaging was performed before each PRRT cycle and at restaging. The disease control rate was defined as complete remission, partial remission (PR), and stable disease. The best objective response rate was defined as patients achieving complete remission or PR at follow-up according to RECIST. The molecular response was evaluated according to European Organization for Research and Treatment of Cancer criteria (23).
Statistical Analysis
A Kaplan–Meier survival analysis was performed to calculate progression-free survival (PFS) and overall survival (OS), defined from the start of PRRT. The log-rank test and the Cox proportional hazards model were used to analyze the survival distribution of subgroups. Continuous variables were denoted as mean ± SD. Differences between 2 independent groups were determined by Student t tests. Differences among groups were compared with 1-way ANOVAs. All statistical tests were 2-tailed, and a P value of less than 0.05 was considered statistically significant.
RESULTS
Safety
No CTCAE grade 4 hematotoxicity was observed, and except for 1 patient (1.4%) with grade 3 leukocytopenia, there was no significant toxicity. No grade 3 or 4 anemia was observed after PRRT, although 2 patients (2.9%) had grade 3 anemia before PRRT. No myelodysplastic syndrome or leukemia occurred during follow-up until death or the study cutoff date.
No CTCAE grade 3 or 4 nephrotoxicity was observed in any patient. At baseline, creatinine was normal in 57 of 69 patients (82.6%), whereas 14.5% (10/69) had grade 1 and 2.9% (2/69) had grade 2 renal dysfunction. On follow-up, 84.6% (44/52) had normal creatinine, 13.5% (7/52) had grade 1 elevation of creatinine, and 1.9% (1/52) had grade 2 elevation of creatinine, respectively. However, there was no correlation with the number of cycles or the cumulative administered radioactivity. No patients with grade 2 renal impairment at baseline demonstrated a further decline in renal function. The glomerular filtration rate did not show any significant change after PRRT, despite the fact that some patients had grade 2 renal impairment at baseline (glomerular filtration rate, 35–60 mL/min/1.73 m2). No liver function abnormality was observed after therapy.
Treatment Response
Response evaluation was possible in 55 patients. Five patients died shortly after the first PRRT cycle, and in 9 patients the clinical condition deteriorated severely, preventing repeated imaging. According to RECIST 1.1, the disease control rate at 3 mo after PRRT was 78.2%, including 30.9% of patients with PR and 47.3% with stable disease. The molecular imaging responses at 3 mo after PRRT were 49.1% with PR, 21.8% with stable disease, 27.3% with progressive disease, and 5.5% with a mixed response. The treatment responses are shown in Table 4.
Treatment Response at 3 Months After PRRT (n = 55)
Survival
Until the study cutoff date in January 2018, 56 of 69 patients (81%) with G3 NENs died. The median follow-up time was 94.3 mo (interquartile range, 56.2–104.9). For the entire group of 69 patients, the median PFS was 9.6 mo and the median OS was 19.9 mo. Among the 64 patients with G3 NENs (excluding 5 patients in whom the exact Ki-67 index was not known), the median PFS for a Ki-67 index of less than or equal to 55% was 11 mo (n = 53) and the median PFS for a Ki-67 index of greater than 55% was 4 mo (n = 11) (P < 0.05) (Fig. 2). The median OS for a Ki-67 index of less than or equal to 55% was 22 mo, and the median OS for a Ki-67 index of greater than 55% was 7 mo (P < 0.05) (Fig. 3).
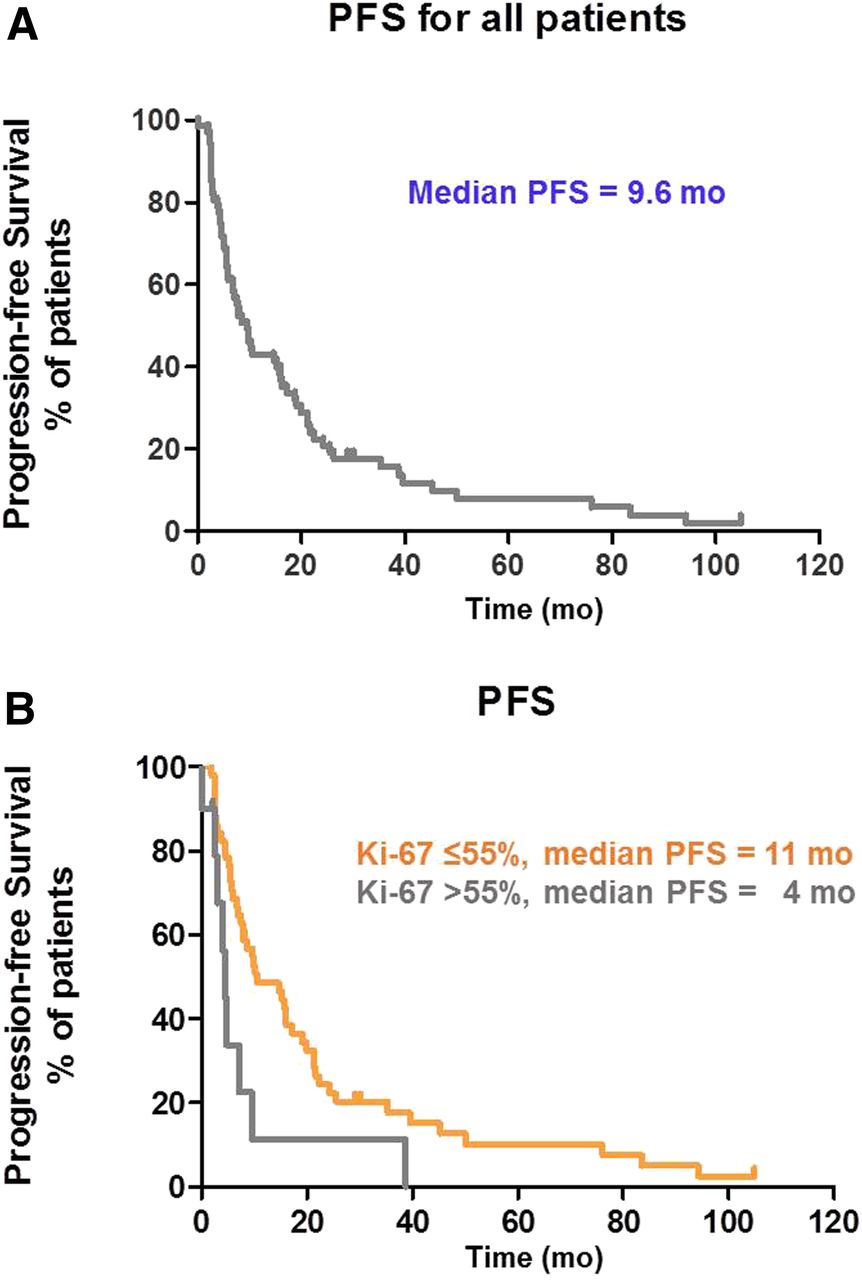
Kaplan–Meier curves for PFS (in months) from start of PRRT for all patients with Ki-67 index of >20% (A) and for subgroups (B) with Ki-67 index of ≤55%, and Ki-67 index of >55%.

Kaplan–Meier curves for OS (in months) from start of PRRT for all patients with Ki-67 index of >20% (A) and for subgroups (B) with Ki-67 index of ≤55%, and Ki-67 index of >55%.
Peptide receptor chemoradionuclide therapy was performed in 22 patients; 18 patients received capecitabine, and 4 patients received temozolomide. In this group, the median PFS was 9.8 mo and the median OS was 21.6 mo.
PET Imaging Related to Response and Survival
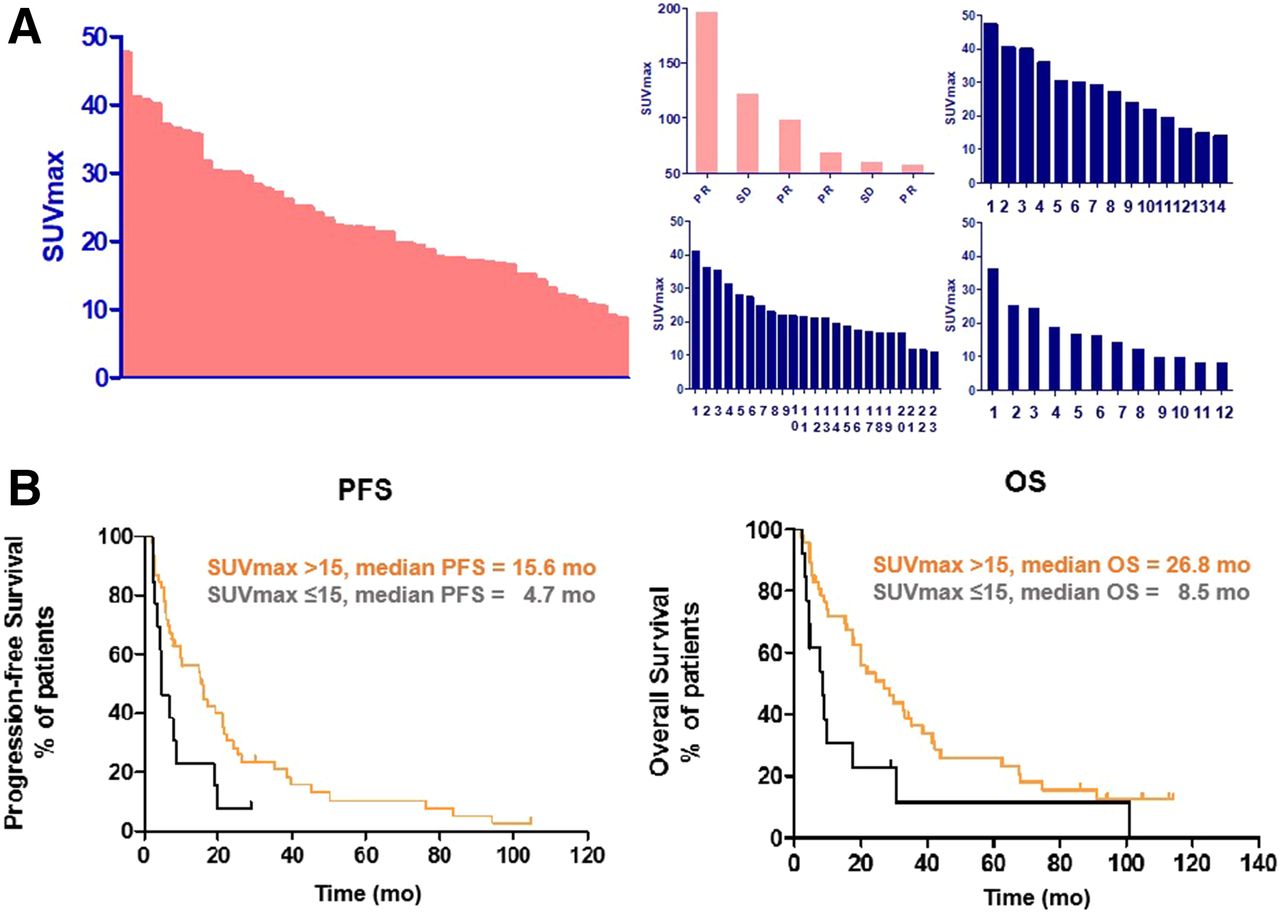
Of the 55 patients for whom a response assessment was performed, 86.0% (37/43) demonstrating an objective response had an SUVmax of greater than 15.0 on baseline 68Ga-SSTR PET/CT. All 6 patients with an SUVmax of greater than 50 had an objective response to PRRT (4 achieving PR and 2 with stable disease) (Fig. 4A). The PFS and OS based on the study-specified 68Ga-SSTR PET/CT SUVmax cutoff of 15.0 are shown in Figure 4B. A significant difference was found for both PFS and OS, with median PFS of 16 mo and 5 mo (P < 0.05) and median OS of 27 mo and 9 mo (P < 0.05) for an SUVmax of greater than 15.0 and an SUVmax of less than or equal to 15.0, respectively.

(A) Distribution of SUVmax on 68Ga-SSTR PET before PRRT (red). Distribution of SUVmax at baseline in subgroups (blue) that had PR (top right), stable disease (SD) (bottom left), and progressive disease (bottom right) at 3 mo after PRRT. (B) Kaplan–Meier curves for PFS and OS in subgroups with SUVmax cutoff of >15 (orange line) and SUVmax cutoff of ≤15 (black line) on baseline 68Ga-SSTR PET imaging.
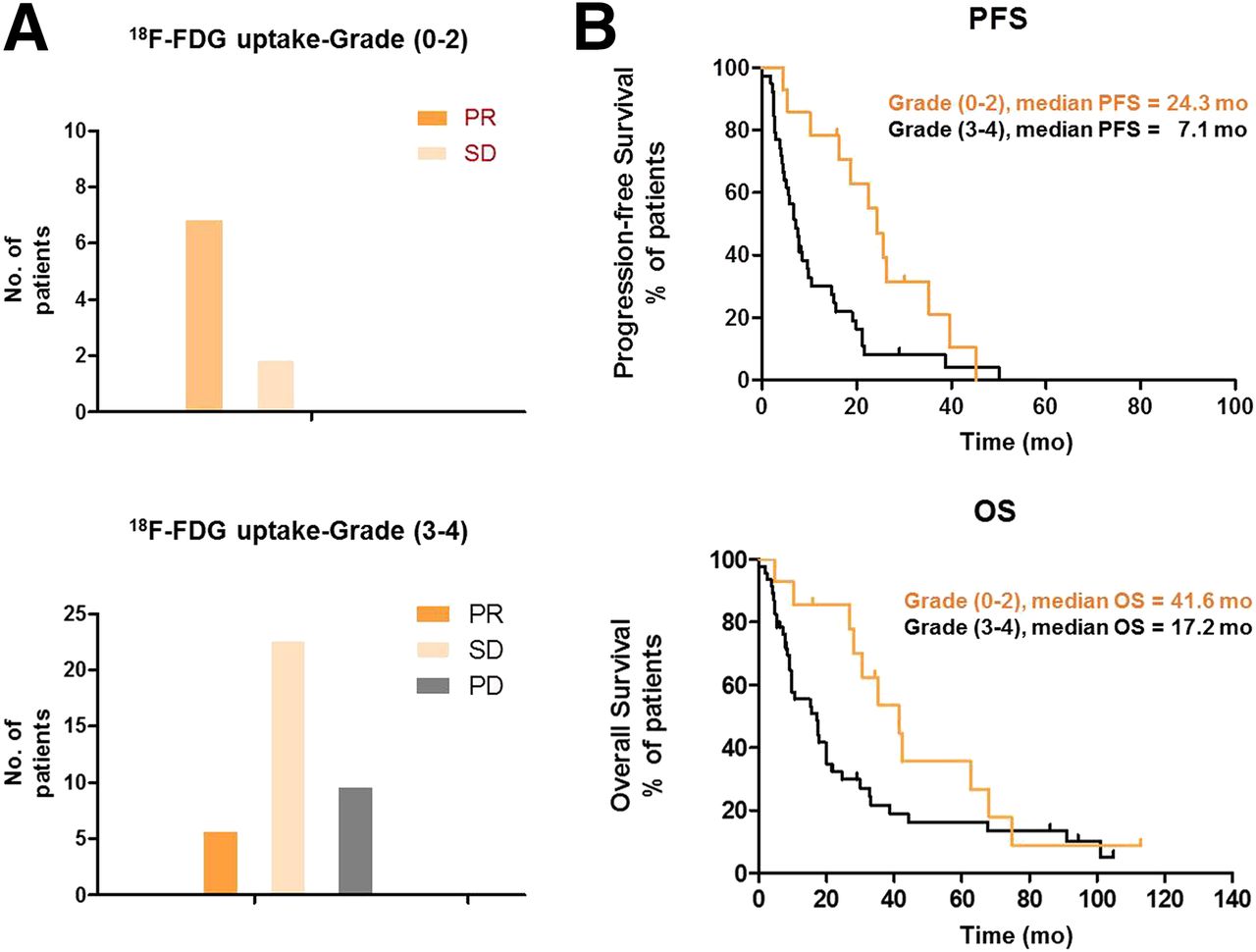
In 48 of 59 patients having baseline 18F-FDG PET/CT, the responses were also evaluated. All 9 patients with grade 0–2 imaging results (no or very mild 18F-FDG uptake, less than that in the liver, mismatch between SSTR and 18F-FDG imaging) had an objective response to PRRT at 3 mo (7 achieving PR and 2 with stable disease). On the other hand, of the 39 patients with grade 3 or 4 status (uptake higher than that in the liver), 6 had PR, 23 had stable disease, and 10 had progressive disease. In the group with 18F-FDG uptake scored as 3 or 4 (n = 45), the median PFS was 7.1 mo and the median OS was 17.2 mo. In the group with 18F-FDG uptake scored as 0–2 (n = 14), the median PFS was 24.3 mo and the median OS was 41.6 mo (Fig. 5).

(A) Response at 3 mo after PRRT in subgroups (patients with grade 0–2 and patients with grade 3 or 4) with 18F-FDG PET at baseline. PD = progressive disease. (B) Kaplan–Meier curves for PFS and OS in subgroups with grade 0–2 (orange line) and grade 3 or 4 (black line) on baseline 18F-FDG PET.
DISCUSSION
Most PRRT studies have focused on G1 and G2 NENs (6–8,24–27). The NETTER-1 study, a prospective randomized controlled phase 3 clinical trial using tandem treatment with 177Lu-DOTATATE and octreotide (long-acting release) (30 mg) in patients with advanced midgut neuroendocrine tumors, also focused on well-differentiated NENs; in that study, a markedly improved PFS and a significantly higher response rate were reported with the tandem treatment than with high-dose octreotide (long-acting release) (6). Clinical experience with PRRT in patients with G3 NENs is limited, even though SSTR expression, in principle, enables the use of a 177Lu- or 90Y-coupled somatostatin analog as a therapy option (Figs. 6 and 7). Only a few PRRT studies have included patients with G3 NENs or NENs with a high proliferation index (5,28–30).
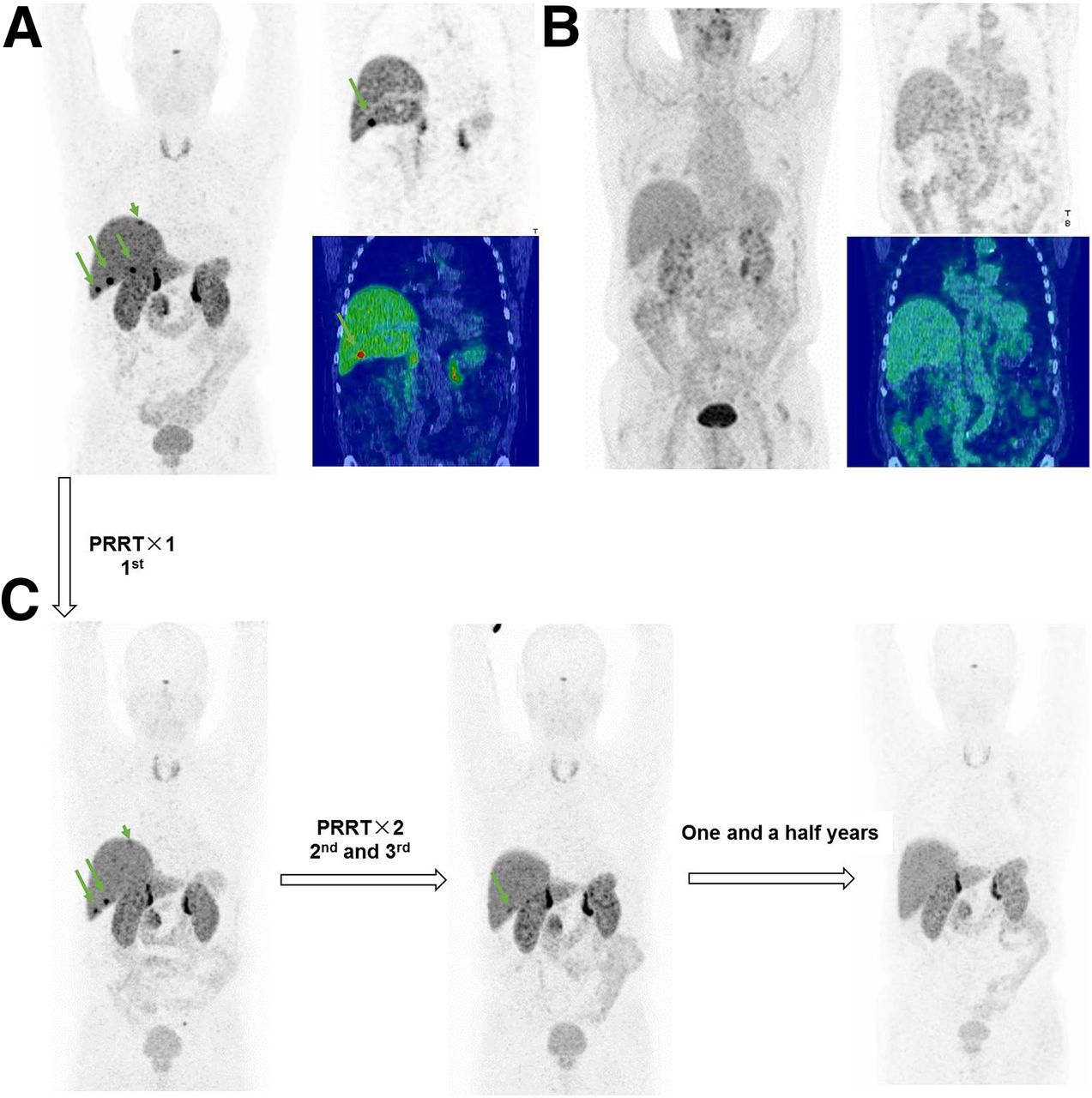
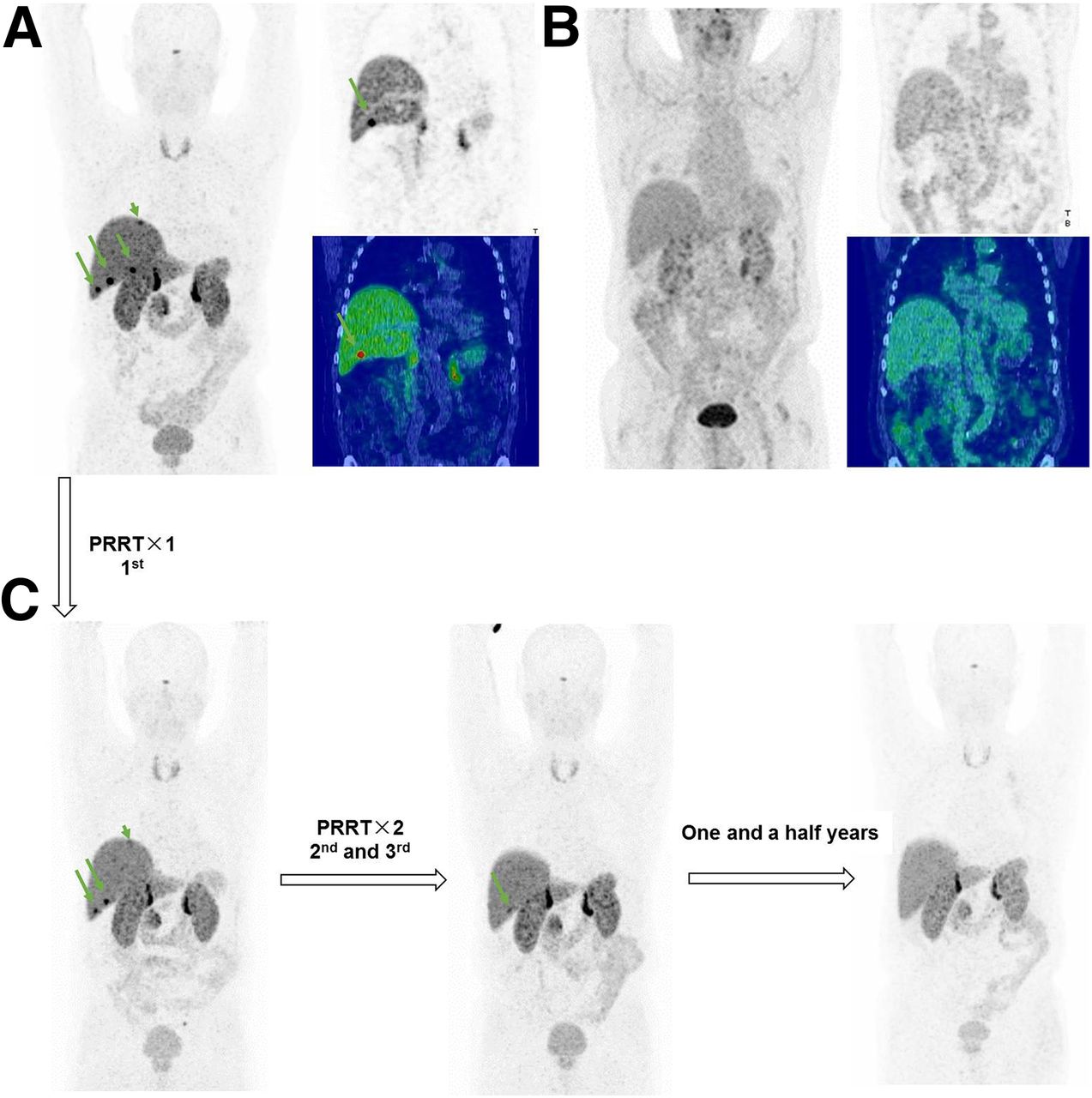
71-y-old woman with metastatic pancreatic NENs and Ki-67 index of 25%. Patient had undergone pancreatic tail resection with splenectomy and adhesiolysis and showed disease progression after 8 cycles of chemotherapy with cisplatin and etoposide within 6-mo period. (A) Maximum-intensity-projection (MIP) (left) and coronal (right) images from 68Ga-SSTR PET/CT showed SSTR expression (arrows) in liver metastases with SUVmax of 40.0. (B) MIP (left) and coronal (right) images from 18F-FDG PET/CT showed no significant 18F-FDG hypermetabolism in liver metastases and complete mismatch between 68Ga-SSTR and 18F-FDG at baseline. Patient was treated with 3 cycles of 177Lu-DOTATOC PRRT with cumulative administered radioactivity of 21.8 GBq. (C) Restaging scans showed significant response in liver metastases at 3 mo (PR) (left) and complete remission on longer follow-up (middle and right), with progression-free interval of 32 mo from first cycle of PRRT.
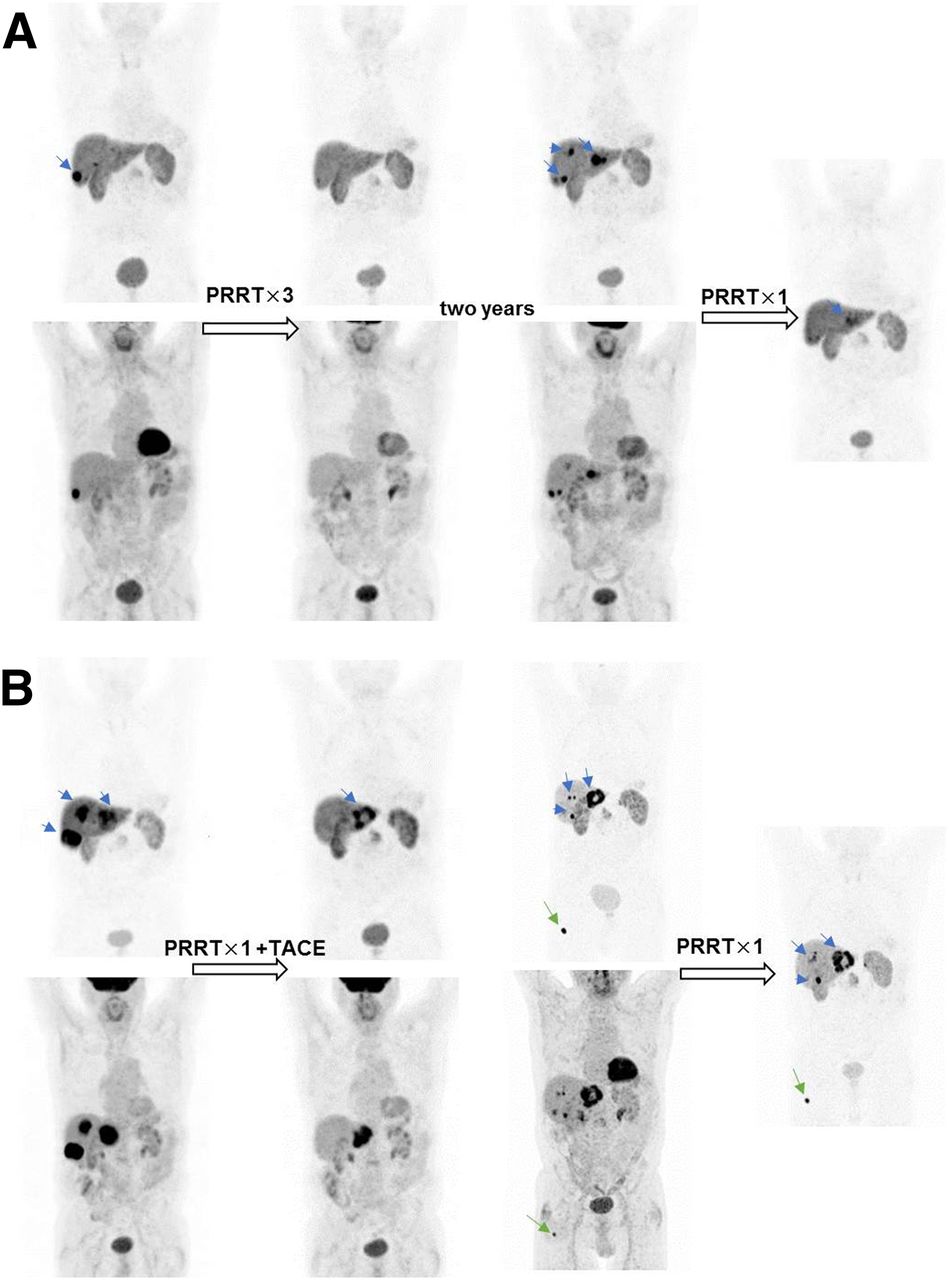
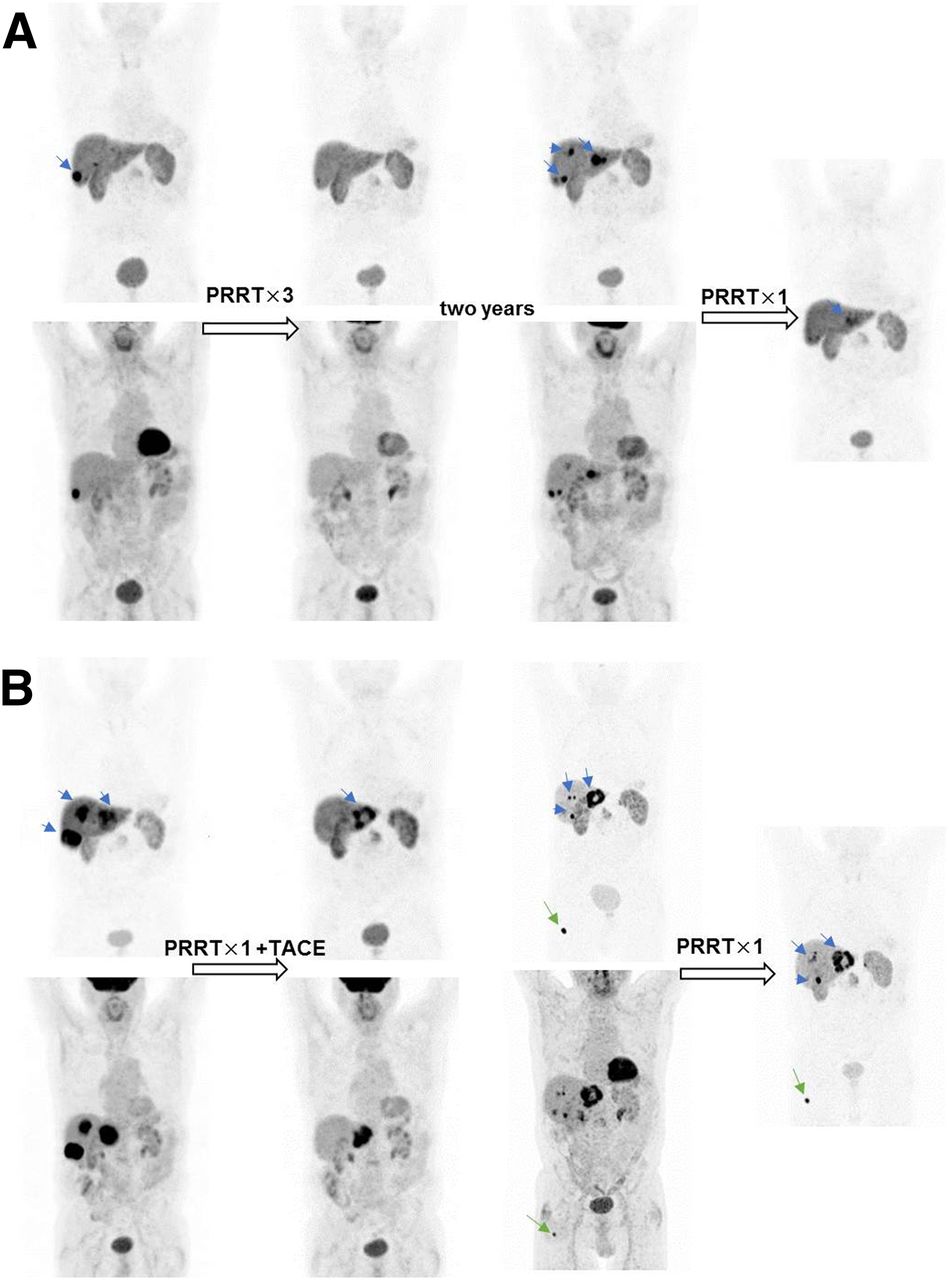
Serial 68Ga-SSTR PET/CT and 18F-FDG PET/CT maximum-intensity-projection (MIP) images of 77-y-old man with pancreatic NENs and liver metastases and with Ki-67 proliferation index of 30% for primary tumor. Previous treatments (from 2006 to 2008) were left pancreatectomy, splenectomy, atypical partial gastrectomy, resection of left colonic flexure, liver metastasis resection and cholecystectomy, gastric fundus resection, liver metastasis radiofrequency ablation, and peritoneal adhesiolysis. (A) Baseline 68Ga-SSTR PET/CT (left) showed SSTR expression in liver metastases with SUVmax of 26.0, and significant hypermetabolism was noted on 18F-FDG PET/CT. After 3 cycles of PRRT, good response (PR) with significant reduction of hepatic tumor burden was seen on both 68Ga-SSTR and 18F-FDG PET/CT. This disease was stable, with progression-free interval of 32 mo. Patient progressed in 2011 with multiple liver metastases (blue arrows) and was further treated with 1 cycle of 177Lu-DOTATATE PRRT; once again, significant regression of hepatic metastases was seen (right). (B) After PFS of 19 mo, patient progressed in 2013 with multiple liver metastases (left), apparent as match between 68Ga-SSTR and 18F-FDG PET/CT. He then underwent combined treatment with 177Lu-DOTATATE PRRT and transarterial chemoembolization (TACE). Restaging scan showed marked PR in hepatic metastases. After short PFS of 10 mo, new bone metastases in right femur were detected on both 18F-FDG and 68Ga-DOTATATE PET/CT (green arrows), and patient was treated with another cycle of PRRT in 2015. In all, this patient received 6 cycles of PRRT with cumulative administered radioactivity of 24.5 GBq of 177Lu-DOTATATE/TOC and 7.5 GBq of 90Y-DOTATATE before he died of disease progression 7.5 y from first cycle of PRRT.
To date, this was the largest reported cohort of patients with SSTR-expressing G3 NENs treated with PRRT. Although this patient group was heterogeneous, including PRRT combined with radiosensitizing chemotherapy in some patients, most G3 NEN patients received only PRRT after the failure of prior chemotherapy. The follow-up (median, 94.3 mo) in this patient cohort was the longest among all published studies.
The median PFS and OS of patients with G3 NENs were significantly shorter than those of patients with well-differentiated G1 and G2 NENs (6,31). However, compared with the results and the PFS and OS obtained with other treatment modalities in G3 NEN patients, our results were very encouraging. In the NORDIC study, a median PFS of just 4 mo and a median OS of only 11 mo were reported for patients who had a World Health Organization classification of G3 and received first-line chemotherapy (32). With a median PFS of 9.6 mo and a median OS of 19.9 mo, our patient cohort treated with PRRT had twice-longer PFS and relatively longer OS; these findings were even more promising because 76.7% of our patients had already received at least 1 line of treatment before PRRT. Our results match well with those of a single-center study in 28 patients from Australia (5), for whom a PFS of 9 mo and a median OS of 19 mo were reported.
The median OS obtained for patients with a Ki-67 index of less than or equal to 55% in the present study was markedly longer than that reported by the NORDIC group (22 vs. 14 mo). These results suggest that, compared with platinum-based chemotherapy, PRRT may be a superior first-line therapeutic option in selected patients with a high level of SSTR expression and a Ki-67 index of less than or equal to 55%. On the contrary, in patients with a Ki-67 index of greater than 55%, the median OS was longer for chemotherapy (7 vs. 10 mo). Therefore, platinum-based chemotherapy may be a better first-line therapy for patients with a Ki-67 index of greater than 55%. The median OS obtained in our patients with a Ki-67 index of less than or equal to 55% was markedly shorter than that in the Australian study (22 vs. 46 mo); the fact that the number of patients in the present study was significantly larger (53 vs. 22) contributed to an even greater heterogeneity among the patient population. Indeed, our results for patients with a Ki-67 index of greater than 55% matched those of the Australian study (7 mo in both studies).
We also found a significant difference between the PFS values for the 2 groups—11 mo for a Ki-67 index of less than or equal to 55% (n = 53) and 4 mo for a Ki-67 index of greater than 55% (n = 11)—a trend similar to that in a recent Italian study (29) in which patients who had a Ki-67 index of greater than 35% were compared with patients who had a Ki-67 index of less than 35%; in that study, the latter patients had a significantly longer PFS (6.8 and 26.3 mo, respectively) (P = 0.005). The difference in the absolute PFS in the present study could be attributed to the lower cutoff for Ki-67 (of 35%) in the Italian study. In addition, the authors of the Italian study included patients with a Ki-67 index of greater than 15%—that is, the “gray zone” (Ki-67 index of 15%–20%), defined by the European Neuroendocrine Tumor Society as G2 tumors (29).
Indeed, Ki-67 alone may not be truly representative of the tumor grade, mainly because the heterogeneity of different metastases yields different values from biopsies of different lesions. 18F-FDG PET/CT plays an important role in the prognosis of NETs, with an 18F-FDG–positive tumor denoting a more aggressive phenotype (33). We characterized the 18F-FDG imaging phenotypes according to the grades of uptake. Patients with no or very faint 18F-FDG uptake responded well to PRRT at 3 mo—that is, a pattern of mismatch between SSTR and 18F-FDG imaging is of prognostic relevance. The median PFS for the group with no to mild 18F-FDG uptake was significantly longer than that for the highly 18F-FDG–avid group. These results are concordant with those of a previous study examining the role of 18F-FDG PET/CT in advanced, well-differentiated grade 1 or 2 NETs (34).
68Ga-SSTR PET/CT may also play an important role in predicting the response to PRRT in G3 NENs. Patients with a good response and a favorable outcome after PRRT had a relatively higher SUVmax on SSTR PET/CT imaging. This finding is in line with those of another study, in which all grades of NENs were included (35). When a cutoff of 15.0 was used for the 68Ga-SSTR PET SUVmax, a significant association with both PFS and OS was observed.
A limitation of the present study is that it was a retrospective analysis. There were variations in SSTR affinities because different radiopharmaceuticals were used. Also, the number of patients with a Ki-67 index of greater than 55% was limited, probably because of the lack of SSTR expression in this group. The fact that 13 patients received only 1 PRRT cycle may have influenced the prognosis. Another limitation is the lack of availability of the exact Ki-67 index in 5 patients; however, these patients were referred from other centers and were characterized as having histopathologically confirmed G3 NENs. Furthermore, almost one-third (31.9%) of the patients with a high-grade 18F-FDG PET/CT phenotype and a more aggressive tumor type received peptide receptor chemoradionuclide therapy, and the potential additional value of the concomitant radiosensitizing chemotherapy is unclear. Further randomized and controlled studies certainly remain warranted.
CONCLUSION
PRRT was efficacious in patients with G3 neuroendocrine neoplasms, even those for whom chemotherapy had failed, resulting in a promising clinical outcome—especially for patients with a Ki-67 index of less than or equal to 55%. A high SUV on SSTR PET/CT and no or minor 18F-FDG avidity were associated with a better prognosis—that is, 18F-FDG PET/CT along with SSTR PET/CT helped to stratify patients with G3 NENs. PRRT was well tolerated, without significant adverse effects.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the radiopharmacists, radiochemists, physician colleagues, nursing staff, and nuclear medicine technologists at Zentralklinik Bad Berka for their support.
Footnotes
Published online Aug. 16, 2018.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 22, 2018.
- Accepted for publication August 7, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Targeting CXCR4 with [212Pb/203Pb]-Pentixather Significantly Increases Overall Survival in Small Cell Lung Cancer
- First-in-Humans Study of the SSTR Antagonist 177Lu-DOTA-LM3 for Peptide Receptor Radionuclide Therapy in Patients with Metastatic Neuroendocrine Neoplasms: Dosimetry, Safety, and Efficacy
- Bowel Obstruction as a Complication of Peptide Receptor Radionuclide Therapy
- 177Lu-DOTA-EB-TATE, a Radiolabeled Analogue of Somatostatin Receptor Type 2, for the Imaging and Treatment of Thyroid Cancer
- Prognostic Value of 18F-FDG PET/CT in a Large Cohort of Patients with Advanced Metastatic Neuroendocrine Neoplasms Treated with Peptide Receptor Radionuclide Therapy
- NANETS/SNMMI Consensus Statement on Patient Selection and Appropriate Use of 177Lu-DOTATATE Peptide Receptor Radionuclide Therapy
- Evaluating the Role of Theranostics in Grade 3 Neuroendocrine Neoplasms