


Abstract
Studies demonstrate that the investigational 64Cu-DOTATATE radiopharmaceutical may provide diagnostic and logistical benefits over available imaging agents for patients with somatostatin receptor (SSTR)–positive neuroendocrine tumors (NETs). Accordingly, we aimed to prospectively determine the lowest dose of 64Cu-DOTATATE that facilitates diagnostic-quality scans and evaluated the diagnostic performance and safety in a phase III study of patients with SSTR-expressing NETs. Methods: A dose-ranging study was conducted on 12 patients divided into 3 dose groups (111 MBq [3.0 mCi], 148 MBq [4.0 mCi], and 185 MBq [5.0 mCi] ± 10%) to determine the lowest dose of 64Cu-DOTATATE that produced diagnostic-quality PET/CT images. Using the 64Cu-DOTATATE dose identified in the dose-ranging study, 3 independent nuclear medicine physicians who were masked to all clinical information read PET/CT scans from 21 healthy volunteers and 42 NET-positive patients to determine those with disease or no disease, as well as those with localized versus metastatic status. Masked-reader evaluations were compared with a patient-specific standard of truth, which was established by an independent oncologist who used all previously available pathology, clinical, and conventional imaging data. Diagnostic performance calculated for 64Cu-DOTATATE included sensitivity, specificity, negative predictive value, positive predictive value, and accuracy. Inter- and intrareader reliability, as well as ability to differentiate between localized and metastatic disease, was also determined. Adverse events were recorded from 64Cu-DOTATATE injection through 48 h after injection. Results: The dose-ranging study identified 148 MBq (4.0 mCi) as the optimal dose to obtain diagnostic-quality PET/CT images. After database lock, diagnostic performance from an initial majority read of the 3 independent readers showed a significant 90.9% sensitivity (P = 0.0042) and 96.6% specificity (P < 0.0001) for detecting NETs, which translated to a 100.0% sensitivity and 96.8% specificity after correcting for an initial standard-of-truth misread. Excellent inter- and intrareader reliability, as well as ability to distinguish between localized and metastatic disease, was also noted. No adverse events were related to 64Cu-DOTATATE, and no serious adverse events were observed. Conclusion: 64Cu-DOTATATE PET/CT is a safe imaging technique that provides high-quality and accurate images at a dose of 148 MBq (4.0 mCi) for the detection of somatostatin-expressing NETs.
The incidence of neuroendocrine tumors (NETs) has increased 6.4-fold in the United States since 1973, with the greatest increase being observed in localized, well-differentiated grade 1 NETs (1). The increase in NET diagnoses is likely due in part to advances in diagnostic imaging (1). The use of somatostatin receptor (SSTR) scintigraphy with 111In-diethylenetriaminepentaacetic acid (DTPA)-octreotide (OctreoScan; Mallinckrodt) in the mid-1990s significantly improved the accuracy with which patients with NETs were identified, staged, and monitored. Octreotide is a somatostatin analog that binds specifically to SSTR types 2 and 5 and allows the molecular imaging and characterization of NETs (2,3). After determining SSTR positivity with 111In-DTPA-octreotide SPECT, peptide receptor radionuclide therapy could then be instituted using therapeutic radionuclides (e.g., 177Lu and 90Y) labeled with the same peptide for personalized treatment (4). However, 111In-DTPA-octreotide was constrained by limitations in image quality and spatial resolution, as well as prolonged imaging protocols (5,6).
In 2016, the U.S. Food and Drug Administration approved the radiopharmaceutical 68Ga-DOTATATE to be used with PET, an imaging modality with higher resolution than SPECT (3). Additionally, the higher affinity of DOTATATE than of DTPA-octreotide to SSTR type 2 further increased the sensitivity, specificity, and accuracy of detecting SSTR-expressing NETs (2,6). Despite the advantages over 111In-DTPA-octreotide, 68Ga-DOTATATE has inherent limitations. In particular, a short 1.1-h half-life requires that it be locally produced via a generator and used proximally, limiting availability of 68Ga-DOTATATE to large medical centers (3). The tight scanning window, moreover, complicates the precise and close coordination that is required between radiochemistry and patient scheduling personnel (7).
64Cu-DOTATATE has been studied as a potential PET radiotracer for SSTR-based imaging. 64Cu-DOTATATE is an investigational somatostatin analog PET radiotracer that has demonstrated lower radiation dose and higher lesion detection rates than 111In-DTPA-octreotide, as well as a lesion detection rate superior to that of 68Ga-DOTATOC, in patients with NETs (7,8). The lower positron energy (0.65 vs. 1.90 MeV), which translates to lower positron range (0.56 vs. 3.5 mm), is thought to explain the anticipated improved spatial resolution and diagnostic performance of 64Cu-DOTATATE over, for example, 68Ga-DOTATOC (9–11). Additionally, the longer physical half-life (12.7 vs. 1.1 h) may increase the shelf-life of 64Cu-DOTATATE, eliminate reliance on a generator, and provide a more flexible scanning window, making 64Cu-DOTATATE attractive for routine clinical imaging (2,7).
The primary objective of this first U.S. phase III, prospective, reader-masked, controlled pivotal trial was to assess the sensitivity and specificity of 64Cu-DOTATATE PET/CT imaging for detecting NETs in subjects with or without disease against a standard of truth (SOT) for each subject. However, unlike most diagnostic performance studies, the phase III study was preceded by an independent dose-ranging study to determine the optimal dose for obtaining diagnostic-quality PET/CT images. Secondary objectives were to compare the performance of 64Cu-DOTATATE using a reader-majority rule determination or individual reader determinations versus the SOT, evaluate the performance of 64Cu-DOTATATE in ascertaining whether subjects had metastatic or local disease compared with the SOT, and assess inter- and intrareader agreement. Consistent with other well-controlled diagnostic performance studies, safety was also evaluated.
MATERIALS AND METHODS
Dose-Ranging Study Design
Twelve patients with NETs were recruited into 3 64Cu-DOTATATE dose groups (111 MBq [3.0 mCi], 148 MBq [4.0 mCi], and 185 MBq [5.0 mCi] ± 10%) with 4 patients per group. Patient demographics and characteristics are shown in Table 1. PET/CT images were acquired at 60 ± 15 min after injection and with a 5-min acquisition time per bed position. Image quality was evaluated by 3 experienced readers masked to dose information. Image quality was assessed using the following scoring system: 0, inadequate (grainy images with poor delineation of lesions); 1, questionable (clear images, but lesion delineation is suboptimal and small lesions [1 cm] are hard to assess); and 2, acceptable (clear images; large and small lesion delineation is possible). Cohort scores were calculated by adding together the average image subject scores in each dosing group. Consistent with the as-low-as-reasonably-achievable (ALARA) principle, the lowest dose level with a cohort score of at least 7 was deemed the lowest 64Cu-DOTATATE dose that provides diagnostic-quality PET/CT images. The study was approved by the Biomedical Research Alliance of New York Institutional Review Board, and all subjects gave written informed consent.
Demographics and Baseline Characteristics (Safety Population)
Phase III Study Design
The pivotal phase III study (NCT03673943) was an open-label, single-dose, single-arm, single-center, prospective design that evaluated the sensitivity and specificity of 64Cu-DOTATATE PET/CT imaging in patients with known or suspected NETs against an independent reader’s SOT for each subject; readers were masked to the SOT. Patient demographics and characteristics are shown in Table 1. To obtain at least a 90% chance of showing more than 0.70 sensitivity and more than 0.60 specificity, 63 subjects were required. After a preestablished 2:1 (NET-positive/NET-negative) ratio, 42 SOT-positive patients and 21 SOT-negative healthy volunteers were recruited under a U.S. Food and Drug Administration–approved Investigational New Drug application. Of note, the 4 patients at the optimal 64Cu-DOTATATE dose (148 MBq [4.0 mCi]) in the dose-ranging study were eligible and subsequently enrolled in the phase III study. NET positivity by the SOT was determined using MRI, CT, 18F-FDG PET/CT, bone scintigraphy, 111In-DTPA-octreotide scans, or 68Ga-DOTATATE PET/CT. This prospective study was performed in accordance with the Helsinki Declaration and followed the International Conference on Harmonisation Good Clinical Practice guidelines. The study was also approved by the Biomedical Research Alliance of New York Institutional Review Board, and all subjects gave written informed consent.
Synthesis and Radiolabeling of 64Cu-DOTATATE
64CuCl2 was produced at the cyclotron facility at Washington University in St Louis, Missouri, and DOTATATE peptide was manufactured by ABX GmbH. 64Cu-DOTATATE drug was prepared by RadioMedix, Inc., according to current good-manufacturing-practice guidelines. Briefly, 64CuCl2 (5,550–9,250 MBq) was added to sodium acetate buffer containing DOTATATE (0.4 mg) and gentisic acid (4.0 mg). The reaction mixture was incubated for 10 min at 95°C and then passed through a Sep-Pak C18 cartridge (Waters). The cartridge-retained product was eluted with 1 mL of ethanol into a vial containing sodium ascorbate solution (50 mg/mL). The contents of the vial were filtered through a 0.22-μm filter. The final 64Cu-DOTATATE drug underwent standard radiopharmaceutical quality control. The radiochemical purity of 64Cu-DOTATATE was more than 95% (high-performance liquid chromatography), and the average specific activity was 29.6 MBq/μg.
Image Acquisition
All subjects had a PET/CT scan performed on a Biograph Horizon 16-slice scanner (Siemens Healthineers). PET/CT scans were undertaken on average 63 min (median, 60 min; range, 39–97 min) after a single intravenous dose of 148 MBq ± 10% (range, 132–163 MBq) of 64Cu-DOTATATE. PET scans (from vertex of skull to mid thigh) were obtained in 3-dimensional mode, with an acquisition time of 5 min per bed position over an approximately 30-min total scan time. A non–contrast-enhanced CT scan was performed using the CT exposure factors of 140 kVp and 80 mA in 0.5 s. PET/CT images were reconstructed using CT for attenuation correction and ordered-subsets expectation maximization with 2 iterations and 24 subsets.
Image Analysis and Data Interpretation
PET/CT images acquired at the clinical site were transferred to an independent medical-imaging-research contract organization that masked all clinical, imaging, and laboratory information. Thereafter, the contract organization randomized the images to 3 experienced, independent, board-certified nuclear medicine physicians who had been trained previously by the contract organization to detect abnormal images associated with SSTRs. Readers 1, 2, and 3 had 37, 5, and 8 y of experience in nuclear medicine, respectively, and all had read hundreds of 68Ga-based SSTR PET/CT scans. On assessment, each physician reader categorized subjects as disease or no disease based only on 64Cu-DOTATATE tumor uptake. Subjects categorized as disease were further subcategorized as localized or metastatic, as appropriate. Ten percent of the images (7 cases) were randomly selected for assessment of interreader variability by reintroducing the images to the independent readers for a second masked read no earlier than 4 wk after the primary read.
In parallel, an independent oncologist established the SOT for each subject using available scan reports from composite conventional imaging modalities and pathology studies; 64Cu-DOTATATE scans were not used to establish the SOT. The SOT oncologist used the collective information to categorize each patient as disease or no disease and as localized or metastatic, as appropriate.
Safety Assessments
Safety was determined primarily through investigator-assessed treatment-emergent adverse events. An adverse event was considered treatment-emergent if the start date and time were on or after the start date and time of 64Cu-DOTATATE injection. Adverse events observed by the investigator or obtained during nonleading telephone interviews 24 and 48 h after injection were recorded using the MedDRA, version 19.1, coding system from the International Council for Harmonisation. In addition, observed or patient-reported immediate adverse events were assessed within 1 h before and 2 h after 64Cu-DOTATATE administration. The severity of adverse events was assessed independently by investigators and graded using the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0, in which grades 1, 2, 3, 4, and 5 indicate a mild adverse event, a moderate adverse event, a severe or medically significant but not life-threatening adverse event, a life-threatening adverse event, and death related to an adverse event, respectively.
Vital signs were recorded within 30 min before and up to 1 h after administration of 64Cu-DOTATATE. Blood samples for clinical laboratory tests and hematology were collected within 30 min before and within 2 h after 64Cu-DOTATATE administration. All subjects also underwent continuous electrocardiogram recording at least 15 min before 64Cu-DOTATATE administration, with continuation for at least 30 min after administration. In addition, a 12-lead static electrocardiogram was performed within 60 min before and after 64Cu-DOTATATE administration. All electrocardiogram data were collected, analyzed, and reviewed by an independent physician to determine normal versus abnormal and whether the abnormality was clinically significant.
For 8 subjects of child-bearing potential, a urine pregnancy test was performed before imaging to rule out pregnancy.
Statistical Analysis
Confidence limits for all binomial parameters, including sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy, were calculated using the Wilson score with continuity correction (the score method). The level of significance for each hypothesis test was a 1-sided α-value of 0.025. Point estimates of sensitivity and specificity were calculated along with 2-sided 95% confidence intervals using the score method. Sensitivity and specificity were calculated on an individual-reader basis. In addition, a majority-read statistical analysis was performed, taking into account the most favored category of reading for each subject from the 3 readers, as it was a consensus reading. Success on the primary endpoints could be declared if 2 of the 3 independent readers achieved a sensitivity and a specificity exceeding preestablished thresholds.
Analysis of NPV, PPV, and accuracy was computed using the majority read (i.e., the majority 64Cu-DOTATATE diagnosis from the 3 readers) and using reader reports. Point estimates of the majority read and individual-reader NPV, PPV, and accuracy were calculated along with 95% confidence intervals using the score method. Sensitivity and specificity were determined relative to the SOT. The statistical analysis plan included a testable hypothesis for the coprimary endpoints (i.e., sensitivity and specificity). Thus, P values were calculated for sensitivity and specificity and not for PPV, NPV, or accuracy. P values of less than 0.05 were considered statistically significant.
For the inter- and intrareader agreement analysis of each reader pair (readers 1 and 2, readers 1 and 3, and readers 2 and 3), a Cohen κ along with a 95% confidence interval on the Cohen κ were computed. A 95% confidence interval for κ was also computed (12). A Fleiss generalized κ and associated 95% confidence interval were used to assess overall agreement among the 3 readers (12).
The data analyses were conducted using SAS Software, version 9.4 or higher (IBM).
RESULTS
Dose-Ranging Study
Table 2 shows the image scoring of the 3 masked readers, as well as the cohort scores for each dose. According to the cohort scores, the 148-MBq (4.0 mCi) and 185-MBq (5.0 mCi) 64Cu-DOTATATE doses displayed image quality superior to that of the 111-MBq (3.0 mCi) dose. On the basis of the ALARA principle, the 148-MBq (4.0 mCi) dose was selected as the optimal dose for the subsequent pivotal phase III study.
Image Scoring of Dose-Ranging Study
Sensitivity and Specificity (Phase III Primary Objective)
Three readers evaluated the sensitivity and specificity of 64Cu-DOTATATE PET/CT compared with an SOT in 63 evaluable subjects with known or suspected NETs (Table 3). Significant sensitivity and specificity were demonstrated for all readers. Reader 1 had a sensitivity and specificity of 90.9% (P = 0.0042) and 96.6% (P = 0.0042), respectively; reader 2 had 90.9% (P = 0.0042) and 80.0% (P = 0.0172), respectively; and reader 3 had 90.9% (P = 0.0042) and 90.0% (P = 0.0003), respectively. The PPVs of the 3 readers ranged from 83.3% to 96.8%; all NPVs were nearly 90.0%, and accuracy ranged from 85.7% to 93.6%. Two of the 3 readers had point estimates of specificity of at least 90.0%, whereas the third had a point-estimate specificity of 80.0% in determining absence of NETs when disease was indeed absent. All readers passed the sensitivity and specificity hypotheses (coprimary effectiveness endpoints with sensitivity > 70.0% and specificity > 60.0%) testing at a 1-sided α value of 0.025.
Individual Reader and Majority Reads for 64Cu-DOTATATE PET/CT Imaging Versus SOT
After the database lock, reasons for failing to detect NETs were reviewed retrospectively, and it was found that SOT reads for 3 subjects were incorrectly recorded as NET-positive (disease) instead of NET-negative (no disease) by the oncologist who established the SOT. Because the objective of the study was to assess not the SOT oncologist’s read but the performance of the PET/CT scan against true-positive and true-negative NET diagnoses, we also measured corrected diagnostic performance parameters that would have been attained if the SOT had been established correctly. Determination of the corrected diagnostic performance found that the sensitivity, specificity, PPV, NPV, and accuracy of readers 1 and 3 would have been 100.0%, 96.8%, 96.7%, 100.0%, and 98.4%, respectively. Reader 2 would have had a 100.0% sensitivity, 81.8% specificity, 83.3% PPV, 100.0% NPV, and 90.5% accuracy.
Majority-Read Imaging Performance, Predictive Value, and Determination of Metastatic Versus Localized Disease (Secondary Objectives)
One of the 64Cu-DOTATATE PET/CT scans for reader 1 was not evaluable because of breathing artifacts. Therefore, secondary objectives were obtained with 62 subjects. According to the SOT, 29 subjects were NET-negative and 33 were NET-positive. On the basis of the 64Cu-DOTATATE PET/CT imaging, the majority read classified 31 subjects as NET-positive and 31 as NET-negative, translating to significant diagnostic performance. Sensitivity, specificity, PPV, NPV, and accuracy for the majority read were 90.9% (P = 0.0042), 96.6% (P < 0.0001), 96.8%, 90.3%, and 93.6%, respectively (Table 3). Using a corrected SOT, the sensitivity, specificity, PPV, NPV, and accuracy for the per-patient majority read were 100.0% (P = 0.0002), 96.8% (P < 0.0001), 96.7%, 100.0%, and 98.4%, respectively. Further, the ability to differentiate between metastatic and localized disease with 64Cu-DOTATATE PET/CT revealed a majority read with 100.0% sensitivity and 100.0% specificity.
Inter- and Intrareader Agreement (Tertiary Objectives)
Overall, the 3 readers demonstrated a substantial degree of interreader agreement (κ = 0.7664), with readers 1 and 3 having almost perfect agreement (κ = 0.8710) among the reader pairs. Table 4 presents a summary of the interreader agreement for assessment of 64Cu-DOTATATE PET/CT imaging.
Summary of Interreader Agreement for Assessment of 64Cu-DOTATATE PET/CT Imaging
For the intrareader variability, readers 1 and 3 demonstrated perfect intrareader agreement on the image reread (κ = 1.0000). Table 5 summarizes intrareader agreement for 64Cu-DOTATATE PET/CT imaging.
Intrareader Agreement of 64Cu-DOTATATE PET/CT Imaging
Safety
Overall, 7.9% (5/63) of subjects experienced a total of 9 mild-to-moderate adverse events, with 8 adverse events deemed by the investigator as probably not related to 64Cu-DOTATATE administration. Adverse events probably not related to administration of 64Cu-DOTATATE included 1 case each of nausea (grade 1), headache (grade 1), syncope (grade 2), melanoderma (grade 1), and flushing (grade 1) and 2 cases of vomiting (both grade 1). One subject (1.6%) experienced grade 2 hypertension that was determined by the investigator to be definitely not related to administration of 64Cu-DOTATATE. No subject experienced a serious adverse event.
No clinically significant changes from baseline in mean serum chemistry, hematology values, or vital signs (5, 10, 30, or 60 min after injection or at discharge) occurred. Additionally, no changes were observed in electrocardiogram parameters from baseline to 1 h after injection of 64Cu-DOTATATE.
DISCUSSION
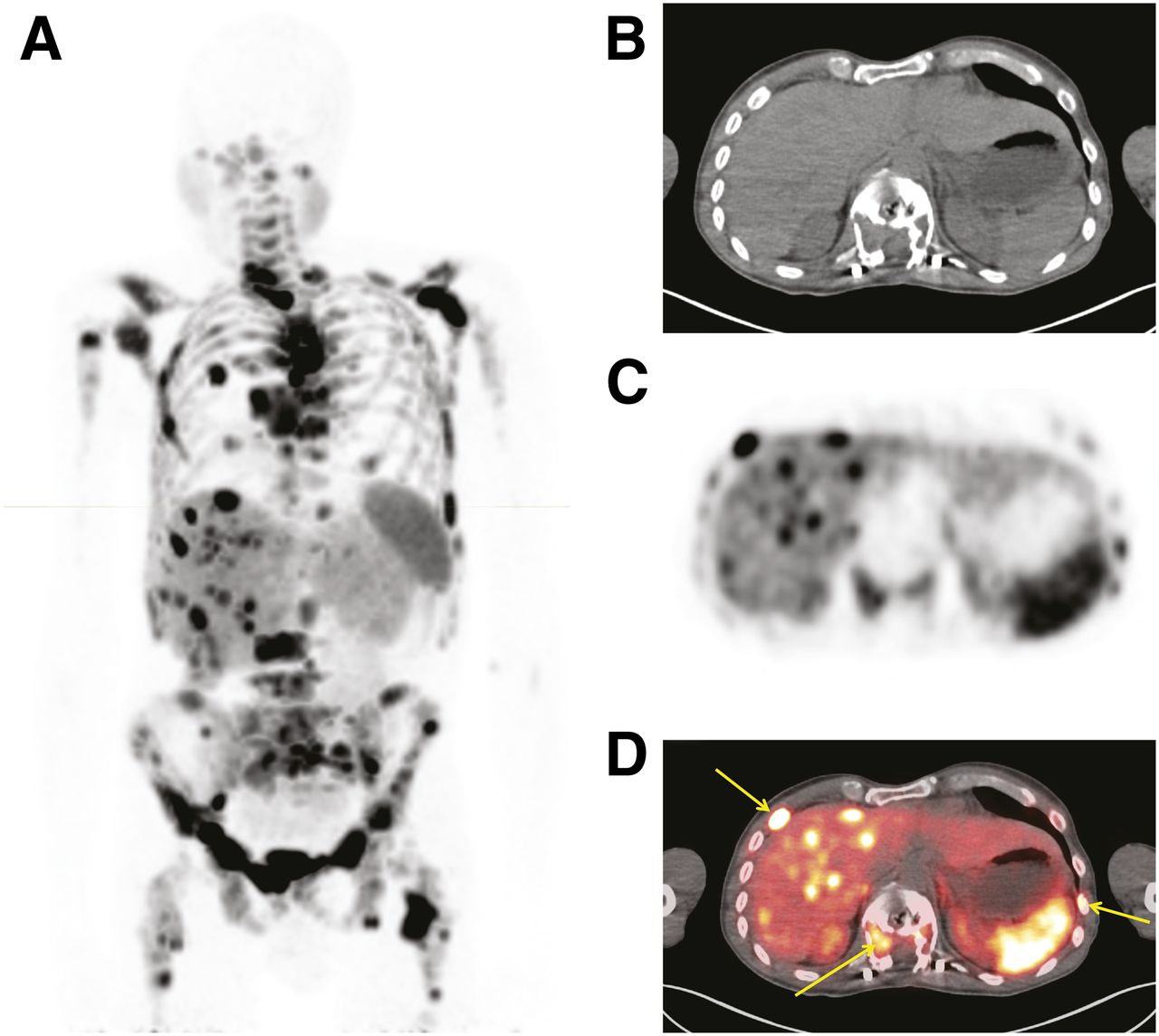
The current study demonstrated that PET/CT imaging with 148 MBq of 64Cu-DOTATATE is a safe and highly accurate approach to the diagnosis of NET-positive patients with SSTR-expressing tumors. We also showed that excellent-quality images can be rendered (Figs. 1 and 2) to facilitate high interreader and intrareader agreement on the presence or absence of metastatic or localized disease. The safety profile of 64Cu-DOTATATE proved excellent in our study, with no serious adverse events or adverse events related to 64Cu-DOTATATE.
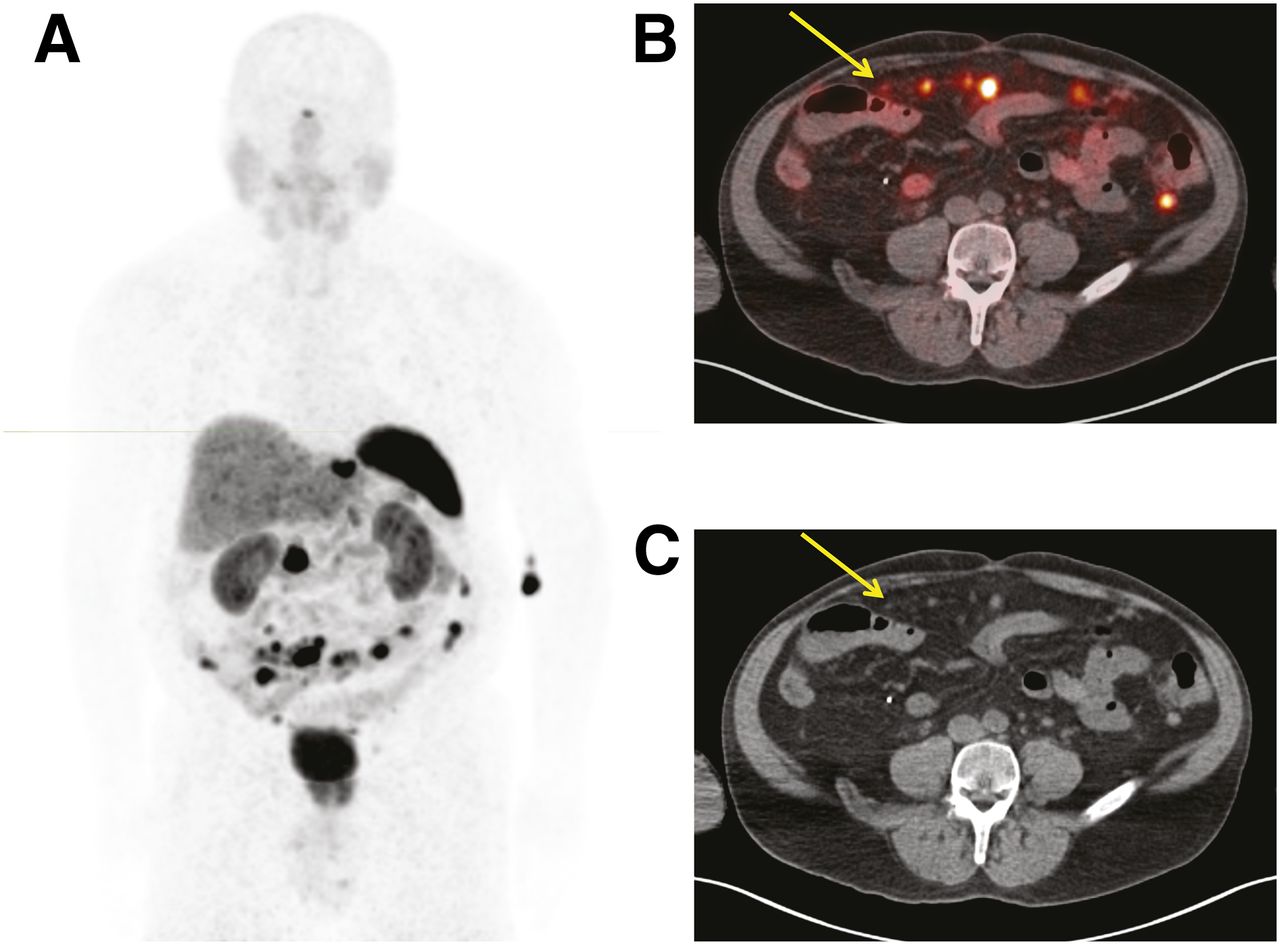
(A) Maximum-intensity-projection PET image of patient with metastatic small-bowel carcinoid tumor. (B and C) Small omental (arrow) and peritoneal tumor implants are visible in PET/CT (B) and corresponding CT (C) images.

(A) Maximum-intensity-projection PET image of patient with metastatic bronchial carcinoid and extensive metastatic disease, including multiple small liver metastases. (B and C) Corresponding CT (B), PET (C), and PET/CT (D) images showing multiple bone metastases (arrows).
The NET-positive instance misread by the SOT oncologist must be considered to accurately gauge the diagnostic performance of 64Cu-DOTATATE in this study. This misread might have been avoided with use of multiple oncologists or a multidisciplinary team to establish the SOT. However, we believe that use of the corrected individual and majority-read values provides an accurate evaluation of the diagnostic performance of 64Cu-DOTATATE.
Despite their previous use in PET radiopharmaceuticals, 64Cu-labeled ligands for PET imaging of NETs have been investigated in only a few studies (7–9). Of the available studies on patients with NETs, the first-in-humans study compared 64Cu-DOTATATE PET/CT with 111In-DTPA-octreotide SPECT/CT imaging in 14 patients with histopathologically confirmed NETs (9). Investigators reported excellent image quality, reduced radiation burden (6.3 vs. 12.0 mSv), and detection of additional lesions in 42.9% (6/14) of patients with 64Cu-DOTATATE (9). In a prospective head-to-head study of 112 patients with histopathologically confirmed NETs, 64Cu-DOTATATE PET/CT identified more true-positive NET patients, lesions, and additional organs with disease involvement than did 111In-DTPA-octreotide SPECT/CT (8). More recently, Johnbeck et al. showed that on a per-patient basis, 64Cu-DOTATATE and 68Ga-DOTATOC displayed the same 100% sensitivity, 90% specificity, 98% PPV, and 100% NPV (7). However, on a per-lesion basis, 64Cu-DOTATATE correctly identified more true-positive discordant lesions than did 68Ga-DOTATOC (83% vs. 17%) (7). Investigators attributed these findings to the physical properties of 64Cu-DOTATATE versus 68Ga-DOTATOC. In particular, investigators noted that the shorter positron range of 64Cu-DOTATATE likely translated to better spatial resolution, improved image quality, and superior detection of smaller lesions (7).
Unlike the aforementioned studies, which used higher radiotracer doses, we conducted a dose-ranging study and found that a lower (than previously published) 64Cu-DOTATATE dose of 148 MBq (4.2–5.1 mSv) provides diagnostic-quality PET/CT images. Our results are encouraging, as the radiation burden associated with the 148-MBq 64Cu-DOTATATE dose is lower than that of 111In-DTPA-octreotide and similar to 68Ga-labeled radiopharmaceuticals at the commercially available approximately 185-MBq (5 mCi) dose (7–9).
A strength of our study is the inclusion of many (21/63) NET-negative healthy volunteers. The preestablished 2:1 (positive-to-negative) ratio translates to a more robust determination of diagnostic performance, which was bolstered by the high interreader (κ = 0.76) and intrareader agreement (κ = 1.0 for 2 of the 3 readers). In diagnostic performance studies using only NET-positive patients, long-term follow-up is typically necessary to confirm initial NET-positive lesions as true-positives. The use of a large population of healthy volunteers and SOT eliminated the need for long-term follow-up and provided a more robust evaluation of specificity and NPV.
64Cu-DOTATATE offers several potentially practical advantages over 68Ga-DOTATATE. First, 64Cu-DOTATATE is a cyclotron-produced positron emitter that can be manufactured in large-scale with a well-controlled process at a centralized location. The production of 68Ga-DOTATATE, by contrast, is largely limited to major tertiary radiopharmacies with varying levels of quality control. The centralized and large-scale production of 64Cu-DOTATATE may ensure greater quality control and eliminate the need for a 68Ge/68Ga generator locally. Second, the longer half-life of 64Cu-DOTATATE than of 68Ga-DOTATATE (12.7 vs. 1.1 h) and centralized production may allow for wider geographic distribution, more flexible patient scheduling, and less strain for nuclear medicine technologists who must coordinate radioisotope delivery with patient and scanner availability. Third, the shorter positron range of 64Cu-DOTATATE and associated improvements in resolution may permit the detection of more or smaller lesions than those observed with 68Ga-DOTATATE. Fourth, the longer half-life of 64Cu-DOTATATE also may provide therapeutic benefits. For example, 64Cu-DOTATATE may permit delayed serial imaging with important implications for personalized dosimetry planning in peptide receptor radionuclide therapy, as well as aid in clarifying suspect findings observed on initial scans. Also, the 12.7-h half-life of 64Cu-DOTATATE may improve radioguided surgery using a dedicated positron hand-held probe (13).
CONCLUSION
64Cu-DOTATATE PET/CT is a safe and highly accurate imaging technique to detect SSTR-expressing NETs. In addition, diagnostic performance for 64Cu-DOTATATE PET/CT is highly reproducible and accurately identifies metastatic versus localized lesions. The longer half-life, lower positron energy, and lower positron range of 64Cu-DOTATATE than of 68Ga-labeled compounds makes 64Cu-DOTATATE a user-friendly radiopharmaceutical with the potential for practical and logistic benefits over currently approved radionuclide tracers used to identify patients with NETs.
DISCLOSURE
Research funding was provided by Curium and RadioMedix, Inc. Ebrahim S. Delpassand, David Ranganathan, Nilesh Wagh, Ali Abbasi, Andreas Kjaer, and Izabela Tworowska are employees and equity holders of RadioMedix. Andreas Kjaer is inventor on a patent covering 64Cu-DOTATATE PET for imaging of NETs in humans. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is 64Cu-DOTATATE PET/CT a potential alternative to 68Ga-labeled SSTR tracers for imaging in patients with NETs?
PERTINENT FINDINGS: The current study was the first U.S. phase III, prospective, reader-masked clinical trial and was conducted on a total of 63 subjects―42 patients with suspected or confirmed SSTR-positive NETs and 21 healthy volunteers known to be true-negative. The study confirmed an ALARA optimal dose for diagnostic-quality images at a lower (than previously published) radiation burden, which was safe, highly reproducible, and accurate for determining the absence or presence of localized or metastatic NET disease.
IMPLICATIONS FOR PATIENT CARE: 64Cu-DOTATATE PET/CT constitutes a viable, highly accurate imaging modality that may improve detection of NET lesions and increase access to high-quality PET/CT.
Acknowledgments
Editorial assistance was provided, under the direction of the authors, by John Lapolla and Chris Ontiveros, PhD (Synchrony Group, West Chester, Pennsylvania), and statistical assistance was provided by Dennis Clason (Statking Consulting, Fairfield, Ohio).
Footnotes
Published online Jan. 10, 2020.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication September 9, 2019.
- Accepted for publication January 3, 2020.





{kind=link}
{kind=link}