


Abstract
Somatostatin receptor scintigraphy is an accurate imaging modality for the diagnosis of neuroendocrine tumor. Because detection of distant metastases has a major impact on treatment, early diagnosis of metastatic spread is of great importance. So far, no standard procedure has become established for the early diagnosis of bone metastases from neuroendocrine tumor. We compared the diagnostic value of CT with that of the novel somatostatin analog 68Ga-1,4,7,10-tetraazacyclododecane-N,N′,N″,N′′′-tetraacetic acid-d-Phe1-Tyr3-octreotide (68Ga-DOTATOC) in the detection of such metastases. Methods: Fifty-one patients (22 women and 29 men; age range, 32–87 y) with histologically verified neuroendocrine tumor were included in this study. PET scans were fused with CT scans using a vacuum fixation device. 18F-NaF or 99mTc-dicarboxypropane diphosphonate bone scans or clinical follow-up served as the reference standard. Results: Twelve of the 51 patients had no evidence of bone metastases on any of the available imaging modalities, and 37 patients had 68Ga-DOTATOC PET results true-positive for bone metastases. 68Ga-DOTATOC PET results were true-negative for 12 patients, false-positive for one, and false-negative for another, resulting in a sensitivity of 97% and a specificity of 92%. 68Ga-DOTATOC PET detected bone metastases at a significantly higher rate than did CT (P < 0.001). Furthermore, conventional bone scans confirmed the results of somatostatin receptor PET but did not reveal additional tumors in any patients. Conclusion: 68Ga-DOTATOC PET is a reliable, novel method for the early detection of bone metastases in patients with neuroendocrine tumor. Our results show that CT and conventional bone scintigraphy are less accurate than 68Ga-DOTATOC PET in the primary staging or restaging of neuroendocrine tumor.
The diagnosis of neuroendocrine tumors is facilitated by radiolabeled somatostatin analogs, allowing accurate initial staging and confirming the possibility of therapy with radiolabeled somatostatin analogs in cases of metastasized, nonresectable neuroendocrine tumor (1–3).
Recently, it has been shown that 68Ga-1,4,7,10-tetraazacyclododecane-N,N′,N″,N′′′-tetraacetic acid-d-Phe1-Tyr3-octreotide (68Ga-DOTATOC) is a useful tool in initial staging and restaging of neuroendocrine tumor, providing more information on the extent of disease than CT can provide (4). 68Ga-DOTATOC PET significantly improves the quality of neuroendocrine tumor imaging, because diagnostic accuracy is higher with PET than with 111In-labeled compounds (5–7).
Early detection of bone metastases is clinically relevant because of the high prevalence of bone metastases in patients with advanced neuroendocrine tumor (8). Furthermore, bone involvement in neuroendocrine tumor is associated with a poor prognosis (9) and is a contraindication for extended surgical resection (10). Thus, diagnosis of bone metastases by different imaging strategies offers the possibility of adequate management at an early stage. Bone scintigraphy has been used for many years to detect bone metastases in patients with metastatic carcinoid tumors (11). Although conventional planar bone scintigraphy using 99mTc-biphosphonates is still the most common procedure to assess bone metastases, its specificity in differentiating metastases from benign processes is less than optimal (12). The results of conventional bone scintigraphy depend on local blood flow within the bone and on local osteoblastic activity. Furthermore, bone-seeking agents cannot depict bone marrow infiltration if there is no significant bone reaction.
18F-NaF PET has recently been proposed as a highly accurate diagnostic tool (13), but uptake of 18F-NaF reflects not only the presence of active tumor cells but also bone mineralization and remodeling. Therefore, the limitations of conventional bone scintigraphy also apply to 18F-NaF PET. Additionally, markers of bone metabolism have only limited value in the early detection of bone metastases. MRI of regions of interest is the most sensitive modality for detecting bone metastases in neuroendocrine tumor. In addition, MRI can be performed as a whole-body technique, although whether whole-body MRI is more accurate than CT and somatostatin receptor scintigraphy in detecting bone metastases from neuroendocrine tumor is not yet clear (14).
The potential advantages of conventional somatostatin receptor scintigraphy over bone scintigraphy in detecting neuroendocrine tumor metastases have been reported previously (15). The aim of our study was to compare the clinical value of 68Ga-DOTATOC PET with that of CT for the detection of bone involvement in neuroendocrine tumor patients. Conventional scintigraphic bone imaging and clinical follow-up were used as the reference standard.
MATERIALS AND METHODS
Patients
Fifty-one patients (22 women and 29 men; age range, 32–87 y) were included in this retrospective investigation. The patients were referred to our department for somatostatin receptor imaging of histologically proven neuroendocrine tumor (Table 1). Eleven patients had neuroendocrine tumor originating from the pancreas, 5 from the lung, 3 from the stomach, and 10 from an unknown site. In 1 patient, the neuroendocrine tumor originated from the prostate gland, whereas the primary was the colon in 3 patients, the small bowel in 15 patients, the rectum in 2 patients, and the anal region in 1 patient. Forty-nine patients had liver metastases, and 33 had lymph node metastases.
Patient Characteristics
Before referral, 27 patients had been treated surgically and 5 had received chemotherapy. Three patients had undergone treatment with long-acting somatostatin analogs alone or in combination with interferon-α, and 2 patients had already undergone chemoembolization of liver metastases.
Sites of 68Ga-DOTATOC uptake were confirmed to be bone metastases through either 18F-NaF PET (34 patients) or bone scintigraphy with 99mTc-dicarboxypropane diphosphonate (21 patients). In 31 patients, PET/CT was repeated at 6 mo for restaging after peptide receptor–mediated radionuclide therapy (16).
18F-FDG PET was available in 25 patients. Seventeen patients had undergone MRI of regions of interest for further assessment of bone metastases.
A history of bone pain was documented through questionnaires (developed by the European Organization for Research and Treatment of Cancer) given to each in-patient on admittance. Furthermore, the referring physician was asked to provide a written report of any changes in bone pain observed during the period of therapy.
Datasets for image fusion were included if the 2 modalities had been performed within 1 mo of each other. In 36 patients, the presence of bone metastases was confirmed by repeating PET/CT 6 mo after the initial PET/CT examination. In the remaining 15 patients, this follow-up was not possible: 11 had died, and 4 did not return to our institution for PET/CT restaging. In all patients, bone scintigraphy was used to confirm bone involvement. All images were evaluated by 2 experienced specialists in nuclear medicine or radiology. Written informed consent for each imaging procedure was obtained from all patients.
68Ga-DOTATOC PET
Preparation of 68Ga-DOTATOC was based on a fully automated synthesis, as described previously (17).
The patients received 150 MBq of 68Ga-DOTATOC (20–30 μg), and the acquisition began 60–90 min afterward. Imaging was performed on a dedicated PET scanner (Advance; GE Healthcare) with a 15-cm axial field of view and a 55-cm transaxial field of view. Imaging was performed in 2-dimensional mode using septa, at 5 min/bed position in emission mode. Images were acquired at 7 bed positions from the head to the mid thigh. Attenuation correction was performed by means of transmission data obtained with a 67Ge pin source at 3 min/bed position. Ordered-subsets expectation maximization was used for image reconstruction, including segmented attenuation correction and model-based scatter correction. For iterative reconstruction, 2 iterations and 26 subsets were used, with an interupdate filter of 4 mm in full width at half maximum and a postprocessing filter of 6 mm in full width at half maximum. Attenuation correction consisted of segmented correction with 10-mm smoothing, excluding axial smoothing.
18F-NaF PET
The patients received 180 MBq of 18F-NaF. Images were obtained by a dedicated PET scanner (Advance) as described for 68Ga-DOTATOC PET, starting 2 h after application.
18F-FDG PET
Ninety minutes after application of 370 MBq of 18F-FDG, PET was performed on a dedicated PET scanner (Advance) using the protocol described for 68Ga-DOTATOC PET. The patients had fasted for at least 8 h.
99mTc-Dicarboxypropane Diphosphonate Bone Scintigraphy
Planar whole-body bone scintigraphy was performed 3–4 h after intravenous injection of 555 MBq of 99mTc-dicarboxypropane diphosphonate, using a double-head γ-camera (e-cam high definition 4, dual-detector system; Siemens) with a low-energy, high-resolution collimator and the energy window centered on the technetium photopeak of 140 keV. SPECT of the abdomen or thorax was performed if the planar imaging findings were equivocal. Tracer uptake was considered to be abnormal if it represented a change from previous bone scan findings or could not otherwise be explained.
CT and Image Registration
All patients underwent 68Ga-DOTATOC PET and contrast-enhanced CT to obtain fused images of histologically proven neuroendocrine tumor. PET and CT scans were usually performed within 2 d of each other. The torso was scanned with helical CT, using a slice thickness of 3 mm on a Somatom Sensation CT scanner (Siemens Medical Solutions). Depending on body weight, 100–150 mL of nonionizing contrast medium (Visipaque 320; GE Healthcare) were administered at a rate of 4 mL/s, followed by imaging after 30 s (late arterial phase) and after 70 s (portal phase). Accurate alignment for image fusion was facilitated by reproducible positioning of the patients on vacuum mattresses during both the PET and the CT acquisitions. Image datasets were coregistered by identifying external markers that had been attached to the fixation device, using a navigation system (Treon StealthStation; Medtronic).
MRI
All MRI examinations were performed on a 1.5-T whole-body system (Magnetom Avanto; Siemens Medical Solutions). Whole-body MRI was performed on 4 patients. Using the integrated body matrix receiver coil system and automated table motion, we applied parallel-acquisition breath-hold technique in 3 spatial directions at a maximum imaging range of 205 cm, without patient repositioning. The patients were examined from the head to the calves with short-τ inversion recovery sequences at 4 body levels in coronal orientation: head/neck/upper thorax (repetition time [TR], 10,000/echo time [TE], 83), lower thorax/abdomen (TR, 6,100/TE, 87), pelvis/thigh (TR, 8,800/TE, 80), and knee/calves (TR, 8,000/TE, 86). Subsequently, the same regions were examined with coronal T1-weighted turbo spin-echo imaging (TR, 532–654/TE, 11). The slice thickness in all sequences was 5 mm.
In 13 patients, sagittal T1-weighted turbo spin-echo (TR, 500/TE, 11) and short-τ inversion recovery (TR, 4,990/TE, 36) sequences were obtained at 2 levels (cervical/upper thoracic spine and lower thoracic/lumbar spine), with a slice thickness of 3 mm.
Image Interpretation
PET and SPECT scans were interpreted by an experienced nuclear medicine physician, and CT scans were interpreted independently by a radiologist. The interpreters had clinical information obtained from the patient's referring physician but no information on the other imaging modality. The criterion for malignancy was clear demarcation of the lesion, with tracer accumulation higher than that in the liver and higher than physiologic activity.
After the independent interpretation, the nuclear medicine physician and radiologist did a consensus reading with lesion-by-lesion analysis and discussed their findings. The PET/CT results were then compared with PET or SPECT bone scintigraphy, which was considered the gold standard for diagnosing bone metastases (18). The results were considered concordant if both modalities showed clear signs of malignancy. In the case of discordant results, further available imaging results, such as those of 18F-FDG PET or MRI, were assessed if those studies had been done within 1 mo before or after the PET/CT. Follow-up control imaging within 6 mo was done on 36 patients. Findings were considered positive if they corresponded to specific, previously described aspects of malignant disease from neuroendocrine tumor (19–22).
All findings were controlled for being true-positive or true-negative. If the results of scintigraphic imaging corresponded to conventional imaging or surgical results, or if follow-up confirmed initial findings after half a year, lesions were considered true-positive. Lesions not visible on scintigraphy but confirmed on radiologic imaging or surgery were considered false-negative. Scintigraphic lesions suggestive of bone involvement but without radiologic or histologic confirmation on exploration were considered false-positive.
CT findings were considered positive if they corresponded to a specific, previously described appearance of malignant disease from neuroendocrine tumor (23).
Assessment of Laboratory Parameters
Alkaline phosphatase, lactate dehydrogenase, chromogranin A, and neuron-specific enolase were measured in all patients. Alkaline phosphatase, lactate dehydrogenase, and neuron-specific enolase were measured using a Modular Analytics system (Roche Diagnostics). Chromogranin A was measured using a BEP 2000 automated analyzer (Dade Behring).
Statistical Analysis
The statistical significance of differences in sensitivity and specificity between 68Ga-DOTATOC PET, CT, fusion, and scintigraphic imaging was calculated using the χ2 test, and differences on a per-patient and per-lesion basis were evaluated using the McNemar test.
Statistical analysis was done using the R system for statistical computation (24). The Pearson χ2 test with Yates continuity correction and the Fisher exact test for count data were performed on all contingency tables by means of batch processing.
RESULTS
68Ga-DOTATOC PET was true-positive in 37 of the 51 patients, revealing somatostatin receptor–positive bone metastases. These findings were obtained independently of clinical symptoms suggestive of bone metastases, such as pain, pathologic fractures, or hypercalcemia. PET findings were true-negative in 12 patients, false-positive in 1 patient, and false-negative in 1 patient.
The 1 false-positive PET finding was interpreted correctly as negative on restaging half a year after the initial imaging. One female patient showed a false-negative result because of low 68Ga-DOTATOC uptake. In 37 patients, PET/CT as the initial staging procedure revealed bone metastases.
Twenty-one patients showed concordant positive findings on CT and 68Ga-DOTATOC PET, whereas in 12 patients the 2 modalities had concordant negative findings. One false-negative finding on 68Ga-DOTATOC PET was true-positive on CT and 18F-NaF, and 17 false-negative findings on CT were true-positive on 68Ga-DOTATOC PET. At the time of the baseline study, the bone metastases diagnosed on 68Ga-DOTATOC PET were also seen on either 18F-NaF PET or bone scintigraphy. However, in 4 patients with lesions that were suggestive on 68Ga-DOTATOC PET but had no correlate on bone scans, PET findings were confirmed by PET/CT follow-up 6 mo after initial staging, revealing signs of bone metastases on CT that corresponded to focal tracer uptake on PET. Concerning detection of bone involvement, CT had a sensitivity of 58%, compared with 97% for 68Ga-DOTATOC PET. The specificity was 100% versus 92%, respectively, providing a significance level of P < 0.001 (Table 2).
Comparison of PET and CT in Detection of Bone Metastases from Neuroendocrine Tumor
Thirteen patients showed diffuse osseous spread throughout the body. Twelve patients had bone metastases spreading to the trunk and 2 to the ribs. Eleven patients had bone metastases in the vertebral spine, 6 in the skull, 2 in the pelvic bone, 2 in the humerus, 1 in the scapula, and 1 in the femur.
Of these patients, 7 with diffuse metastatic bone disease, 3 with metastases to the trunk, and 2 with metastases to the spine experienced bone pain. Of the patients with bone metastases, 95% had liver metastases and 71% had lymph node metastases. All except one functionally active tumor (3 of unknown primary, 1 colonic, 4 small bowel, 2 pancreatic neuroendocrine, and 1 rectal) had positive findings for bone metastases. One patient with Zollinger–Ellison syndrome that was due to a functionally active gastric neuroendocrine tumor did not show bone metastases.
Nineteen patients already had bone metastases at the time of the initial diagnosis, 7 patients had an onset of bone metastases within 1 y after diagnosis, and in 12 patients the onset was more than 1 y after diagnosis.
In 17 of 51 patients, MRI was performed along with 68Ga-DOTATOC PET to confirm scintigraphic findings. Four patients underwent whole-body MRI, and in 13 patients the MRI was restricted to dedicated regions of interest. In 12 of these patients, MRI showed signs of bone metastases (Table 3). In 2 patients, neither 68Ga-DOTATOC PET nor MRI showed any sign of bone metastases. In the remaining 3 patients, MRI was negative for bone metastases, but the bone lesions seen on 68Ga-DOTATOC PET were confirmed in 2 patients through 18F-NaF PET (osteoblastic) and in 1 patient through 18F-FDG PET (osteolytic). In 2 patients, MRI was positive for bone metastases whereas 68Ga-DOTATOC PET showed no signs of bone metastases. In 1 of these 2 patients, the positive MRI findings were confirmed by 18F-NaF PET. In the other patient, CT and bone scintigraphy showed no signs of bone involvement. Whole-body MRI showed concordant negative findings in 1 patient and a concordant positive finding in 1 patient but, in 2 patients, did not show a single skull metastasis that had been correctly diagnosed on 68Ga-DOTATOC PET and confirmed by 18F-NaF PET.
Comparison of MRI and 68Ga-DOTATOC PET in Number of Bone Metastases Detected
In the group of patients who underwent PET with all 3 tracers, 6 patients had findings positive for bone metastases with all tracers, 7 patients had negative findings with all tracers, 5 patients had negative findings only with 18F-FDG, and 1 patient had positive findings only with 18F-FDG and 18F-NaF (Table 4).
Comparison of 18F-NaF, 18F-FDG, and 68Ga-DOTATOC PET in Number of Bone Metastases Detected
Within the group of 31 patients who underwent PET/CT restaging half a year after the initial somatostatin receptor imaging, the initial PET findings were confirmed in 30 patients. One false-positive PET result was true-negative on the follow-up control study.
18F-FDG PET was performed on 25 patients and was concordant with the findings of 68Ga-DOTATOC PET in 22 patients, 15 of whom were positive and 7 negative for bone metastases. Three patients, however, did not show bone involvement on 18F-FDG PET but were positive for osteoblastic bone metastases on 68Ga-DOTATOC PET.
Analysis on a Neuroendocrine-Tumor Basis
Of a total of 673 bone lesions detected on 68Ga-DOTATOC PET, 346 were visualized on both PET and CT, and 129 of 673 were visualized in addition on PET/CT. One patient showed bone marrow infiltration only on bone scintigraphy. This finding was confirmed by MRI. In 27 patients, PET and CT showed complementary results on a lesion-based analysis, including patients showing no bone metastases on conventional bone scintigraphy.
Bone Metastases and Tumor Markers
The possible predictive value of alkaline phosphatase, lactate dehydrogenase, chromogranin A, and neuron-specific enolase were evaluated, but none showed significant sensitivity or specificity in the detection of bone involvement in neuroendocrine tumor patients (Tables 5–8⇓⇓⇓). Furthermore, in 12 patients with pain due to bone metastases, these laboratory parameters showed no significant correlation with the course of bone pain.
Alkaline Phosphatase Values and Bone Metastases
Lactate Dehydrogenase Values and Bone Metastases
Chromogranin A Values and Bone Metastases
Neuron-Specific Enolase Values and Bone Metastases
DISCUSSION
Somatostatin receptor imaging with PET has become a widely accepted modality in patients with neuroendocrine tumor. Recently, we have shown that 68Ga-DOTATOC PET is more accurate than conventional somatostatin receptor scintigraphy or CT in the staging of patients with neuroendocrine tumor (4).
When comparing PET to planar somatostatin receptor scintigraphy and SPECT, PET provides a substantially higher resolution and 3-dimensional anatomic information, which leads to superior sensitivity and specificity (25). The higher spatial resolution of PET together with a well-adapted imaging protocol allows for more precise image interpretation. By permitting the clear depiction of even small lesions, the high sensitivity and specificity of PET in primary staging and restaging (26) provide additional information not gained by other imaging modalities. PET also has the advantage of higher receptor affinity in the case of 68Ga-DOTATOC, as emphasized in the literature (5). Furthermore, imaging of tumor cell characteristics such as the expression of somatostatin receptors offers a higher sensitivity and specificity in the detection of bone metastases, in comparison with scintigraphic imaging of bone metabolism.
Because bone metastases in neuroendocrine tumor worsen prognosis, early awareness of them plays an important role in the management of therapy, allowing it to begin earlier or to be changed to symptomatic palliation (15).
Radiographic signs of bone metastases are often subtle and can be missed easily, as is reflected by the much lower sensitivity of CT detection than of PET detection in our study (Fig. 1). Up to now, CT has been the state of the art for whole-body morphologic imaging of neuroendocrine tumor. However, MRI of regions of interest has been described as the most sensitive imaging modality for the detection of bone metastases in neuroendocrine tumor (27). Furthermore, whole-body MRI is not yet the standard imaging procedure for staging neuroendocrine tumor. At our institution, whole-body MRI is not routinely done, because the scans take a long time to acquire and are inconvenient to patients. One published report comparing whole-body MRI with somatostatin receptor scintigraphy recommends that the latter be combined with MRI of the spine as the most accurate method for detecting bone metastases in neuroendocrine tumor (14). The findings of that study correlate with our findings, as 2 of the 4 patients who had undergone whole-body MRI had false-negative MRI findings for bone metastases of the skull.

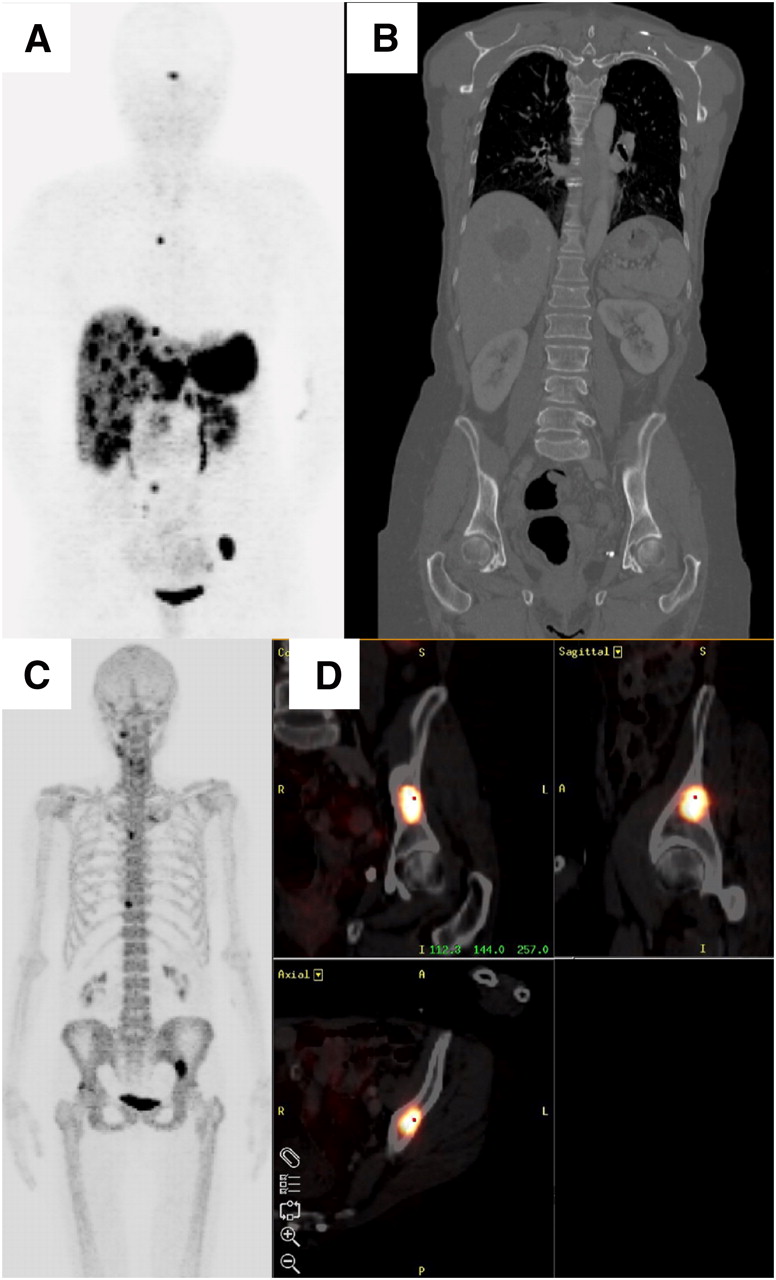
A 68-y-old woman with metastatic neuroendocrine tumor of small bowel: (A) 68Ga-DOTATOC PET depicts diffuse liver metastases and bone metastases to thoracic spine and left iliac bone. (B) CT does not show bone metastases to left iliac bone. (C) 18F-NaF PET shows bone metastases to thoracic spine and left iliac bone. (D) PET/CT confirms metastases to bone of left hip.
However, 2 patients did not show consistent findings, and PET/CT was mandatory to clarify the findings in an interdisciplinary approach. One false-positive finding on 68Ga-DOTATOC PET in a patient with neuroendocrine tumor was caused by extensive vertebral osteophytes with an inflammatory component that showed moderate 68Ga-DOTATOC uptake. CT did not reveal signs of bone metastases in this patient but showed extensive degenerative changes. In this patient, 68Ga-DOTATOC PET on restaging was true-negative. One false-negative finding on 68Ga-DOTATOC PET was in a patient with neuroendocrine tumor of the bronchi. CT, 18F-NaF, and 18F-FDG PET confirmed metastatic tumors in this patient. The false-negative findings may have been due to the fact that dedifferentiated metastases of neuroendocrine tumor are not visible on scintigraphic images because of low, or an absence of, somatostatin receptor expression. Patients with 68Ga-DOTATOC uptake in only part of the known tumors may have a variation in tumor cell differentiation. Hence, dedifferentiation of parts of the tumor should be excluded. 18F-FDG PET can be used to confirm lesions with high glucose metabolism.
Bone scintigraphy and octreotide scintigraphy can provide complementary information on the presence of bone metastases. However, the detection of bone metastases from carcinoid tumors by bone scintigraphy is hampered by several factors, such as the low resolution of planar scintigraphy (23). Furthermore, bone scintigraphy cannot always distinguish active metastases from a repair process. In the literature, the percentage of patients having neuroendocrine tumor with bone metastases diagnosed by scintigraphy has ranged from 4% (23) to 12% (28,29). Further studies have reported that in 7%−15% of patients with neuroendocrine tumor, metastases to the bone have been diagnosed (26,30,31).
Compared with conventional bone scintigraphy, 18F-NaF PET has the potential to detect bone metastases with increased sensitivity.
The number of lesions detected by 68Ga-DOTATOC PET is higher than that detected by bone scintigraphy, and scintigraphic procedures showed bone lesions not seen by the radiologic techniques. An explanation is the higher resolution of PET than of SPECT, allowing PET to depict smaller lesions and lesions with low expression of human somatostatin receptor subtype 2. Because bone scintigraphy detects metastases that include osteoblastic reaction and PET detects lesions that are somatostatin receptor–positive, lesions with different imaging characteristics can be detected. However, 1 patient in this study showed bone marrow infiltration on bone scintigraphy, and the finding was proven by MRI. Bone marrow infiltration in this patient caused an osteoblastic reaction in the cortical bone. Although 18F-NaF PET showed an even higher number of lesions in the bone, 68Ga-DOTATOC PET was superior in the initial detection of still-unknown bone involvement in neuroendocrine tumor and thereby had implications for therapeutic management.
In addition, a malignant bone disease that has been treated may remain abnormal on CT but will not show 68Ga-DOTATOC uptake anymore. 18F-FDG PET may be helpful in the diagnosis of metastasis with high anaerobic glycolysis and low somatostatin receptor expression. As published earlier, MRI has been the most sensitive modality for detection of bone metastases in neuroendocrine tumor (32–35) but is usually done to investigate regions of the body suspected of harboring bone metastases.
The incidence of bone metastases in this patient cohort was 74.5%. Similar studies have shown that 7%−15% of patients with neuroendocrine tumor have bone metastases (26,29–31). The incidence in our study was high because the patients, who had been referred for radionuclide-peptide therapy, were already in an advanced stage of disease (Fig. 2). However, it is unlikely that this referral bias could have influenced the results of this comparative study. Furthermore, there was no preferential primary site of bone metastases and no significant correlation between the primary site and the incidence of bone metastases, as confirms earlier reports (18).
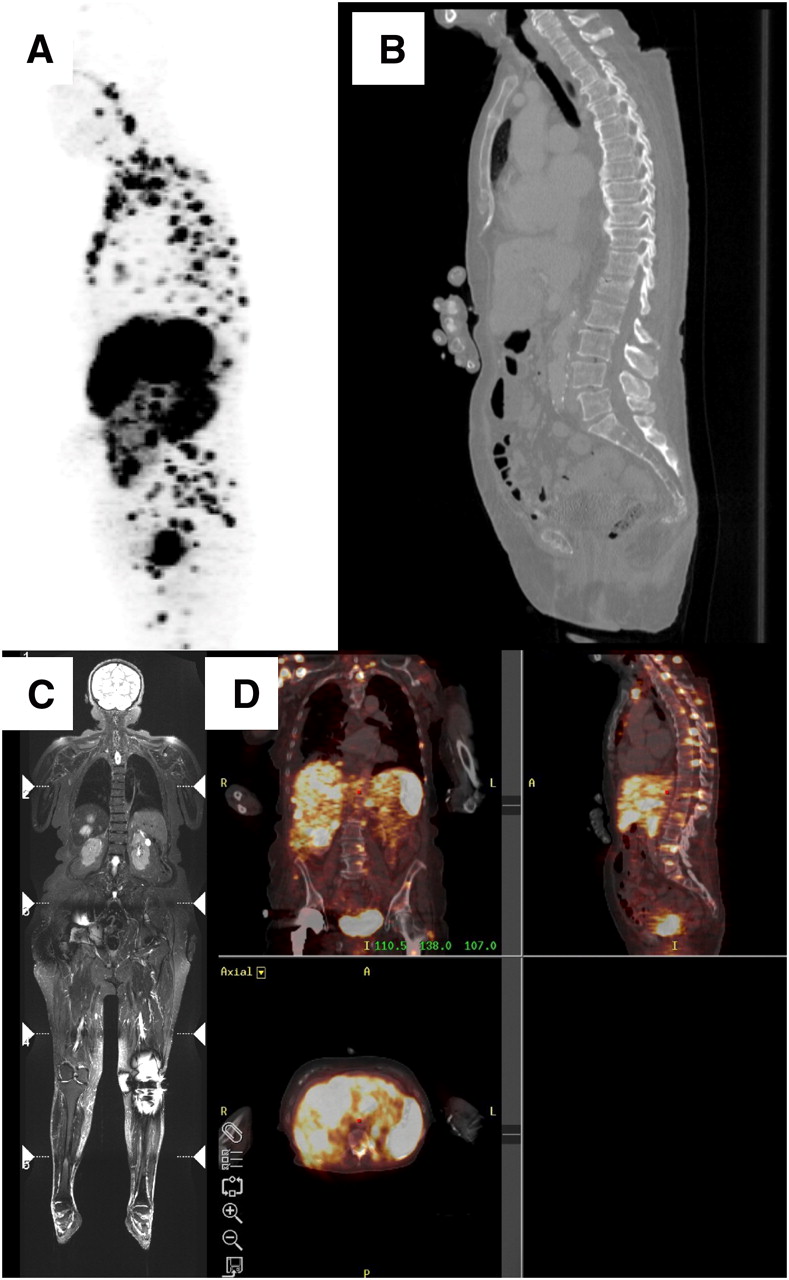
A 78-y-old woman with neuroendocrine tumor of unknown primary: (A) 68Ga-DOTATOC PET depicts diffuse bone metastases. (B) CT shows only part of widespread bone involvement. (C) Widespread bone involvement is clearly seen on MRI. (D) PET/CT confirms multiple bone lesions, not all of which were detected on CT.
However, the time between disease onset and the appearance of bone metastases ranges widely, and the disease often shows an indolent course. Pain still is the principal symptom in neuroendocrine tumor patients who have slowly growing metastases to the axial skeleton (18). That is why we closely monitored changes in tumor-associated pain, using the questionnaire of the European Organization for Research and Treatment of Cancer and requesting written reports from the referring medical institution about changes in pain. However, the presence of bone pain in these patients did not correlate with any clinical parameters of bone metabolism, demonstrating the need for another reliable diagnostic tool for the early presence of bone metastases in neuroendocrine tumor.
Clinical parameters did not prove to be reliable indicators of the presence of bone metastases in this patient group. When patients with elevated chromogranin A, neuron-specific enolase, alkaline phosphatase, and lactate dehydrogenase were compared with patients who had at least one of these parameters within the physiologic limit, no significant difference could be observed. Thus, discrepancies between the clinical parameters and the scintigraphic findings should still lead to further clinical investigation of suspected bone metastases. 68Ga-DOTATOC PET, as an imaging method of high sensitivity, allows for early diagnosis of bone involvement in neuroendocrine tumor and reveals asymptomatic bone metastases.
CONCLUSION
Our study proved that 68Ga-DOTATOC PET is more useful than CT for the early detection of bone metastases in patients with neuroendocrine tumor. Negative 68Ga-DOTATOC PET findings in a patient with neuroendocrine tumor exclude the presence of somatostatin receptor–positive bone metastases. 68Ga-DOTATOC PET should replace conventional bone scintigraphy in patients with neuroendocrine tumor.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 14, 2008.
- Accepted for publication April 16, 2009.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 64Cu-DOTATATE PET in Patients with Neuroendocrine Neoplasms: Prospective, Head-to-Head Comparison of Imaging at 1 Hour and 3 Hours After Injection
- Safety, tolerability and clinical implementation of 'ready-to-use 68gallium-DOTA0-Tyr3-octreotide (68Ga-DOTATOC) (SomaKIT TOC) for injection in patients diagnosed with gastroenteropancreatic neuroendocrine tumours (GEP-NETs)
- Appropriate Use Criteria for Somatostatin Receptor PET Imaging in Neuroendocrine Tumors
- Current Concepts in 68Ga-DOTATATE Imaging of Neuroendocrine Neoplasms: Interpretation, Biodistribution, Dosimetry, and Molecular Strategies
- Bone metastases and skeletal-related events from neuroendocrine tumors
- 68Ga-DOTATATE PET/CT, 99mTc-HYNIC-Octreotide SPECT/CT, and Whole-Body MR Imaging in Detection of Neuroendocrine Tumors: A Prospective Trial
- Quantitative and Qualitative Intrapatient Comparison of 68Ga-DOTATOC and 68Ga-DOTATATE: Net Uptake Rate for Accurate Quantification
- The Role of 68Ga-DOTATATE PET/CT in Suspected Neuroendocrine Tumors
- Nuclear medicine imaging of neuroendocrine tumours
- Radiopeptide Imaging and Therapy in Europe
- Response and Long-Term Control of Bone Metastases After Peptide Receptor Radionuclide Therapy with 177Lu-Octreotate
- Incidence of Increased 68Ga-DOTANOC Uptake in the Pancreatic Head in a Large Series of Extrapancreatic NET Patients Studied with Sequential PET/CT