


Abstract
In this investigation, the efficacy of scintigraphy using 99mTc-labeled hydrazinonicotinyl-Tyr3-octreotide (HYNIC-TOC) in the evaluation of extraadrenal pheochromocytoma was assessed and compared with 131I-labeled metaiodobenzylguanidine (MIBG) imaging. Methods: Ninety-seven patients who were suspected of having pheochromocytoma but showed no definite adrenal abnormalities on CT were evaluated by both 99mTc-HYNIC-TOC scintigraphy and 131I-MIBG imaging. The results were compared with pathology findings or clinical follow-up. Results: Of 58 patients proven to be without pheochromocytoma, 99mTc-HYNIC-TOC and 131I-MIBG imaging excluded 56 and 58 patients, respectively, rendering a specificity of 96.6% for 99mTc-HYNIC-TOC imaging and 100% for 131I-MIBG imaging. In the evaluation of adrenal pheochromocytoma (14 patients), the sensitivity of 99mTc-HYNIC-TOC scintigraphy and 131I-MIBG imaging was 50% and 85.7%, respectively. However, in the evaluation of extraadrenal pheochromocytomas (25 patients), the sensitivity of 99mTc-HYNIC-TOC scintigraphy and 131I-MIBG imaging was 96.0% and 72.0%, respectively. Conclusion: 99mTc-HYNIC-TOC scintigraphy is more sensitive than 131I-MIBG imaging in the detection of extraadrenal pheochromocytomas.
- extraadrenal pheochromocytoma
- 99mTc-hydrazinonicotinyl-tyr3-octreotide (HYNIC-TOC)
- metaiodobenzylguanidine (MIBG)
Extraadrenal pheochromocytomas arise within the sympathetic nervous system and originate from the neural crest. They can be located in sympathetic ganglions anywhere from the neck to the pelvis. As opposed to the traditional teaching that 10% of all pheochromocytomas are at extraadrenal sites, the real incidence of extraadrenal pheochromocytomas is much higher (1,2). Up to 40% of extraadrenal pheochromocytomas can be malignant and may be unexpected at the time of the initial imaging. 123I- or 131I-labeled metaiodobenzylguanidine (MIBG) imaging is the main nuclear medicine modality in the evaluation of pheochromocytoma. However, the sensitivity of 131I-MIBG imaging is significantly lower in the diagnosis of extraadrenal pheochromocytoma than in the diagnosis of adrenal pheochromocytoma (3,4). Somatostatin receptor imaging using 111In-labeled octreotide is also known to have value in the evaluation of pheochromocytoma (5). In addition, 68Ga-labeled DOTA-Tyr3-octreotide (DOTATOC), as a somatostatin analog and a PET tracer, has great potential for accurate diagnosis of a variety of neuroendocrine tumors (6–8) because of the superior resolution and quantitative ability of modern PET and PET/CT scanners. However, experience with 68Ga-DOTATOC in the evaluation of pheochromocytoma is still limited. Recently, 99mTc-labeled octreotides have also been used in the evaluation of several different types of malignancies (9–11). It was reported that 99mTc-hydrazinonicotinyl-Tyr3-octreotide (HYNIC-TOC) achieved higher tumor–to–normal-tissue ratios than did 111In-labeled octreotide and, therefore, had higher sensitivity than did 111In-labeled octreotide as an imaging agent for the localization of somatostatin receptor–expressing tumors (12). In this investigation, the efficacy of 99mTc-labeled octreotide HYNIC-TOC scintigraphy in the detection of both adrenal and extraadrenal pheochromocytoma was assessed and compared with 131I-MIBG imaging.
MATERIALS AND METHODS
Patients
In this retrospective investigation, 1,001 charts of patients with unexplainable hypertension and suspected pheochromocytomas, referred nationwide to our institution, were reviewed. All patients had symptoms such as profuse sweating, tachycardia, and headache. These patients were referred to us for imaging studies evaluating for possible pheochromocytoma. However, only those patients with postsurgical pathologic confirmation of the lesions or those with clinical follow-up for more than 1 y were included in our analysis. In addition, only those patients whose abdominal CT scans (within 4 mo before 131I-MIBG imaging) revealed either no adrenal abnormalities or ambiguous findings underwent both 131I-MIBG imaging and 99mTc-HYNIC-TOC scintigraphy. Because our surgeons preferred that at least 2 different imaging modalities be positive before surgery, both 131I-MIBG imaging and 99mTc-HYNIC-TOC scintigraphy were generally performed. Those patients with definite adrenal abnormality on CT underwent 131I-MIBG studies but not 99mTc-HYNIC-TOC scintigraphy and therefore were not included in our analysis. 131I-MIBG imaging and 99mTc-HYNIC-TOC scintigraphy were performed within a 2-wk interval. Ninety-seven patients (53 male and 44 female; age range, 8–75 y ) met the criteria to be included in the final analysis. The 99mTc-HYNIC-TOC and 131I-MIBG images were interpreted by 2 experienced nuclear medicine physicians who were unaware of other clinical and imaging information. The chart review and image analysis for the patients in this study were approved by the institutional review board.
99mTc-HYNIC-TOC Scintigraphy
99mTc-HYNIC-TOC was synthesized and labeled according to a method published previously (13). Images were also acquired following a published protocol (13). The images were interpreted jointly by 2 experienced nuclear medicine physicians who were aware of neither the histopathologic diagnosis nor the previously reported interpretation of the 99mTc-HYNIC-TOC scintigraphy findings.
131I-MIBG Imaging
Each patient was given a potassium perchlorate preparation for 5 d, starting 3 d before the 131I-MIBG administration. Twenty-four hours after intravenous administration of 1.48 MBq of 131I-MIBG per kilogram of body weight, whole-body images were acquired using a dual-head γ-camera with a window setting of 364 keV.
RESULTS
No patients had any complaints related to the 99mTc-HYNIC-TOC or 131I-MIBG administration. For all patients in whom pheochromocytoma was ultimately confirmed to be present, both readers correctly interpreted the images as positive for pheochromocytoma. There was no interreader disagreement. The image findings were compared with the final histopathologic diagnosis of the removed tumors after surgery and biopsy (n = 42) and clinical follow-up for more than 1 y (n = 55).
Patients Without Pheochromocytoma
Fifty-eight patients were proven not to have pheochromocytoma. Among these, 99mTc-HYNIC-TOC scintigraphy excluded 56, for a specificity of 96.6% (56/58). Both false-positive interpretations of pheochromocytomas on 99mTc-HYNIC-TOC scintigraphy were due to 99mTc-HYNIC-TOC uptake by adrenal carcinomas. 131I-MIBG imaging was negative in all 58 patients, for a specificity of 100.0% (58/58).
Patients with Pheochromocytomas
Thirty-nine patients had pheochromocytomas confirmed by either histopathologic examination after surgery and biopsy (n = 37) or clinical follow-up and other studies (n = 2). The tumors of 14 patients were in the adrenal glands, whereas 25 patients had extraadrenal lesions. On a per-patient basis, 99mTc-HYNIC-TOC scintigraphy identified 31 patients with pheochromocytoma, for a sensitivity of 79.5% (31/39). The sensitivity of 131I-MIBG imaging was 82.1% (32/39), or slightly higher than the sensitivity of 99mTc-HYNIC-TOC scintigraphy.
Of the 14 adrenal pheochromocytomas, 99mTc-HYNIC-TOC scintigraphy identified only 50% (7/14). In contrast, 131I-MIBG imaging revealed 85.7% (12/14).
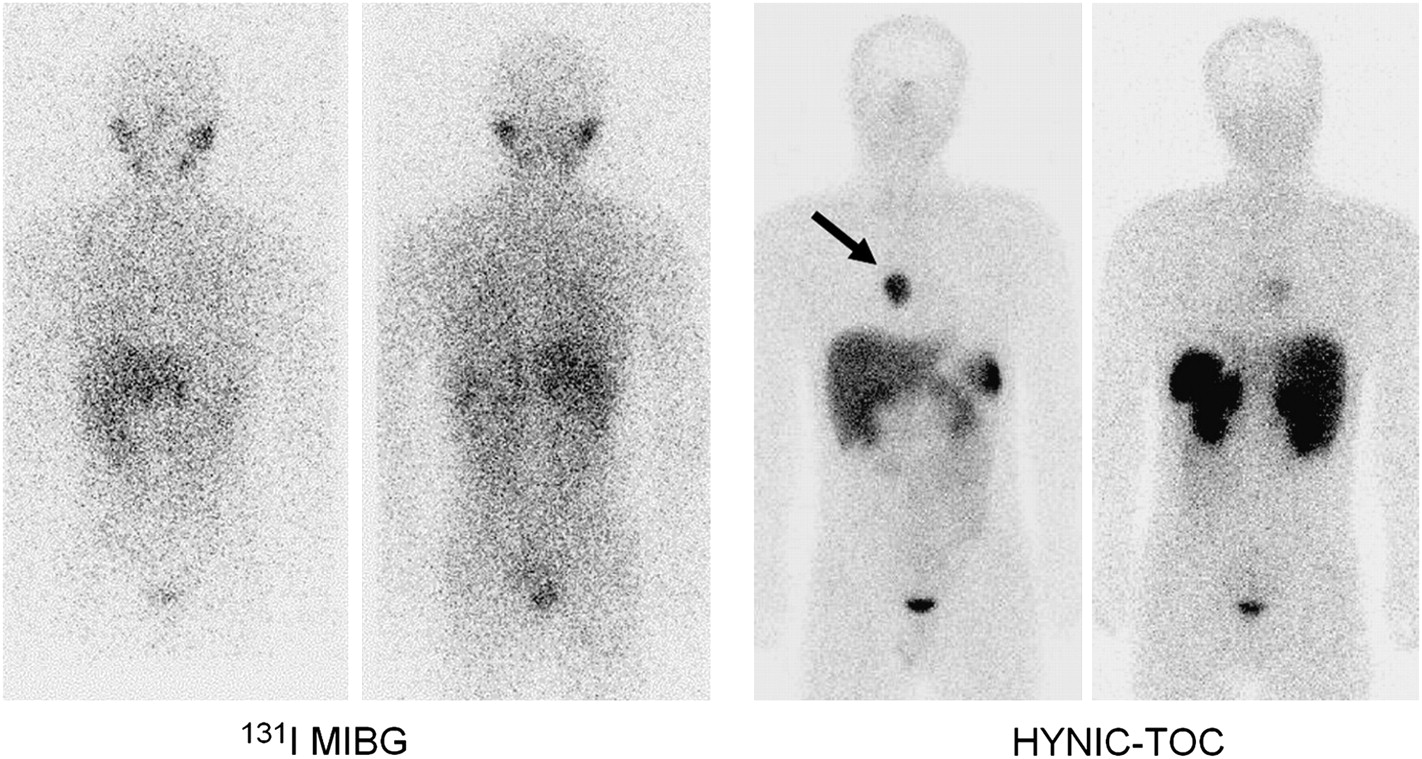
Twenty-five patients had extraadrenal pheochromocytomas. Of these 25, 14 had benign extraadrenal pheochromocytomas (all in either the mediastinal or abdominal paraspinal region). Ten of 14 benign extraadrenal lesions were successfully detected by both 131I-MIBG imaging and 99mTc-HYNIC-TOC scintigraphy. However, 3 patients with benign extraadrenal pheochromocytomas had negative 131I-MIBG findings but their lesions were successfully detected by 99mTc-HYNIC-TOC scintigraphy (Fig. 1). Both 131I-MIBG imaging and 99mTc-HYNIC-TOC scintigraphy failed to detect 1 lesion in 1 patient. Therefore, 99mTc-HYNIC-TOC scintigraphy offered a sensitivity of 92.9% (13/14) in this clinical setting. In comparison, the sensitivity of 131I-MIBG imaging in the detection of benign extraadrenal pheochromocytoma is lower, at 71.4% (10/14).

A woman presented with dizziness, palpitation, and perspiration. Pheochromocytoma was suspected, and her urine catecholamine level was elevated. However, abdominal CT from an outside institution had no abnormal findings. 131I-MIBG imaging was unrevealing. In contrast, 99mTc-HYNIC-TOC scintigraphy identified abnormal activity in mediastinum (arrow), which was surgically removed and histopathologically proven to be pheochromocytoma.
Eleven patients had malignant extraadrenal pheochromocytomas. Of these 11, 8 had positive findings on both 131I-MIBG imaging and 99mTc-HYNIC-TOC scintigraphy. However, the abnormalities in 3 patients were detected by 99mTc-HYNIC-TOC scintigraphy but not 131I-MIBG imaging (Fig. 2). Therefore, for malignant extraadrenal pheochromocytoma, 99mTc-HYNIC-TOC scintigraphy had a sensitivity of 100% (11/11) whereas the sensitivity of 131I-MIBG imaging again was lower, at 72.7% (8/11).
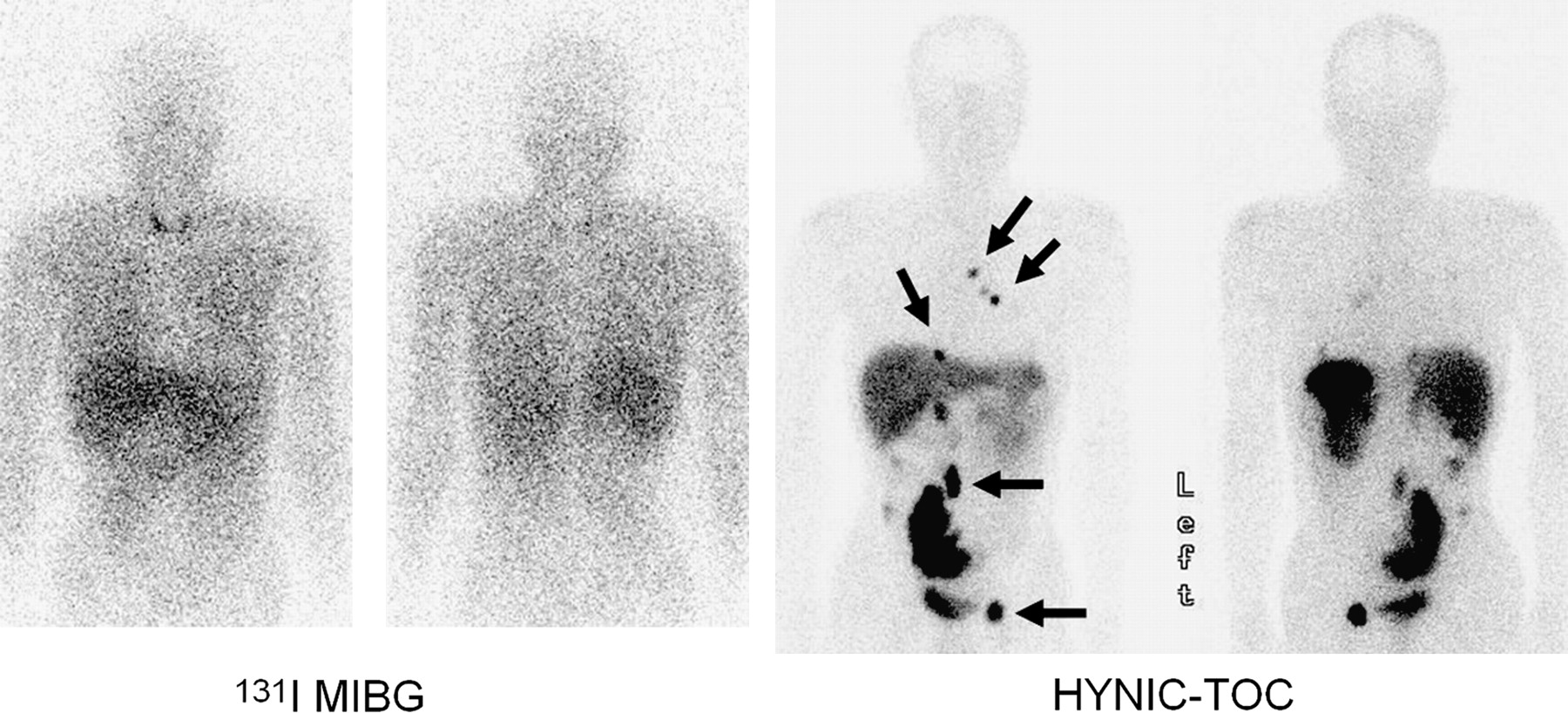
A 58-y-old man had pheochromocytoma 10 y ago, and the primary tumor had been successfully removed surgically. One year before patient underwent 131I-MIBG imaging and 99mTc-HYNIC-TOC scintigraphy, groin pain had developed. 131I-MIBG imaging did not reveal any abnormalities except for mildly increased activity in thyroid bed, which was attributed to unlabeled free 131I. However, subsequent 99mTc-HYNIC-TOC scintigraphy demonstrated many foci of intense activity (arrows), indicating metastatic malignant pheochromocytomas, as confirmed by biopsy.
For the evaluation of extraadrenal pheochromocytoma, the overall sensitivity of 99mTc-HYNIC-TOC scintigraphy is, therefore, 96.0%, (24/25), whereas the sensitivity of 131I-MIBG imaging is 72.0% (18/25).
DISCUSSION
Although our results showed that 99mTc-HYNIC-TOC scintigraphy is excellent in the detection of extraadrenal lesions, it cannot replace 131I-MIBG imaging in the evaluation of patients with suspected pheochromocytoma. The overwhelming majority of pheochromocytomas are intraadrenal, and 99mTc-HYNIC-TOC is less accurate than 131I-MIBG imaging in evaluating intraadrenal lesions. Therefore, most patients should still undergo 131I-MIBG imaging first in the work-up of pheochromocytoma, and the role of 99mTc-HYNIC-TOC scintigraphy lies mainly in those patients who have negative or ambiguous results on 131I-MIBG imaging and when an extraadrenal pheochromocytoma is suspected.
It is unclear why 99mTc-HYNIC-TOC is superior to 131I-MIBG in the detection of extraadrenal pheochromocytoma. These 2 tracers are very different in their mechanism of uptake by cells. 99mTc-HYNIC-TOC is a somatostatin analog binding to receptors, whereas 131I-MIBG is a guanethidine analog that is sequestered mainly in the storage granules of chromaffin cells. Cellular 131I-MIBG uptake is driven both by saturable active type I uptake and by passive diffusion (14). A subsequent active uptake mechanism, different from the transmembrane uptake mechanism, is responsible for the translocation of intracellular 131I-MIBG into the storage granules (15). It is well known that 131I-MIBG uptake by the tumor can significantly be affected by large ranges of medications (16). Therefore, for those individuals who cannot follow prescan instructions to stop related medicines, the sensitivity of 131I-MIBG imaging may be decreased. Extraadrenal pheochromocytoma may be malignant in up to 40% of cases (2,17). Malignant pheochromocytoma may undergo tumor dedifferentiation, with loss of specific neurotransmitter transporters (18). The result is an inability to accumulate these isotopes and a consequent lack of localization, that is, decreased sensitivity in 131I-MIBG imaging (5). Physiologic cardiac uptake of 131I-MIBG (19) can be significant, making it difficult to use 131I-MIBG to evaluate superimposed malignancy in the mediastinum. In contrast, because of the absence of any physiologic cardiac uptake of 99mTc-HYNIC-TOC, pheochromocytoma in the mediastinal or pericardial regions can be more easily recognized by 99mTc-HYNIC-TOC scintigraphy than by 131I-MIBG imaging (20).
There are many advantages to a technetium-based tracer in nuclear medicine. These include a frequently lower radiation dose to the patient; an optimal 140-keV energy peak, which results in better images; and a shorter procedure (a few hours for 99mTc-HYNIC-TOC scintigraphy, as opposed to more than 1 d for MIBG imaging). In addition, the quality of SPECT images is excellent when technetium is used but is often less than optimal when other tracers are used. Furthermore, 99mTc is easily available, and 99mTc-HYNIC-TOC can be prepared in any nuclear medicine service equipped with trained personnel—factors that are potentially cost-saving.
One drawback of our investigation was its retrospective nature. Unintended bias in patient selection is difficult to avoid in a retrospective study. Most pheochromocytomas are in the adrenal glands. However, in our study, only a small portion of the patients had adrenal lesions, because in many patients with adrenal pheochromocytoma, the disease can be detected by CT. However, when pheochromocytoma is suspected at our institution, only those patients without a definite adrenal abnormality or with ambiguous results on CT are further imaged by both 131I-MIBG imaging and 99mTc-HYNIC-TOC scintigraphy, significantly reducing the number of the patients with adrenal pheochromocytoma in our final analysis. It is conceivable that if all patients suspected of having pheochromocytoma had been included in the final analysis without CT preselection, the accuracy of 99mTc-HYNIC-TOC scintigraphy and 131I-MIBG imaging would have been different from what we presented.
99mTc-HYNIC-TOC can show increased accumulation in other types of tumors, as was also seen in our study. The positive findings on two 99mTc-HYNIC-TOC scans were later proven to be due to adrenal carcinomas. Therefore, in our final analysis, the findings in these 2 cases were treated as false-positive. However, from a patient-care point of view, the results of these two 99mTc-HYNIC-TOC scans should be regarded as true-positive because the findings were crucial to subsequent patient management.
CONCLUSION
Our preliminary results indicate that 131I-MIBG imaging remains the method of choice in the evaluation of adrenal pheochromocytoma. However, 99mTc-HYNIC-TOC scintigraphy is superior to 131I-MIBG imaging in the evaluation of extraadrenal pheochromocytomas. Larger prospective studies are necessary for validation of our findings.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication September 30, 2008.
- Accepted for publication December 5, 2008.





{kind=link}
{kind=link}