


Abstract
Radiolabeled peptides have been an important class of compounds in radiopharmaceutical sciences and nuclear medicine for more than 20 years. Despite strong research efforts, only somatostatin-based radiopeptides have a real impact on patient care, diagnostically and therapeutically. [111In-diethylenetriaminepentaacetic acid0]octreotide is commercially available for imaging. Imaging was highly improved by the introduction of PET radionuclides such as 68Ga, 64Cu, and 18F. Two peptides are successfully used in targeted radionuclide therapy when bound to DOTA and labeled with 90Y and 177Lu.
Neuroendocrine tumors are regarded as rare, but their incidence and prevalence have increased substantially over the last 30 years (1). This has to do in part with improved modern diagnostic work-up, such as through somatostatin receptor imaging with SPECT and PET, methods based on somatostatin receptor expression in these tumors. To date, 5 human somatostatin receptor subtypes (sst1–sst5) have been characterized (2). These subtypes belong to the superfamily of G protein–coupled receptors and represent the molecular basis for their detection by imaging probes, for targeted radionuclide therapy, and for the use of stable analogs such as octreotide and lanreotide for treatment of gastroenteropancreatic neuroendocrine tumors and acromegaly.
TARGETED DIAGNOSIS AND THERAPY OF SOMATOSTATIN RECEPTOR–POSITIVE TUMORS
Imaging and targeted radionuclide therapy require a probe labeled with a diagnostic or therapeutic radionuclide that is injected intravenously into patients. The tracer will extravasate and bind to sites with high somatostatin receptor density. Agonist-based radiopeptides will internalize on binding to the receptor. This will lead to an accumulation of radioactivity in the tumor and is regarded as the decisive mechanism for high accumulation and tumor retention. Clearance via the kidneys is preferable to clearance via the gastrointestinal tract.
DEVELOPMENT OF SOMATOSTATIN RECEPTOR–TARGETING RADIOPEPTIDES
The molecular basis for the development and clinical application of somatostatin-based radiopeptide targeting is the high expression of somatostatin receptors on the plasma membrane of tumor cells. In vitro receptor evaluation using receptor autoradiography or immunohistochemistry is mandatory before radioligands can be developed for in vivo studies. The most reliable method is autoradiography characterizing and quantifying the receptor protein. Receptor density and homogeneity, as well as incidence, are important factors in predicting successful in vivo targeting. Somatostatin receptors have been identified at high density and incidence in most neuroendocrine tumors, including gastroenteropancreatic tumors, pheochromocytomas, pituitary adenomas, and paragangliomas but also in tumors of the nervous system such as neuroblastomas, medulloblastomas, and meningiomas. At lower incidence and density, somatostatin receptors are present in insulinomas, lymphomas, breast carcinomas, renal cell carcinomas, hepatocellular carcinomas, medullary thyroid carcinomas, and small cell lung carcinomas. A high variability has been observed: although most neuroendocrine tumors have a homogeneous distribution, others such as breast cancers express somatostatin receptors quite heterogeneously. Among the 5 somatostatin receptor subtypes, sst2 was found to be predominantly expressed (2).
Equally important is the receptor expression in normal tissue. Physiologic expression of somatostatin receptors is found in the brain, pituitary, thyroid, pancreas, adrenals, kidneys, gastrointestinal tract, and immune system. Low physiologic expression is important in regard to good image contrast but is a more critical safety issue in targeted radiotherapy.
IMAGING AND THERAPY PROBES
Several critical parameters determine the suitability of somatostatin-based radiopeptides for clinical applications. First, receptor-binding affinity should be in the low nanomolar range. Small peptides often lose their affinity on radiolabeling. They have molecular weights of around 1,000 Da; a chelator such as DOTA (1,4,7,10-tetraaza-cyclododecane-1,4,7,10-tetraacetic acid) adds about 500 Da, illustrating that chelators and prosthetic groups for radiohalogenation may strongly influence receptor affinity and biologic potency in general.
Second, the internalization rate appears to be important if agonistic peptides are selected, as it correlates well with tumor uptake (3). The pharmacokinetics are of higher importance than the above parameters. The first and second radiopeptides studied in patients, [123I-Tyr3]octreotide and [111In-DTPA0]octreotide (DTPA = diethylenetriaminepentaacetic acid), respectively, are good examples. Whereas the former shows high sst2 affinity and a high rate of internalization, the latter is a poor radioligand with a low internalization rate (3,4). The poor pharmacokinetics showing mainly hepatobiliary excretion (5), along with a tedious labeling procedure, led to the abandonment of the former and registration of the latter.
Third, peptides are metabolically unstable because of in vivo proteolysis. Radiolabeled endogenous peptide ligands are therefore not suitable because of insufficient in vivo stability and bioavailability. Somatostatin-14 has a short plasma half-life of 2–3 min, whereas octreotide shows a highly improved plasma half-life of more than 1 h.
A fourth critical parameter is label stability. Radioligands used in somatostatin receptor targeting are labeled mostly with radiometals. These often are bone seekers or strongly bind to plasma proteins; therefore, encapsulation of the radiometals is important to avoid premature release. Cage-type macrocyclic molecules such as DOTA confer extreme stability to its radiometal complexes, allowing safe clinical use. A recent review by Waddas et al. discussed the role of coordination chemistry of important radiometals (6).
PEPTIDE-BASED PROBES FOR SOMATOSTATIN RECEPTOR–POSITIVE TUMORS
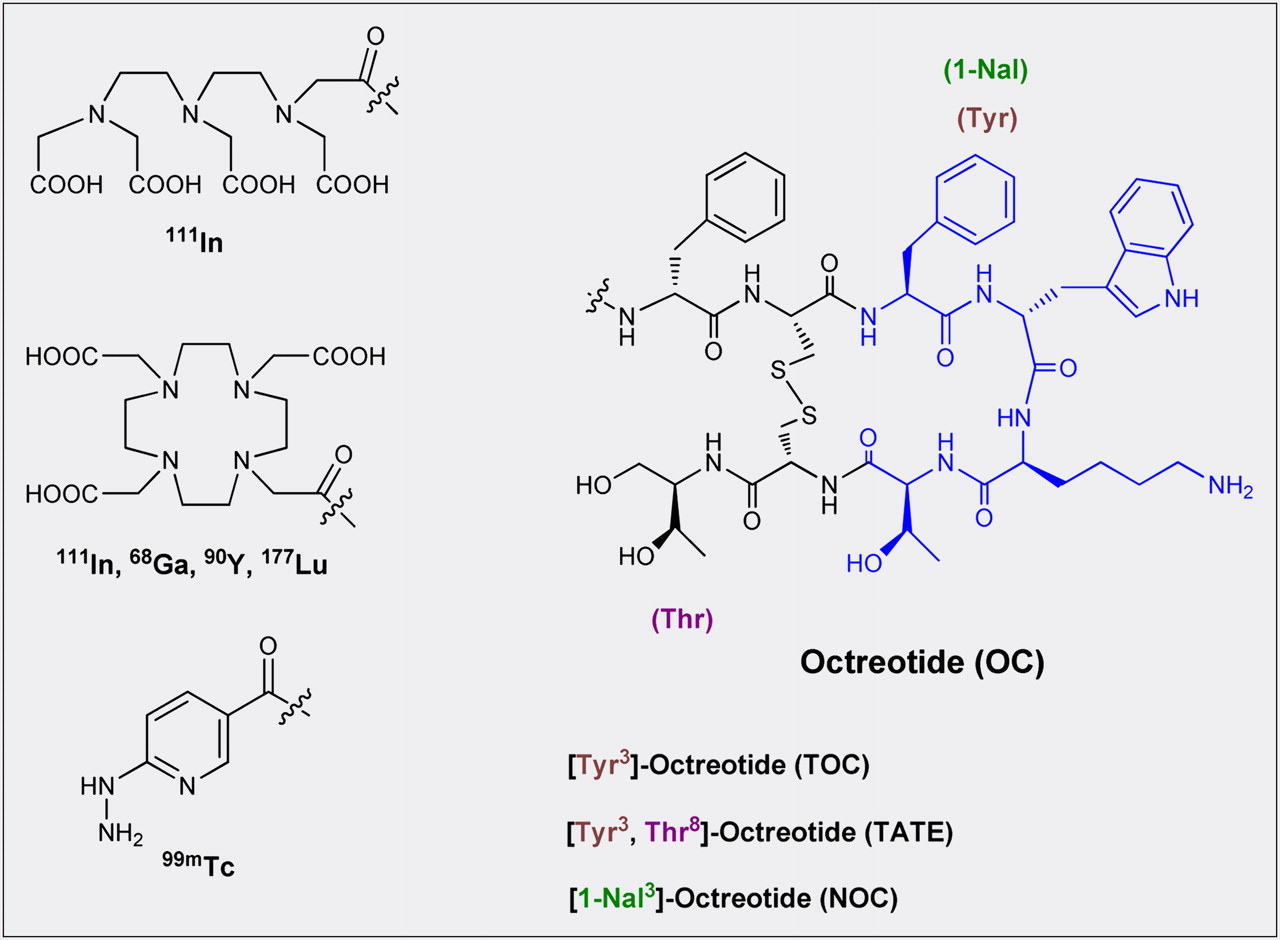
The early proof of principle using [123I-Tyr3]octreotide and the registration of [111In-DTPA0]octreotide were a strong motivator for developing new somatostatin receptor–targeting agents. The incentive came from the known shortcomings of the 2 radiotracers. Research programs to develop more suitable radiopeptides were initiated. The most important ones are summarized in Figure 1. They are based on the γ-emitters 99mTc and 111In; the β+-emitters 68Ga, 64Cu, 86Y, and 18F; and the particle emitters 90Y (high-energy β−) and 177Lu (low-energy β−). A review by Schottelius and Wester provides more information (7).
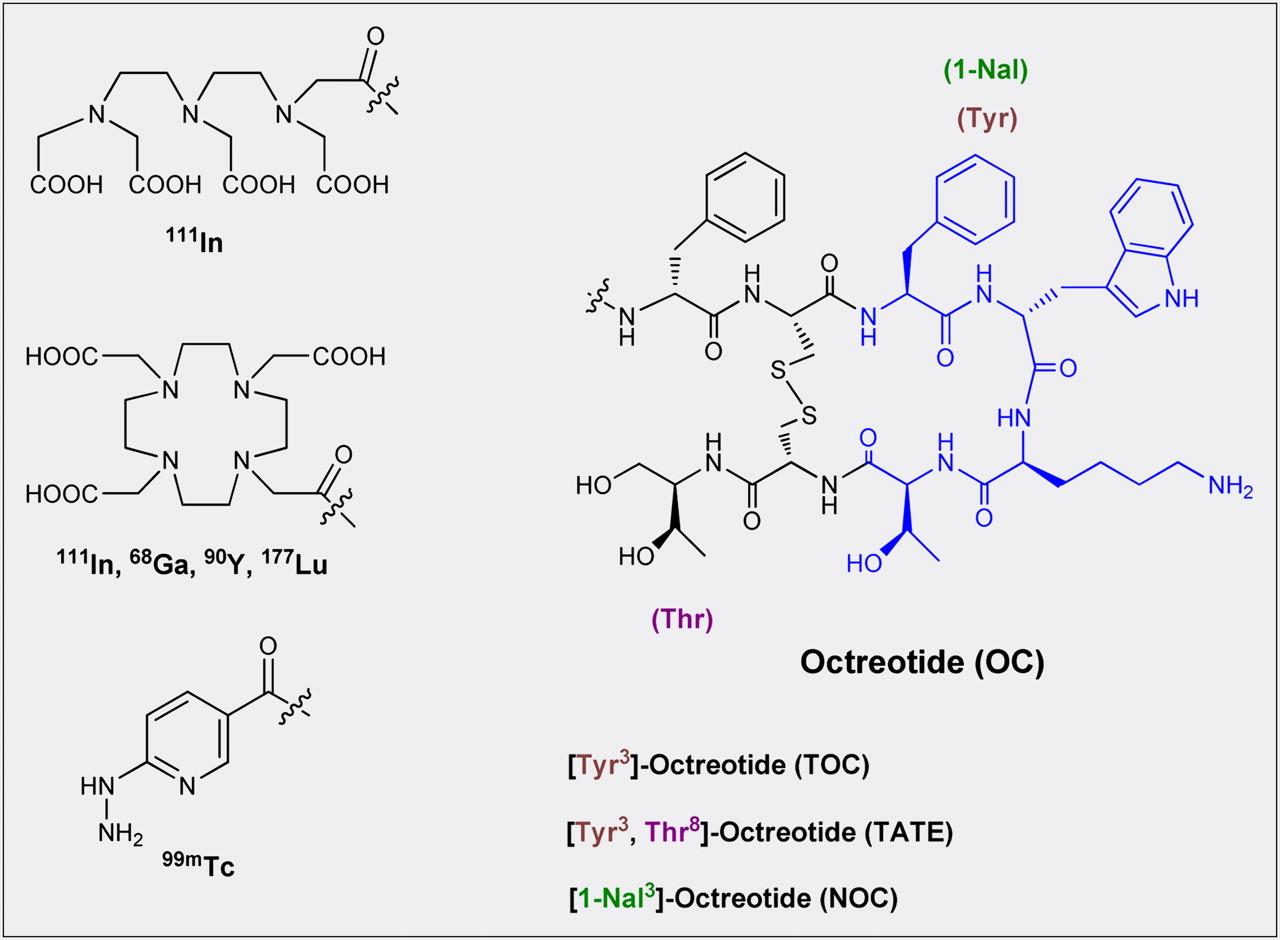
Structures, chelators, and radiometals for imaging and targeted therapy; they represent the radioligands most frequently used in the clinic.
Figure 1 depicts the conjugates most commonly used in clinical practice, and the respective radiometals. They are based on octapeptides such as octreotide (OC), [Tyr3]octreotide (TOC), [1-Nal3]octreotide (NOC), and [Tyr3,Thr8]octreotide (TATE). As indicated, [111In-DTPA0]octreotide was the first commercially available imaging agent. [99mTc-hydrazinonicotinamide (HYNIC)/ethylenediamine-N,N′-diacetic acid (EDDA),Tyr3]octreotide (99mTc-HYNIC-TOC) is commercially available in some European countries.
For stable labeling with radiolanthanides and 90Y, DTPA was replaced by DOTA, which is a better choice as it forms thermodynamically and kinetically stable complexes with 3+ charged radiometals.
The replacement of Phe3 in octreotide by Tyr3 leads to an improved sst2 affinity, but the sst3 and sst5 affinity is reduced; the C-terminal introduction of Thr for Thr(ol) results in a sst2-selective ligand with a 7-fold improvement of sst2 affinity (4). The NOC derivative (1-Nal in position 3) leads to a radiopeptide with affinity to sst2,3,5. Interestingly, a change of radiometal may profoundly influence receptor affinity. Labeling of the above DOTA conjugates with 68Ga improves sst2 affinities by up to 8-fold (8).
Besides these clinically most frequently used radiopeptides, many others have been studied preclinically and preliminarily in patients. Among them are 18F- and 11C-labeled glycated octreotate derivatives and 64Cu-labeled peptides (9). Excellent preclinical and clinical data have also been obtained with a tetramine-based TATE conjugate labeled with 99mTc (7).
THERANOSTIC PAIRS
Personalized medicine is used along with targeted therapy in general. The targeting of somatostatin receptor–positive tumors is an ideal example of this approach. It combines powerful new diagnostics and radiotargeted therapeutics. A diagnostic scan with a γ- or β+-emitting nuclear probe is used to identify tumors and metastases that overexpress somatostatin receptors and is therefore predictive of the potential for targeted radionuclide therapy in patients. It also allows the study of dosimetry, thereby estimating doses to tumors and normal organs. If the therapeutic window appears wide enough, the same probe can be applied, labeled with a particle emitter. The final goal is a therapy probe with pharmacokinetics the same as or similar to the diagnostic probe. Ideally, this is possible with so-called matched pairs; that is, diagnostic radionuclides sharing the chemistry of the therapeutic congener. Examples are 99mTc/186,188Re, 86Y/90Y, and 64Cu/67Cu. Because of the similar coordination chemistry, 111In is often used as a surrogate of 90Y but also of β−-emitting radiolanthanides.
CLINICAL STUDIES (DIAGNOSIS)
[111In-DTPA0]octreotide has been used for more than 15 y in the diagnosis and staging of sst-positive tumors. In recent years, its performance has been compared with new SPECT and PET tracers based on 99mTc and 68Ga. Hubalewska-Dydejczyk et al. demonstrated the superiority of the SPECT tracer [99mTc-HYNIC/EDDA]octreotate over [111In-DTPA0]octreotide in 75 patients (10). The superiority was confirmed by other groups.
68Ga-based PET tracers are widely used in Europe, in particular 68Ga-DOTATOC, 68Ga-DOTATATE, and 68Ga-DOTANOC; the last of these has affinity for sst2, sst3, and sst5, resulting in a somewhat higher diagnostic sensitivity than 68Ga-DOTATATE, which has the highest sst2 affinity of all these tracers (11,12).
Several studies comparing the 68Ga-based peptides with [111In-DTPA0]octreotide were performed and showed the distinctly higher sensitivity of the PET tracers (13). A typical example of images in the same patient is shown in Figure 2. In addition to the better imaging performance, the radiation dose to the patient is lower and the final result of the study is available within a few hours after injection. For an even broader application, a registered 68Ge/68Ga generator is urgently needed along with a kit formulation of one of the peptides. Bushnell and Baum recently provided an overview of imaging techniques (14).

Patient with metastasized neuroendocrine tumor. Planar (left) and PET (right) images were obtained 3 wk apart. p.i. = after injection. (Courtesy of Damian Wild, University Hospital Freiburg.)
CLINICAL STUDIES (THERAPY)
Numerous centers across Europe routinely provide targeted radionuclide therapy using radiolabeled somatostatin analogs to patients with metastasized or unresectable neuroendocrine tumors. The most frequently used radiopeptides are 90Y-DOTATOC and 177Lu-DOTATATE, and different combinations thereof have also been applied. Several phase I and II clinical studies on targeted radionuclide therapy have been published (15,16). The variability in the therapeutic schemes applied in these studies (injected dose and number of treatment cycles), as well as in the recruited population (inclusion criteria and selection of the patients), makes the comparison of these data nearly impossible. Therefore, the answer to the question of which radiopeptide is preferable and which therapeutic scheme should be followed is still debatable.
Despite their complexity and diversity, the published clinical studies on patients treated with targeted radionuclide therapy have reported an objective response rate (defined as complete remission and partial remission) ranging from 9% to 33%. A median time to progression of 29–40 mo and a median overall survival of 37–46 mo have been reported for patients with gastroenteropancreatic-neuroendocrine tumor. An impressive example of a partial remission after a single therapy cycle is shown in Figure 3.

Transaxial (A and B) and coronal (C and D) SPECT/CT images obtained after first (A and C) and second (B and D) therapy cycles with 90Y/111In-DOTATOC (111In is added for imaging). Impressive partial remission is seen after first therapy cycle. (Courtesy of Flavio Forrer and Guillaume Nicolas, University Hospital Basel, Switzerland.)
Targeted radionuclide therapy can be regarded as relatively safe. Severe toxicity rarely may occur as a result of the radiation-absorbed dose in healthy organs. Kidneys and bone marrow are the dose-limiting organs in this treatment.
FUTURE DEVELOPMENTS
New Strategies
The general strategy used to develop peptide radioligands has been to identify a high-affinity peptide analog to which a chelator or a prosthetic group can be coupled. Crucial requirements are a high binding affinity and a high internalization rate, a general characteristic of agonistic peptides. This strategy has led to the development of a large number of excellent somatostatin agonist radioligands. Recently, however, several observations have challenged this strategy.
First, it has been shown that potent somatostatin receptor antagonists, known to poorly internalize into tumor cells, can visualize tumors in vivo as well as or even better than agonists (17). This unexpected phenomenon was found for sst2- and sst3-selective somatostatin analogs and may be due to the binding of the antagonist to a larger number of sites and to its lower dissociation rate. A pilot clinical trial with an 111In-DOTA-sst2 antagonist recently confirmed the animal data (18). More potent sst2 antagonists for the same purpose are in development (19). To achieve this goal, several functional tests able to distinguish an agonist from an antagonist had to be developed (19,20).
Second, it was observed that some established somatostatin agonists, in particular those belonging to the pan-somatostatin family, were biased agonists. For instance, the 2 pansomatostatins, SOM230 and KE108, which had been established as full and potent sst2 agonists on growth hormone release or in the adenylate cyclase assay, were found to be sst2 antagonists in calcium assays and extracellular signal-regulated kinase phosphorylation assays (20). These compounds were also found to poorly trigger the sst2 internalization (21) and therefore to be poorly internalized themselves (22). Third, it was observed that the simple addition of a DOTA chelator to a potent sst3 antagonist switches its functional behavior toward an agonist (23).
This new information indicates the complexity of developing peptide radioligands and shows that it is mandatory to evaluate in vitro the peptide ligands of interest at each step of development.
Another strategy to find new compounds is to modify the physicochemical properties of the peptides. A recent example is the development of bicyclic somatostatin-based radiopeptides, a neglected family of radiopeptides, developed by Fani et al. (24). These molecules have fast background clearance and therefore high tumor–to–normal organ ratios. This new structural motif represents a promising basis for new radiopeptides with improved properties.
Multireceptor Targeting
In vitro autoradiography studies have shown that multiple receptors may be coexpressed on the same tumor, allowing the use of a cocktail of radiopeptides to increase the probability of targeting a particular tumor type. Gastrinomas coexpress sst2 and sst5 receptors, glucagonlike peptide receptor 1, and gastrin-releasing peptide receptor. Insulinomas coexpress glucagonlike peptide 1, gastrin, and sst1 and sst2 receptors. Ileal carcinoids often concomitantly express sst1, sst2, and sst5 receptors; neuromedin B receptor; and gastrin receptors (2).
CONCLUSION
Diagnostic and radiotherapeutic targeting of neuroendocrine tumors with peptide-based nuclear probes has been proven useful. To fully exploit its potential, the development of new radiopeptides with improved pharmacokinetics is warranted.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication March 18, 2011.
- Accepted for publication April 11, 2011.





{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- TARGETED DIAGNOSIS AND THERAPY OF SOMATOSTATIN RECEPTOR–POSITIVE TUMORS
- DEVELOPMENT OF SOMATOSTATIN RECEPTOR–TARGETING RADIOPEPTIDES
- IMAGING AND THERAPY PROBES
- PEPTIDE-BASED PROBES FOR SOMATOSTATIN RECEPTOR–POSITIVE TUMORS
- THERANOSTIC PAIRS
- CLINICAL STUDIES (DIAGNOSIS)
- CLINICAL STUDIES (THERAPY)
- FUTURE DEVELOPMENTS
- CONCLUSION
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Biodistribution and Radiation Dosimetry for the Chemokine Receptor CXCR4-Targeting Probe 68Ga-Pentixafor
- Impact of 68Ga-DOTATATE PET/CT on the Management of Neuroendocrine Tumors: The Referring Physician's Perspective
- The Glucose-Dependent Insulinotropic Polypeptide Receptor: A Novel Target for Neuroendocrine Tumor Imaging--First Preclinical Studies
- Receptor Affinity and Preclinical Biodistribution of Radiolabeled Somatostatin Analogs
- Evaluation of 177Lu-DOTA-sst2 Antagonist Versus 177Lu-DOTA-sst2 Agonist Binding in Human Cancers In Vitro