


Abstract
An 18F-labeled PET amyloid-β (Aβ) imaging agent could facilitate the clinical evaluation of late-life cognitive impairment by providing an objective measure for Alzheimer disease (AD) pathology. Here we present the results of a clinical trial with (E)-4-(2-(6-(2-(2-(2-18F-fluoroethoxy)ethoxy)ethoxy)pyridin-3-yl)vinyl)-N-methyl benzenamine (18F-AV-45 or flobetapir F 18). Methods: An open-label, multicenter brain imaging, metabolism, and safety study of 18F-AV-45 was performed on 16 patients with AD (Mini-Mental State Examination score, 19.3 ± 3.1; mean age ± SD, 75.8 ± 9.2 y) and 16 cognitively healthy controls (HCs) (Mini-Mental State Examination score, 29.8 ± 0.45; mean age ± SD, 72.5 ± 11.6 y). Dynamic PET was performed over a period of approximately 90 min after injection of the tracer (370 MBq [10 mCi]). Standardized uptake values and cortical-to-cerebellum standardized uptake value ratios (SUVRs) were calculated. A simplified reference tissue method was used to generate distribution volume ratio (DVR) parametric maps for a subset of subjects. Results: Valid PET data were available for 11 AD patients and 15 HCs. 18F-AV-45 accumulated in cortical regions expected to be high in Aβ deposition (e.g., precuneus and frontal and temporal cortices) in AD patients; minimal accumulation of the tracer was seen in cortical regions of HCs. The cortical-to-cerebellar SUVRs in AD patients showed continual substantial increases through 30 min after administration, reaching a plateau within 50 min. The 10-min period from 50 to 60 min after administration was taken as a representative sample for further analysis. The cortical average SUVR for this period was 1.67 ± 0.175 for patients with AD versus 1.25 ± 0.177 for HCs. Spatially normalized DVRs generated from PET dynamic scans were highly correlated with SUVR (r = 0.58–0.88, P < 0.005) and were significantly greater for AD patients than for HCs in cortical regions but not in subcortical white matter or cerebellar regions. No clinically significant changes in vital signs, electrocardiogram, or laboratory values were observed. Conclusion: 18F-AV-45 was well tolerated, and PET showed significant discrimination between AD patients and HCs, using either a parametric reference region method (DVR) or a simplified SUVR calculated from 10 min of scanning 50–60 min after 18F-AV-45 administration.
Although the etiology of Alzheimer disease (AD) has not been established, converging evidence suggests that the amyloid-β (Aβ) peptide plays an important role in AD pathogenesis (1). Plaques containing Aβ fibrils are found in the AD brain and are a key component of the neuropathologic criteria for autopsy-based confirmation of diagnosis (2,3). Immunologic therapies that decrease Aβ deposition have been shown to stabilize or reverse cognitive deficits in transgenic mouse models of AD (4). Additionally, Aβ deposition is thought to precede cognitive symptoms in AD and is a potential preclinical marker of disease (5). Thus, Aβ deposition is a major target for novel AD treatments currently in human trials.
However, these efforts have been hampered by the absence of reliable, noninvasive markers for brain Aβ load. A reliable biomarker could aid diagnosis by documenting the presence of disease-specific pathology and could be useful for the prediction of postdisease progression, evaluation of effects of therapy on disease progression, and presymptomatic identification of subjects at risk for developing AD. Although cerebrospinal fluid Aβ levels are reliably decreased in AD (6), cerebrospinal fluid studies are inevitably indirect markers. Imaging techniques using radiolabeled PET tracers that bind to the aggregated Aβ peptides in Aβ plaques have the potential to directly assess relative brain Aβ plaque pathology. To date, the most widely researched imaging approach has used the 11C-labeled PET tracer [N-methyl-]2-(4′-methylaminophenyl)-6-hydroxybenzothiazole (6-OH-BTA), also known as Pittsburgh compound B or PIB (7). Despite these encouraging results, the short half-life (20 min) of the 11C isotope may limit the utility of 11C-PIB as a tool for aiding in community-based diagnosis and therapeutic evaluation.
Because 18F has a radioactive half-life of 110 min, regional preparation and shipping of doses is possible, thereby reducing the cost and greatly increasing the number of potential imaging center users. Several 18F-labeled Aβ tracers have been successfully tested in clinical trials (Supplemental Fig. 1; supplemental materials are available online only at http://jnm.snmjournals.org) (8–10). However, a ligand with faster kinetics was desired to enable shorter imaging procedures of AD patients. (E)-4-(2-(6-(2-(2-(2-18F-fluoroethoxy)ethoxy)ethoxy)pyridin-3-yl)vinyl)-N-methyl benzenamine (18F-AV-45 or flobetapir F 18) was selected from a series of agents as the tracer with the optimum kinetics and selectivity for Aβ plaques (11). The present study was designed as a preliminary exploration of the brain-imaging properties, pharmacokinetics, and tolerability of 18F-AV-45 (flobetapir F 18) in elderly cognitively healthy controls (HCs) and in patients with AD.
MATERIALS AND METHODS
18F-AV-45 (flobetapir F 18) was studied at 3 sites—Johns Hopkins Hospital/Johns Hopkins University (JHU), Memory Enhancement Center of America, Long Branch, NJ, and Community Health Research, North East, MD—in elderly subjects who were cognitively healthy and patients with AD.
Eligibility and Overall Study Design
18F-AV-45 was studied in a total of 16 HC volunteers and 16 AD patients. Patients with AD had to be older than 50 y and have a probable diagnosis of AD according to the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association, with a Mini-Mental State Examination (MMSE) score of between 10 and 24, inclusively (12,13). HCs had to be older than 50 y, with no evidence of cognitive impairment by history and psychometric testing, and had to have an MMSE score of at least 29. Subjects who showed evidence of any other significant neurodegenerative or psychiatric disease on clinical examination or MRI or clinically significant medical comorbidities that might pose a safety risk to the subject or interfere with interpretation of the scan were excluded from the study. Patients with AD could be on a stable dose (by investigator judgment: not in titration period, no change in medication being considered) of an acetylcholinesterase inhibitor, memantine, or vitamin E. Patients who had participated in an experimental study with a treatment that targeted Aβ (e.g., immunotherapy, secretase inhibitor, selective Aβ-lowering agents) were excluded. All procedures were approved by the appropriate Institutional Review Board, and all participants or an appropriate representative signed informed consent forms, consistent with established criteria (12).
Similar acquisition protocols were used at the 3 centers. All subjects received a single intravenous bolus of approximately 370 MBq (10 mCi) of 18F-AV-45, and PET began. Dynamic brain PET images were collected for approximately 90 min. The PET scanners used were the Advance (GE Healthcare) (PET only, at JHU), Discovery LS (GE Healthcare) (PET/CT, at Community Health Center and The Memory Enhancement Center), and Discovery ST (GE Healthcare) (PET/CT, at The Memory Enhancement Center). In addition, plasma metabolites were analyzed using the method of Hilton et al. (14). The supplemental information provides detailed PET, metabolite analysis, and image-acquisition procedures.
Radiosynthesis of 18F-AV-45
The doses of 18F-AV-45 were prepared individually on the day of administration at either the JHU cyclotron or radiochemistry laboratory or at the Avid Radiopharmaceuticals radiochemistry laboratory in accordance with the Avid Radiopharmaceuticals Investigational New Drug master batch record and quality control release criteria. Mean specific activity at the time of injection was 74,777 ± 72,409 GBq/mmol (2,021 ± 1,957 Ci/mmol).
Image Analysis
Computation of Standardized Uptake Values (SUVs) and SUV Ratios (SUVRs)—All Subjects
PET images for each subject were resliced (realigned) to create a mean image across all frames (individual acquisition time blocks). This image was normalized to Talairach space by SPM (version 2; Wellcome Trust Centre for Neuroimaging). Each individual frame was then fitted to this normalized mean image. No partial-volume correction was performed. To identify volumes of interest (VOIs) for analysis, images of 10 subjects were segmented to identify gray and white matter, cerebrospinal fluid, and skull. Images from the first 10 min after administration in the first 15 subjects were then analyzed, and high-flow areas were determined and compared with the previously segmented gray matter dataset. VOIs were created in the high-flow regions of the frontal, temporal, parietal, occipital, anterior cingulate, posterior cingulate, and precuneus cortical gray matter, and counts were extracted. SUVs were then generated from the VOI for each time frame. SUVRs were calculated using cerebellar gray matter as the primary reference region and centrum semiovale white matter as an alternative reference region.
Mathematic Kinetic Modeling (for Distribution Volume Ratio [DVR] Measures)
In a subset of subjects (9 AD patients and 8 HCs) for whom adequate MRI scans were available, time–activity curves were presented as percentage injected dose and kBq/cm3 for kinetic analyses. A parametric mapping approach with the cerebellum as a reference region (15) was used to calculate DVRs (16).
Whole-Body Imaging and Dosimetry Estimation
Because this was an exploratory, first-in-humans study, brain imaging in 4 healthy subjects was interrupted, and whole-body scans were obtained for preliminary dosimetry estimation from approximately 20 to 45 min after administration of the dose and again from approximately 160 to 185 min after administration of the dose. One subject's data were not available because of technical problems with image retrieval. Data were fit using the SAAM II software (17). Time integrals of activity (18) were entered into the OLINDA/EXM software (19) using the adult male model. Urinary and intestinal tract excretion data were treated with the OLINDA/EXM urinary bladder and International Commission on Radiological Protection gastrointestinal tract model (20).
RESULTS
Subjects
Thirty-two subjects were injected with the imaging agent (16 elderly HCs and 16 AD patients). Baseline characteristics are summarized in Table 1. The first human study worldwide was performed at Johns Hopkins University on June 8, 2007.
Demographics: All Subjects, All 3 Centers
The mean radioactivity injected was 381.1 ± 41.07 MBq (10.3 ± 1.11 mCi) in the AD patients and 358.9 ± 40.7 MBq (9.7 ± 1.1 mCi) in HCs. As would be expected, the baseline average MMSE was lower in the AD patients than in the HCs (19.1 ± 3.1 vs. 29.8 ± 0.45). The AD and HC groups were similar in age, weight, and education. A slightly higher proportion of men composed the HC than in the AD group (10/16 vs. 8/16, respectively). Despite the mass dose range (0.56–9.1 μg), no correlation with SUVR for AD, HC, or the combination of the two was observed.
All elderly HCs and 15 of 16 (94%) AD patients completed the study. One AD patient (6.3%) withdrew consent after 5 min in the scanner. All subjects who received 18F-AV-45 for injection were included in the safety analysis. Efficacy was analyzed for subjects who underwent PET for at least 10 min and had no significant technical failures in the imaging session. Technical failures occurred in 5 subjects. Four of the 5 technical failures occurred in AD patients who exhibited poor placement or excessive movement while in the scanner, which limited proper attenuation correction and quantification of the results. For the fifth subject, operational difficulties with the scanner precluded reconstruction of the data, and no usable images were obtained from the scanner. Thus, valid data for the evaluable population were available for 15 HCs and 11 AD patients.
Imaging Results
Figure 1 shows a typical image from an AD patient and HC subject. These count ratio (SUVR) images were averaged across two 5-min frames, beginning 50 min after the intravenous administration of 18F-AV-45. Each voxel was divided by the average number of counts per voxel in the cerebellar gray matter.
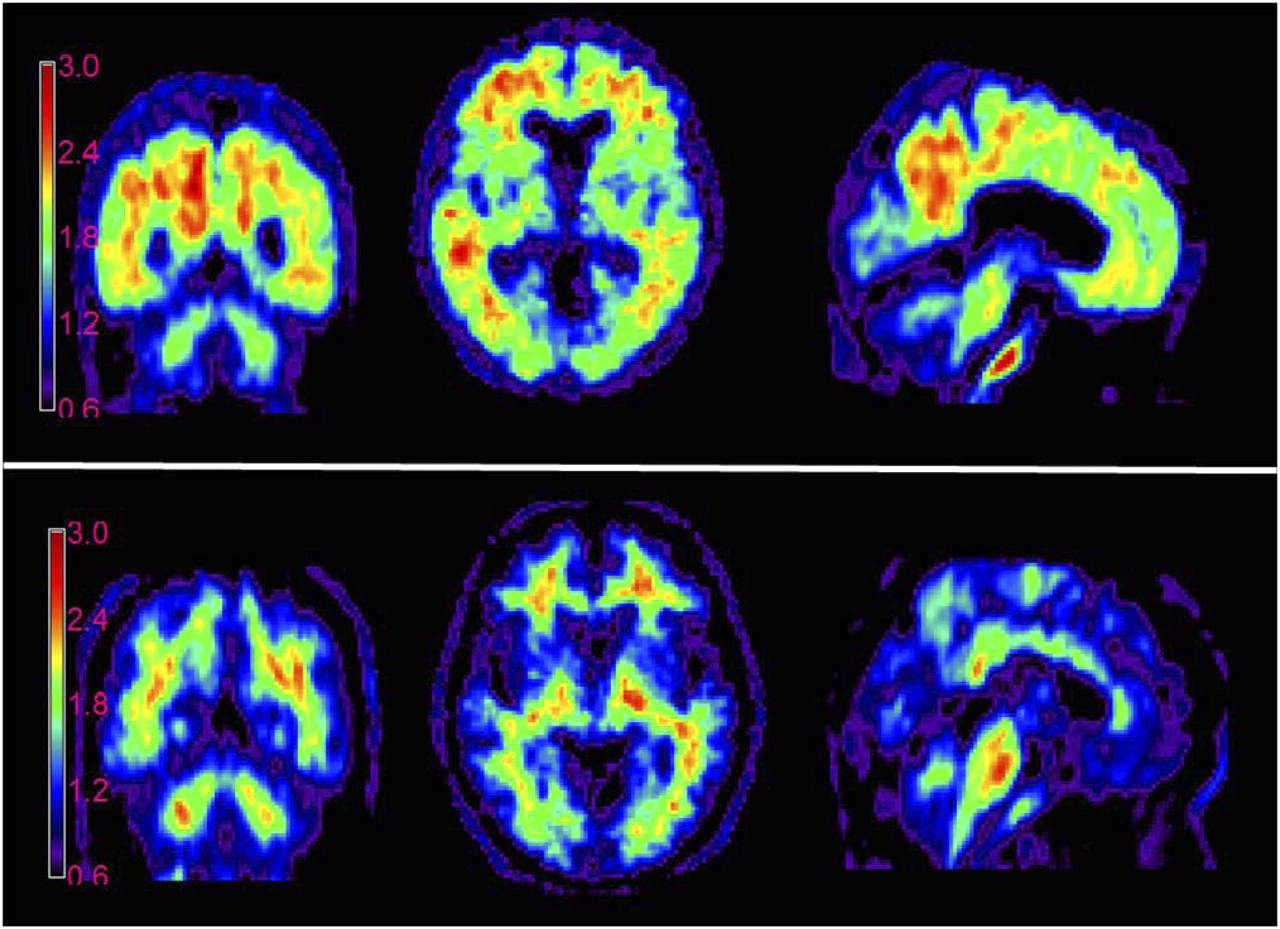
Average of 2 consecutive 5-min 18F-AV-45 PET brain images (obtained 50–60 min after injection of 370 MBq [10 mCi] of 18F-AV-45): 77-y-old woman with mild AD with MMSE of 24 (top) and 82-y-old cognitively healthy man with MMSE of 30 (bottom). Experimental conditions and imaging and computational parameters were identical for the 2 subjects. Counts are shown as ratio to average of gray matter in cerebellum for each subject (SUVR).
In the AD patient, accumulation of tracer can be seen in cortical target areas such as the frontal cortex, temporal cortex, and precuneus—areas expected to be high in Aβ deposition. In contrast, the HC shows tracer accumulation predominantly in white matter areas. Similar results were obtained for most of the other AD patients and HCs.
Figure 2 illustrates the average 18F-AV-45 time–activity relationship (SUV units) from 0 to 90 min after the dose administration for AD patients and HCs. 18F-AV-45 was rapidly distributed to the brain of both AD patients and HCs. The tracer was cleared rapidly from the cerebellum (nontarget or reference) VOI of both AD patients and HCs but was selectively retained in cortical target regions, particularly the precuneus, of the AD patients.
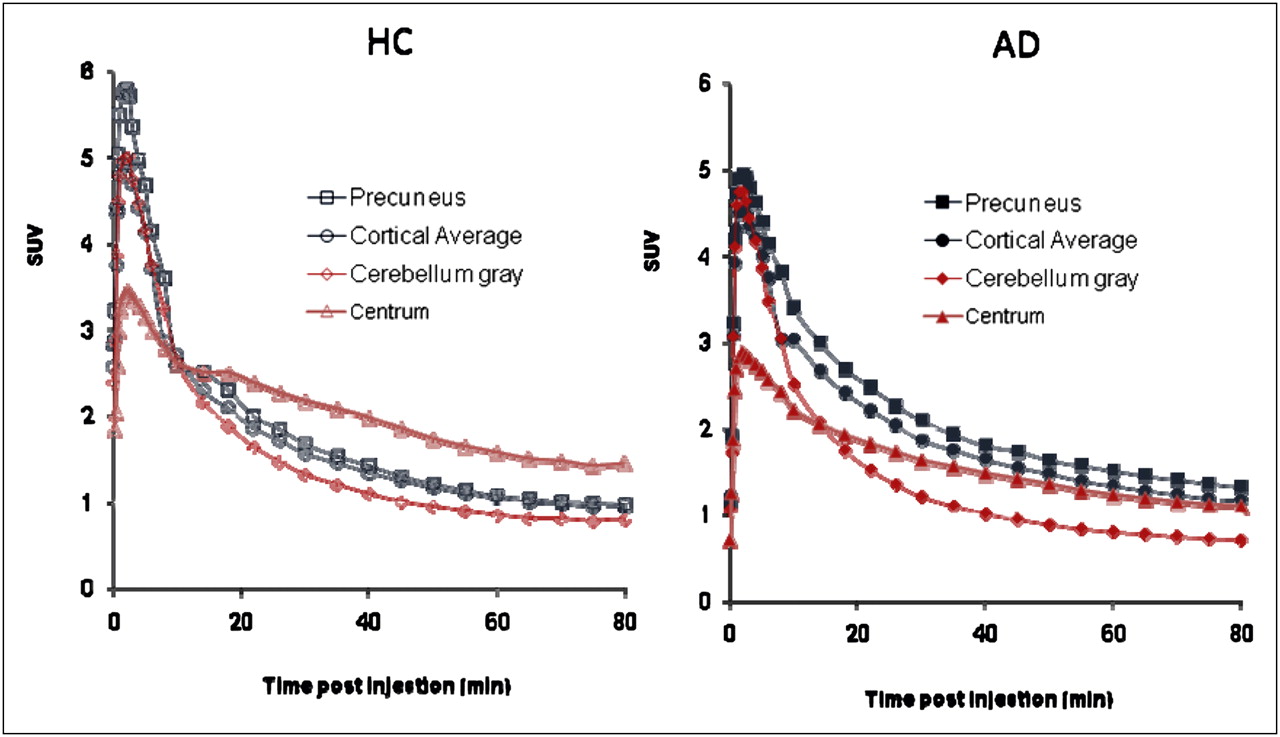
Mean time–activity curves. Mean precuneus, cortical average, and cerebellum SUVs are shown for subjects who were cognitively healthy (HC) and patients with AD. Subjects were scanned for approximately 90 min (horizontal axis represents beginning of each imaging time point, for example, 80–90 min).
Figure 3 shows the average cortical-to-cerebellum SUVR for AD patients and HCs for the 0- to 90-min period. Cortical average SUVRs relative to the cerebellum were higher in AD patients than in HCs. The average cortical-to-cerebellar SUVRs in AD patients show continual substantial increases from 0 to 30 min after administration, with only small changes thereafter, essentially reaching an asymptote by 40–50 min after injection. SUVRs in both AD patients and HCs were relatively constant between 45 and 90 min. Thus, the 10-min period from 50 to 60 min was taken as a representative sample for the asymptotic period.
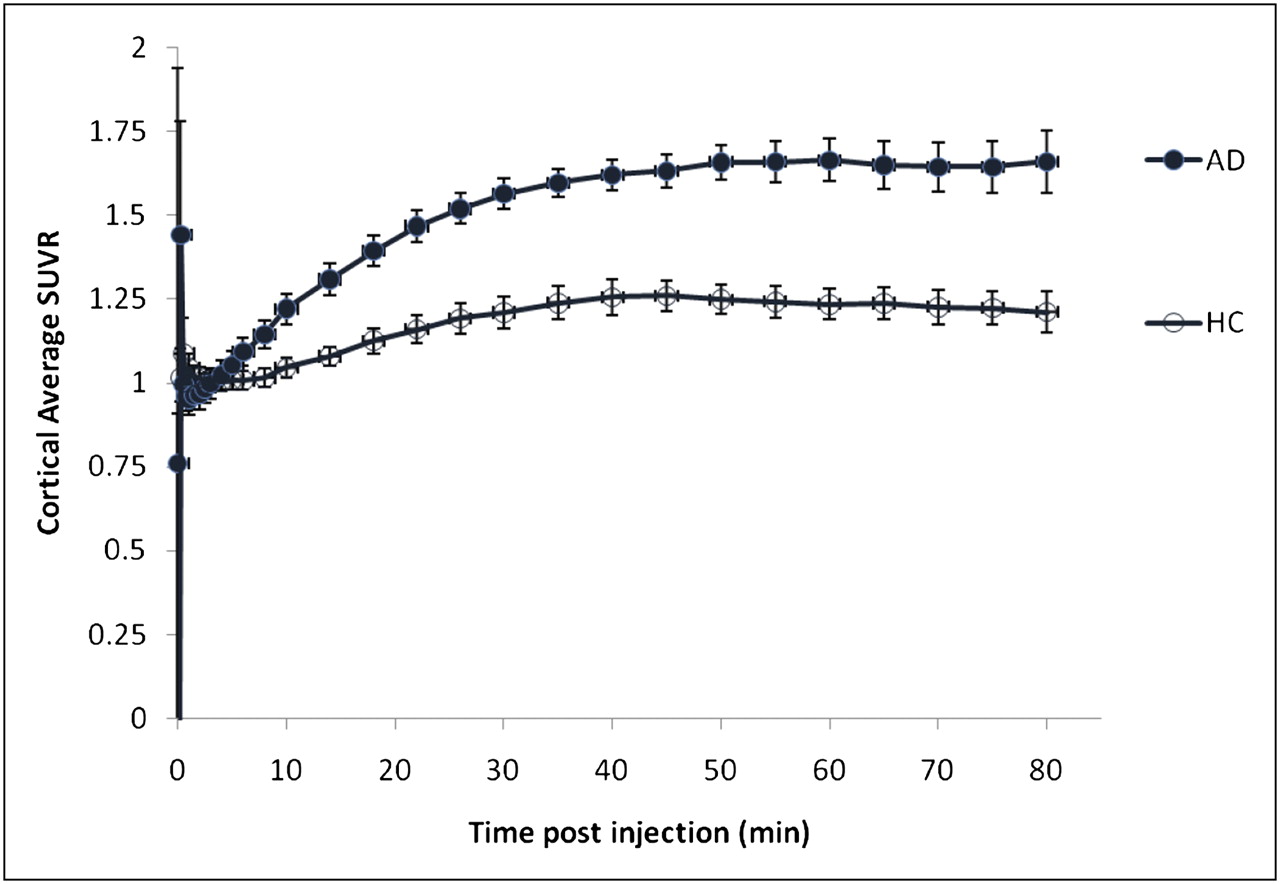
Mean cortical average SUVR for subjects who were cognitively healthy (HC) and patients with AD. As would be expected from SUV time–activity curves (Fig. 2), cortical target-to-cerebellum SUVRs for both AD patients and HCs approached asymptote at 50 min and remained essentially unchanged between 50 and 90 min after injection of 18F-AV-45. Subjects were scanned for approximately 90 min (horizontal axis represents beginning of each imaging time point, for example, 80–90 min).
Table 2 shows the mean SUVRs by cortical region for the 50- to 60-min time frame. The difference in tracer retention between patients with AD and HCs was greatest in the precuneus; SUVRs relative to the cerebellum were 1.86 ± 0.24 and 1.31 ± 0.27 for AD patients and HCs, respectively. In contrast, only a small, relatively inconsistent elevation in tracer retention was observed in the occipital cortex of AD patients. The overall cortical average SUVRs relative to the cerebellum were 1.67 ± 0.18 and 1.25 ± 0.18 for AD patients and HCs, respectively. For both AD patients and HCs, SUVRs relative to the centrum semiovale were lower than SUVRs relative to the cerebellum, but the pattern of separation between AD patients and HCs was similar to that seen with the cerebellar reference region.
SUVRs of Cortical Brain Region Relative to Cerebellum and Centrum Semiovale for 50- to 60-Minute Block: Evaluable Population
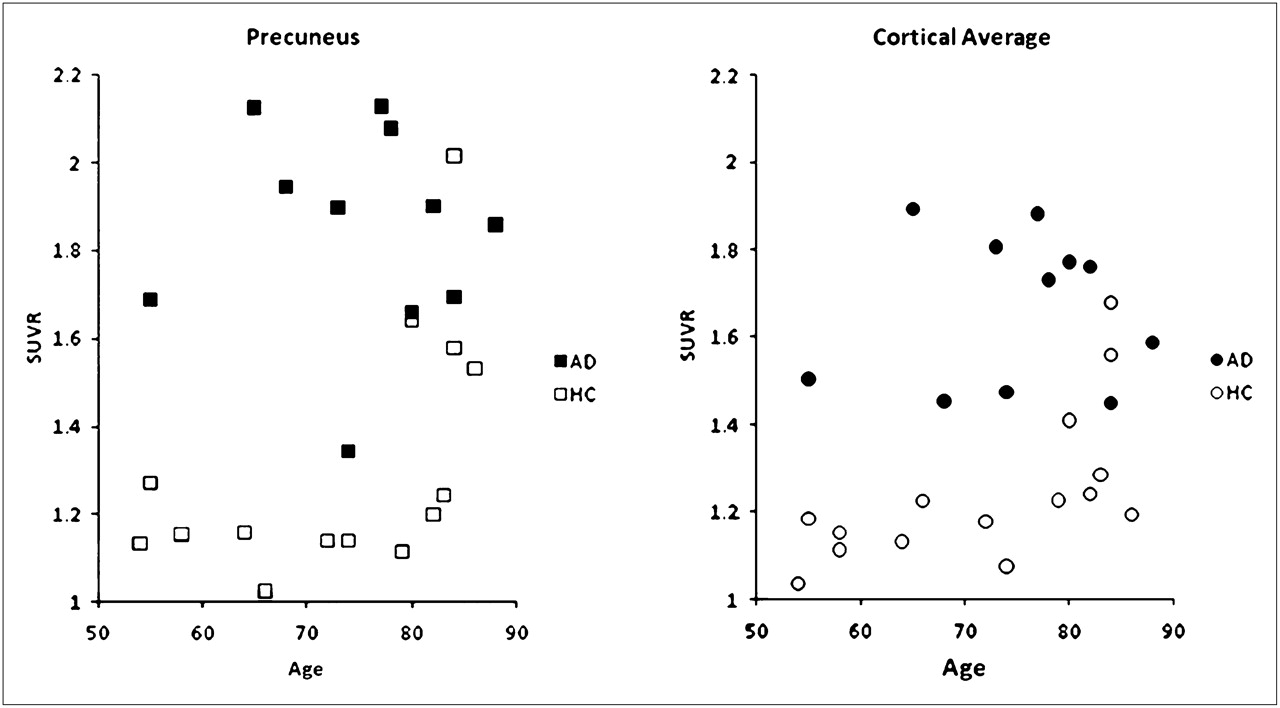
Figure 4 shows the precuneus and cortical average SUVRs for the 50- to 60-min time frame for individual AD patients and HCs. Most of the HC values were below the range seen in the AD patients, regardless of subject age. However, in 2 HCs older than 80 y, levels of tracer uptake were similar to those in AD patients; 2 other HCs older than 80 y showed borderline high tracer uptake, particularly in the precuneus. Although none of the AD patients had cortical average SUVRs in the HC range, 1 subject did have relatively low levels of 18F-AV-45 binding in the frontal cortex (not shown) and precuneus. Interestingly, this patient had an atypical presentation, including prominent behavior symptoms, gait disturbance, and mild cogwheeling, and was being treated for parkinsonism.

Precuneus and cortical average SUVR relative to cerebellum for individual AD patients and cognitively healthy subjects (HC) for all 3 imaging sites.
Comparison of SUVR Versus DVR
DVRs were measured in multiple brain regions for a subset of the subjects. Across all centers, the DVR values for individual patients were highly correlated with the corresponding regional SUVR for all regions tested (Spearman ρ ranged from 0.58 for the occipital cortex to 0.88 for the temporal cortex, P < 0.01 in all cases).
Radiolabeled Metabolite Analysis of 18F-AV-45
After an injection of 18F-AV-45, the total radioactivity in plasma and the fraction of plasma radioactivity accounted for by 18F-AV-45 were rapidly reduced. Plasma radioactivity was decreased by approximately 80% within 10 min and by approximately 90% within 20 min of injection. In addition to the parent, 18F-AV-45, 3 metabolite peaks were observed. These peaks were matched to cold reference standards and identified as desmethyl-18F-AV-45 (desmethyl 18F-AV-45 can be referred to as 18F-AV-160), N-acetyl-18F-AV-160, and an 18F polar species, the identity of which has not been confirmed.
The supplemental data provide further results pertaining to DVR and SUVR relationships, metabolite analysis, radiation dosimetry and safety.
Whole-Body Radiation Dosimetry
Although the number of subjects and whole-body imaging time points was too few to provide definitive quantitative estimates of radiation dosimetry, preliminary results revealed no unexpected accumulation of tracer. The preliminary estimate of whole-body effective dose was approximately 0.013 mSv/MBq. The organs of excretion—particularly gallbladder, liver, intestines, and urinary bladder—received the greatest exposure.
DISCUSSION
Sixteen AD patients and 16 elderly HCs received 18F-AV-45, with usable imaging data for a total of 11 AD patients and 15 HCs. AD patients showed accumulation of 18F-AV-45 in gray matter cortical target areas expected to be high in Aβ deposition, such as the frontal cortex, temporal cortex, and precuneus. Less consistent tracer accumulation was seen in the occipital cortex, in which Aβ deposition is thought to occur variably and later in the course of the disease. In contrast, HCs showed minimal tracer accumulation, predominantly in white matter areas. This pattern is similar to that previously reported for 11C-PIB (21,22) and 18F-BAY94-9172 (9).
The highest SUVRs were observed in the precuneus of AD patients, and the greatest difference between 18F-AV-45 activity in AD patients and HCs was observed in the precuneus and temporal cortex. This finding is consistent with the known localization of Aβ in these areas in postmortem tissue (23), with recent literature suggesting the precuneus is involved in integrative functions including visual spatial coordination and working memory retrieval (24)—and with results from other Aβ radiotracers (9,25).
The brain kinetics for 18F-AV-45 also appear to be similar to those for 11C-PIB but faster than those for other 18F-labeled Aβ imaging agents such as 18F-BAY94-9172 and 18F-GE-067. The SUV time–activity curves for AD patients (but not HCs) showed a clear separation between cortical and cerebellar activity beginning around 30 min after injection. The average cortical-to-cerebellar SUVRs and the average cortical-to-centrum semiovale SUVRs in AD patients showed continual substantial increases from 0 to 30 min after administration. These SUVRs exhibited only small changes thereafter, reaching a plateau by 40–50 min after injection and remaining stable until at least 90 min after injection. In contrast, other 18F-labeled Aβ imaging agents appear not to reach asymptote until 90 min or more after administration (9,10). The present data suggest that short imaging times (5–10 min) for imaging conducted less than an hour after the administration of 18F-AV-45 will be feasible for routine clinical use.
Although there were clear differences in mean cortical-to-cerebellar SUVR between AD patients and HCs, 2 of 15 HCs (13%) showed a pattern of tracer uptake similar to that in AD patients and 2 other HCs showed borderline-high tracer uptake, particularly in the precuneus. Mintun et al. (22) similarly observed AD-like uptake in 10% of controls and borderline-high uptake in another 10% of controls imaged with 11C-PIB. The present findings are also consistent with literature suggesting that 13%−45% of cognitively healthy subjects have significant Aβ pathology at autopsy (26–29). Mintun et al. (22) argued that elevated retention of PET Aβ imaging agents in otherwise cognitively healthy elderly subjects might reflect preclinical AD pathologic changes. However, longitudinal studies will ultimately be required to determine the significance of such findings for both 11C-PIB and 18F-AV-45.
Although none of the AD patients had cortical average SUVRs in the HC range, 1 presumed AD patient had an HC-like pattern of tracer uptake, particularly in the frontal cortex and precuneus. Interestingly, this AD patient had an unusual presentation, including prominent behavior symptoms, gait disturbance, and mild cogwheeling, and was being treated for parkinsonism. These symptoms, together with the limited tracer uptake, may point to an alternative or additional etiology for the patient's cognitive decline. On the other hand, although this presumed AD patient has an arguably atypical presentation, it would not be unexpected to find low 18F-AV-45 binding or low Aβ burden in some clinically diagnosed AD patients, even with more typical presentations. Literature reports suggest that approximately 10%−20% of patients diagnosed as having probable AD may fail to meet pathologic criteria for AD at autopsy (30–33).
To test the validity of the SUVR analysis used for the present study, DVRs were measured in all brain regions for a subset of the subjects using an analogous but independent set of VOIs and a more sophisticated mathematic modeling approach previously described by Zhou et al. (15). This approach has been successfully used with 11C-PIB and has been useful in demonstrating subtle differences associated with mild cognitive impairment (16). Despite the fact that slightly different VOIs were considered in the 2 approaches (the DVR analysis in this study used the VOIs from the Zhou et al. studies (15,16), rather than the VOIs from the SUVR analysis of this study), the results from the DVR analysis were consistent and highly correlated with the results of the SUVR analysis (Table 3; Supplemental Figs. 2 and 3). DVRs in AD patients were significantly elevated in comparison to DVRs in HCs. Thus, both standard SUVRs during the representative imaging period (50–60 min after the dose administration) and dynamic parametric mapping methods showed significant elevations in 18F-AV-45 in several brain regions of AD patients, compared with HCs. These findings provide strong cross validation for the methods and results (and the VOIs) obtained via the SUVR analysis. In our companion paper, we (Paul B. Rosenberg, Dean F. Wong, Steven Edell, et al., submitted 2010) will report on the relationship between behavioral and neuropsychologic measures and 18F-AV-45 for both SUVs and some DVR measures.
Average and SD of DVRs in AD Patients and HCs
Tracer plasma kinetics and metabolism were also examined in this study (supplemental materials). Although brain SUVs reached a plateau at 50–60 min of around 20% (in nontarget tissue) to 40% of initial levels (in Aβ-containing cortical tissue of AD patients), plasma radioactivity was reduced to less than 10% of the initial level by 20 min after injection (Supplemental Fig. 4). Because of the rapid clearance of total radioactivity from plasma, it seems unlikely that plasma levels of radioactive metabolite could be high enough to account for the observed tracer activity in the brain. The supplemental material provides additional information.
18F-AV-45 was shown to be well tolerated in the population studied (supplemental material). No serious adverse events or clinically significant changes in laboratory or electrocardiogram parameters were observed. Additionally, whole-body imaging revealed no unexpected accumulation of tracer.
A weakness of the present study is that the number of subjects and whole-body imaging time points was too few to provide definitive quantitative estimates of radiation dosimetry. However, a subsequent study evaluated whole-body exposure for up to 6 h after the administration of 18F-AV-45. A preliminary report (34) confirmed the present finding that the organs of excretion—particularly the gallbladder, liver, intestines, and urinary bladder—received the greatest radiation exposure.
A second potential weakness of the study is that 6 of 32 planned subjects were not included in the primary analysis. Data from the first HC were lost because of PET scanner problems; 1 AD withdrew consent, and 4 of 16 AD patients exhibited significant movement during the 90-min scanning. Because this was a first study in humans, designed to evaluate the potential of 18F-AV-45 for future development, the decision was made to focus only on the 26 images that could be accurately quantified with minimal movement artifacts and attenuation error. On visual examination, the images of the 4 excluded AD patients were not atypical, but accurate quantification of these images was precluded by potential attenuation error.
These imaging failures illustrate the need for a simple and brief acquisition procedure when imaging AD patients in a community setting. In the present study, scans averaged over a 10-min period beginning 50 min after injection were sufficient to reliably distinguish 18F-AV-45 binding in AD patients from that in HCs in each of the relevant cortical areas (Table 2). Additionally, Figure 3 suggests that scans as short as 5 min could be effective. Moreover, because AD and HC SUVRs appear stable between 40 and 90 min, an opportunity may exist to reposition and repeat a scan if a patient moves or a technical error occurs during the initial 10-min scan.
CONCLUSION
18F-AV-45 was shown in this first study in humans to be well tolerated, with no serious adverse events. The cortical target regions in patients with AD had higher uptake of 18F-AV-45 over time than did regions in subjects who were cognitively healthy. The greatest increase in uptake occurred in the precuneus and temporal cortex of AD patients, compared with HCs. Scans 50–60 min after injection produced reliable imaging results. 18F-AV-45—given its relatively long radioactive half-life, relatively rapid kinetics (requiring a short postdose waiting period and short imaging durations), and relatively long, stable plateau (providing flexibility in timing of the image)—may be a robust imaging tool and potentially well suited as a biomarker for AD in large multicenter treatment and natural history trials (e.g., Alzheimer's Disease Neuroimaging Initiative) and for imaging in community settings.
Acknowledgments
We thank Joel Ross and Steven Edell, principal investigators at the Memory Enhancement Center and the Community Health Research center, respectively; Weiguo Ye, Mohab Alexander, Jeffery Galecki, Maria Thomas, Melanie Charlotte, and Cynthia Hawes for technical support and recruitment; Hiroto Kuwabara for assistance with the use of his data-analysis software; Olivier Rousset for scientific discussions; and Michael Stabin, of Vanderbilt University, for radiation dosimetry calculations. This study was supported in part by Avid Radiopharmaceuticals and NIH grants K24DA000412, MH078175, and AA012839 (all DFW). The study was presented in part at the Society for Nuclear Medicine annual meeting in June 2008 and the World Congress of Molecular Imaging in July 2008. JHU employees are also associated with phase III contracts (Pfizer, Lilly) with therapeutic AD drugs using 18F-AV-45 as an outcome measure. Abhinay D. Joshi, Daniel M. Skovronsky, and Michael J. Pontecorvo are Avid Radiopharmaceuticals employees. Hank F. Kung is a scientific advisor and shareholder of Avid Radiopharmaceuticals.
Footnotes
-
COPYRIGHT © 2010 by the Society of Nuclear Medicine, Inc.
References
- Received for publication August 4, 2009.
- Accepted for publication January 5, 2010.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Analyzing heterogeneity in Alzheimer Disease using multimodal normative modeling on imaging-based ATN biomarkers
- Traumatic brain injury and Alzheimers Disease biomarkers: A systematic review of findings from amyloid and tau positron emission tomography (PET)
- Inter-scanner A{beta}-amyloid PET harmonization using barrel phantom spatial resolution matching
- The RSNA QIBA Profile for Amyloid PET as an Imaging Biomarker for Cerebral Amyloid Quantification
- Synthesizing Images of Tau Pathology from Cross-modal Neuroimaging using Deep Learning
- Multimodal brain age estimates relate to Alzheimer disease biomarkers and cognition in early stages: a cross-sectional observational study
- Dynamic Amyloid PET: Relationships to 18F-Flortaucipir Tau PET Measures
- Defining the Lowest Threshold for Amyloid-PET to Predict Future Cognitive Decline and Amyloid Accumulation
- Switching on Brain PET to Light Up Amyloid Pathology In Vivo (perspective on "In Vivo Imaging of Amyloid Deposition in Alzheimer Disease Using the Radioligand 18F-AV-45 (Florbetapir F 18)" J Nucl Med. 2010;51:913-920)
- Detecting earlier stages of amyloid deposition using PET in cognitively normal elderly adults
- Spatial relationships between white matter degeneration, amyloid load and cortical volume in amnestic mild cognitive impairment
- [18F]Florbetapir positron emission tomography: identification of muscle amyloid in inclusion body myositis and differentiation from polymyositis
- Amyloid Load: A More Sensitive Biomarker for Amyloid Imaging
- Spatial Normalization of 18F-Flutemetamol PET Images Using an Adaptive Principal-Component Template
- Regional amyloid accumulation and cognitive decline in initially amyloid-negative adults
- White Matter Reference Region in PET Studies of 11C-Pittsburgh Compound B Uptake: Effects of Age and Amyloid-{beta} Deposition
- Flortaucipir F 18 Quantitation Using Parametric Estimation of Reference Signal Intensity
- Clinical Neurology and Epidemiology of the Major Neurodegenerative Diseases
- Clinical utility of amyloid PET imaging with (18)F-florbetapir: a retrospective study of 100 patients
- Validation of the Semiquantitative Static SUVR Method for 18F-AV45 PET by Pharmacokinetic Modeling with an Arterial Input Function
- Prediction of the Clinical SUV Ratio in Amyloid PET Imaging Using a Biomathematic Modeling Approach Toward the Efficient Development of a Radioligand
- Predicting Alzheimer disease from a blood-based biomarker profile: A 54-month follow-up
- Molecular Structure of Aggregated Amyloid-{beta}: Insights from Solid-State Nuclear Magnetic Resonance
- Standardized Expression of 18F-NAV4694 and 11C-PiB {beta}-Amyloid PET Results with the Centiloid Scale
- Visualization and Quantification of 3-Dimensional Stereotactic Surface Projections for 18F-Flutemetamol PET Using Variable Depth
- Impact of MR-Based Attenuation Correction on Neurologic PET Studies
- A{beta}-related memory decline in APOE {varepsilon}4 noncarriers: Implications for Alzheimer disease
- Performance of 11C-Pittsburgh Compound B PET Binding Potential Images in the Detection of Amyloid Deposits on Equivocal Static Images
- A Semiautomated Method for Quantification of F 18 Florbetapir PET Images
- Technical Considerations in Brain Amyloid PET Imaging with 18F-Florbetapir
- Optimal Target Region for Subject Classification on the Basis of Amyloid PET Images
- Use of Standardized Uptake Value Ratios Decreases Interreader Variability of [18F] Florbetapir PET Brain Scan Interpretation
- Measurement of Longitudinal {beta}-Amyloid Change with 18F-Florbetapir PET and Standardized Uptake Value Ratios
- 18F-Florbetapir PET in Patients with Frontotemporal Dementia and Alzheimer Disease
- Automated Quantification of 18F-Flutemetamol PET Activity for Categorizing Scans as Negative or Positive for Brain Amyloid: Concordance with Visual Image Reads
- Molecular Imaging of Alzheimer Disease Pathology
- Seoul criteria for PiB(-) subcortical vascular dementia based on clinical and MRI variables
- Cortical {beta}-amyloid levels and neurocognitive performance after cardiac surgery
- Longitudinal Amyloid Imaging Using 11C-PiB: Methodologic Considerations
- Implementation and Validation of an Adaptive Template Registration Method for 18F-Flutemetamol Imaging Data
- Head-to-Head Comparison of 11C-PiB and 18F-AZD4694 (NAV4694) for {beta}-Amyloid Imaging in Aging and Dementia
- Brain Amyloid Imaging
- Amyloid-{beta} Imaging with Pittsburgh Compound B and Florbetapir: Comparing Radiotracers and Quantification Methods
- Imaging Approaches for Dementia
- Preclinical Characterization of a Novel Class of 18F-Labeled PET Tracers for Amyloid-{beta}
- Initial Clinical Comparison of 18F-Florbetapir and 18F-FDG PET in Patients with Alzheimer Disease and Controls
- Relative Equilibrium Plot Improves Graphical Analysis and Allows Bias Correction of Standardized Uptake Value Ratio in Quantitative 11C-PiB PET Studies
- Brain Imaging in Alzheimer Disease
- Clinical Validation of 18F-AZD4694, an Amyloid-{beta}-Specific PET Radioligand
- Performance Characteristics of Amyloid PET with Florbetapir F 18 in Patients with Alzheimer's Disease and Cognitively Normal Subjects
- Brain Amyloid Imaging
- Amyloid Imaging with 18F-Florbetaben in Alzheimer Disease and Other Dementias
- Early 11C-PIB Frames and 18F-FDG PET Measures Are Comparable: A Study Validated in a Cohort of AD and FTLD Patients
- Target-Specific PET Probes for Neurodegenerative Disorders Related to Dementia