


Abstract
This article reviews the results of somatostatin receptor imaging (SRI) in patients with somatostatin receptor–positive neuroendocrine tumors, such as pituitary tumors, endocrine pancreatic tumors, carcinoids, gastrinomas, and paragangliomas, or other diseases in which somatostatin receptors may also be expressed, like sarcoidosis and autoimmune diseases. [111In-DTPA0]octreotide is a radiopharmaceutical that has great potential for helping visualize whether somatostatin receptor–positive tumors have recurred. The overall sensitivity of SRI to localize neuroendocrine tumors is high. In several neuroendocrine tumor types, inclusion of SRI in the localization or staging procedure may be very rewarding in terms of cost effectiveness, patient management, or quality of life. The value of SRI in patients with other tumors, such as breast cancer or malignant lymphomas, or in patients with granulomatous diseases has to be established. The application of radiolabeled peptides may be clinically useful in another way: after the injection of [111In-DTPA0]octreotide, surgeons can detect tumor localizations by a probe that is used during the operation. This may be of particular value if small tumors with a high receptor density are present (e.g., gastrinomas). As the success of peptide receptor scintigraphy for tumor visualization became clear, the next logical step was to try to label these peptides with radionuclides emitting α or β particles, or Auger or conversion electrons, and to perform radiotherapy with these radiolabeled peptides. The results of the described studies with 90Y- and 111In-labeled octreotide show that peptide receptor radionuclide therapy using radionuclides with appropriate particle ranges may become a new treatment modality. One might consider the use of radiolabeled somatostatin analogs first in an adjuvant setting after surgery of somatostatin receptor–positive tumors to eradicate occult metastases and second for cancer treatment at a later stage.
- [111In-DTPA0]octreotide
- [90Y-DOTA0,Tyr3]octreotide
- somatostatin receptor scintigraphy
- peptide receptor radionuclide therapy
Cells express on their cellular membranes a variety of receptor proteins with a high affinity for regulatory peptides, including somatostatin. Somatostatin receptors are integral membrane glycoproteins that are distributed in a variety of tissues throughout the body (1). Alterations of somatostatin receptor expression during disease, such as overexpression in many neoplasia, can be exploited by imaging techniques. Therefore, peptide receptor scintigraphy with the small radioactive somatostatin analog, [111In-DTPA0]octreotide, appeared to be a sensitive and specific technique to show in vivo the presence of somatostatin receptors on various tumors. Receptor-positive tumors may originate in the neuroendocrine system, such as pituitary adenomas, gastroenteropancreatic tumors, and pancreatic islet-cell tumors (2–3), but other tumors, such as lymphomas and breast cancer, may possess these receptors as well (4,5). A new and fascinating application of somatostatin receptors is the use of radiolabeled somatostatin analogs for peptide receptor radionuclide therapy (PRRT).
In receptor-mediated endocytosis systems, cell membrane receptors bind their ligands from the extracellular milieu. We have studied internalization and degradation of radiolabeled [DTPA0]octreotide in somatostatin receptor–positive tumor cell lines. This process appeared to be receptor specific and temperature dependent (6). Receptor-mediated internalization of [111In-DTPA0]octreotide results in degradation to the final radiolabeled metabolite 111In-DTPA-D-Phe in the lysosomes (7). This metabolite is not capable of passing through the lysosomal or other cell membrane(s) and will, therefore, stay in the lysosomes, causing the long intracellular retention time of 111In (7). This internalization process of [111In-DTPA0]octreotide is essential for successful scintigraphy and radionuclide therapy of tumors, because various radionuclides that are suitable for radiotherapy (e.g., those emitting conversion and Auger electrons such as 111In) are only effective in a short distance of only a few nanometers to micrometers from their target, the nuclear DNA. Because there is a long biologic half-life for 111In in tumor tissue, 111In-labeled [DTPAo]octreotide has an appropriate distribution profile in humans for scintigraphy and radionuclide therapy.
In experiments involving saturable processes, the target-to-background ratio is often improved by lowering the mass of the radiotracer, by increasing its specific activity, or both. In our first preclinical studies, the administered mass of peptide and the radioactive dose were such that more than 90% of the ligand was unlabeled (8). Theoretically, an excess of unlabeled [DTPA0]octreotide may have a negative effect on the percentage of dose uptake of [111In-DTPA0]octreotide in somatostatin receptor–positive tissues, because of competition for the same receptor. Therefore, we investigated whether receptor scintigraphy showed an optimal target-to-background ratio at the lowest possible mass of peptide (i.e., the highest specific activity), which would lead to a higher sensitivity of the imaging technique. We also felt this study to be important because another report (9) suggested that prior administration of unlabeled peptide to patients increased uptake of the radioactive peptide in the tumor. Our investigations in rats indicated that, contrary to what we expected, uptake of [111In-DTPA0]octreotide in octreotide receptor–positive tissues is not maximal at the lowest possible peptide amount or maximum specific activity. The uptake expressed as percentage administered dose is a bell-shaped function of the injected mass (10). These findings have also been confirmed by research on humans, which has shown that when a standard dose of 220 MBq 111In is coupled to less than 5 μg [DTPA0]octreotide, there is a decreased quality of scintigraphy and a significantly reduced uptake in tumors (11). Therefore, [111In-DTPA0]octreotide scans should always be performed with at least 10 μg peptide (as supplied in the kit formulation).
SCINTIGRAPHY
Scanning Protocol
The preferred dose of [111In-DTPA0]octreotide (with at least 10 μg of the peptide; see above) is approximately 200 MBq. With such a dose, it is possible to perform SPECT, which may increase the sensitivity in detecting somatostatin receptor–positive tissues and give a better anatomic delineation than planar views. Acquiring sufficient counts per view and obtaining spot images with a sufficient counting time, instead of performing whole-body scanning with a too-low count density, are other important points that may influence the success of a localizing study.
Planar images are obtained with a double-head or large field of view gamma camera, equipped with medium-energy, parallel-hole collimators. The pulse height analyzer windows are centered over both 111In photon peaks (172 keV and 245 keV) with a window width of 20%. The acquisition parameters for planar images (preferably spot views) are 300,000 preset counts or 15 min per view for the head and neck and 500,000 counts or 15 min for the remainder of the body. If whole-body acquisition is used, scan speed should not exceed 3 cm/min. Using higher scan speeds, such as 8 cm/min, will result in failure to recognize small somatostatin receptor–positive lesions and lesions with a low density of these receptors (12). For SPECT images with a triple-head camera the acquisition parameters are: 40 steps of 3° each, 64 × 64 matrix, and at least 30 s per step (45 s for SPECT of the brain). SPECT analysis is performed with a Wiener or Metz filter on original data. The filtered data are reconstructed with a ramp filter.
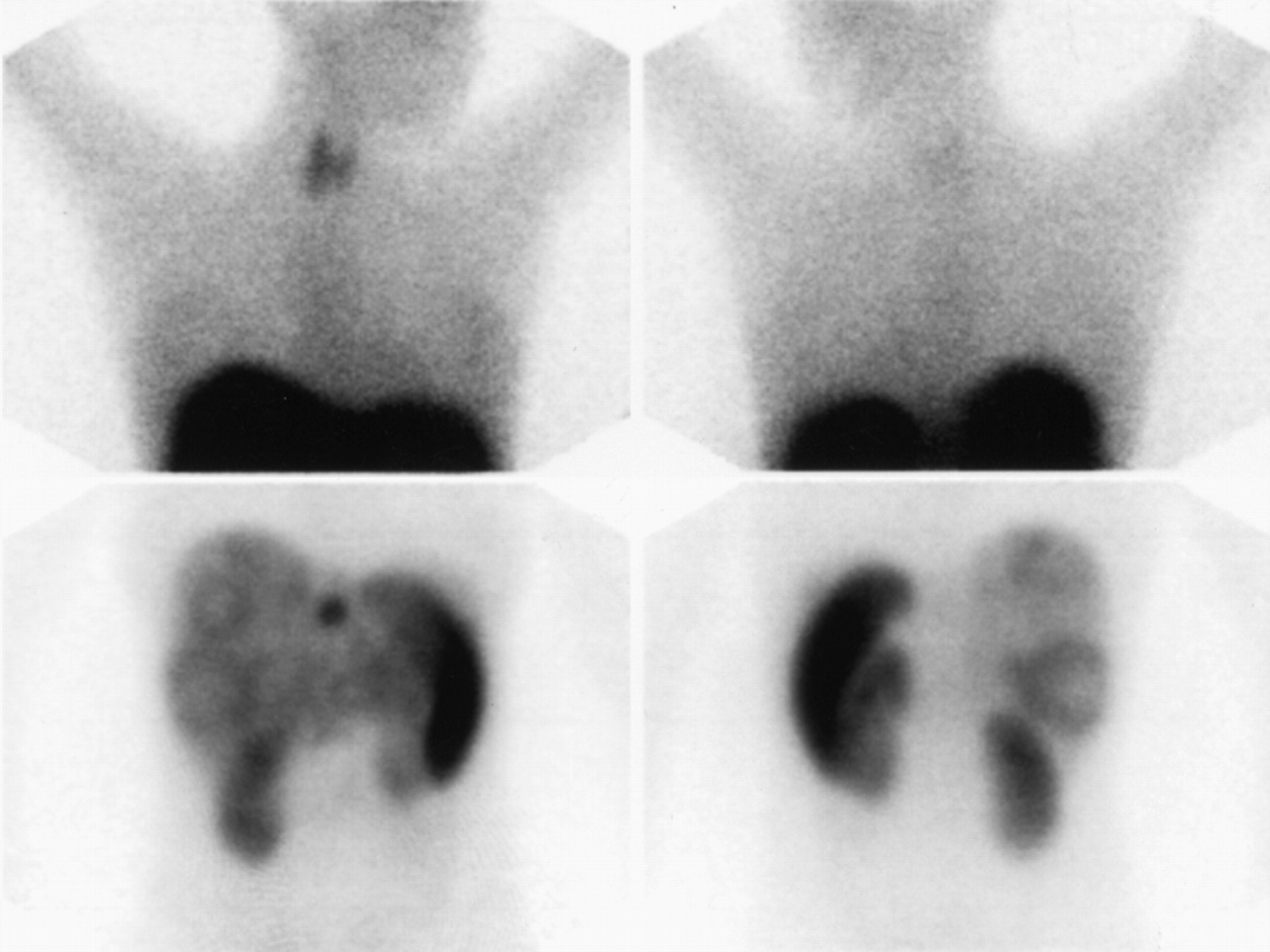
Because of its relatively long effective half-life, [111In-DTPA0]octreotide is a radiolabeled somatostatin analog that can be used to see somatostatin receptor bearing tumors efficiently after 24 and 48 h, when interfering background radioactivity is minimized by renal clearance. Therefore, planar and SPECT studies are preferably performed 24 h after injection of the radiopharmaceutical. A higher lesion-detection rate of 24 h planar imaging over 4 h acquisition was reported by Jamar et al. (13), as well as the additional value of SPECT imaging (Fig. 1). Planar studies can be performed with the same protocol after 24 and 48 h. Repeat scintigraphy after 48 h is particularly important when 24 h scintigraphy shows accumulation in the abdomen, which may also represent radioactive bowel content.

Example of additional information obtained with SPECT imaging (A and B) compared with planar abdominal imaging (C and D). With planar imaging, there is homogeneous liver activity; there is some breast attenuation on anterior image (C). Increased activity in cranial part of liver can be seen in A and especially B. Note gallbladder activity in B.
Normal Scintigraphic Findings and Artifacts
Normal scintigraphic features include visualization of the thyroid, spleen, liver, kidneys, and in part of the patient's pituitary. In addition, the urinary bladder and the bowel (to a variable degree) are usually visualized (Fig. 2). The visualization of the pituitary, thyroid, and spleen occurs because of receptor binding. Uptake in the kidneys is for the most part from reabsorption of the radiolabeled peptide in the renal tubular cells after glomerular filtration, although somatostatin receptors have been demonstrated in human renal tubular cells and vasa recta (14). There is a predominant renal clearance of the somatostatin analog, although hepatobiliary clearance into the bowel also occurs, which necessitates the use of laxatives to facilitate the interpretation of abdominal images.
Normal SRI scan, 24 h after injection. Left lateral anterior, posterior, and right lateral images of head and neck (A), and anterior (B) and posterior (C) spot views. Note faint uptake in pituitary and thyroid glands. Normal visualization of kidneys, liver, spleen, and bowel and bladder activity.
False-positive results of somatostatin receptor scintigraphy (SRI) have been reported. In virtually all cases the term “false-positive” is a misnomer because somatostatin receptor–positive lesions are present that are not related to the pathology for which the investigation is performed; examples include the visualization of the gallbladder, thyroid abnormalities, accessory spleens, recent CVAs, activity at the site of a recent surgical incision, and so forth. Many of these results have been reviewed by Gibril et al. (15). In addition, chest uptake after irradiation and diffuse breast uptake in female patients can be mistaken for other pathology. In some patients, the coexistence of 2 different somatostatin receptor–positive diseases should be considered. Diminished uptake in the spleen because of ongoing treatment with octreotide may occur, which may be accompanied by a lower liver uptake. In case of hepatic metastases, this phenomenon may be misinterpreted as a better uptake in the liver metastases.
Imaging Results in Neuroendocrine and Other Tumors
Pituitary Tumors.
On virtually all growth hormone (GH)–producing pituitary adenomas, somatostatin receptors are present. Also, in vivo SRI is positive in most cases (16,17), but other pituitary tumors and pituitary metastases from somatostatin receptor–positive neoplasms, parasellar meningiomas, lymphomas, or granulomatous diseases of the pituitary may be positive. Therefore, the diagnostic value of SRI in pituitary tumors is limited (18).
Controversy exists as to the relationship between the calculated tumor-to-background ratios in pituitary acromegaly using SRI with [111In-DTPA0]octreotide and the extent of suppressibility of GH levels during octreotide treatment. Most investigators find no or only a weak correlation however (17,19). SRI, therefore, does not seem to help physicians decide whether to treat an acromegalic patient with octreotide.
Because of the limited effect of octreotide on hormone secretion by clinically nonfunctioning pituitary tumors, both in vivo and in vitro, and because of the absence of tumor shrinkage in the majority of patients studied, octreotide treatment in patients with a clinically nonfunctioning pituitary tumor does not seem promising (20,21). Therefore, there is no role for SRI in treatment selection (18).
Endocrine Pancreatic Tumors.
The majority of the endocrine pancreatic tumors can be seen using SRI (Figs. 3–5), so SRI can be of great value in localizing tumor sites in this type of patient. SRI can also be useful in those cases where surgery is indicated but no tumor localization can be found with conventional imaging modalities, which is frequently the case. Reported data on the sensitivity of SRI in patients with gastrinomas vary from 60–90% (22–25), and part of the discrepancy in results most likely is because of insufficient scanning technique (particularly short acquisition time), not performing SPECT studies, or injection of relatively low doses of [111In-DTPA0]octreotide, all of which lead to a poorer performance of SRI.
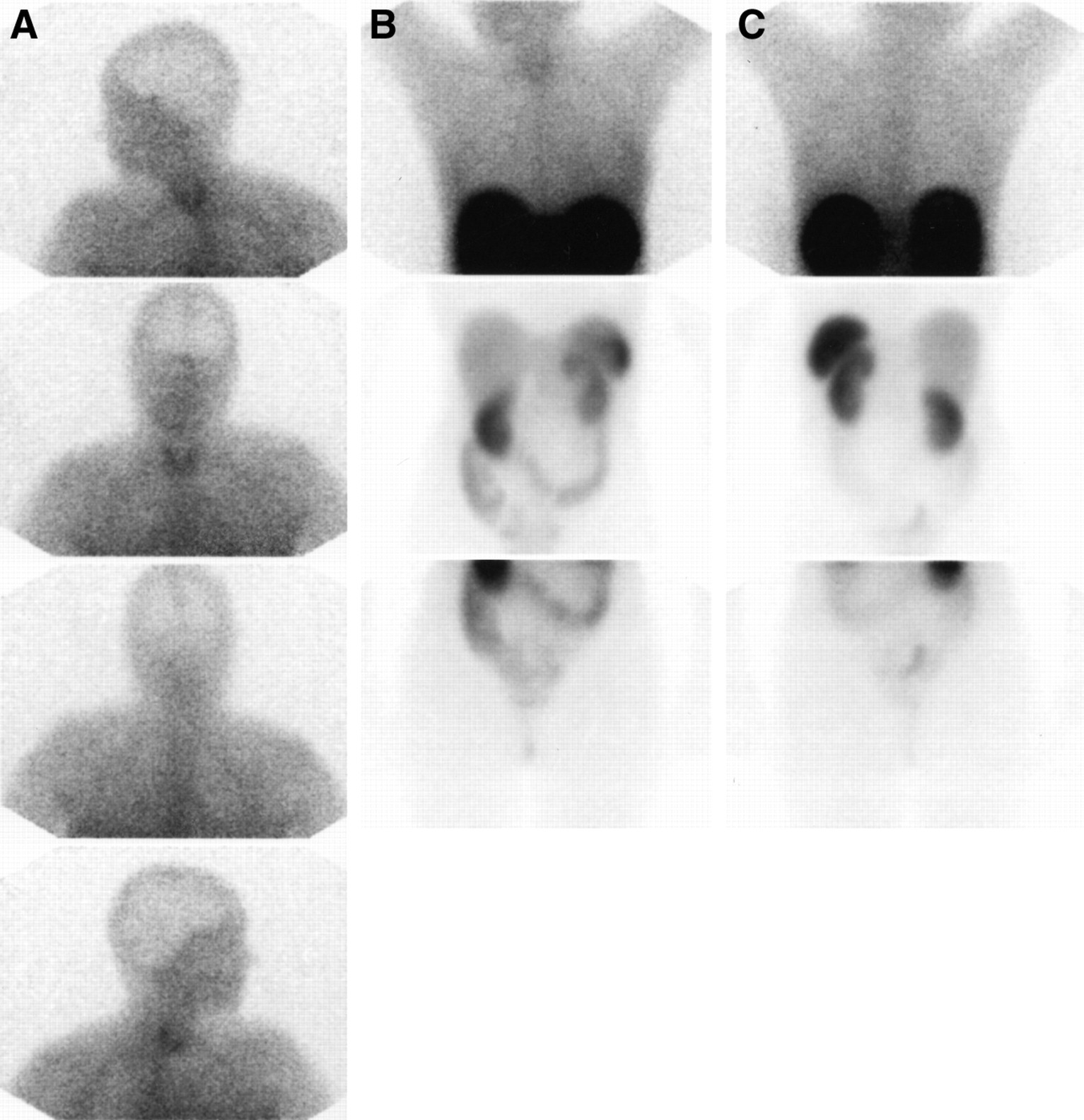
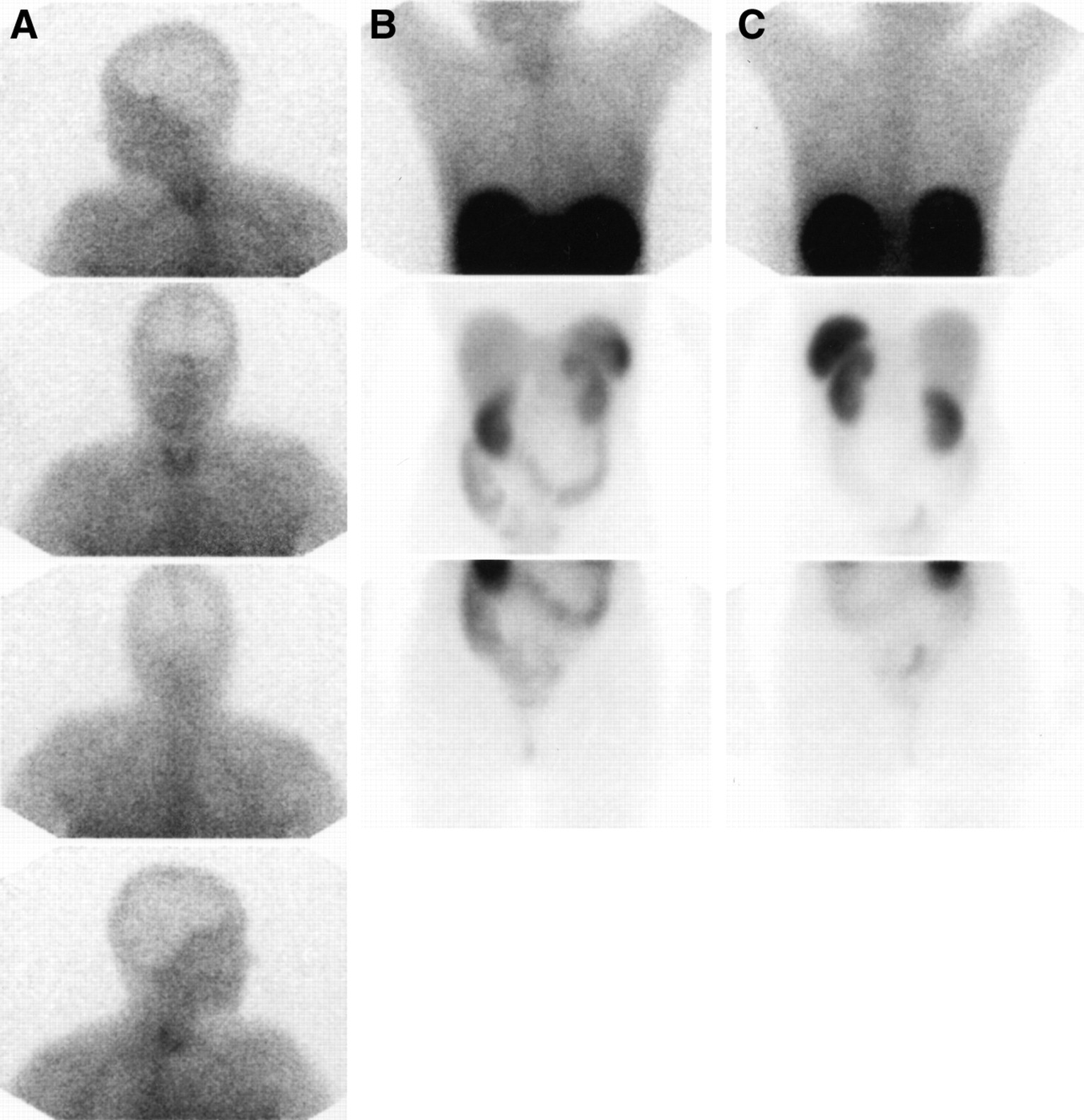
Lateral views of the head (A), anterior and posterior view of thorax (B), and anterior and posterior view of abdomen (C) 24 h after injection in patient with metastatic insulinoma. Note clear uptake in multiple liver metastases and in left supraclavicular region; also, note faint breast uptake that occurs in approximately 15% of female patients.

Visualization of neuroendocrine pancreatic tumor with liver metastases in patient with multiple endocrine neoplasia syndrome.

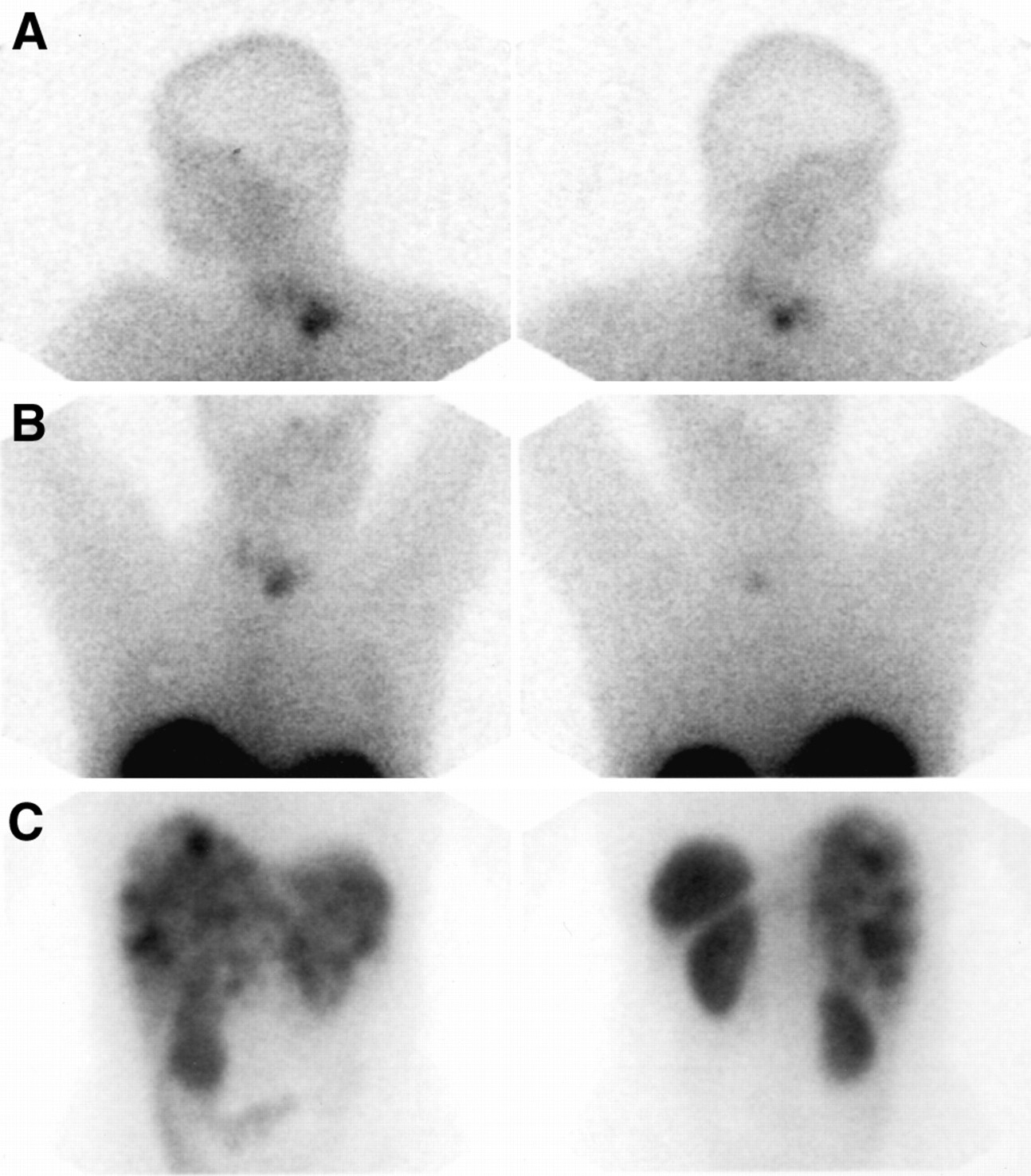
Images of patient with multiple liver metastases of neuroendocrine tumor. Note intense uptake in small lesion in midline and multiple lesions in liver with central necrosis. As in Figure 3, there is faint breast uptake.
With ultrasound, CT, MRI, or angiography, endocrine pancreatic tumors can be localized in about 50% of cases (26). Endoscopic ultrasound has been reported to be very sensitive in detecting endocrine pancreatic tumors, even when CT or transabdominal ultrasound fails to show the tumor (27). Results from studies that compared the value of endoscopic ultrasonography with SRI in the same patients have been favorable for SRI (23,25). Gibril et al. (24) published the results of a prospective study in 80 patients with Zollinger-Ellison syndrome, comparing SRI with a variety of other imaging techniques as well as angiography. They found that SRI was as sensitive as all of the other imaging studies combined, and they advocated using it as the first imaging method in these patients because of its sensitivity, simplicity, and cost effectiveness. Lebtahi et al. (28) reported that the results of SRI in 160 patients with gastroenteropancreatic tumors modified patient classification and surgical therapeutic strategy in 25% of patients. In addition, Termanini et al. (29) reported that the results from SRI caused physicians to alter patient management in 47% of 122 patients with gastrinomas. However, results in patients with insulinomas were disappointing, possibly because part of these tumors may either have been somatostatin receptor–negative or contained somatostatin receptors that did not bind octreotide.
Carcinoids.
Reported values for the detection of known carcinoid tumor localizations vary from 80% to nearly 100% (30–32). In addition, the detection of unexpected tumor sites, which were not suspected with conventional imaging, has been reported by several investigators (30,32,33).
Treatment with octreotide may cause a relief of symptoms and a decrease of urinary 5-HIAA levels in patients with the carcinoid syndrome (34). In patients with the carcinoid syndrome, SRI, because of its ability to show somatostatin receptor–positive tumors, could be used to help physicians select those patients who are likely to respond to octreotide treatment. On the other hand, for those patients who have somatostatin receptor–negative tumors, only chemotherapy is effective (35).
The impact of SRI use on patient management is fourfold: SRI may detect resectable tumors that would be unrecognized with conventional imaging techniques, it may prevent surgery in patients whose tumors have metastasized to a greater extent than can be detected with conventional imaging, it may direct the choice of therapy in patients with inoperable tumors, and it may be used to select patients for peptide receptor radionuclide therapy (PRRT; see below).
Paragangliomas.
In virtually all patients with paragangliomas, tumors can be easily detected (36), and unexpected additional paraganglioma sites are frequently found. Multicentricity and distant metastases have been reported as occurring in 10% of patients; in this study with SRI, we found multiple sites of pathology in 9 of 25 patients (36%) with a known paraganglioma (36). One of the major advantages of SRI is that it provides information on potential whole-body tumor sites in patients with paraganglioma. Therefore, SRI could be used as a screening test, to be followed by CT scanning, MRI, or ultrasound of the sites at which abnormalities are found.
Medullary Thyroid Carcinoma and Other Thyroid Cancers.
In patients with medullary thyroid carcinoma (MTC) the sensitivity of SRI in detecting tumor localizations is 50%–70% (37,38). In 17 patients with MTC who we studied (37), the ratio of calcitonin over carcinoembryonic antigen levels was significantly higher in patients for whom SRI was successfully used. This may imply that somatostatin receptors can be detected in vivo on the more differentiated forms of MTC. In addition, SRI is positive more frequently in patients with high serum tumor markers and large tumors (38) and, therefore, seems less suitable for showing microscopic disease (38,39).
Although papillary, follicular, and anaplastic thyroid cancers and also Hürthle-cell carcinomas do not belong to the group of traditional neuroendocrine tumors, the majority of patients with these cancers show uptake of radiolabeled octreotide during SRI (40,41) (Fig. 6). In addition, to perform SRI (42), it is not necessary to stop l-thyroxine suppression therapy in patients. Interestingly, differentiated thyroid cancers that do not take up radioactive iodine, may also show radiolabeled octreotide accumulation (40). In some patients, this could provide new therapeutic options: surgery, if the number of observed lesions is limited, or PRRT, if the uptake is sufficient.

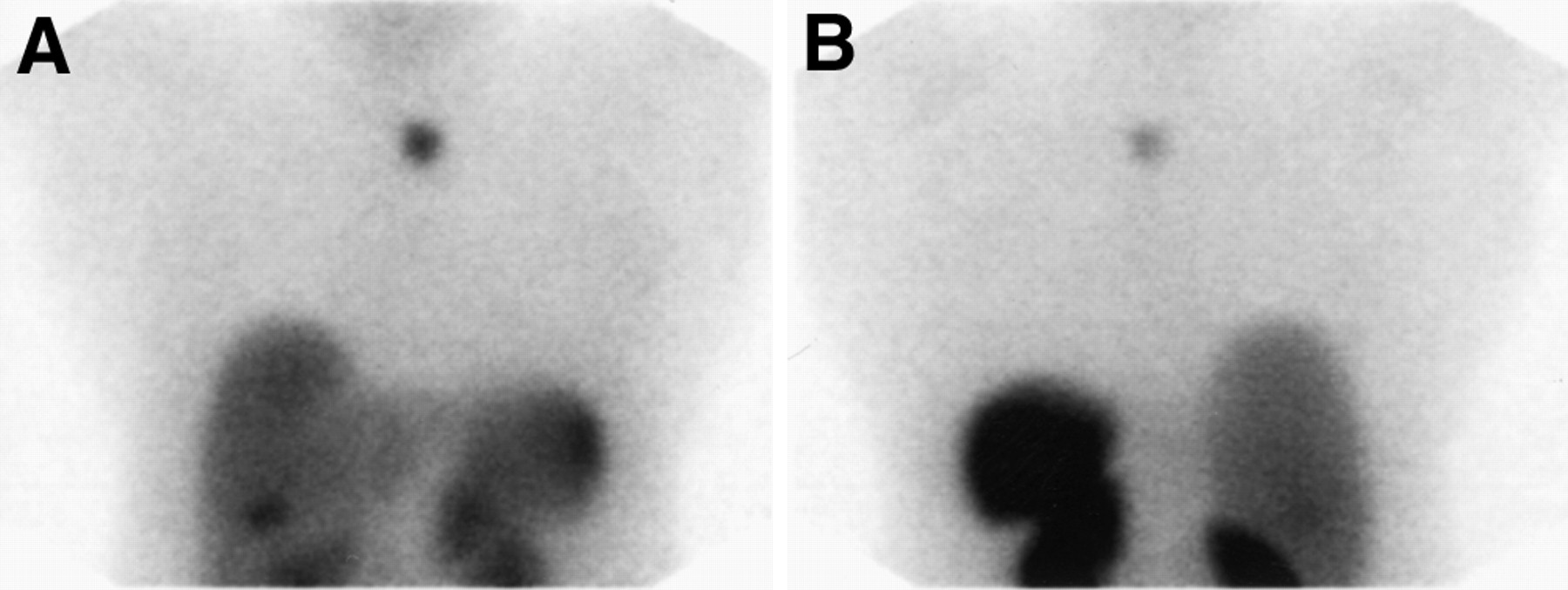
Anterior (A) and posterior (B) thoracic images in patient with remnant of Hürthle-cell carcinoma of thyroid. There is clear visualization of tumor and activity in liver, spleen, and kidneys. Note gallbladder visualization on anterior image.
Merkel Cell Tumors.
Trabecular carcinomas of the skin, or Merkel cell tumors, are aggressive neoplasms that tend to occur in sun-exposed skin. Often, these tumors metastasize, and, despite therapy, disease-related death is high. Ultrastructurally and immunocytochemically, the majority of these tumors have neuroendocrine characteristics.
In 1 study using SRI, 4 of the 5 patients in whom tumors had been found by CT, ultrasound, or both, had sites that were recognized on the scintigrams. In 2 patients, SRI demonstrated more metastatic tumor localizations than previously recognized (43).
If SRI were performed in patients with Merkel cell tumors, the sites of abnormal accumulation of radioactivity could be visualized thereafter using CT scanning or ultrasound, and biopsies could be taken. Establishing the extent of the disease in this way may ensure an optimal choice of treatment for these tumors.
Small Cell Lung Cancer (SCLC).
With SRI, the primary tumors can be demonstrated in virtually all patients with SCLC (44–46), but part of the known metastases may be missed. The unexpected finding of brain metastases, in particular, has been reported by several authors (44,45). Others, however, have reported the lack of any additional information using SRI (47). Of special interest are 2 groups of patients in whom the additional information provided by SRI may have therapeutic consequences: those in whom unexpected cerebral metastases are found and those in whom the additional information leads to upstaging the diagnosis from limited disease (LD) to extensive disease (ED). Adding SRI to the staging protocol in patients with SCLC would lead to an upstaging in 5 of 14 patients (36%) out of a group of 26 untreated patients whom we studied (45), who seemingly had LD with conventional imaging only. With conventional imaging, cerebral metastases were discovered in 2 patients. SRI showed cerebral metastases in these 2 and in another 5 patients. In 4 of the patients, cerebral metastases occurred within 1 y.
Inclusion of SRI in the staging protocol of patients with SCLC may lead to upstaging in some of the patients with LD. The cost increase of using SRI compared with conventional procedures alone needs only to be weighed against an unnecessary treatment in a portion of patients with LD (i.e., local chest radiotherapy if a complete remission is achieved) (48). Using SRI for the diagnostic procedures of patients with SCLC would help detect otherwise unseen brain metastases. From a radiotherapeutic point of view, it would be preferable to irradiate brain metastases when they are small. Therefore, the cost increase compared with the conventional diagnostic procedure is justified by the therapeutic consequences: irradiation of the brain at an early stage, which may lead to a postponement of neurologic symptoms and a better quality of life.
Breast Cancer.
In 1 study, SRI helped to localize 75% (39/52) of primary breast cancers (49). Images of the axillae showed nonpalpable cancer-containing lymph nodes in 4 of 13 patients with subsequently histologically proven metastases. A special remark needs to be made with respect to the observation of bilateral and diffuse physiologic breast uptake in women with noncancerous breasts. This faint uptake is present in about 15% of patients 24 h after injection and is different from the more localized accumulation at the site of breast cancer. Currently, the basis for this finding is unknown. In follow-up testing after a mean of 2.5 y, SRI in 28 of the 37 patients who originally had somatostatin receptor–positive cancer was positive in 2 patients with clinically recognized metastases, as well as in 6 of the remaining 26 patients who were symptom free. SRI may be of value in selecting patients for clinical trials with somatostatin analogs or other medical treatments. Furthermore, SRI is sensitive for detecting recurrences of somatostatin receptor–positive breast cancer.
Malignant Lymphomas.
Although in many patients with non-Hodgkin's lymphoma (NHL) 1 or more lesions may be somatostatin receptor positive, in a substantial number of patients, lesions are not visualized (50). In addition, uptake of [111In-DTPA0]octreotide in lymphomas is lower compared with the uptake in neuroendocrine tumors (51,52). Therefore, the role for SRI in patients with NHL is limited. In 126 consecutive untreated patients with histologically proven Hodgkin's disease, the results of SRI were compared with physical and radiologic examinations (53), and SRI was positive in all patients. In 51% (44/87) of patients with stage I and II disease, SRI detected lymphoma localizations that were not seen after procedures of conventional staging. As a result, in 26 patients (30%), SRI resulted in an upgrading. In 18 stage I or stage II patients, the clinical stage was upgraded to stage III or stage IV. Therefore, SRI seems to be promising in the clinical staging and management of patients with Hodgkin's disease.
Melanoma.
In 1 study, positive octreotide scintigrams were reported in 16 of 19 patients with melanoma (54). The exact impact of SRI on staging and patient management remains to be determined.
Neuroblastomas and Pheochromocytomas.
In about 90% of patients with neuroblastoma and pheochromocytoma, SRI detected tumor deposits (55). Patients with neuroblastomas that were somatostatin receptor–positive in vitro had a longer survival compared with the somatostatin receptor–negative neuroblastomas (56). A drawback of SRI use for localization of these tumor types in the adrenal gland is the relatively high radioligand accumulation in the kidneys. MIBG scintigraphy is preferred for its localization in this region.
Cushing's Syndrome.
In a study of 19 patients with Cushing's syndrome, none of the pituitary adenomas of 8 patients with Cushing's syndrome or the adrenal adenoma of another patient could be visualized with SRI (57). In 8 of the other 10 patients, the primary ectopic corticotropin or corticotropin releasing hormone (CRH)–secreting tumors were successfully identified with SRI. Phlipponneau et al. (58) and Weiss et al. (59) have reported successful localizations of a 6-mm diameter corticotropin-secreting bronchial carcinoid and a 10-mm diameter corticotropin-secreting bronchial carcinoid with 1 lymph node metastasis, respectively. Therefore, SRI can be included as a diagnostic step in the procedure for identifying Cushing's syndrome with a suspected ectopic corticotropin or CRH-secreting tumor. Others, however, have concluded that, although SRI may be helpful in selected cases, it is not a significant advance over conventional imaging (60).
Brain Tumors.
SRI localizes meningiomas in virtually all patients (61,62). The majority of well-differentiated astrocytomas (grades I and II) are somatostatin receptor positive, whereas the undifferentiated glioblastomas (grade IV) are somatostatin receptor negative. An inverse relationship between the presence of somatostatin and epidermal growth factor receptors has been observed. In grade III astrocytomas, both receptors can be found (63). Astrocytomas have been visualized with SRI (62). A prerequisite for the localization with this radioligand is a locally open blood–brain barrier; particularly in the lower graded astrocytomas, this barrier may be unperturbed. Therefore, the grading of glia-derived brain tumors with SRI is not promising at this moment.
Other Diseases.
In vivo SRI is also helpful in several granulomatous and autoimmune diseases, such as sarcoidosis, tuberculosis, Wegener's granulomatosis, DeQuervain's thyroiditis, aspergillosis, Graves' hyperthyroidism and Graves' ophthalmopathy (64–66). It is expected that SRI may contribute to a more precise staging and a better evaluation of disease activity of several of these diseases (Fig. 7).

Bone scan (A) and SRI (B; lower 2 images run from pelvis to knees) in patient with Erdheim-Chester disease, a granulomatous disease related to histiocytosis. Skeletal disease involvement and soft-tissue chest involvement are visualized with SRI.
In a cross-sectional study in 46 patients with sarcoidosis, known mediastinal, hilar, and interstitial lesions were recognized in 36 of 37 patients (67). In addition, such pathology was found in 7 other patients who had chest radiographs that were normal. In 5 of these, SRI indicated interstitial disease. SRI was repeated in 13 patients. In 5 of 6 patients who had a chest-radiograph–monitored improvement of disease activity, SRI also showed a decrease of pathologic uptake. In 2 of 5 patients who had unchanged chest radiograph but had decreased serum angiotensin converting enzyme concentrations and improved lung function, a normalization on octreotide scintigrams was found. To determine the value of SRI in the follow-up of patients with sarcoidosis, a prospective longitudinal study will need to be performed.
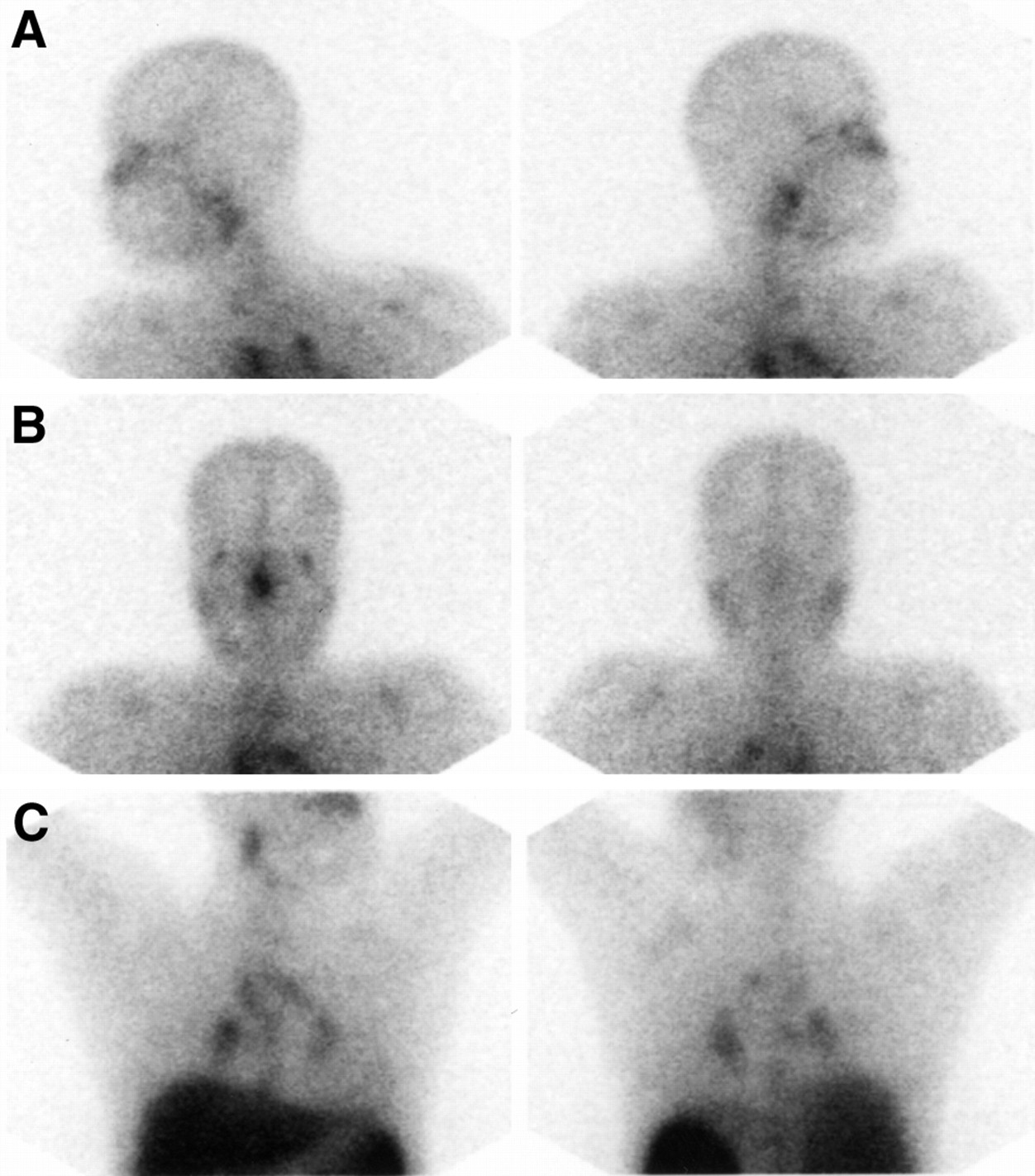
In summary, in virtually all patients with sarcoidosis, granulomas can be visualized. Uveitis may be the presenting symptom of sarcoidosis. In our experience, in patients with uveitis, octreotide scintigraphy cannot infrequently be of help because of the typical pattern of uptake in the mediastinum, lung hili, and parotid glands that can be seen in patients that eventually appear to have sarcoidosis, even when the chest radiograph or CT is normal (Fig. 8). Thus, octreotide scintigraphy can be used to diagnose a disease and can influence how to treat this type of disease.
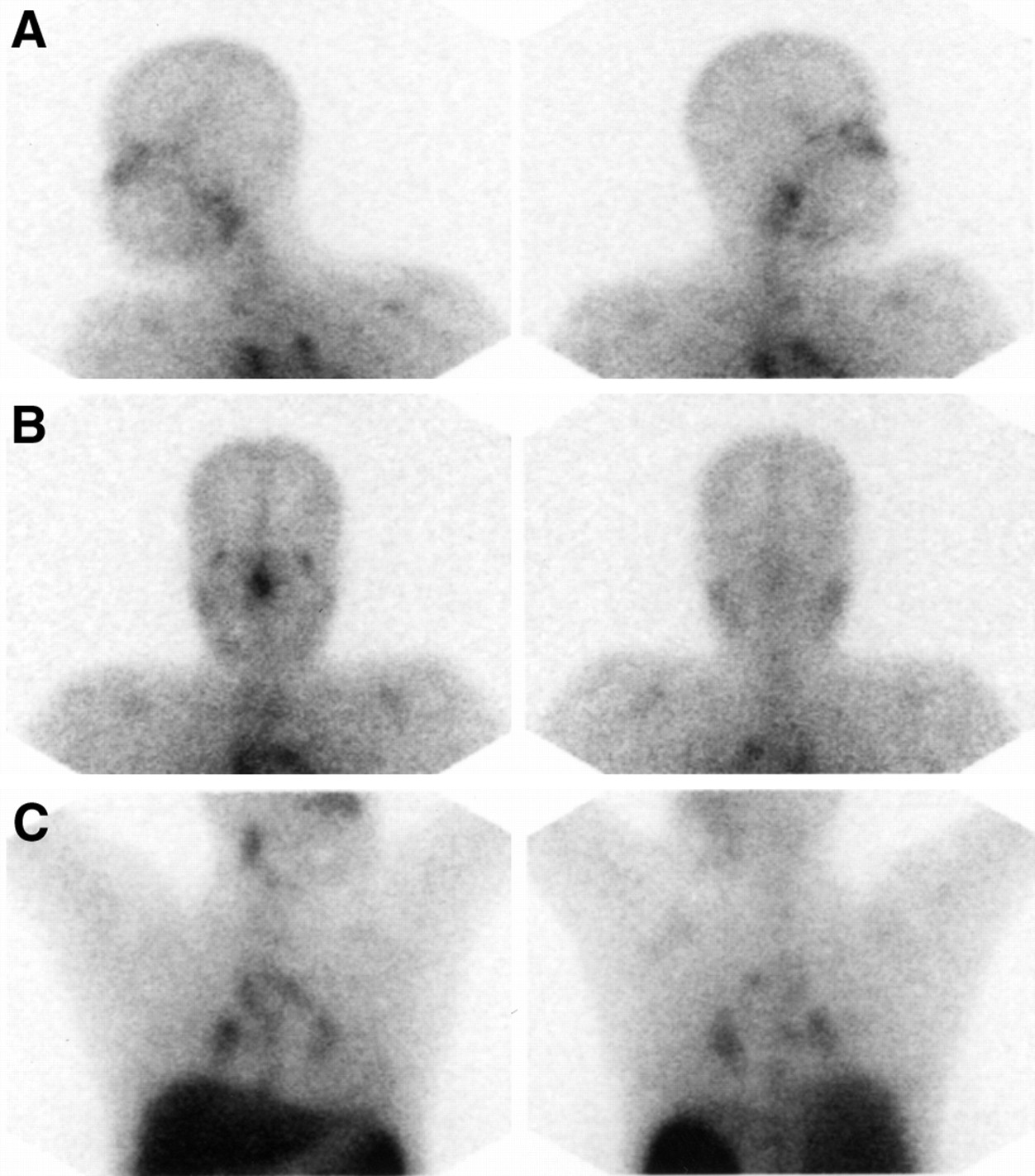
Lateral (A) and anterior and posterior views of head (B) and thorax (C) 24 h after injection in patient with sarcoidosis. There is typical pattern of uptake, resembling gallium scan, with uptake in salivary and lacrimal glands and nose, and in chest mediastinal and bihilar pathology is seen.
In Graves' hyperthyroidism, accumulation of radiolabeled octreotide in the thyroid gland is markedly increased and correlates with serum levels of free thyroxine and thyrotropin binding inhibiting immunoglobulins. In vitro studies showed that the follicular cells express somatostatin receptors in Graves' disease (68). In clinically active Graves' ophthalmopathy, the orbits show accumulation of radioactivity 4 h and 24 h after injection of [111In-DTPA0]octreotide (65). SPECT is required for a proper interpretation of orbital scintigraphy. There is also a correlation between orbital [111In-DTPA0]octreotide uptake and the Clinical Activity Score and Total Eye Score (65,69). In addition, uptake is high in clinically active disease but low if ophthalmopathy is inactive (66). The clinical value of SRI in Graves' disease has yet to be established. It is possible that this technique could help determine those patients with Graves' ophthalmopathy who might benefit from treatment with octreotide (66,69).
In summary, [111In-DTPA0]octreotide is a radiopharmaceutical with a great potential for the visualization of somatostatin receptor–positive tumors. The overall sensitivity of SRI to localize neuroendocrine tumors is high. In several neuroendocrine tumor types, inclusion of SRI in the localization or staging procedure may be very beneficial, in terms of cost effectiveness, patient management, or quality of life. The value of SRI in patients with other tumors, such as breast cancer or malignant lymphomas or in patients with granulomatous diseases, has to be established.
The application of radiolabeled peptides may be clinically useful in another way: after the injection of [111In-DTPA0]octreotide, tumor localizations can be seen by the surgeon by a probe that is used during the operation (70,71). This may be of particular value if small tumors with a high receptor density are present, such as in gastrinomas.
PEPTIDE RECEPTOR RADIONUCLIDE THERAPY
In patients with somatostatin receptor–positive pathology, SRI is useful if it can localize otherwise undetectable disease, or if it can be used for treatment selection (usually the choice between symptomatic treatment with somatostatin analogs or other medical treatment). In patients with known metastatic disease, however, in whom little or no treatment alternatives are available, SRI has a limited role. This situation changes if imaging has a sequel in treatment. The request for iodine scans of the thyroid would be a fraction of what it is if radioiodine treatment were not available. Analogously, the option of treatment with radiolabeled somatostatin analogs may become the impetus to SRI.
As the success of peptide receptor scintigraphy for tumor visualization became clear, the next logical step was to try to label these peptides with radionuclides emitting α or β particles, or Auger or conversion electrons, and to perform radiotherapy with these radiolabeled peptides.
[111In-DTPA0]Octreotide Therapy
Radionuclide therapy with high doses of [111In-DTPA0]octreotide has been performed in a clinical phase-1 study. In 30 patients with end-stage cancer (primarily neuroendocrine tumors), who received a cumulative dose of up to 74 GBq, the only side effects were a transient decline in platelet counts and lymphocyte subsets (72).
The typical dose per administration was 6000–7000 MBq 111In incorporated in 40–50 μg [DTPA0]octreotide. Doses were given with at least 2-wk intervals between administrations, and a total of 8 administrations were planned, with extensions in a few patients to about 20 administrations. Radionuclide therapy with [111In-DTPA0]octreotide was applied after witnessed informed consent by the patient and approval by the medical ethics committee of our hospital were obtained. The usual hematologic and chemical analyses of bone marrow, liver, kidney, and endocrine pancreatic (glucose or Hb A1c) function, performed before and between all administrations, served as parameters of possible side effects. Pituitary function (free T4, postmenopausal women: luteinizing and follicle-stimulating hormones; men: testosterone) was assessed before and 4 wk after the fourth and eighth administration of [111In-DTPA0]octreotide, and possible effects on (a) the endocrine activity of the tumors, their production of specific serum markers, or both; and (b) tumor size (measured by CT or MRI) were investigated. Pituitary–adrenal-axis function testing (metyrapone test) before and after 8 administrations as well as long-term follow up with 3–4-mo intervals were investigated when it was feasible.
Patients were also scanned 3 and 7 d after each administration of the radiotherapeutical dose. Uptakes decreased slowly or remained the same if the interval between the successive administrations was less than 1 mo. In patients who had 6 or more administrations of 6000–7000 MBq [111In-DTPA0]octreotide with intervals of maximally 1 mo between administrations, uptake in the tumor was still clearly visible after the last administration. Typical radiation doses to tissues with doses of 6000–7000 MBq [111In-DTPA0]octreotide are: kidneys, 300–1400 cGy (depending on the relative biologic effectiveness [RBE, 1–20] for Auger electrons); spleen, 200 cGy; liver, 50 cGy; bone marrow, 13 cGy (target organ for gamma photons); thyroid gland, 25 cGy; and pituitary gland, 70 cGy. The critical organs are kidneys and spleen. With these doses, the estimated tumor radiation doses for a 10-g tumor (assumptions: 1% uptake; effective half-life is the physical half-life) are 1700 and 6700 cGy (RBE for Auger electrons 1 and 20, respectively) and for a 100-g tumor (1% uptake), 250 and 750 cGy, respectively.
Of the 21 patients who received a cumulative dose of more than 20 GBq, a reduction in tumor size was found in 6 patients and stable disease in 8 others. There was a tendency toward better results in patients with a high tumor uptake (72). The observed responses to this radionuclide therapy agree with internalization of [111In-DTPA0]octreotide into tumor cells and with an antiproliferative effect that has also been shown in other studies (73,74).
[90Y-DOTA0,Tyr3]Octreotide Therapy
111In-coupled peptides, because of the small particle range of the Auger electrons and, therefore, short tissue penetration, may not always be the ideal radiopharmaceuticals for radionuclide therapy. Recently, another somatostatin analog, [DOTA0,Tyr3]octreotide (DOTATOC) was developed, to which the high-energy β emitter, 90Y, can be linked in a very stable manner (75). In studies with humans and rats, the uptake of radioactivity in known somatostatin receptor–positive organs and tumors was higher after 111In-DOTATOC than after [111In-DTPA0]octreotide (76,77). Recent studies (75,78) showed favorable results of 90Y-DOTATOC treatment. In addition, a study comparing both the uptake of 111In-DOTATOC and 86Y-DOTATOC as well as the effects of treatment with 90Y-DOTATOC in the same patients is underway (79). There is 1 problem in radionuclide therapy that is caused by the high uptake of radioactivity in the kidneys: small peptides in the blood plasma are filtered through the glomerular capillaries in the kidneys and subsequently reabsorbed by and retained in the proximal tubular cells, thereby reducing the scintigraphic sensitivity for detection of small tumors in the perirenal region and the possibilities for radionuclide therapy. We showed that the renal uptake of [111In-DTPA0]octreotide in rats could be reduced by positively charged amino acids (e.g., with about 50% by single intravenous administration of 400 mg/kg l- or d-lysine (80). Therefore, during PRRT with 90Y-DOTATOC, an infusion containing the positively charged amino acids l-lysine and l-arginine is given during and after the infusion of the radiopharmaceutical to reduce the kidney uptake. A very recent analysis of the results of 90Y-DOTATOC treatment in a phase 1 trial in 22 patients with end-stage progressive cancer showed a partial tumor response in 2, a minor response in 3, and stable disease in 10 patients (79). A phase 2 trial of 90Y-DOTATOC treatment in patients with SCLC and breast cancer is expected to start soon.
Preclinical studies have shown radiotherapeutic effects of 90Y-DOTATOC in the rat CA20948 tumor model (81). Tumor growth inhibition was found after treatment of CA20948 tumor-bearing rats with 370 MBq/kg of 90Y-DOTATOC, and complete tumor reduction was observed in 5 of 7 rats (81). We compared the radiotherapeutic effect of different doses of 90Y-DOTATOC or [111In-DTPA]octreotide in rats who had smaller (≤1 cm2) versus larger (≥8 cm2) pancreatic CA20948 tumors (unpublished data). For [111In-DTPA]octreotide a dose–response relationship was found, primarily in rats that had small tumors to 25%–50% complete response (CR). In rats that had large tumors, only 100% partial response (PR) was achieved after the highest dose (3 × 370 MBq) but no CR was found. After 370 MBq 90Y-DOTATOC, 50% CR was reached for the small tumors and only PR (100%) in the large tumors. These studies underscore the feasibility of radionuclide therapy with both 111In- and 90Y-labeled analogs and the importance of starting radionuclide therapy as early as possible.
Radiolabeled peptides are new radioligands that are not only for staging of (recurrence of) neuroendocrine and other tumors. The future application of radiolableled peptides in tumor scintigraphy may be aimed at their in vivo use as prognostic predictors and not necessarily for localization per se. Peptide receptor radionuclide therapy using radionuclides with appropriate particle ranges may become a new treatment modality. One might consider the use of radiolabeled somatostatin analogs, first, in an adjuvant setting after surgery of somatostatin receptor–positive tumors to eradicate occult metastases and, second, for cancer treatment at a later stage.
Footnotes
Received Mar. 27, 2000; revision accepted Jun. 13, 2000.
For correspondence or reprints contact: Eric P. Krenning, MD, PhD, Department of Nuclear Medicine, University Hospital Rotterdam, 3015 GD Rotterdam, The Netherlands.
*NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ARTICLE ON THE SNM WEB SITE (http://www.snm.org) UNTIL APRIL 2001.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Somatostatin Receptor Imaging and Theranostics: Current Practice and Future Prospects
- Multiple Endocrine Neoplasia Type 1: A Case Report With Review of Imaging Findings
- Tailoring Peptidomimetics for Targeting Protein-Protein Interactions
- Radiopeptide Imaging and Therapy in Europe
- Clinical and imaging follow-up after exhaustive liver resection of endocrine metastases: a 15-year monocentric experience
- Bone Metastases in Patients with Neuroendocrine Tumor: 68Ga-DOTA-Tyr3-Octreotide PET in Comparison to CT and Bone Scintigraphy
- Highly Efficient In Vivo Agonist-Induced Internalization of sst2 Receptors in Somatostatin Target Tissues
- 111In-LLP2A-DOTA Polyethylene Glycol-Targeting {alpha}4{beta}1 Integrin: Comparative Pharmacokinetics for Imaging and Therapy of Lymphoid Malignancies
- 68Ga-DOTA-Tyr3-Octreotide PET in Neuroendocrine Tumors: Comparison with Somatostatin Receptor Scintigraphy and CT
- Androgen-Dependent Expression of the Gastrin-Releasing Peptide Receptor in Human Prostate Tumor Xenografts
- Dosimetry in Peptide Radionuclide Receptor Therapy: A Review
- In Vitro and in Vivo Antitumor Effects of Cytotoxic Camptothecin-Bombesin Conjugates Are Mediated by Specific Interaction with Cellular Bombesin Receptors
- Internalization of sst2, sst3, and sst5 Receptors: Effects of Somatostatin Agonists and Antagonists
- Combined Molecular Targeting for Cancer Therapy: A New Paradigm in Need of Molecular Imaging
- Megalin Is Essential for Renal Proximal Tubule Reabsorption of 111In-DTPA-Octreotide
- Candidates for Peptide Receptor Radiotherapy Today and in the Future
- High Expression of Neuropeptide Y Receptors in Tumors of the Human Adrenal Gland and Extra-Adrenal Paraganglia
- Evaluation of the solitary pulmonary nodule: clinical management, role of CT and nuclear medicine
- Cellular detection of sst2A receptors in human gastrointestinal tissue
- Radiation Therapy of Small Cell Lung Cancer with 177Lu-DOTA-Tyr3-Octreotate in an Animal Model
- Quality of Life in Patients With Gastroenteropancreatic Tumors Treated With [177Lu-DOTA0,Tyr3]octreotate
- Development of High Affinity Camptothecin-Bombesin Conjugates That Have Targeted Cytotoxicity for Bombesin Receptor-containing Tumor Cells
- In Vitro and In Vivo Evaluation of 111In-DTPAGlu-G-CCK8 for Cholecystokinin-B Receptor Imaging
- Somatostatin Receptors in Malignant Lymphomas: Targets for Radiotherapy?
- Effect of Molecular Size of Pegylated Peptide on the Pharmacokinetics and Tumor Targeting in Lymphoma-Bearing Mice
- An Intrapatient Comparison of 99mTc-EDDA/HYNIC-TOC with 111In-DTPA-Octreotide for Diagnosis of Somatostatin Receptor-Expressing Tumors
- Specific and High-Level Targeting of Radiolabeled Octreotide Analogues to Human Medulloblastoma Xenografts
- Preclinical Comparison of 111In-Labeled DTPA- or DOTA-Bombesin Analogs for Receptor-Targeted Scintigraphy and Radionuclide Therapy
- New Advances in Peptide Receptor Radionuclide Therapy
- Quantitative Evaluation of Somatostatin Receptor Subtype 2 Expression in Sporadic Colorectal Tumor and in the Corresponding Normal Mucosa