


Abstract
In routine PET, a 10- to 20-min transmission scan with a rotating 68Ge source is commonly obtained for attenuation correction (AC). AC is time-consuming using this procedure and could considerably be shortened by instead using a rapid CT scan. Our aim was to evaluate the feasibility of CT AC in quantitative myocardial perfusion PET using a hybrid PET/CT scanner. Methods: 13N-labeled NH3 and PET were used to measure myocardial blood flow (MBF) (mL/min/g) at rest and during standard adenosine stress. In group 1 (n = 7), CT scans (0.5 s) of the heart area with different tube currents (10, 40, 80, and 120 mA) were compared with a standard 68Ge transmission (20 min) and with no AC. In group 2 (n = 3), the repeatability of 8 consecutive CT scans at a tube current of 10 mA was assessed. In group 3 (n = 4), emission was preceded and followed by 3 CT scans (10 mA) and 1 68Ge scan for each patient. For reconstruction, filtered backprojection (FBP) was compared with iterative reconstruction (IT). Results: For group 1, no significant difference in mean MBF for resting and hyperemic scans was found when emission reconstructed with 68Ge AC was compared with emission reconstructed with CT AC at any of the different tube currents. Only emission without any correction differed significantly from 68Ge AC. For group 2, repeated measurements revealed a coefficient of variance ranging from 2% to 5% and from 2% to 6% at rest and at stress, respectively. For group 3, similar reproducibility coefficients (RC) for MBF were obtained when 68Ge ACFBP was compared with 68Ge ACIT (RC = 0.218) and when CT ACFBP was compared with CT ACIT (RC = 0.227). Even better reproducibility (lower RC) was found when 68Ge ACFBP was compared with CT ACFBP (RC = 0.130) and when 68Ge ACIT was compared with CT ACIT (RC = 0.146). Conclusion: Our study shows that for the assessment of qualitative and quantitative MBF with a hybrid PET/CT scanner, the use of CT AC (with a tube current of 10 mA) instead of 68Ge AC provides accurate results.
PET is currently the accepted gold standard in noninvasive imaging of coronary perfusion in patients with suspected or known coronary artery disease (CAD). Its main advantage over SPECT is its better spatial resolution and the fact that perfusion values can be not only estimated qualitatively but calculated quantitatively, using a dynamic scanning protocol with appropriate tracers such as 13N-labeled NH3 or 15O-labeled H2O (1). To accurately quantify tracer uptake, photon attenuation correction (AC) is crucial. At present, a rotating 68Ge source is commonly used for photon AC in oncology studies and in cardiac viability studies and perfusion scanning. 68Ge sources have only a low photon flux, which necessitates long acquisition times of up to 20 min (2,3), although with current methods transmission times of much less than 20 min can be used. The result is an increased chance of motion artifacts and poor anatomic image quality, as well as patient discomfort and economic losses because of lower patient throughput (4). Introduction of hybrid PET/CT systems using the CT scan for AC is expected to improve these limitations, since a high-end CT scanner can acquire images with a far higher spatial resolution in a much shorter time than can a conventional 68Ge transmission scan. Our group has already shown the feasibility of obtaining adequate photon AC with a CT scan in static 18F-FDG PET scans (5,6). However, it remains unclear whether a CT scan provides adequate photon AC for calculating myocardial blood flow (MBF) in a standardized non–electrocardiography (ECG)-gated dynamic cardiac perfusion PET scan using 13N-labeled NH3. Because of physiologic cardiac motion and the short duration of a CT scan of the heart (3.9 s), compared with a conventional 68Ge transmission scan of the heart, the need for ECG gating of the heart cycle has to be investigated. The required CT tube currents must also be considered, since high currents mean increased radiation to the patient. For reconstruction of emission data of dynamic cardiac PET, filtered backprojection (FBP) is a widely accepted standard, but iterativereconstruction (IT) (i.e., ordered-subset expectation maximization [OSEM]) is considered an established alternative, particularly in static PET (7). Whether this alternative also applies to CT AC in dynamic cardiac PET remains unclear.
The aim of the present study was, therefore, to determine the lowest possible adequate CT energy dose for CT AC, compare the accuracy and repeatability of nongated CT AC and routine 68Ge AC for dynamic cardiac perfusion measurements, and find the most appropriate reconstruction parameters.
MATERIALS AND METHODS
Study Population
Fourteen consecutive patients (12 men and 2 women; mean age, 62 y; range, 45–76 y) were included in the study. All participants had angiographically documented CAD defined as one or more vessels with >50% diameter reduction (3 patients had 1-vessel disease, 1 had 2-vessel disease, and 10 had 3-vessel disease). All patients were clinically stable, and the scans were obtained primarily for clinical purposes. According to clinical indications, a perfusion scan was obtained for all patients at rest and was repeated for 7 patients during adenosine stress. The study was approved by the local ethics committee, and all participants gave informed written consent.
Study Design
In group 1 (n = 7), emission was preceded by 4 CT AC scans with different CT tube currents (10, 40, 80, and 120 mA) and was followed by 1 68Ge AC scan. In 4 patients of this group, MBF was also assessed during standard pharmacologic stress, that is, a 7-min infusion of adenosine at 0.14 mg/min/kg of body weight (8,9).
In group 2 (n = 3), each emission (resting and hyperemic MBF) was preceded by 8 CT AC scans using a constant CT tube current of 10 mA. The CT scans were obtained at random times during the heart cycle to test the repeatability of CT AC regardless of the motion of the beating heart.
In group 3 (n = 4), emission (resting MBF only) was preceded and followed by 3 CT AC scans at a CT tube current of 10 mA each. Additionally, 2 68Ge AC scans were obtained, one before and another after emission for each patient. These scans were used to compare CT AC and 68Ge AC with different reconstruction algorithms.
Image Acquisition
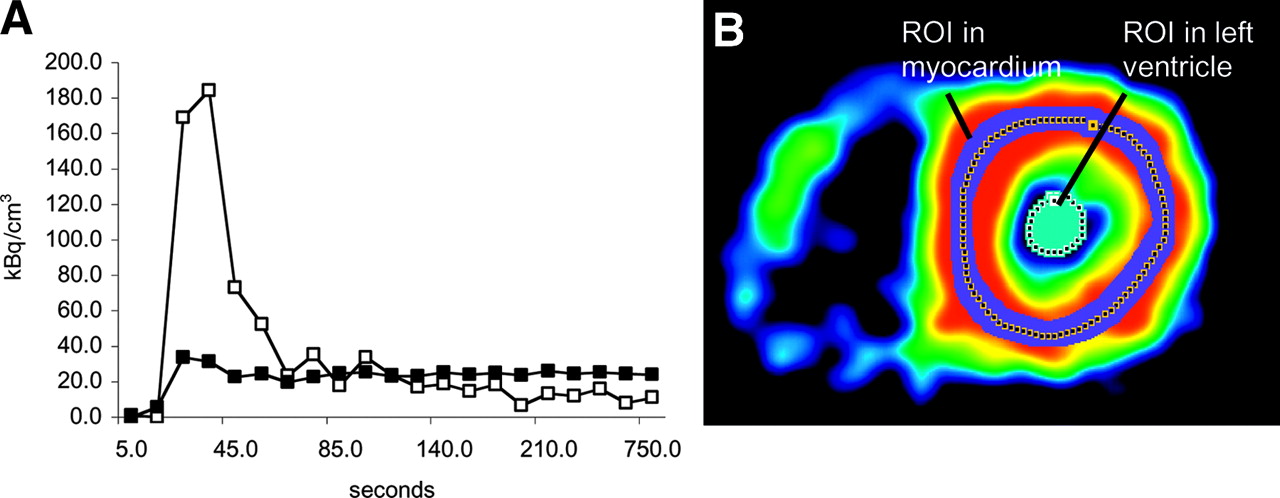
Imaging was performed on a Discovery LS PET/CT scanner (General Electric Medical Systems). This scanner integrates the Advance PET system, with a 7-mm reconstructed in-plane resolution, and a 4-row helical CT scanner (LightSpeed Plus). First, a CT scout scan providing an anteroposterior and lateral view of the chest area was acquired. This scan was used to localize the field of view for the following emission and transmission scans. All patients received a 700- to 900-MBq injection of 13N-labeled NH3 into a peripheral vein before the start of serial transaxial tomographic imaging of the heart. Ammonia was injected during 10 s with a dynamic imaging sequence, which was previously designed to get a sampling rate sufficient to measure the tracer bolus (10) and consisted of nine 10-s, six 15-s, three 20-s, two 30-s, and one 900-s frames (Fig. 1). Transmission data for photon AC were acquired in a 20-min transmission scan with external 68Ge and in a nongated CT transmission scan of the chest area, using the following parameters: scan length, 15 cm; rotation time, 0.5 s; total scan time, 3.9 s; 140 kV; and slice thickness, 5 mm. AC was performed using the standard reconstruction software of the Discovery LS. For CT-based AC, this software performs a bilinear conversion of the CT Hounsfield units into linear attenuation coefficients at the PET energy, as outlined previously in detail (5). To achieve accurate image fusion, the same landmarks were used for repeated scans.
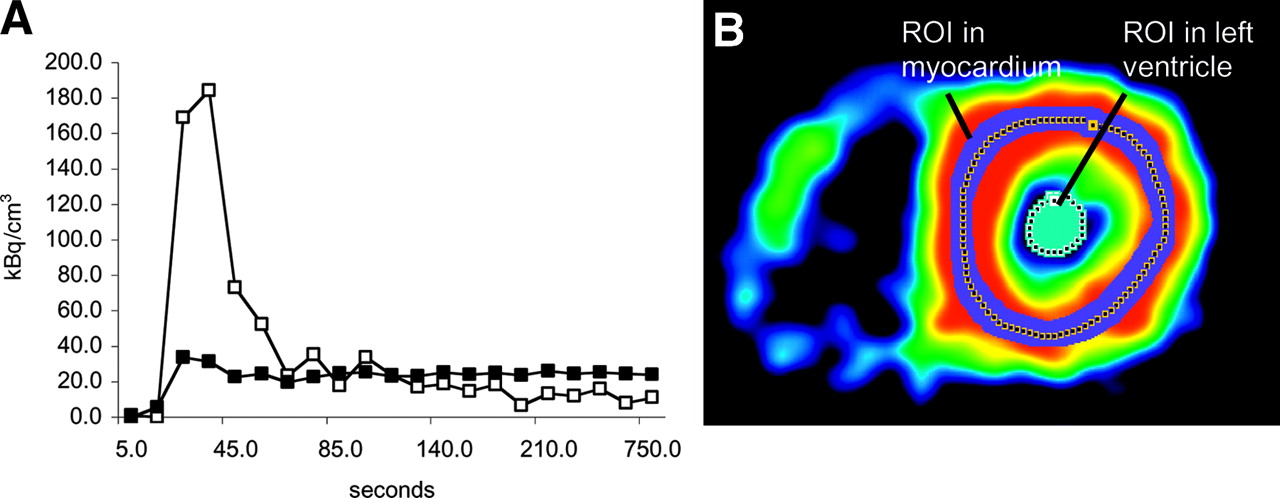
(A) Time–activity curves of left ventricular blood pool (□) (input function) and left ventricular myocardium (▪). (B) ROIs for left ventricular cavity and myocardial tissue drawn on a short-axis cut of the heart.
Image Processing
For groups 1 and 2, emission data were reconstructed with each corresponding transmission scan (CT or 68Ge) using either OSEM IT for CT ACIT (2 iterations, 28 subsets, 3.49-mm postfilter, 2.50-mm loop filter) or FBP for 68Ge ACFBP (Hanning filter, 5.0-mm cutoff). For group 3, emission data were reconstructed with all corresponding CT- and 68Ge-transmission scans using FBP and IT, respectively. Reconstructed images were then transferred to a model 2200 personal computer (Transtec Computer AG) and analyzed with the PMOD software package (PMOD Technologies GmbH) as previously reported (9). Regions of interest (ROIs) were drawn semiautomatically using a centerline within the myocardium in the short-axis projection. The junctions of the right and left ventricles were marked to indicate the septum. The left ventricular free wall was then subdivided geometrically into 3 segments of the same size (anterior, lateral, and inferior). An ROI was drawn in each segment and in the left (for input function) and right (for septal spillover correction) ventricular blood pool on the 900-s frames. The same ROIs were used for the CT AC and the 68Ge AC datasets. MBF was estimated by model fitting of the myocardial time–activity curves (11). Partial volume and spillover (both accounting for the resolution distortion) were corrected using the method developed (12) and validated (13) by Hutchins et al. and previously used by our group (10). Briefly, the relationship between the measured PET count in a region (CPET) and the true count in myocardium (Cm) and in arterial blood (Ca) was modeled as follows: CPET(t) = FaCa(t) + (1 − Fa)Cm(t), where Fa is the fractional contribution of the blood pool to measured PET counts in a region and is dependent on the placement of the region, the resolution of the camera, and the movement of the myocardium. The ROIs were positioned to contain only myocardial tissue and blood, thus allowing overlap of tissue with blood (Fig. 1). Because the contribution of the myocardium to total regional counts decreases with an increasing blood-pool fraction, Cm is multiplied by (1 − Fa). This strategy of spillover correction seems to be the most appropriate in view of the potential heterogeneity of myocardial thickness in CAD patients. The model includes one tissue compartment and accounts for signal contributions from the left and right ventricles. An iterative Levenberg–Marquardt algorithm was used for unweighted least squares fitting of the model curve to the segmental time–activity curves. MBF is given in mL/min/g of tissue.
Visual Assessment
We studied the effect of the different attenuation approaches on regional 13N-labeled NH3 concentration when only static images were obtained. For this purpose, we qualitatively assessed the 900-s frames of all group-1 resting and hyperemic perfusion scans reconstructed with 68Ge AC as well as with the lowest (10 mA) and the highest (120 mA) CT tube current AC. The 16-segment model was applied (14), and each segment was graded as normal or abnormal by an experienced reader who was unaware of the study condition.
Statistical Analysis
Values are given as mean ± SD. MBF values were compared using ANOVA for repeated measurements; P values of <0.05 were considered significant. Agreement between 2 methods was estimated according to the method of Bland and Altman (15) by reporting a reproducibility coefficient (RC) of 1.96 × the SD as absolute values and as a percentage. The coefficient of variation was reported as a percentage. For the visual assessment, a χ2 test was performed and the κ-value was calculated.
RESULTS
Group 1
No significant differences in mean MBF (mL/min/g) for resting and hyperemic scans were found when emission reconstructed with 68Ge AC was compared with emission reconstructed with CT AC of various tube currents: 0.80 ± 0.24 (68Ge AC), 0.83 ± 0.32 (CT AC, 10 mA), 0.78 ± 0.30 (CT AC, 40 mA), 0.82 ± 0.30 (CT AC, 80 mA), and 0.75 ± 0.32 (CT AC, 120 mA) (P = not statistically significant). Mean MBF derived from uncorrected emission data (1.62 ± 1.06) was significantly different from all corrected data (P < 0.005) (Fig. 2). The quality of the CT scan with 10 mA was clearly worse than that of the CT scan with 80 or 120 mA. However, after degradation with a gaussian filter of 8 mm in full width at half maximum, both scans looked similar and demonstrated still higher resolution than the 68Ge transmission scan. This finding is in agreement with the findings of our previous study (6) that extensively evaluated the impact of lowering the CT tube current on CT AC. The applied acquisition parameters in this setting lead to an estimated effective irradiation dose of 0.05 mSv for a 10-mA CT scan (dose length product = 7.57 mGy × cm), compared with 0.38 mSv for an 80-mA CT scan (dose length product = 60.6 mGy × cm).
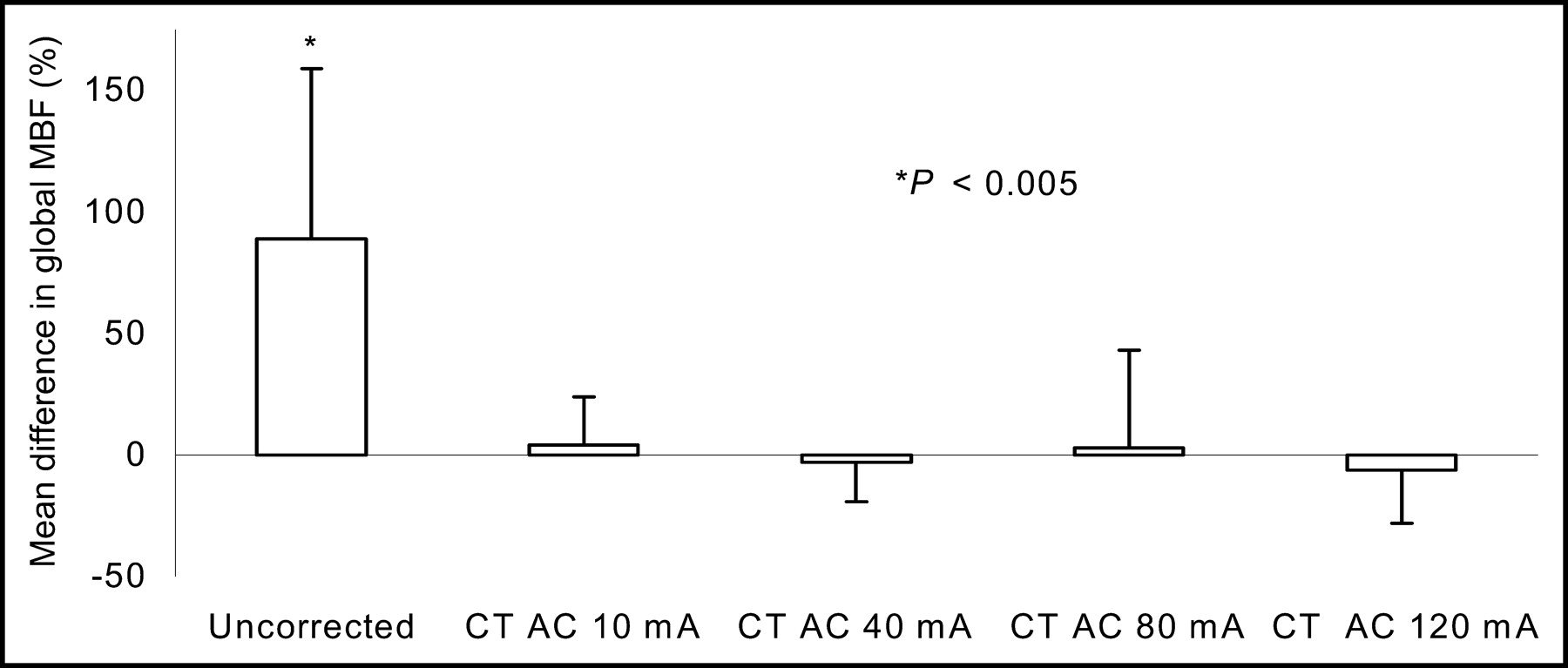
Percentage difference of CT AC at different tube currents vs. standard 68Ge AC.
Visual assessment of the 900-s scan revealed a highly significant χ2 value (P < 0.001) for comparison of AC with 68Ge and 10 mA, AC with 68Ge and 120 mA, and AC with 10 mA and 120 mA. The respective agreement percentages and κ-values were 90% and 0.781, 94% and 0.869, and 94% and 0.871.
Group 2
Global MBF and coefficients of variance are shown in Figure 3. Regional values are given in Table 1. Coronary angiography revealed severe, moderate, and mild CAD in patients 1, 2, and 3, respectively, as reflected by the small, intermediate, and large differences between resting and hyperemic MBF in each patient.

Repeated MBF measurements using CT AC (10 mA). Coefficients of variance (COV) are given as percentages.
Global MBF and COV at Rest and During Stress
Group 3
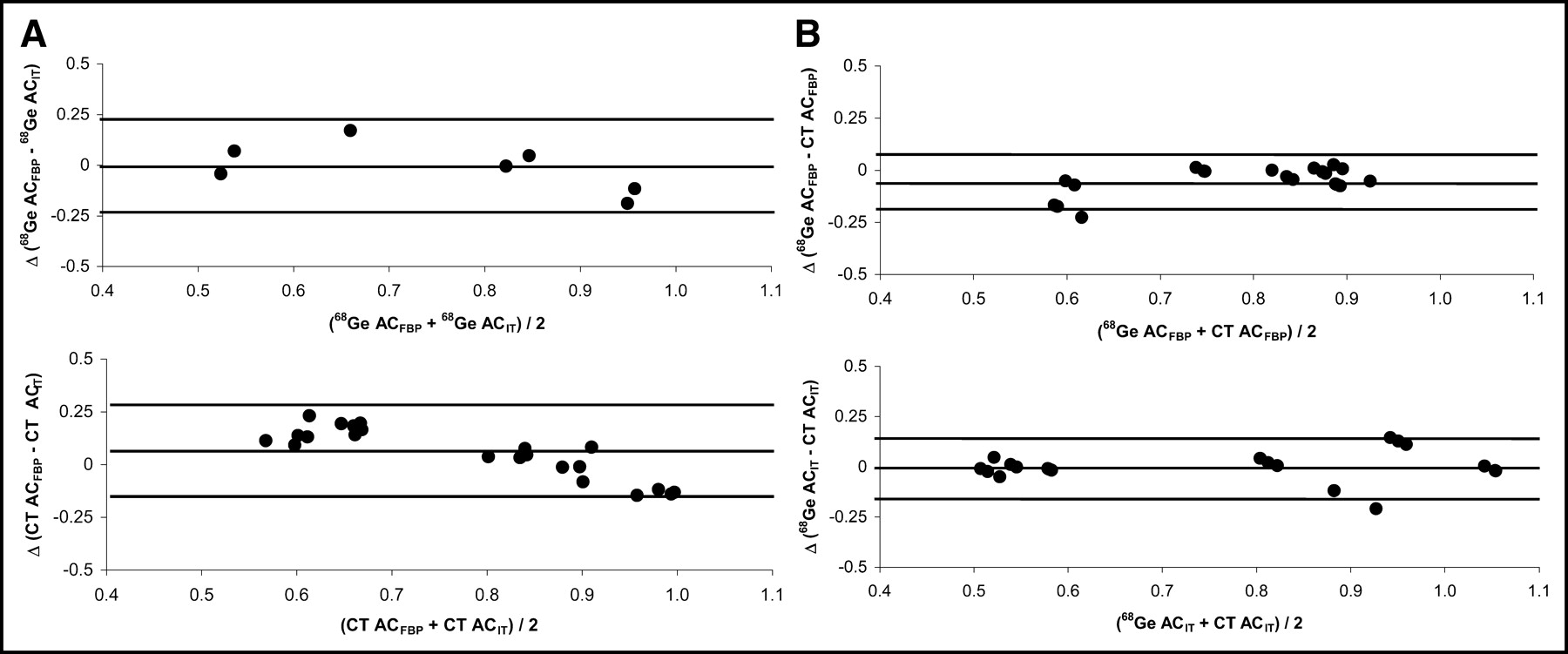
Similar RCs for MBF were found when 68Ge ACFBP was compared with 68Ge ACIT (RC = 0.218) and when CT ACFBP was compared with CT ACIT (RC = 0.227) (Fig. 4A). Similar RCs for MBF were also found when 68Ge ACFBP was compared with CT ACFBP (RC = 0.130) and when 68Ge ACIT was compared with CT ACIT (RC = 0.146) (Fig. 4B).

Bland–Altman plots of MBF (mL/min/g) in group 3. (A) Comparison of reconstruction algorithms: FBP vs. IT. Top graph shows 68Ge AC (RC = 0.22 mL/min/g [29%]). Bottom graph shows CT AC (RC = 0.23 mL/min/g [29%]). (B) Comparison of AC sources: 68Ge vs. CT. Top graph shows FBP (RC = 0.13 mL/min/g [17%]). Bottom graph shows IT (RC = 0.15 mL/min/g [19%]).
DISCUSSION
The main findings of our study were that AC with low-dose CT for dynamic 13NH3 myocardial perfusion scanning is feasible and provides reliable and repeatable global and regional MBF results in patients with CAD. For CT AC, ECG gating seems not mandatory, as nongated CT scans provide repeatable results. CT AC provides results that are highly comparable to those obtained using 68Ge AC if the same reconstruction algorithms are used. Furthermore, the high agreement in visual assessment of defects in the 900-s scans confirms that these results also apply when only static images are obtained and regional myocardial 13NH3 activity concentrations are determined.
The results for group 1 showed that different tube currents for CT AC do not lead to significant differences in MBF and that CT AC with each tube current is highly comparable to 68Ge AC. Therefore, a 10-mA CT scan seems sufficient for CT AC. These results are in line with those of Kamel et al. (6), who found that lowering of the CT tube current to 10 mA did not affect tumor 18F-FDG uptake or detectable lesion size. High currents improve image quality but also increase radiation dose to the patient. Because high-quality anatomic information is not mandatory in dynamic PET of myocardial perfusion, there is no need to elevate the radiation dose for this purpose. The CT current could possibly have been reduced even more without compromising the attenuation map. For technical reasons, however, our system did not allow this option. Because further current reduction may be possible in the future without compromising the accuracy of the AC, but possibly reducing image quality, we recommend that the ROI for quantification continue to be drawn directly on images obtained from the 900-s frame of the PET scan.
Registration of a 68Ge AC scan of the beating heart over an interval of up to 20 min results in blurring of all cardiac cycles. Additional body-motion artifacts often further decrease image quality, because many patients, particularly those with back pain or with congestive heart failure and dyspnea, find it challenging to remain still throughout a PET examination.
In group 2, however, we found highly reproducible MBF values, as shown by the low coefficients of variance (Table 1), for the 8 consecutive nongated CT attenuation scans at a tube current of 10 mA. Because the scan duration is 3.9 s, the relative contribution of the systolic and diastolic phases may approximate one third to two thirds—similar to the 20-min 68Ge AC scan but not exactly predictable for each slice. The substantially shortened acquisition time of the transmission scan with CT AC may have reduced the likelihood of noncardiac motion artifacts and thus contributed to the excellent repeatability of the MBF results, suggesting no need for ECG gating for CT AC. Determining whether repeatability could be further improved through use of breathing protocols, as suggested by Goerres et al. for patients with lung cancer (16), was beyond the scope of the present study.
MBF values calculated using 10-mA CT AC showed excellent agreement with those calculated using 68Ge AC (Fig. 4) as long as the same reconstruction algorithm, that is, either FBP or IT, was used for both AC scans. Differences in MBF values were greater between the 2 reconstruction algorithms (FBP and IT) than between the 2 methods of AC (68Ge AC and CT AC) (Fig. 4). Thus, 68Ge AC and CT AC are interchangeable, but the same reconstruction algorithm must always be chosen. We use FBP because it has been established at our institution as the standard reconstruction algorithm in those experimental animal studies that have validated myocardial PET perfusion against the microsphere gold standard (17–19).
Our results may have implications for future cardiac PET/CT protocols. First, for tracers with a short half-life, such as 82Rb or H215O, a short CT AC will increase patient throughput. Second, combined assessment of myocardial perfusion and coronary anatomy with hybrid PET/CT will allow use of the CT scan for AC of the PET scan, improving the efficiency of the scan protocol.
CONCLUSION
Our study shows that for the assessment of qualitative and quantitative MBF with a hybrid PET/CT scanner, the use of CT AC, with a tube current of 10 mA, instead of 68Ge AC provides accurate results.
Acknowledgments
This study was supported by an SNSF Professorship grant from the Swiss National Science Foundation, by a grant from EMDO STIFTUNG Zurich and Radiumfonds Zürich, and by General Electric Medical Systems.
Footnotes
Received Sep. 8, 2003; revision accepted Nov. 21, 2003.
For correspondence or reprints contact: Philipp A. Kaufmann, MD, Nuclear Cardiology, Cardiovascular Center, University Hospital C NUK 32, Raemistrasse 100, CH-8091 Zurich, Switzerland.
E-mail: pak{at}usz.ch
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Absolute Myocardial Blood Flow and Flow Reserve Assessed by Gated SPECT with Cadmium-Zinc-Telluride Detectors Using 99mTc-Tetrofosmin: Head-to-Head Comparison with 13N-Ammonia PET
- The Effect of Misregistration Between CT-Attenuation and PET-Emission Images in 13N-Ammonia Myocardial PET/CT
- SNMMI/ASNC/SCCT Guideline for Cardiac SPECT/CT and PET/CT 1.0
- Hybrid PET/MR Imaging of the Heart: Potential, Initial Experiences, and Future Prospects
- Evaluation of a Mitochondrial Voltage Sensor, (18F-Fluoropentyl)Triphenylphosphonium Cation, in a Rat Myocardial Infarction Model
- Diagnostic Value of 13N-Ammonia Myocardial Perfusion PET: Added Value of Myocardial Flow Reserve
- Structural Abnormalities of the Coronary Arterial Wall--in Addition to Luminal Narrowing--Affect Myocardial Blood Flow Reserve
- Improved Outcome Prediction by SPECT Myocardial Perfusion Imaging After CT Attenuation Correction
- Agreement of Visual Estimation of Coronary Artery Calcium From Low-Dose CT Attenuation Correction Scans in Hybrid PET/CT and SPECT/CT With Standard Agatston Score
- Validation of CT Attenuation Correction for High-Speed Myocardial Perfusion Imaging Using a Novel Cadmium-Zinc-Telluride Detector Technique
- Decreased Perfusion in the Lateral Wall of the Left Ventricle in PET/CT Studies with 13N-Ammonia: Evaluation in Healthy Adults
- Long-Term Prognostic Value of 13N-Ammonia Myocardial Perfusion Positron Emission Tomography: Added Value of Coronary Flow Reserve
- Comparison of Myocardial Perfusion 82Rb PET Performed with CT- and Transmission CT-Based Attenuation Correction
- SPECT/CT
- Reducing Radiation Dose in Rest-Stress Cardiac PET/CT by Single Poststress Cine CT for Attenuation Correction: Quantitative Validation
- Absolute Quantification of Myocardial Blood Flow with 13N-Ammonia and 3-Dimensional PET
- Radiation Dose to Patients From Cardiac Diagnostic Imaging
- Added Value of Coronary Artery Calcium Score as an Adjunct to Gated SPECT for the Evaluation of Coronary Artery Disease in an Intermediate-Risk Population
- Frequent Diagnostic Errors in Cardiac PET/CT Due to Misregistration of CT Attenuation and Emission PET Images: A Definitive Analysis of Causes, Consequences, and Corrections
- Respiration-Averaged CT for Attenuation Correction in Canine Cardiac PET/CT
- PET/CT Attenuation Correction: Breathing Lessons
- Cardiac Image Fusion from Stand-Alone SPECT and CT: Clinical Experience
- Artifacts from Misaligned CT in Cardiac Perfusion PET/CT Studies: Frequency, Effects, and Potential Solutions
- Noninvasive Characterization of Myocardial Molecular Interventions by Integrated Positron Emission Tomography and Computed Tomography
- Comparison of 64-Slice CT with Gated SPECT for Evaluation of Left Ventricular Function
- 18F-Choline Images Murine Atherosclerotic Plaques Ex Vivo
- Caffeine Decreases Exercise-Induced Myocardial Flow Reserve
- PET/CT: Challenge for Nuclear Cardiology
- Novel Doppler Assessment of Intracoronary Volumetric Flow Reserve: Validation Against PET in Patients With or Without Flow-Dependent Vasodilation
- Integrated PET/CT for the Assessment of Coronary Artery Disease: A Feasibility Study
- Myocardial Blood Flow Measurement by PET: Technical Aspects and Clinical Applications
- {beta}-Adrenergic Blockade and Myocardial Perfusion in Coronary Artery Disease: Differential Effects in Stenotic Versus Remote Myocardial Segments