


Abstract
The aim of this study was to validate attenuation correction (AC) using low-dose standard CT for myocardial perfusion imaging (MPI) on a novel ultra fast γ-camera with cadmium-zinc-telluride (CZT) detector technology. Methods: Sixty-six patients (body mass index ± SD, 27.2 ± 3.5 kg/m2; range, 19.1–36.0 kg/m2) underwent a 1-d 99mTc-tetrofosmin adenosine stress–rest imaging protocol with 15-min acquisitions on a standard dual-head SPECT camera. All scans were repeated within minutes on the CZT camera, with 3-min acquisitions for stress (low dose) and 2-min acquisitions for rest (high dose) as recently established. We compared maximum myocardial uptake (20-segment model) from CZT versus standard SPECT MPI by intraclass correlation without and with CT AC. In addition, clinical agreement for each coronary territory for all scans from both devices was assessed, and Bland–Altmann (BA) limits of agreement for percentage uptake were calculated. Results: The clinical agreement between CZT and standard SPECT cameras was 96% for noncorrected low- and high-dose images (r = 0.90 and BA = −18 to 15, and r = 0.91 and BA = −15 to 16, respectively), and agreement after AC was 96% for low- and 99% for high-dose images (r = 0.87 and BA = −16 to 14, and r = 0.88 and BA = −16 to 14, respectively). Conclusion: Our results support that AC of MPI on the novel CZT camera, compared with AC MPI on a conventional SPECT camera, is feasible because it provides a high correlation of segmental tracer uptake and an excellent clinical agreement.
SPECT MPI is a widely accepted method for evaluating diagnosis and prognosis of ischemic coronary artery disease (CAD) as a guide for patient management in daily clinical routine. However, technical limitations such as soft-tissue attenuation of tracer activity mainly from the inferior myocardial wall (1,2) may affect its specificity. Prone or combined supine–prone acquisition (3) and external radionuclide sources, such as 153Gd (4), have been evaluated for attenuation correction (AC). Recently, attenuation maps obtained from unenhanced CT x-ray scans have been introduced as a reliable method for AC of myocardial perfusion imaging (MPI) in clinical practice (1,5,6). CT AC proved superior to prone MPI acquisition (7) and has several advantages over external radionuclide sources for AC, such as higher photon flux and hence no influence by cross-talk from the SPECT radionuclide, no decay of transmission source, and shorter scan times (8,9).
Not only the need for increased patient throughput to improve cost-effectiveness but also the necessity of reducing patients’ discomfort and minimizing motion artifacts have induced the search for strategies for shortening MPI acquisition and protocol times. Recently, a new γ-camera was introduced with a novel generation of detectors using cadmium-zinc-telluride (CZT) semiconductor technology, which allows reduction of scan time down to a few minutes (10,11). Despite these remarkable refinements, the discrimination of artifacts due to soft-tissue attenuation from real perfusion defects has remained a challenge. Therefore, the aim of this study was to validate x-ray–based CT AC of MPI from a CZT camera using a conventional dual-head SPECT camera as a standard of reference.
MATERIALS AND METHODS
The present study included 66 consecutive patients who were referred to MPI for the assessment of ischemic CAD. All patients underwent MPI on a standard dual-detector SPECT camera (Ventri; GE Healthcare) and on a novel ultrafast CZT camera (Discovery NM 530c; GE Healthcare). The study protocol was approved by the local ethics committee, and written informed consent was obtained from each patient.
Study Protocol
All 66 patients underwent a 1-d 99mTc-tetrofosmin adenosine stress–rest imaging protocol (12). The patients were told to refrain from caffeine-containing beverages for at least 12 h before the MPI study. Pharmacologic stress was induced by infusion of adenosine at a rate of 140 μg/kg/min. A standard dose of 300–350 MBq of 99mTc-tetrofosmin was injected 3 min into the pharmacologic stress. Ninety minutes later, stress study images were acquired on the standard SPECT camera, followed within minutes by the acquisition on the CZT camera. Thereafter, a tracer dose of 2.5–3 times the stress dose was administered at rest, followed by image acquisition on both cameras with the same sequence and protocol as at stress (Fig. 1).

Scheme of study protocol.
CT AC
To create AC maps, all patients underwent an unenhanced 64-slice CT examination on a standalone Light Speed VCT Scanner (GE Healthcare) during a breath-hold, as previously reported (13). The scans covered the entire heart using prospectively electrocardiogram-triggered sequential images at 75% of the R-R interval, 2.5-mm section thickness, and 0.35-s gantry rotation times at 120 kV and 200–250 mA, depending on the patient's size. For CT, attenuation-corrected images were reconstructed with 5.0-mm thickness using a reconstruction algorithm with a 512 × 512 matrix and a full chest–sized adapted field of view of 50 × 50 cm. The reconstructed CT images were then transferred to the Xeleris workstation (GE Healthcare) for AC map generation (13).
SPECT Myocardial Perfusion Image Acquisition and Reconstruction
The first acquisition was performed on a standard dual-head SPECT camera with a low-energy, high-resolution collimator; a 20% symmetric window at 140 keV; a 64 × 64 matrix; and an elliptic orbit with step-and-shoot acquisition at 3° intervals over a 180° arc (45° right anterior oblique to 45° left posterior oblique) with 30 steps (60 views). Scan time was set to 25 s per frame for stress and rest. This scan time resulted in a total acquisition time of 14 min 52 s (including interstep rotation time) for each scan, as recommended by the American Society of Nuclear Cardiology (14). Images were reconstructed on the same dedicated workstation as was used for CT maps, with a standard iterative reconstruction algorithm—ordered-subset expectation maximization (2 iterations, 10 subsets) with and without CT AC—into standard short-axis and vertical and horizontal long-axis views and polar maps of perfusion encompassing the entire left ventricle. A Butterworth postprocessing filter (frequency, 0.50; order, 10) was applied to the reconstructed slices.
CZT Image Acquisition and Reconstruction
The second scan was acquired on a CZT camera with pinhole collimation (15), for which the conventional sodium iodide (NaI) crystals have been replaced by CZT semiconductor detectors that directly convert radiation into electric signals without any of the steps of violet light production, transport, and conversion as occurs with NaI crystals (16). Compared with a dedicated cardiac γ-camera (Ventri; GE Healthcare) (10,11), for the CZT camera the energy and spatial resolutions (radial resolution, 4.3 mm) were improved by a factor of 2, and the sensitivity (21.0 counts/s/MBq [21.0 counts/s/mCi]) was improved by a factor of almost 4. The new CZT technology is extremely compact, and this miniaturization—together with the increased resolution—offers the opportunity to construct a stationary array of 19 small γ-cameras packed closely together and focused on the heart. The stationary array simultaneously acquires all the views necessary for tomographic reconstruction, saving the time taken by conventional cameras to acquire views while rotating around the subject. All the views are simultaneously focused on the heart to maximize efficiency of cardiac imaging. To fit the multiple views, the image is reduced by means of pinhole collimation, matching the miniaturization to the improved intrinsic pixel resolution of the detectors. This reduction allows for the maximization of detector surface use, which translates into increased system efficiency. The pinhole geometry has several advantages: the reduction in pinhole sensitivity with increasing distance significantly diminishes the contribution of background organs and tissues to the cardiac data, facilitating reliable 3-dimensional iterative reconstruction. In addition, the oblique angles of incidence also improve the already superior energy resolution of the CZT.
Stress (low-dose) scans were acquired over 3 min and rest (high-dose) scans over 2 min as previously suggested (10). Images were reconstructed on the same workstation as was used for CT AC, with a new dedicated iterative algorithm with integrated collimator geometry modeling, using maximum penalized likelihood iterative reconstruction to obtain perfusion images in standard axes. The same operator, experienced in nuclear cardiology, reconstructed the datasets from both scanners to ascertain the use of identical reorientation parameters. Forty and 50 iterations for low and high counts, respectively, were performed, requiring approximately 1-min processing time. A Butterworth postprocessing filter (frequency, 0.37; order, 7) was applied to the reconstructed slices, according to the manufacturer's recommendations based on phantom studies.
Quantitative Analysis
Quantitative analysis was performed on MPI polar maps of noncorrected and attenuation-corrected images, and images were analyzed using a 20-segment left ventricular model for the left ventricle (14). Uptake was normalized to 100% of peak activity, and relative percentage count uptake of γ-ray emissions was assessed for each segment from standard SPECT camera and CZT data for low and high dose scans.
Visual Analysis
Masked visual analysis was performed for noncorrected and attenuation-corrected images with regard to the presence or absence of perfusion defects in the 3 main coronary territories—that is, left anterior descending artery, circumflex artery, and right coronary artery—as previously suggested (14). Two experienced nuclear cardiologists made the clinical analysis by consensus.
Statistics
SPSS software (15.0; SPSS Inc.) was used for statistical testing. Quantitative variables were expressed as mean ± SD and categoric variables as frequencies, mean, or percentages. Tracer uptake values (percentage of maximum myocardial uptake) from the CZT camera were compared segmentwise by intraclass correlation to the standard SPECT camera data, and Bland–Altman (BA) limits of agreement were calculated. Clinical agreement was assessed per coronary territory. P values of less than 0.05 were considered statistically significant, and the 95% confidence intervals (CIs) are presented.
RESULTS
All 66 patients (48 men) successfully underwent MPI on the standard SPECT and CZT cameras. Forty patients (61%) were referred because of suspected ischemia but unknown CAD and 26 patients (39%) because of known CAD with suspected deterioration. Mean age (±SD) was 65 ± 11 y (range, 38–82 y), and the mean body mass index was 27.2 ± 3.7 kg/m2 (range, 19.1–36.0 kg/m2) for the men and 26.1 ± 3,1 kg/m2 (range, 21.7–30.8 kg/m2) for the women. A mean (±SD) of 335.7 ± 25.0 MBq of 99mTc-tetrofosmin (range, 303–455 MBq) for stress and 945.0 ± 73.4 MBq (range, 894.0–1,244 MBq) for rest were administered.
Quantitative Analysis
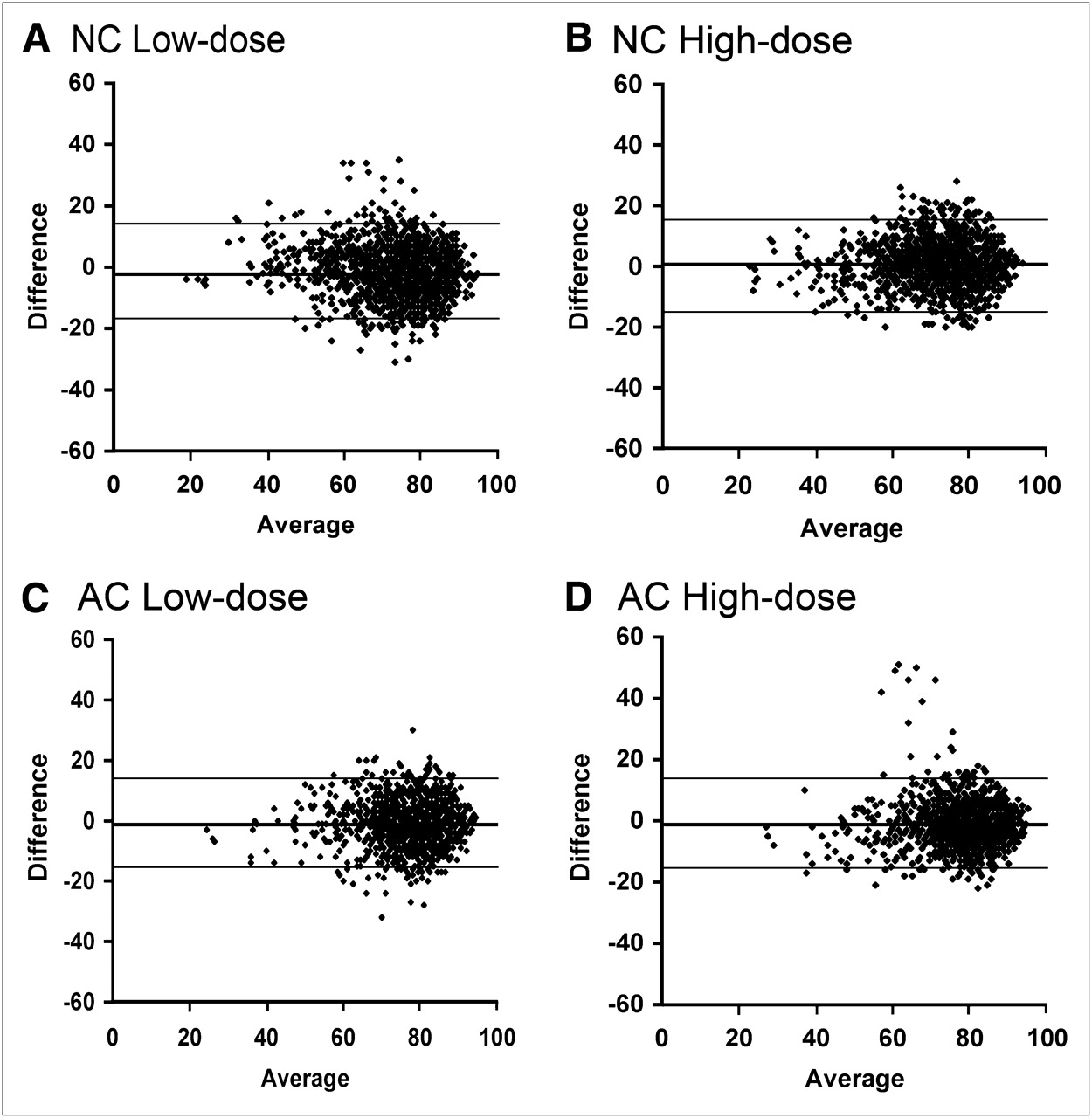
The intraclass correlation coefficient (between CZT and standard SPECT data) for quantitative tracer uptake of noncorrected images was 0.90 (95% CI, 0.88–0.91; BA, −18 to 15) for low-dose images (stress) and 0.91 (95% CI, 0.90–0.92; BA, −15 to 16) for high-dose images (rest). Similarly, for attenuation-corrected images, the correlation coefficient was 0.87 (95% CI, 0.85–0.88; BA, −16 to 14) for low-dose images and 0.88 (95% CI, 0.86–0.89; BA, −16 to 14) for high-dose images (Table 1; Fig. 2).
Percentage Segmental Tracer Uptake: Correlation Between CZT and Standard Cameras

Bland–Altman limits of agreement for percentage segmental tracer uptake for noncorrected (NC) and attenuation-corrected (AC) myocardial perfusion images from CZT and standard SPECT cameras.
Visual Analysis
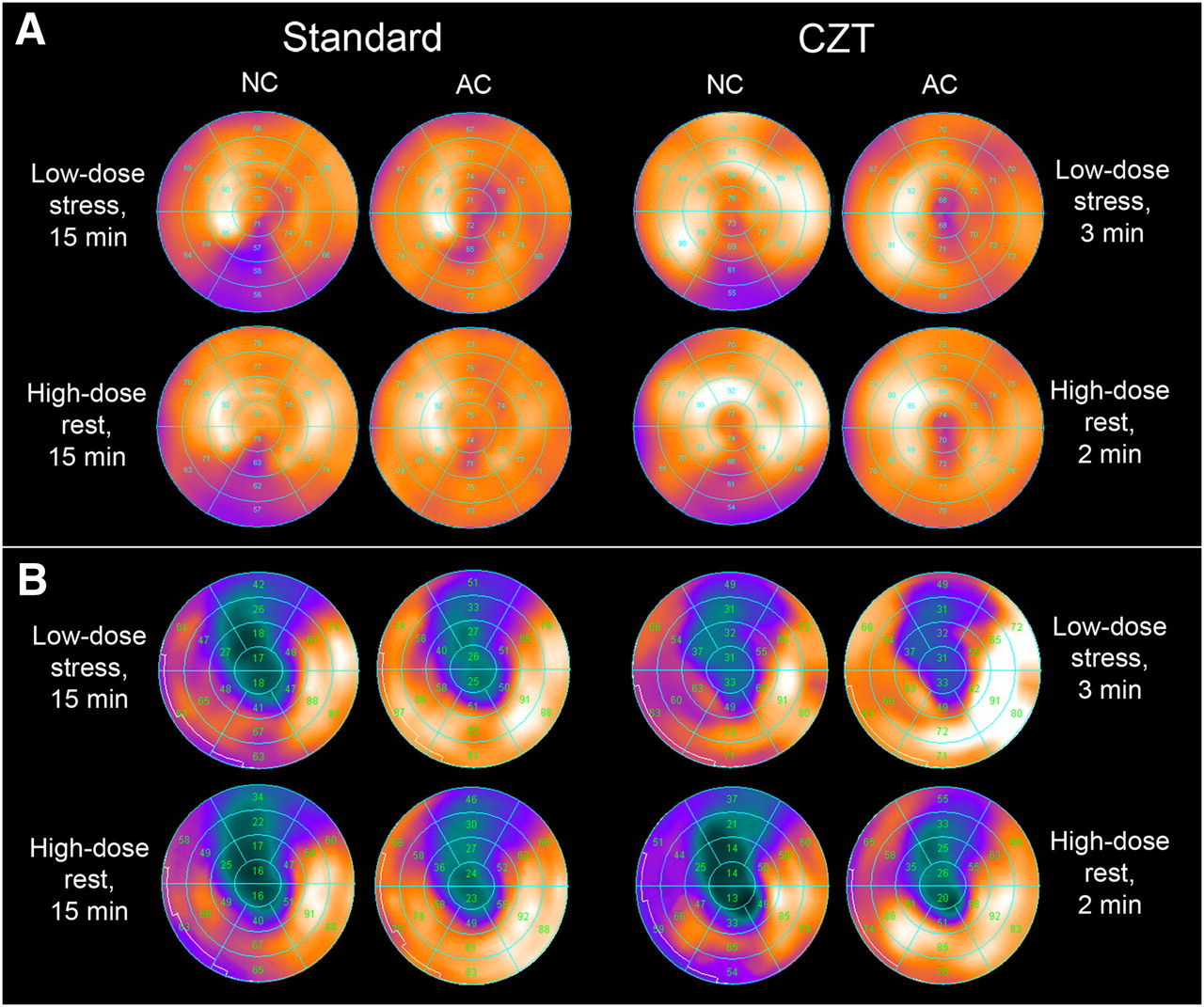
Image quality was diagnostic for all MPI on both the standard SPECT and the CZT cameras. Of the 198 possible coronary territories (66 patients × 3 coronary territories), 61 revealed a perfusion defect at stress (low-dose scan) and 55 at rest (high-dose scan). For noncorrected images the clinical agreement per territory between the CZT and standard SPECT cameras was 96% for both stress (95% CI, 0.92%–0.98%) and rest (95% CI, 0.93%–0.99%) scans. Similarly, for attenuation-corrected images the clinical agreement was 96% (95% CI, 0.93%–0.99%) for stress scans and 99% (95% CI, 0.96%–0.99%) for rest scans (Fig. 3). On the standard SPECT camera, 28 of 61 stress perfusion defects and 29 of 55 rest perfusion defects were unmasked as artifacts because they disappeared after correction with x-ray–based CT attenuation maps. These artifacts were predominantly located in the right coronary artery (stress, n = 24/28; rest, n = 27/29) and mainly found in male patients (stress, 22 men; rest, 25 men). The territory- and patient-based results are summarized in Table 2. Twenty-three of these 28 stress artifacts and 26 of these 29 rest artifacts were also present in CZT scans and were appropriately unmasked by AC.

Polar plot presentation of nuclear myocardial perfusion images from patient with normal perfusion (A) and from one with fixed anteroapical perfusion defect (B) with attenuation (AC) and without attenuation (NC) on standard SPECT camera (left) and novel CZT camera (right).
Clinical Agreement Between CZT and Standard Cameras
DISCUSSION
Our study is the first, to our knowledge, to establish the feasibility and validate the accuracy of CT AC for MPI on the novel CZT camera, compared with scans from a conventional dual-head SPECT camera reconstructed with AC as a standard of reference. The CZT solid-state detector technology allows MPI with increased resolution and a minimized scan time (10,17) and may therefore have the potential to emerge as an alternative to conventional SPECT cameras. Tissue attenuation plays a major role in SPECT MPI because it can affect the diagnostic accuracy, mainly by decreasing specificity, and as a consequence reduce cost-effectiveness (18,19) or even lead to nondiagnostic studies (20). Therefore, several strategies for AC have been evaluated, among which CT AC has proven most successful (1). Interestingly, the present study reveals that attenuation artifacts can nevertheless occur with this latest-generation camera, despite the increase of system sensitivity of CZT detectors and improved signal specificity of multipinhole technique. In the present study with 66 patients and 198 possible coronary territories, 28 defects at stress and 29 defects at rest were unmasked as attenuation artifacts in MPI on a standard SPECT camera. These artifacts were predominantly located in the right coronary artery territory, in line with several previous reports (1,13,21). All defects found in conventional SPECT MPI and classified as artifacts by CT AC were also identified in CZT MPI.
We have chosen CT AC because this method has been reported to be technically well established not only in hybrid SPECT/CT scanners integrating a γ-camera with a CT device but also when CT AC maps are obtained from a standalone CT scanner (13).
CT AC has been reported in 1 study to substantially increase confidence and improve diagnostic performance, primarily by increasing the specificity of MPI (21). The degree of specificity improvement in that study depended on the interpretative attitude, as readers prone to high sensitivity or with less experience had the greatest gain in the normalcy rate, whereas readers prone to higher specificity had improvement in sensitivity and specificity but not the normalcy rate. Thus, improvements in any of the diagnostic variables were not counterbalanced by degradation of other variables, supporting that CT-based AC of SPECT MPI is well suited for routine use in clinical practice. The unenhanced low-dose CT scan for AC has been shown to allow the calculation of the calcium score (13), which may improve the diagnostic and prognostic accuracy of MPI when used as an adjunct to SPECT MPI (22,23). The new CZT camera differs in many respects from conventional SPECT γ-cameras, because not only a new semiconductor to replace the NaI crystals but also multiple detector heads allowing simultaneous image acquisition using a pinhole geometry in 19 angles have been introduced. Despite these significant differences, x-ray–based CT AC remains feasible and helpful for the successful discrimination of artifacts from true perfusion defects. In fact, these results show excellent agreement with conventional SPECT MPI scans for both quantitative segmental tracer uptake and clinical findings and diagnostic conclusions.
The following limitations have to be considered: we included patients with a body mass index ranging from 19.1 to 36.0 kg/m2 into our study population. Therefore, our results must be read with caution when extrapolating them to patients with a substantially different body mass index, particularly when exceeding the upper range. Similarly, as the present results are mainly based on inferior artifacts (generally perceived as male pattern) because of underrepresentation of women in this study (27%), an evaluation in a large population of female patients should be considered. Furthermore, we did not use invasive coronary angiography as a standard of reference. Thus, we theoretically cannot entirely exclude overcorrection of true inferior artifacts.
However, we felt it more appropriate to use an MPI modality as a standard of reference for a study assessing MPI with a new device, particularly because the accuracy of CT AC for SPECT has been well established (21).
CONCLUSION
Our results support the feasibility of AC of MPI on the novel CZT camera. Segmental tracer uptake correlated strongly with AC of MPI on a conventional SPECT camera, and clinical agreement was excellent.
Acknowledgments
We thank our radiography team, especially Edlira Loga and Ennio Müller, for their excellent technical support. The study was supported by a grant from the Swiss National Science Foundation (SNSF) and by the ZIHP (Zurich Center for Integrative Human Physiology, University of Zurich, Switzerland). The university hospital holds a research contract with GE Healthcare.
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication April 13, 2010.
- Accepted for publication July 8, 2010.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Direct Attenuation Correction Using Deep Learning for Cardiac SPECT: A Feasibility Study
- Absolute Myocardial Blood Flow and Flow Reserve Assessed by Gated SPECT with Cadmium-Zinc-Telluride Detectors Using 99mTc-Tetrofosmin: Head-to-Head Comparison with 13N-Ammonia PET
- Flow-Dependent Uptake of 123I-CMICE-013, a Novel SPECT Perfusion Agent, Compared with Standard Tracers
- Achieving Very-Low-Dose Radiation Exposure in Cardiac Computed Tomography, Single-Photon Emission Computed Tomography, and Positron Emission Tomography
- Attenuation Correction Maps for SPECT Myocardial Perfusion Imaging from Contrast-Enhanced Coronary CT Angiography: Gemstone Spectral Imaging with Single-Source Dual Energy and Material Decomposition
- Cadmium-Zinc-Telluride Myocardial Perfusion Imaging in Obese Patients
- Transplantation and Tracking of Human-Induced Pluripotent Stem Cells in a Pig Model of Myocardial Infarction: Assessment of Cell Survival, Engraftment, and Distribution by Hybrid Single Photon Emission Computed Tomography/Computed Tomography of Sodium Iodide Symporter Transgene Expression
- Semiconductor Detectors Allow Low-Dose-Low-Dose 1-Day SPECT Myocardial Perfusion Imaging
- Cardiac Dedicated Ultrafast SPECT Cameras: New Designs and Clinical Implications