


Abstract
We have evaluated the impact of increased body mass on the quality of myocardial perfusion imaging using a latest-generation γ-camera with cadmium-zinc-telluride semiconductor detectors in patients with high (≥40 kg/m2) or very high (≥45 kg/m2) body mass index (BMI). Methods: We enrolled 81 patients, including 18 with no obesity (BMI < 30 kg/m2), 17 in World Health Organization obese class I (BMI, 30–34.9 kg/m2), 15 in class II (BMI, 35–39.9 kg/m2), and 31 in class III (BMI ≥ 40 kg/m2), including 15 with BMI ≥ 45 kg/m2. Image quality was scored as poor (1), moderate (2), good (3), or excellent (4). Patients with BMI ≥ 45 kg/m2 and nondiagnostic image quality (≤2) were rescanned after repositioning to better center the heart in the field of view. Receiver-operating-curve analysis was applied to determine the BMI cutoff required to obtain diagnostic image quality (≥3). Results: Receiver-operating-curve analysis resulted in a cutoff BMI of 39 kg/m2 (P < 0.001) for diagnostic image quality. In patients with BMI ≥ 40 kg/m2, image quality was nondiagnostic in 81%; after CT-based attenuation correction this decreased to 55%. Repositioning further improved image quality. Rescanning on a conventional SPECT camera resulted in diagnostic image quality in all patients with BMI ≥ 45 kg/m2. Conclusion: Patients with BMI ≥ 40 kg/m2 should be scheduled for myocardial perfusion imaging on a conventional SPECT camera, as it is difficult to obtain diagnostic image quality on a cadmium-zinc-telluride camera.
Among the many refinements of SPECT myocardial perfusion imaging (MPI) that have occurred over the past decade, most have been related to new reconstruction algorithms (1), early imaging protocols (2,3), and tracer development rather than to fundamental advancements of hardware. Only recently has a new generation of cardiac γ-cameras emerged using the concept of miniaturized cadmium-zinc-telluride (CZT) semiconductor detectors serially aligned around the patient. The multipinhole design renders rotation of the camera around the patient unnecessary, as it covers the entire heart throughout the scan. This advance has multiplied system sensitivity. The first results (4) from CZT cameras have fuelled high expectations with regard to lower activity (5), shorter scan times (6), and possibly improved image quality (7). In particular, the multipinhole geometry may have the potential to decrease artifacts from extracardiac activity and from abdominal soft-tissue attenuation. This is of particular importance in obese subjects, who represent a growing proportion of patients undergoing evaluation for coronary artery disease and may benefit the most from multipinhole geometry. On the other hand, as a result of this geometry, the heart has to be centered in a much smaller field of view than with conventional cameras, and image acquisition may often be challenging in obese patients even after repositioning of the patient.
The aim of the present study was to systematically assess the feasibility of CZT MPI scanning in patients with high, very high, or excessive body mass index (BMI).
MATERIALS AND METHODS
Study Population
We enrolled 65 obese patients (BMI ≥ 30 kg/m2) and 18 randomly selected nonobese patients (BMI < 30 kg/m2) referred for the assessment of known or suspected coronary artery disease by 1-d stress/rest MPI on a CZT γ-camera (NM/CT 570c; GE Healthcare). Patients were assigned according to the World Health Organization into obese class I (BMI, 30–34.9 kg/m2), II (BMI, 35–39.9 kg/m2), or III (BMI ≥ 40 kg/m2). Class III patients were further categorized as “morbid obese” (BMI ≥ 40 kg/m2) or “super obese” (BMI ≥ 45 kg/m2) as previously suggested (8). We enrolled a minimum of 15 patients per group. In addition to BMI, the chest wall circumference of supine patients was measured at the level of the mammillae. The need to obtain written informed consent was waived because of the nature of the study, which included solely clinical data collection.
Image Acquisition
All patients underwent a 1-d pharmacologic stress/rest SPECT MPI protocol with standard adenosine infusion (0.14 mg/kg/min over 6 min). After 392 ± 47 MBq of 99mTc-tetrofosmin had been administered, stress MPI images were acquired approximately 60 min later (during 5 min) on the CZT camera. This acquisition was followed by rest MPI using the identical protocol several minutes after administration of a 3 times higher dose of 99mTc-tetrofosmin (1,143 ± 133 MBq), as previously validated (9,10). MPI scans were acquired using a multipinhole collimator and 19 stationary detectors simultaneously imaging 19 different views of the heart as previously reported (6). In brief, each detector contains 32 × 32 pixelated (2.46 × 2.46 mm) CZT elements; the system design allows acquisition without detector or collimator motion, and a 10% symmetric energy window at 140 keV was used. An unenhanced low-dose 64-slice CT scan with prospective triggering at 75% of the R-R interval was performed for attenuation correction (AC) of CZT MPI (11,12).
Whenever the heart was out of the camera field of view (19-cm diameter) on supine CZT MPI scanning, the acquisition was immediately repeated on the same camera after repositioning the patient by inclination of the chest by 20°–30° or by shifting the body closer to the CZT detector. All 15 patients with a BMI ≥ 45 kg/m2 were additionally scanned on a conventional dual-head SPECT/CT camera (Infinia; GE Healthcare) at the same session according to our clinical routine for super obese patients. Briefly, emission data were acquired with a parallel-hole, low-energy, high-resolution collimator with a 20% symmetric window centered at 140 keV (3° of rotation per stop, 180° for each head, and 25 s per projection). After MPI, CT for AC was performed using the Infinia system at 140 keV and 3.0 mA (13).
MPI Image Reconstruction
CZT images were reconstructed as previously described (6,9) on a dedicated Xeleris workstation (GE Healthcare) applying an iterative reconstruction algorithm with maximum-likelihood expectation maximization. The software Myovation for Alcyone (GE Healthcare) was used for image reconstruction, and a Butterworth postprocessing filter was applied to the reconstructed slices. All MPI scans were reconstructed in standard axes (short axis, vertical long axis, and horizontal long axis), and polar maps of perfusion were generated using a commercially available software package (Cedars QGS/QPS; Cedars-Sinai Medical Center) (14).
Image Quality Assessment
MPI scans were visually scored for quality using an adapted 4-grade scoring system (1 = poor, 2 = moderate, 3 = good, and 4 = excellent) (15) by 2 masked experienced nuclear cardiologists based on predefined cardiac image characteristics (homogeneity of myocardial radionuclide uptake, integrity or truncation of left ventricle as previously defined (16), and position of left ventricle in the field of view) or interference from extracardiac radioactivity (no activity, minor activity adjacent to the myocardium but not affecting image interpretation, or excessive blood-pool activity or activity significantly reducing confidence in image interpretation). Discrepancies between the 2 readers were resolved by consensus. If the image quality was at least 3 or better, the MPI was considered diagnostic.
Statistical Analysis
Quantitative variables were expressed as mean ± SD, and categoric variables as frequencies or percentages. SPSS software, version 19.0 (IBM), was used for all statistical analysis. Receiver-operating-curve analysis was applied to measure the area under the curve (AUC) to determine optimal cutoffs for BMI and chest wall circumference to ensure diagnostic image quality. The Mann–Whitney U test and the Jonckheere Terpstra test were used to check for significant differences in image quality between the different modalities. P values of less than 0.05 were considered statistically significant.
RESULTS
After exclusion of 2 patients with a BMI over 60 kg/m2 from further analysis due to geometric inability to fit into either the CZT or the conventional SPECT camera, this study included 18 nonobese patients (BMI, 25 ± 2 kg/m2) and 63 obese patients. The patient baseline characteristics are given in Table 1. Eight patients were rescanned on the CZT camera after repositioning, as the heart was out of the field of view. The upper limit of chest circumference to fit into the gantry of the CZT (and the conventional SPECT) camera in the present study was 141 cm. Chest circumference was closely related to BMI (r = 0.87, P < 0.001). Image quality from the CZT scanner was significantly higher in men than in women, both with AC (3.1 ± 0.1 vs. 2.7 ± 0.2, P < 0.05) and without AC (2.9 ± 0.1 vs. 2.4 ± 0.2). Heart size was comparable in nonobese and obese patients (end-diastolic volume, 92.3 ± 42.9 vs. 92.4 ± 50.4, P = not statistically significant).
Patient Baseline Characteristics
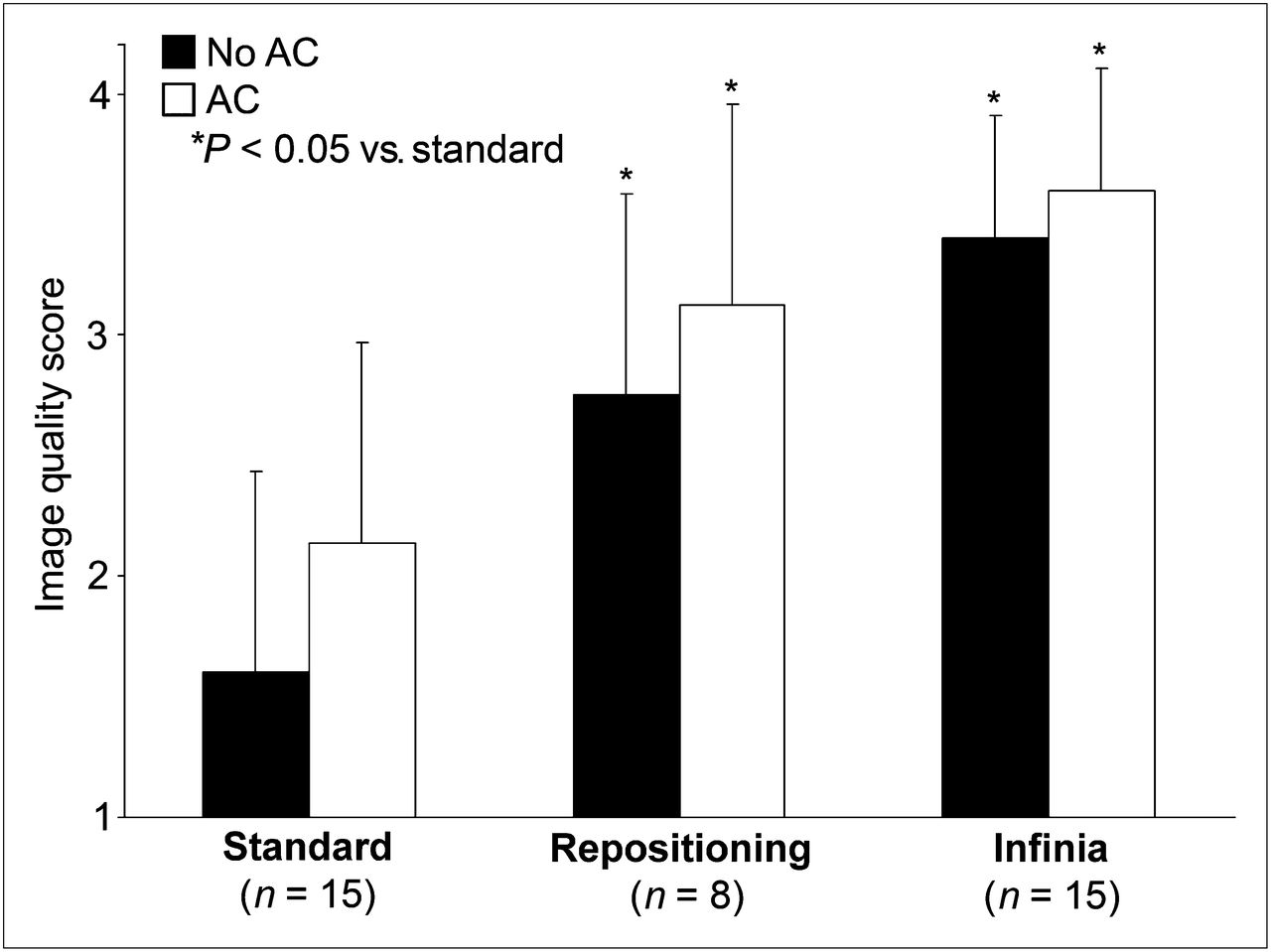
Image quality of the different BMI groups is given in Tables 2 and 3. In patients with BMI ≥ 40 kg/m2, 81% of the CZT scans were nondiagnostic (Fig. 1), mainly because the cardiac position was out of focus, causing truncation artifacts of the left ventricle (Fig. 2). After application of AC, this rate significantly decreased to 55% (P < 0.05). In patients with BMI ≥ 45 kg/m2, the CZT image quality (no AC; 1.6 ± 0.7; AC, 2.1 ± 0.8) improved significantly (Fig. 3) after patient repositioning within the CZT camera (no AC, 2.8 ± 0.7; AC, 3.1 ± 0.8; P < 0.05). Similarly, image quality from SPECT MPI was substantially and significantly higher (no AC, 3.4 ± 0.5; AC, 3.6 ± 0.5; P < 0.001) than that from CZT MPI, reaching diagnostic image quality in every patient. Overall, 59 (73%) of 81 scans were reported as normal.
Image Quality in Patients with BMI < 45 kg/m2
Image Quality in Patients with BMI ≥ 45 kg/m2
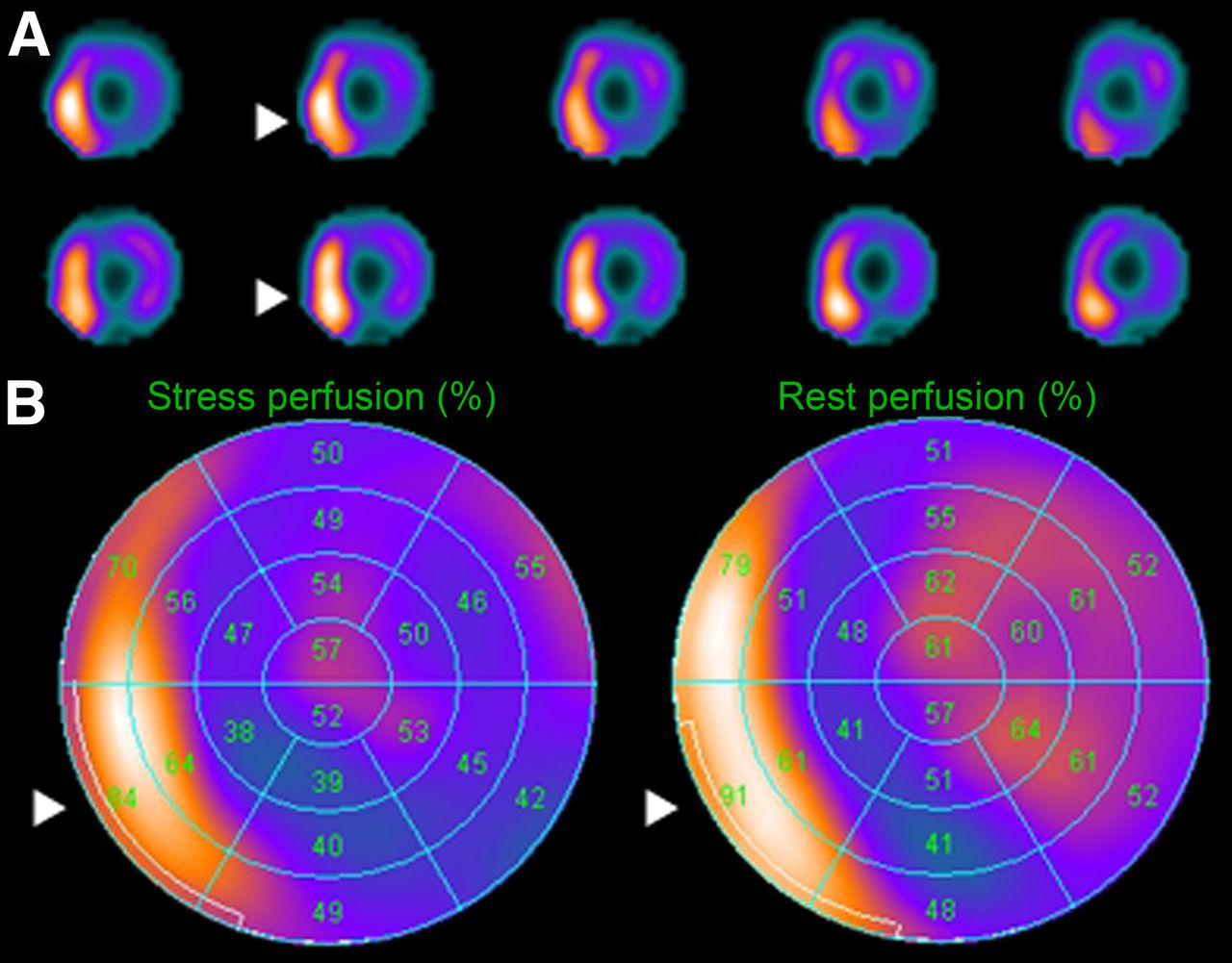
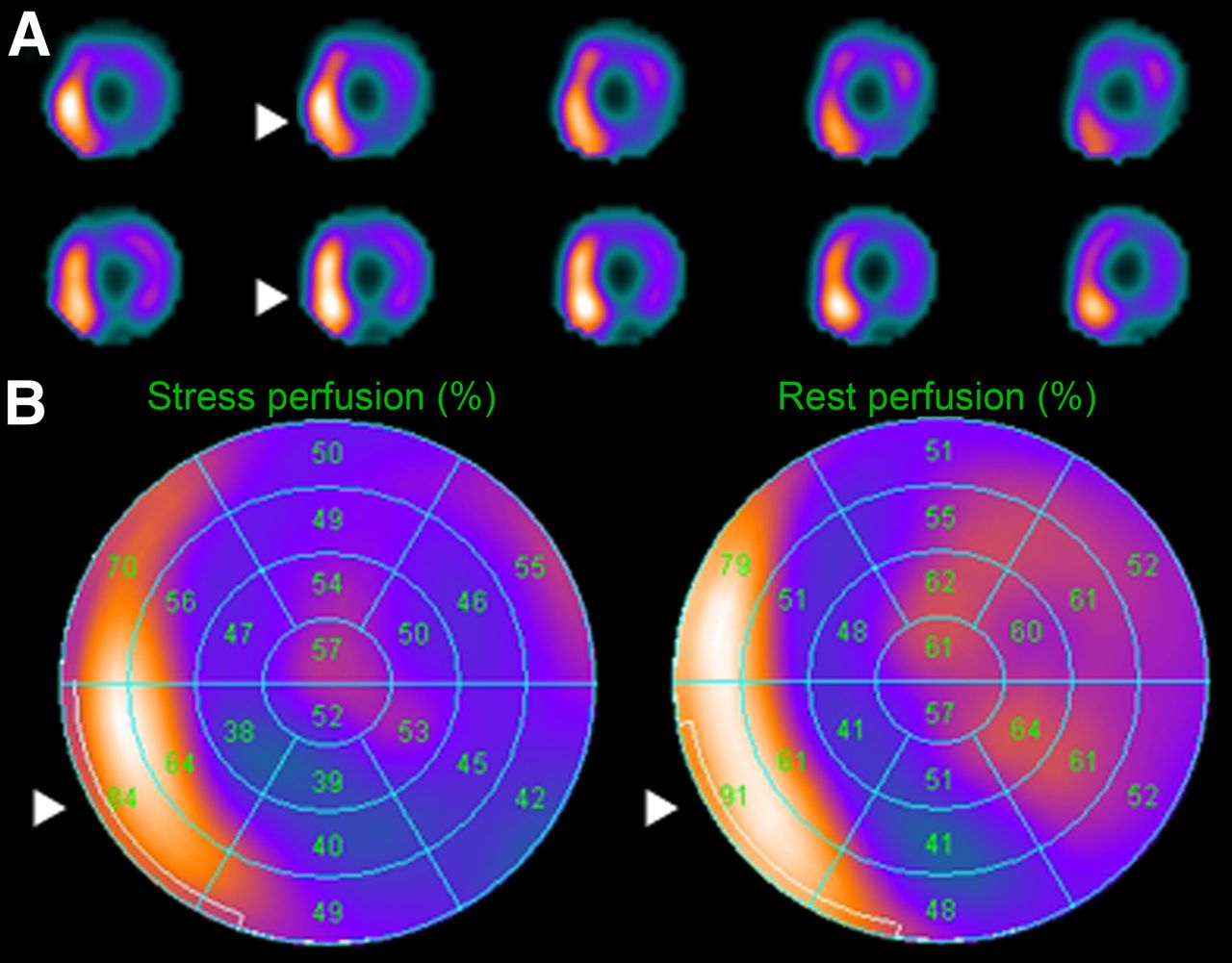
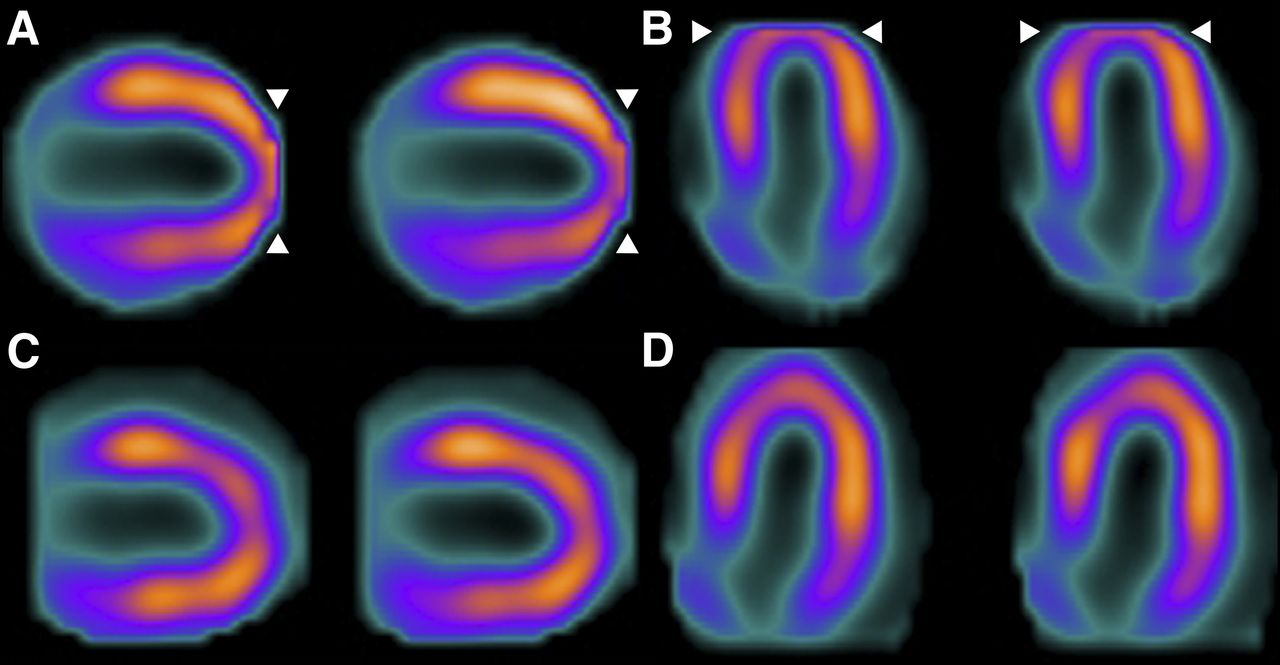
Obesity artifact in SPECT MPI. Typical artifact (banana shape; arrowheads) observed in CZT scanning of obese patients is shown on short-axis images (A) and corresponding polar maps (B).

Apical truncation artifact. Eccentric position of heart causes apical truncation artifact (arrowheads), illustrated in vertical (A) and horizontal (B) long-axis views; for comparison, same views are given without truncation artifact (C and D).
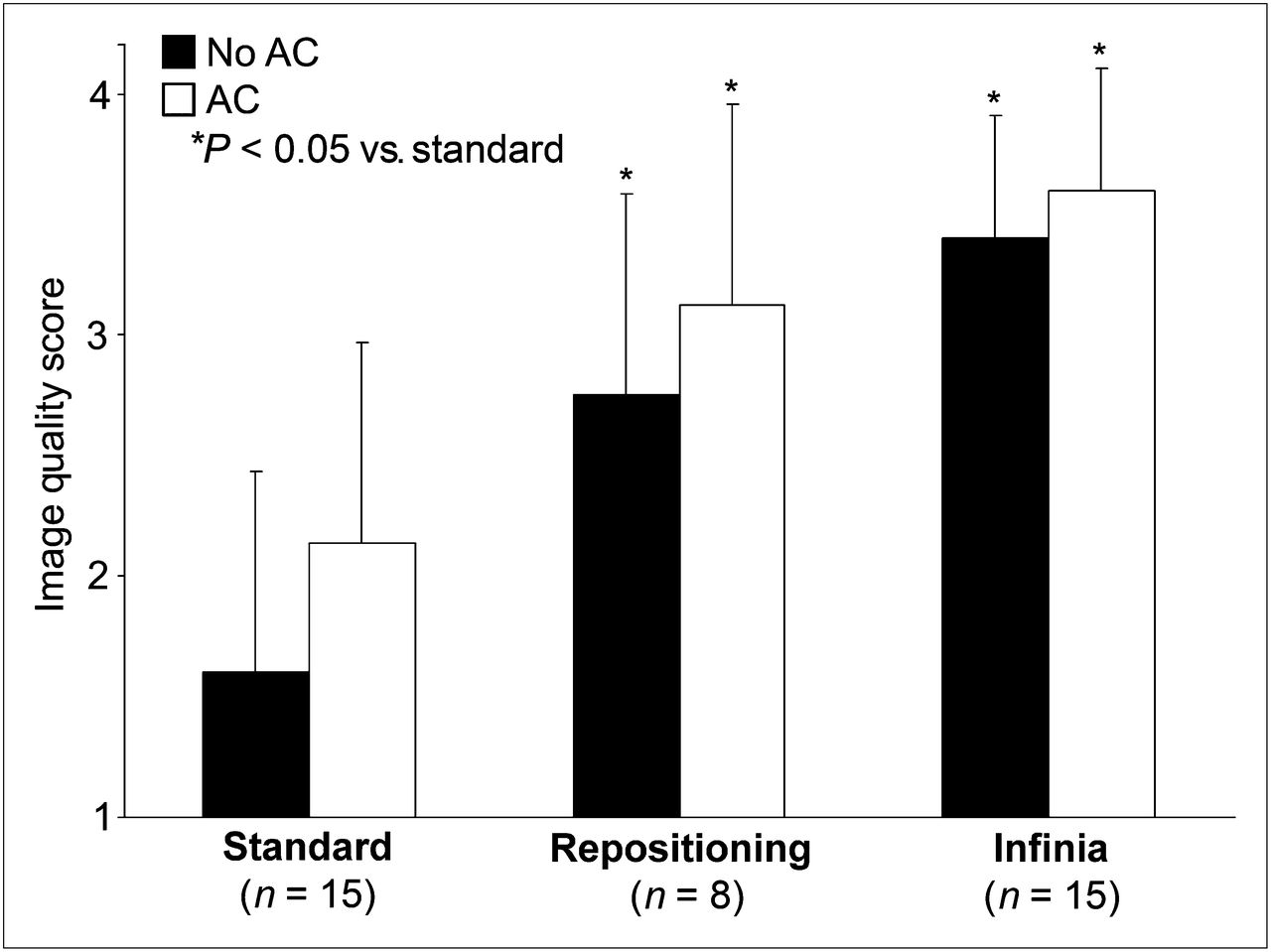
Image quality in patients with BMI ≥ 45 kg/m2. Shown is image quality of standard CZT MPI (n = 15), CZT MPI after repositioning (n = 8), and conventional SPECT (n = 15).
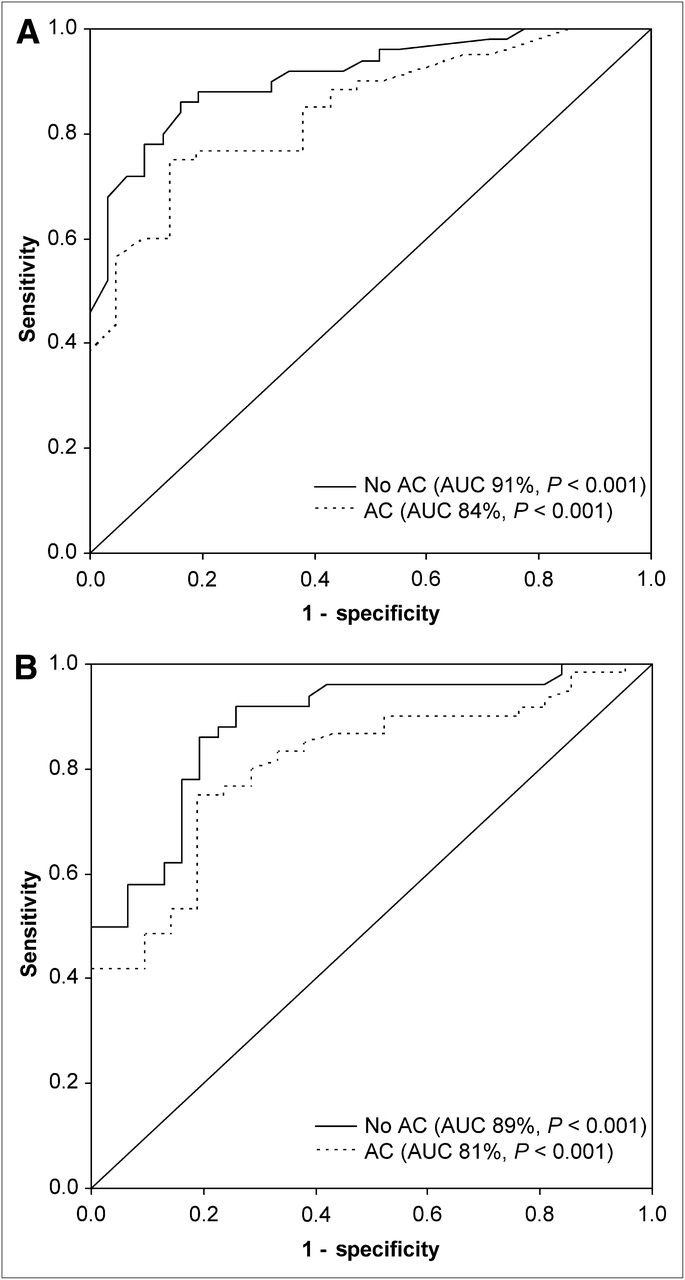
Receiver-operating-curve analysis (Fig. 4A) revealed a cutoff BMI of 39 kg/m2 to obtain diagnostic MPI quality for both non-AC images (AUC, 91%; confidence interval, 0.85–0.97; P < 0.001) and AC images (AUC, 84%; confidence interval, 0.75–0.93; P < 0.001). Similarly, for chest wall circumference, receiver-operating-curve analysis (Fig. 4B) revealed a cutoff of 123 cm to obtain diagnostic MPI quality for both non-AC images (AUC, 89%; confidence interval, 0.81–0.96; P < 0.001) and AC images (AUC, 81%; confidence interval, 0.71–0.91; P < 0.001). Differences in image quality between non-AC and AC images were not statistically significant.
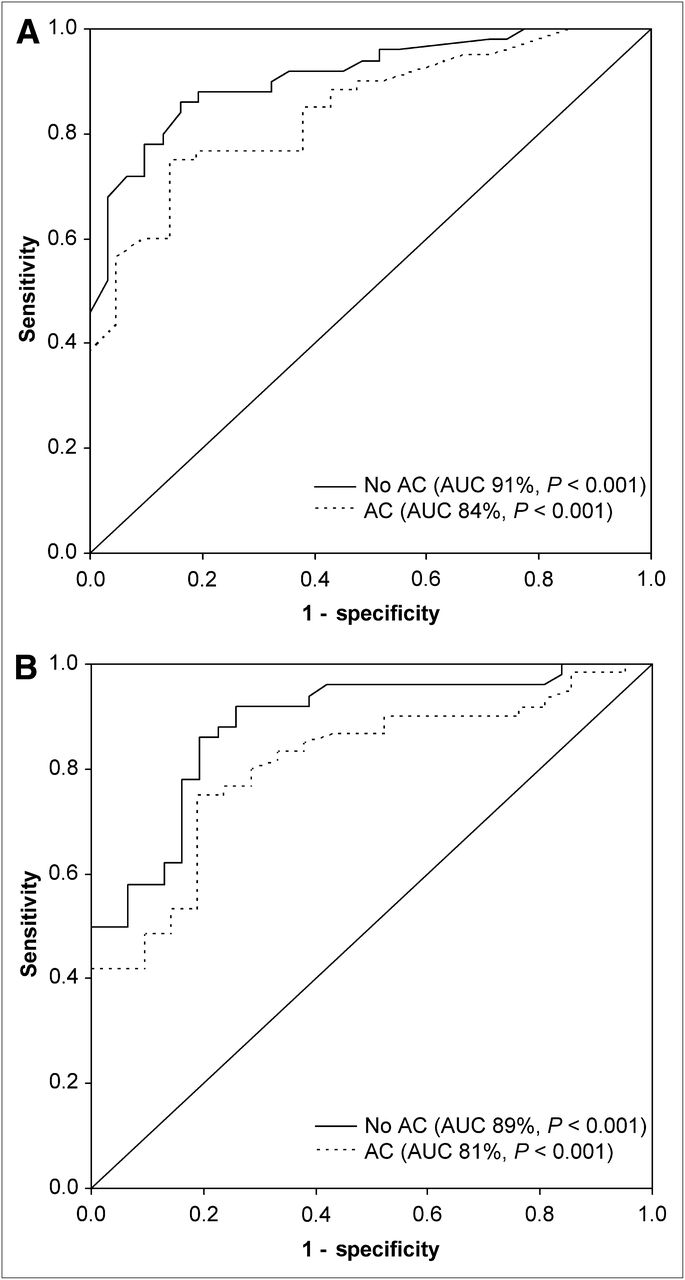
Receiver-operating-curve analysis for CZT MPI image quality and BMI (A) or chest wall circumference (B).
DISCUSSION
Our results suggest that for patients with morbid obesity, MPI on CZT cameras may often yield insufficient image quality; the patient’s heart cannot get close enough to the detectors because the body mass is too high for the size of the gantry. As a result, in patients with BMI ≥ 40 kg/m2, 81% of non-AC scans and 55% of AC scans were nondiagnostic. By contrast, image quality was significantly better from a conventional γ-camera and was diagnostic in all patients.
Obesity may often affect the quality of SPECT MPI scans, mainly because of reduction of test specificity by diaphragm soft-tissue attenuation and extracardiac activity (17–21). CT-based AC has been found to compensate at least in part for inferior soft-tissue attenuation, resulting in improved SPECT MPI diagnostic (22) and prognostic (23) accuracy. The latest generation of γ-cameras with CZT detectors was expected to offer improved image quality in obese patients, as its detector geometry with pinhole collimation should help avoid image degradation by soft-tissue attenuation. Attenuation artifacts can nevertheless occur but can be corrected with x-ray–based CT attenuation maps (12). In the new generation of cardiac CZT cameras the target organ, the heart, has to be centered accurately within the field of view, which is substantially smaller than that on standard SPECT cameras. For most patients in our daily routine, this requirement does not present any limitation. However, in patients with morbid obesity this limitation becomes critical, particularly in a center such as ours, which receives regular referrals for preoperative MPI from an associated busy bariatric surgery program.
Our data show that AC may improve image quality but fails to solve the fundamental problem of imaging obese patients with CZT cameras. Even careful repositioning frequently remains unsuccessful in some very obese patients, in whom the standard SPECT camera remains the first-choice tool. By receiver-operating-curve analysis, we have identified a BMI of 39 kg/m2 as the cutoff for direct scheduling of scanning on a standard camera. BMI rather than absolute weight is used to categorize obesity, as the absolute weight in tall persons may be high without reflecting obesity. Consequently, BMI rather than absolute weight is most appropriate for identifying patients who should not undergo CZT scanning. Very rarely, however, the patient’s circumference exceeds the gantry even of such a camera, as was the case in 2 of our patients, rendering scanning impossible on any of our available devices. The ability of the patient to fit within the scanner should therefore be routinely tested before any tracer activity is injected.
It may be seen as a potential limitation of the present study that we did not assess the accuracy of CZT by comparing it with a reference standard such as invasive coronary angiography with fractional flow reserve. Such an assessment, however, was beyond the scope of the present feasibility study, which was designed to evaluate how severe obesity interacts with diagnostic image quality in the new-generation CZT γ-camera. Furthermore, not all patients were rescanned on a conventional SPECT camera for direct comparison, and therefore the relatively small size of the study subgroups may appear as a limitation. However, all patients with BMI ≥ 45 kg/m2 (n = 15) were rescanned, and this rescanning increased the rate of diagnostic image quality to 100%. It may be reasonable to assume that in less obese patients, MPI on a standard SPECT camera would not be less successful. Similarly, only 8 of 15 patients—mainly those with nondiagnostic image quality after AC—were repositioned and rescanned with the heart better centered in the field of view. However, the subjective discomfort induced by repositioning of super obese patients was considered too high to justify such a maneuver in patients with diagnostic image quality. Although image quality was higher in men than women overall, the present study was not designed to provide such comparison data for each BMI group. Further, the present study used vasodilator stress although the use of physical exercise stress might have reduced extracardiac activity and potentially improved image quality. However, severe obesity often hampers the ability to perform adequate physical exercise. Finally, in this non–heart-failure population, heart size was similar in obese and nonobese patients. The role of increased heart size on image quality from CZT cameras with a small field of view remains to be evaluated in patients with an enlarged left ventricle.
CONCLUSION
The introduction of CZT γ-cameras, with their advantages over conventional SPECT cameras, has not solved the issue of image quality degradation from obesity. On the contrary, it appears that the actual design of CZT cameras, with pinhole collimation geometry and a smaller field of view, is more prone to artifacts in very obese patients. Therefore, patients with a BMI of 40 kg/m2 and above should be scheduled on a conventional SPECT camera for MPI scanning.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We thank Ennio Mueller and Patrick von Schulthess for their excellent technical support. This study was supported by a grant from the Swiss National Science Foundation. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jun. 29, 2012.
↵* Contributed equally to this work
- © 2012 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 27, 2011.
- Accepted for publication April 2, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Solid-State Detector SPECT Myocardial Perfusion Imaging
- Radiation Dose and Prognosis of Ultra-Low-Dose Stress-First Myocardial Perfusion SPECT in Patients with Chest Pain Using a High-Efficiency Camera
- Comparison of Image Quality, Myocardial Perfusion, and Left Ventricular Function Between Standard Imaging and Single-Injection Ultra-Low-Dose Imaging Using a High-Efficiency SPECT Camera: The MILLISIEVERT Study
- Cadmium-Zinc-Telluride SPECT in Very Morbidly Obese Patients Routinely Provides High-Diagnostic-Quality Myocardial Perfusion Imaging
- Reply: Cadmium-Zinc-Telluride SPECT in Very Morbidly Obese Patients Routinely Provides High-Diagnostic-Quality Myocardial Perfusion Imaging