


Abstract
An accurate, noninvasive technique for the diagnosis of coronary artery disease (CAD) should provide complementary information on coronary anatomy and pathophysiologic lesion severity. We present, what is to our knowledge, the first clinical evaluation of integrated PET/CT for combined acquisition of coronary anatomy and perfusion. Methods: On an integrated PET/CT scanner, contrast-enhanced CT angiography (CTA) and rest/adenosine-stress myocardial perfusion scanning with 13N-ammonia were performed on 25 patients with CAD documented by coronary angiography. Contrast-enhanced CTA was performed with retrospective electrocardiography gating after injection of 150 mL of intravenous contrast medium. Decisions on whether to treat with revascularization (anatomic lesion plus ischemia) or conservatively (no lesion or no ischemia) based on PET/CT were compared with those based on PET plus coronary angiography. Results: Of the 100 coronary artery segments (left main, left anterior descending, left circumflex, and right in 25 patients), 7 (in 5 patients) were considered impossible to evaluate by CT because of rapid vessel movement but were correctly categorized by PET alone. In the remaining 93 segments, the sensitivity and specificity of PET/CT versus PET plus coronary angiography were 90% and 98%, respectively. Positive and negative predictive values were 82% and 99%, and accuracy was 97%. Conclusion: The data of this preliminary study suggest that PET/CT allows accurate noninvasive clinical decision making about CAD. Because of its high negative predictive value, PET/CT may play an important role in noninvasive selection of CAD patients for revascularization. Integration of higher-performance multislice spiral CT scanners into PET/CT hybrids will accelerate the clinical implementation of this technique.
Coronary angiography is at present the only accepted method for clinical imaging of coronary artery disease (CAD). Despite its cost, inconvenience to patients, and a small but distinct procedure-related morbidity (1.5%) and mortality (0.2%) rate, more than 1 million invasive diagnostic coronary angiography procedures are performed per year in the United States alone. Although coronary angiography is the standard imaging method, it is far from being perfect. Its accuracy is severely hampered by a significant intraobserver and interobserver variability in defining the anatomic relevance of stenoses (up to 50%) (1,2) as underlined by a poor correlation with postmortem coronary anatomy (3,4). In addition, angiographic findings are not able to predict the physiologic relevance of a coronary stenosis (2,5–8). Therefore, it has become clinical standard to require proof of ischemia by a noninvasive test before considering revascularization procedures (9,10).
Because between 20% and 40% of all diagnostic invasive coronary angiograms reveal clinically insignificant disease (11), noninvasive procedures have the potential to play an important role in avoiding unnecessary coronary angiography. Several strategies have been suggested for noninvasive coronary imaging, such as dichromatic synchrotron radiation (12), electron beam tomography (13), MRI (14,15), and multislice spiral CT (1–5,9,10,16).
We hypothesized that assessment of CAD with the combination of PET and contrast-enhanced CTA would noninvasively provide comprehensive information that allows accurate decisions on whether to treat with revascularization or conservatively.
MATERIALS AND METHODS
Study Population
Twenty-five consecutive patients (mean age, 62 y; range, 39–78 y; 22 men and 3 women) who had a history of CAD and underwent elective coronary angiography for recurrent chest pain were invited to participate in the study. A history of myocardial infarction, bypass graft surgery, or previous successful angioplasty was found in 13, 6, and 5 patients, respectively. A coronary artery stenosis was defined as relevant if a diameter reduction of up to 50% was documented by x-ray coronary angiography. Triple-vessel disease was found in 7, dual-vessel disease in 6, and single-vessel disease in 12 patients. All patients had sinus rhythm (mean heart rate, 68 beats per minute; range, 51–83 beats per minute) and were clinically stable. The interval between the coronary angiography and the PET/CT scan was less than 4 wk. Exclusion criteria were severe heart failure (left ventricular ejection fraction < 30%) and renal failure (serum creatinine level > 1.2 mg/dL). All patients had been referred for clinical reasons for a PET perfusion scan. Written informed consent for an additional CT scan was obtained from all patients before the study, which had been approved by the local ethics committee.
PET/CT Scanning
Images were acquired on a Discovery LS PET/CT scanner (GE Healthcare), an integration of an Advance NXi PET scanner with a LightSpeed Plus 4-row helical CT scanner.
The field of view for the multislice spiral CT angiographic study was localized by a scout scan from the carina to 1 cm below the inferoposterior wall of the heart. Afterward, a bolus of 15 mL of iopentol contrast agent (Imagopaque 300; Amersham Health) was injected intravenously and antecubitally at a speed of 3.5 mL/s, and after a delay of 10 s a sequence of 12 axial images was acquired. The interval between injection and peak enhancement in the aortic root was determined as transit time. All patients underwent contrast-enhanced CTA with 150 mL of contrast medium (3.5 mL/s) and simultaneous acquisition of 4 parallel slices. Images were acquired during a breath-hold after inspiration, and electrocardiography was recorded continuously.
This study was followed by a myocardial perfusion PET scan without moving the patient. All subjects received 700–900 MBq of 13N-ammonia into a peripheral vein by bolus injection while acquisition of the serial (9 × 10-s, 6 × 15-s, 3 × 20-s, 2 × 30-s, and 1 × 900-s frames) transaxial tomographic images of the heart was started and followed by a CT transmission scan for photon attenuation correction (17). After allowing for decay of the 13N, perfusion scanning was repeated during a standard infusion of intravenous adenosine at a rate of 0.14 mg/kg/min.
CT Image Reconstruction
CT raw data were reconstructed using a conventional multislice spiral CT algorithm. Cross-sectional images were then reconstructed at 1-mm intervals. Spiral data were collected from successive heartbeats by applying a filter function not only in the z direction (along the patients’ longitudinal axis) but also in the heart phase, using routine filtered backprojection for CT and applying retrospective electrocardiography gating. Several image sets were analyzed by moving the center of image acquisition from 60% toward the end of the cardiac cycle in increments of 10%. For each coronary artery, the dataset containing the fewest motion artifacts was chosen for further evaluation.
Image Fusion
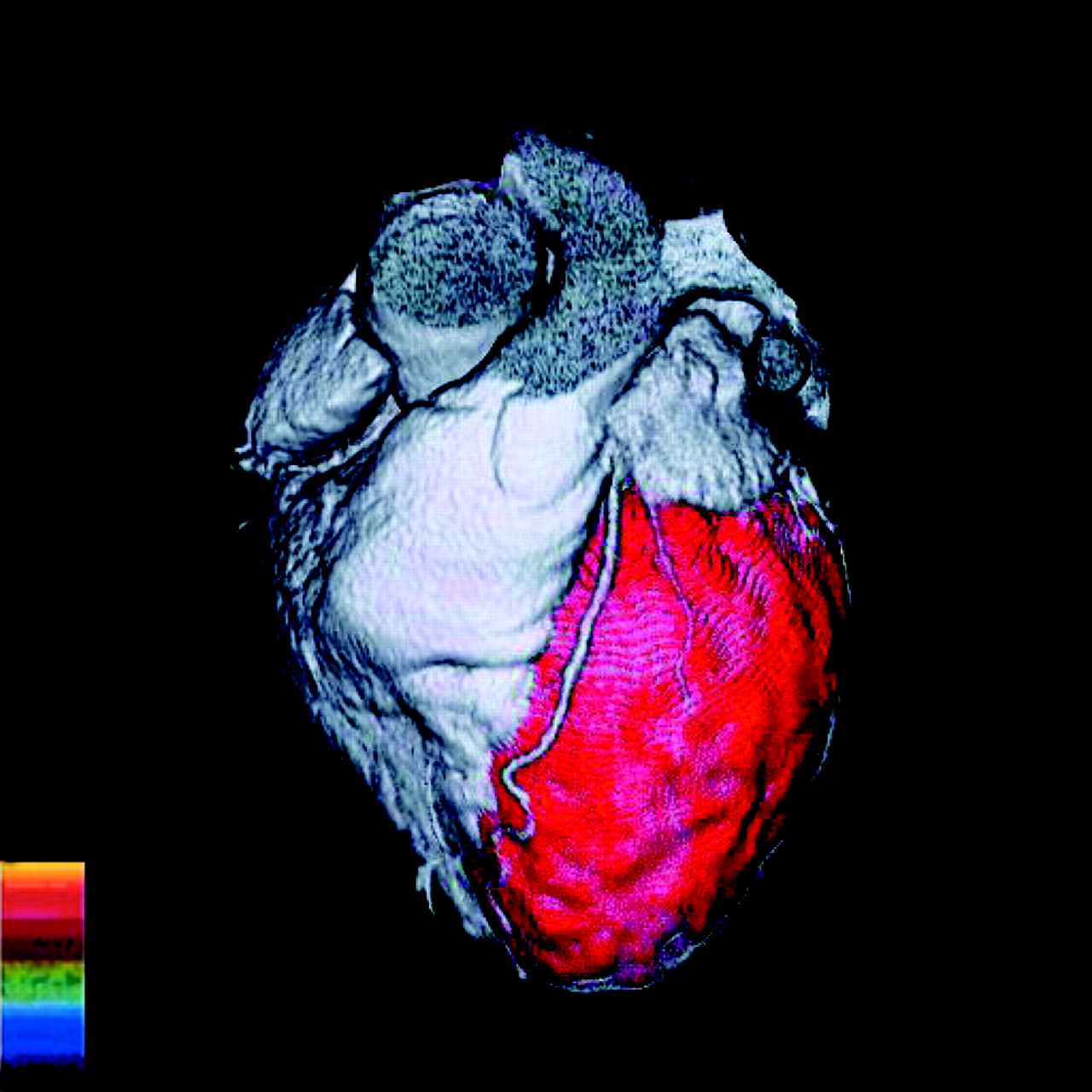
The CT images were segmented on an image-by-image basis to eliminate all structures that would obstruct the view of the coronary arteries (i.e., chest wall, pulmonary vessels, and atrial appendages). Three-dimensional reconstructions of the multislice spiral CT scans were performed using the Advantage Windows software package (version 4.1; GE Healthcare), providing the coronary artery tree and the shape of the heart. Onto the myocardial surface as visualized by CT, the color-coded qualitative perfusion images obtained by PET were superimposed (Fig. 1). The images of the last 900-s frame were used to assess ischemia. A reversible defect during adenosine infusion, disappearing at rest, was considered to represent ischemia (Fig. 2).
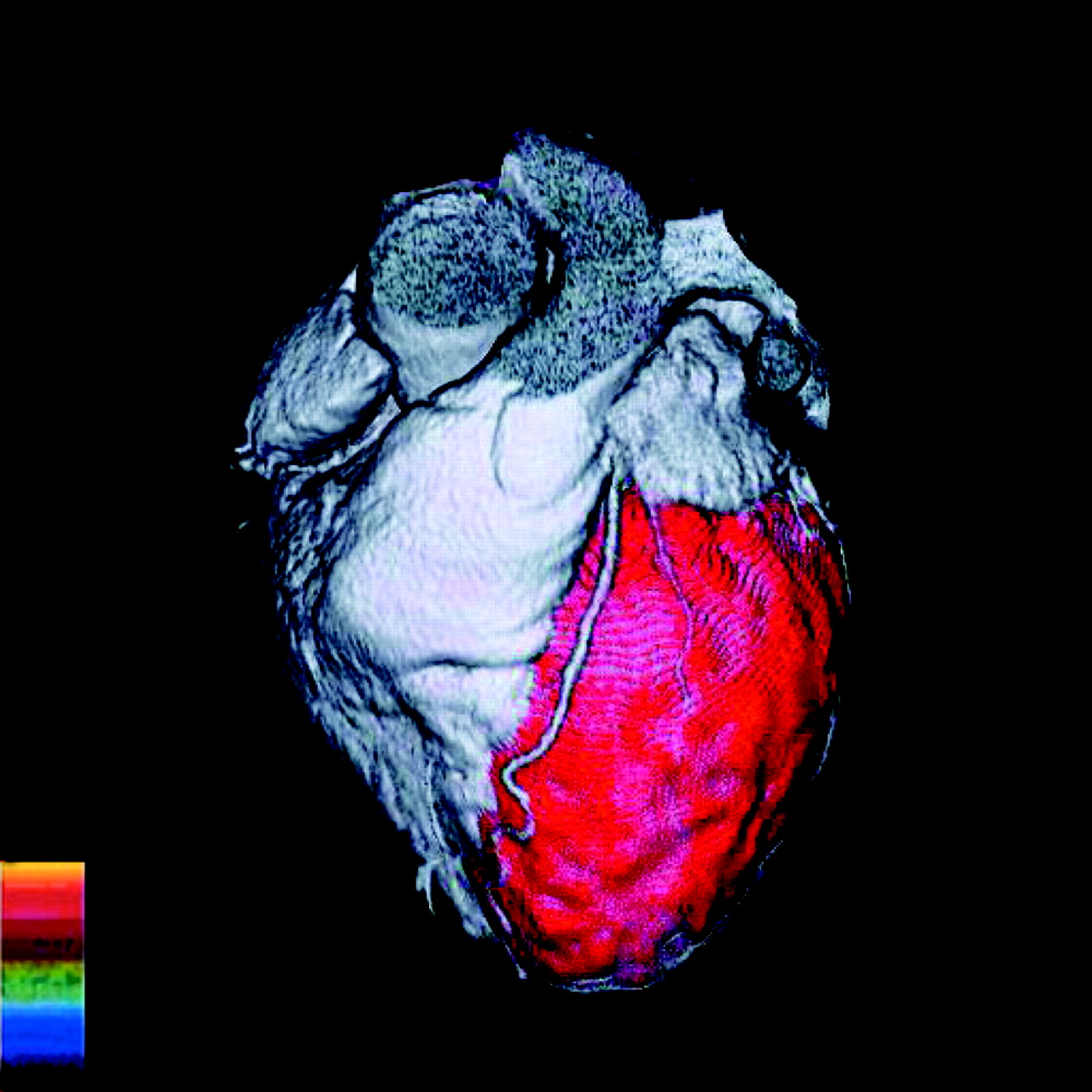
Three-dimensional reconstruction of multislice spiral CT scan showing coronary artery tree and shape of heart, superimposed by color-coded qualitative stress perfusion image obtained by PET. Ammonia has been used as perfusion tracer; red indicates normal stress perfusion response in anterior and lateral segments of left ventricle.
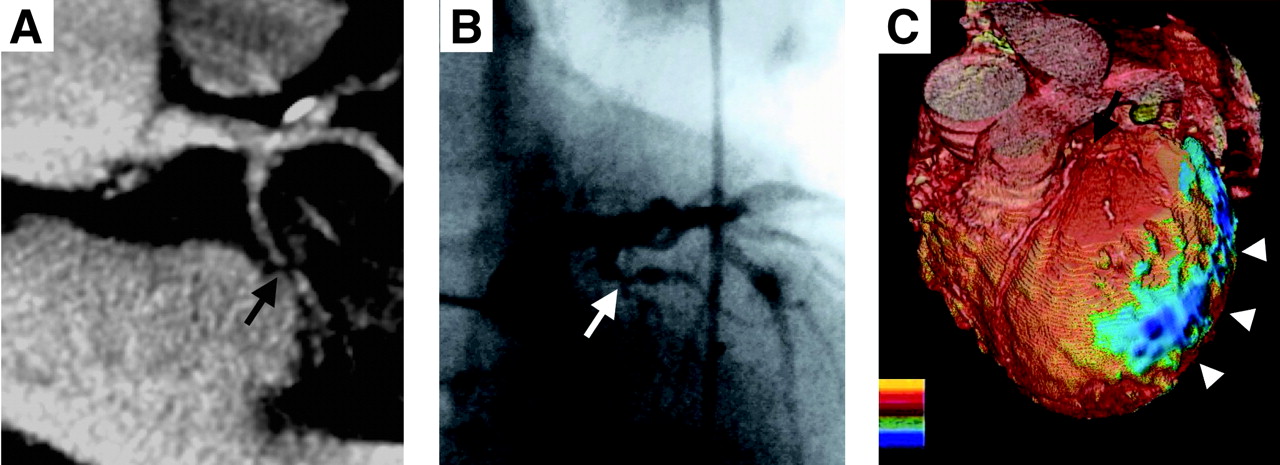
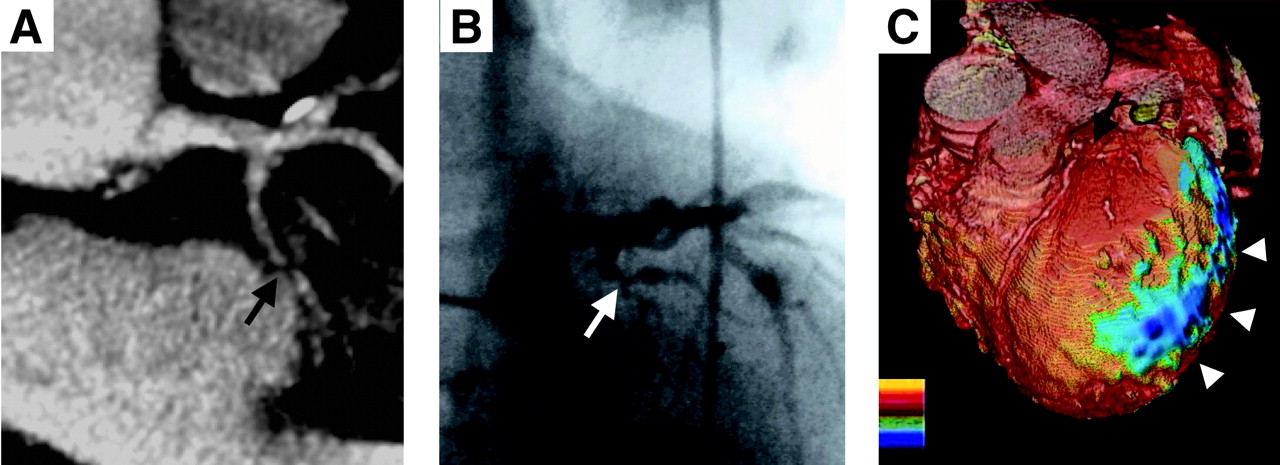
(A) Contrast-enhanced CT angiogram showing stenotic lesion in left circumflex coronary artery with faint poststenotic flow (arrow). (B) Coronary angiogram showing same stenotic lesion (arrow). (C) Combined 3-dimensional reconstruction of multislice spiral CT scan showing coronary artery tree and shape of heart, superimposed by color-coded qualitative stress perfusion image obtained by PET. Blue indicates reversible perfusion defect (i.e., ischemia). Lesion described in A and B is hemodynamically relevant, as documented by reduced hyperemic response to adenosine stress in lateral wall (arrowheads).
Data Interpretation
Using the contrast-enhanced CTA images, 2 readers visually categorized the major epicardial arteries and the bypass grafts as either being occluded/having a significant stenosis (>50% diameter stenosis equaling >75% area narrowing, and occlusions) or showing neither occlusion nor stenosis or being impossible to evaluate. We analyzed the left main, the left anterior descending (from 0 to 4 cm), the left circumflex (from 0 to 3 cm), and the right coronary (from 0 to 5 cm) arteries. Neither reader was aware of the coronary angiography findings. The clinical cardiologist analyzed the angiogram. To reflect daily clinical routine at our institution, we did not perform a separate analysis or quantitative coronary angiography.
Combined information on anatomy (coronary angiography or contrast-enhanced CTA) and perfusion (PET) was used in making decisions about revascularization or conservative treatment (Fig. 3). According to the respective guidelines (9,10), only the combination of significant stenosis plus evidence of ischemia (by PET) led the decision toward revascularization, whereas the combination of no stenosis plus no ischemia or stenosis without ischemia led the decision toward conservative treatment (Fig. 4). The results of the combined evaluation by PET plus coronary angiography served as the gold standard against which the combined evaluation by PET/CT was validated (Fig. 5).
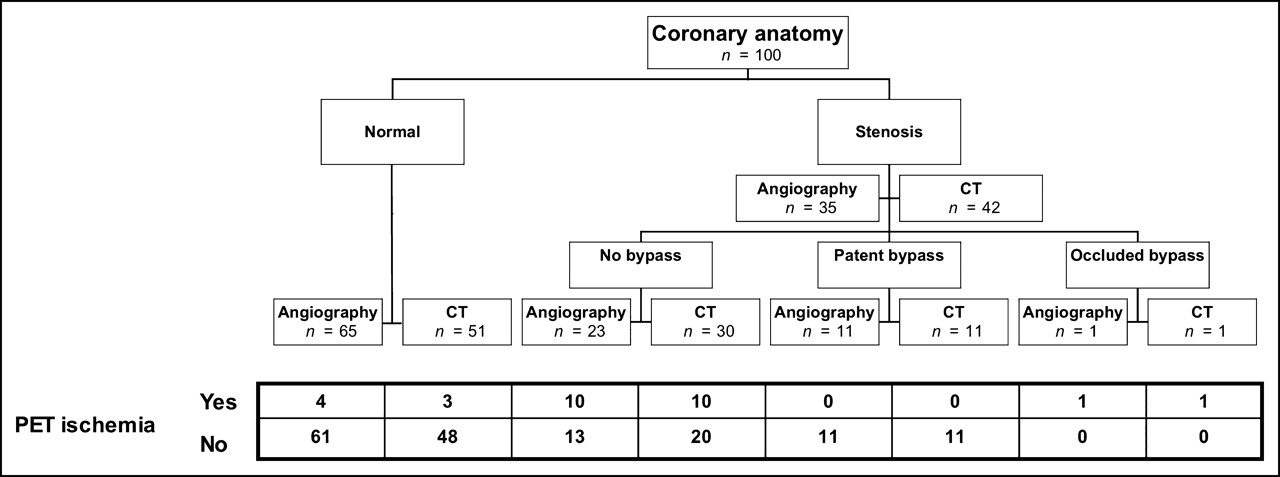
Overview of morphologic findings (angiography and CT) and functional findings (PET). For all territories subtended by normal or stenotic coronary vessels, categoric information on ischemia as assessed by PET is given.

Diagnostic algorithm for clinical decision making. Only the combination of angiographically significant stenosis and evidence of ischemia (by PET) led the decision toward revascularization. Angio = angiography.
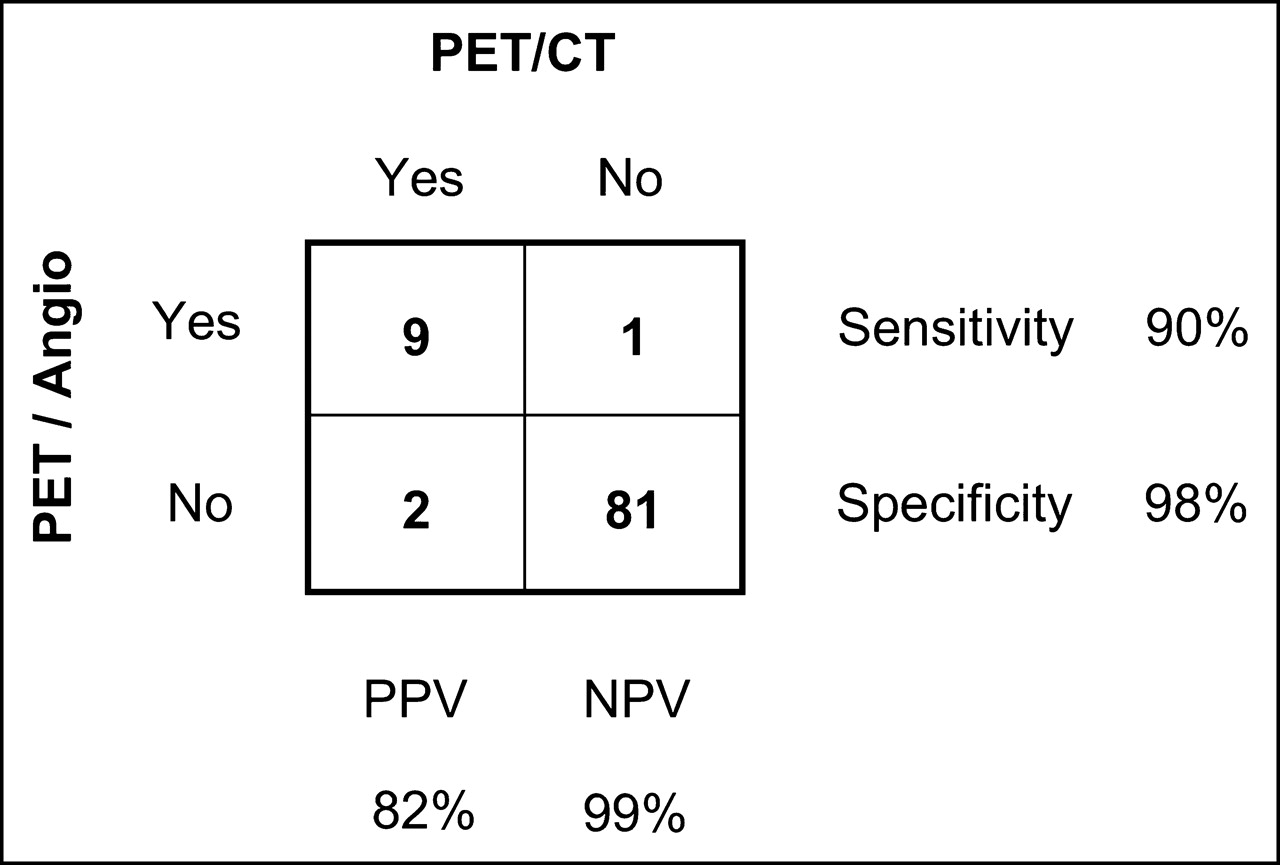
Clinical decision making according to findings of PET plus angiography (Angio) represents gold standard. Decisions made according to PET/CT findings were compared with gold standard. NPV = negative predictive value; PPV = positive predictive value.
RESULTS
In all patients, CTA and PET were performed without complications. The mean time needed for image acquisition by CT was 38 ± 15 s per patient, and an additional 15 min were required for all preparations before scanning. The time needed for PET was 2 × 20 min for emission plus 30 min in between to allow for decay of 13N. The mean heart rate was 68 ± 9 beats per minute. Because all patients were taking standard β-receptor antagonists, no additional β-receptor antagonists were administered to any patient during the study.
Contrast-Enhanced CTA Versus Coronary Angiography
Of the 100 coronary arteries (left main, left anterior descending, left circumflex, and right in 25 patients) and 12 bypass grafts, 7 segments (in 5 patients) were considered impossible to evaluate because of blurring (rapid vessel movement). The respective coronary artery territories, however, could successfully be evaluated using PET data.
After the 7% of segments that were not assessable by CT (left anterior descending, 4 times; left circumflex, 3 times) had been excluded from the primary analysis, contrast-enhanced CTA alone correctly detected the 1 substantial lesion of the left main coronary artery, 12 of the 14 lesions of the left anterior descending coronary artery, 7 of the 7 lesions of the left circumflex coronary artery, 7 of the 8 lesions of the right coronary artery, and the 1 bypass graft occlusion (sensitivity, 90%).
In the arteries that could be evaluated by CT angiography, the absence of significant lesions was correctly determined in 20 of 24 left main coronary arteries, in 8 of 11 left anterior descending coronary arteries, in 9 of 15 left circumflex coronary arteries, in 11 of 13 right coronary arteries, and in 12 of 12 patent bypass grafts (specificity, 75%). Most of the false-positive findings by CT were caused (at least in part) by artifacts due to calcifications, which are likely to affect contrast-enhanced CTA (performed with a 4-slice CT scanner) in a population with an average age of 62 y.
Combined Results: PET/CT Versus PET Plus Coronary Angiography
In 10 of the 13 patients with a history of myocardial infarction, PET documented a resting defect, which was located in the territory of an occluded artery in 9 patients and in the territory of a vessel with a high-grade stenosis in 1 patient. CT revealed the lesion in all of these patients. Furthermore, the location of the stress-induced perfusion defects corresponded to the site of the coronary stenosis as identified by CT angiography. The 3-dimensional volume–rendered view appeared particularly helpful for correlating the location of the lesion with the corresponding defect (Fig. 2).
Interestingly, for 13 of 23 lesions documented by coronary angiography and contrast-enhanced CTA, PET revealed no ischemia, providing no indication for revascularization. In addition, contrast-enhanced CTA found 7 false-positive lesions, which, however, were correctly assigned to “no revascularization” when the PET information was added (Fig. 4). The combination of PET plus coronary angiography classified 11 lesions as requiring, and 89 as not requiring, revascularization according to the predefined gold standard (i.e., anatomic lesion plus ischemia). For PET/CT, these numbers were 11 (sensitivity, 90%) and 82 (specificity, 98%), respectively. Positive and negative predictive values were 82% and 99%, respectively, resulting in an accuracy of 97% (Fig. 5). Table 1 compares the contrast-enhanced CTA findings with the CT findings and stress perfusion defects. As summarized in Figure 4, 10 segments had ischemia subtended by a stenotic coronary artery. Four of these had a proximal coronary lesion and a large stress perfusion defect, whereas 6 had a distal lesion and a small perfusion defect. Thirteen segments had a stenotic lesion documented by invasive angiography but no corresponding ischemia. Most of these false-negative PET findings occurred in patients with multivessel disease, a fact that may have contributed to the false-negative findings.
Comparison of Contrast-Enhanced CTA Findings with CT Findings and Stress Perfusion Defects
DISCUSSION
We have demonstrated the feasibility and accuracy of combined PET/CT for visualization of coronary anatomy with simultaneous assessment of the functional significance of lesion severity by means of rest/stress PET perfusion scanning. Although angiography is the accepted standard for morphologic assessment of CAD, it represents no gold standard for myocardial perfusion (6,7). Large trials have shown that angiography cannot predict the recurrence of ischemia or reocclusion in patients after thrombolysis (18–21). Therefore, it has become clinical standard to require proof of ischemia by a noninvasive test before considering revascularization procedures (9,10). Accordingly, in our study only the 11 angiographically documented lesions with ischemia in the subtended myocardial territories confirmed by PET were considered for revascularization. By contrast, the 89 segments with either no stenosis or no ischemia or a combination of both did not qualify for revascularization. Eighty-two of these segments were correctly classified by PET/CT toward no revascularization, indicating that an invasive diagnostic procedure could have been avoided. In the present study, 91 of 93 evaluated lesions were correctly classified with the entirely noninvasive PET/CT approach with a sensitivity and specificity of 90% and 98%, respectively. Thus, the noninvasive CAD evaluation by PET/CT seems to allow accurate clinical decision making (accuracy, 97%) without the need for invasive diagnostic procedures.
Previous studies either have concentrated on patients without coronary stenoses or have included a large share of patients without coronary stenoses (16,22). In view of this, the high negative predictive value despite the high pretest probability in our study population is particularly remarkable with regard to a potential future role of PET/CT as a screening test, that is, in an intermediate-pretest-probability population. In addition, all 7 false-positive lesions and the 7 coronaries that were not amenable to an evaluation by contrast-enhanced CTA because of motion artifacts were correctly classified after the PET information had been included. This synergistic effect further substantiates the great clinical benefit of integrated PET/CT. Contrast-enhanced CTA artifacts due to rapid coronary artery motion are a well-known shortcoming of multislice spiral CT (23–25) but can—at least in part—be outweighed by the information gained from the simultaneous PET scan.
The benefit of simultaneous noninvasive assessment of coronary anatomy and myocardial perfusion seems to lie in a substantially improved diagnostic confidence in deciding on the best therapeutic strategy. Elective interventional therapy can be planned carefully, contributing to avoid overuse of angioplasty and stent placement. This is extremely relevant, because overuse of expensive intravascular stents is a key driver of cost in invasive cardiology practice. When lesion anatomy appears unsuitable for angioplasty, bypass grafting can be considered directly without the need for further preoperative diagnostic coronary angiography, provided the contrast-enhanced CTA images are of adequate quality.
The present study had several shortcomings, which were mainly technical. The type of CT scanner used has been shown unable to produce consistently high-quality contrast-enhanced CTA images in most hands. However, the latest developments of multislice CT—faster gantry rotation speeds of 16 and more slices—will substantially improve image quality, specifically at higher heart rates (26). In addition, technical innovations will allow reduction of the radiation dose. The radiation dose of a CT scan has been extensively studied and was recently confirmed to be about 7 mSv by Nieman et al. (26). We did not measure the radiation dose in our imaging protocol, but as the scans are additive, one can readily calculate the total dose to be 7 mSv (contrast-enhanced CTA) + 2 × 1 mSv (PET scan) + 0.3 mSv (CT transmission scan) = 10–12 mSv, which is comparable to values found with invasive coronary angiography (3–10 mSv) (27). This radiation dose is still acceptable, considering the fact that many serial CT scans may have radiation doses as high as 20–30 mSv.
The relatively long breath-hold required constitutes another limitation. Because all our patients were receiving long-term β-receptor antagonist treatment, heart rate was relatively low, although medication was withheld for the day of the study and we did not administer β-receptor antagonists for heart rate control because of the possible effect on the adenosine-stress perfusion PET scan.
A major limitation of the present study was the small number of patients included. The patients were few because the study was designed to assess the feasibility of combined PET/CT, rather than its impact on clinical decision making.
CONCLUSION
Combination of myocardial perfusion PET and multislice spiral contrast-enhanced CTA is a feasible and interesting approach for noninvasive complementary evaluation of morphologic and functional CAD. Besides being a noninvasive alternative, the PET/CT technique adds functional information on the pathophysiologic impact of a lesion, allowing accurate clinical decision making on the best therapeutic strategy. Certainly, the present findings must be considered preliminary in view of the small number of patients in this initial study. Therefore, firm conclusions about a potential role for integrated cardiac PET/CT in clinical decision making cannot be drawn from our results but must await further confirmation in larger trials. The encouraging results of this investigation, however, seem to justify further efforts to improve the accuracy of PET/CT for the detection of CAD by implementing higher-performance multislice spiral CT scanners into PET/CT hybrids. Such technical refinements may accelerate the clinical implementation of PET/CT.
Acknowledgments
This study was funded by a grant from the Swiss National Science Foundation (SNSF-professorship grants PP00A-68835 and 31-68386), from GE Healthcare, and from Amersham Health, Medical Diagnostics Europe. Mehdi Namdar and Thomas F. Hany contributed equally to this study.
Footnotes
Received Sep. 3, 2004; revision accepted Feb. 26, 2005.
For correspondence or reprints contact: Philipp A. Kaufmann, MD, Nuclear Cardiology Section, Cardiovascular Center NUK C 32, University Hospital, Raemistrasse 100, CH-8091 Zurich, Switzerland.
E-mail: pak{at}usz.ch
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Hybrid Imaging Using Quantitative H215O PET and CT-Based Coronary Angiography for the Detection of Coronary Artery Disease
- Diagnostic Performance of Noninvasive Myocardial Perfusion Imaging Using Single-Photon Emission Computed Tomography, Cardiac Magnetic Resonance, and Positron Emission Tomography Imaging for the Detection of Obstructive Coronary Artery Disease: A Meta-Analysis
- Image Fusion: Is It Merely the Blending of Pretty Pictures?
- Nuclear Myocardial Perfusion Imaging with a Cadmium-Zinc-Telluride Detector Technique: Optimized Protocol for Scan Time Reduction
- Integrated positron emission tomography/computed tomography (PET/CT) in coronary disease
- Detection of inflammation in patients with acute aortic syndrome: comparison of FDG-PET/CT imaging and serological markers of inflammation
- SPECT/CT
- Noninvasive Cardiac Imaging with Computed Tomography
- Cardiac Image Fusion from Stand-Alone SPECT and CT: Clinical Experience
- Integrated Single-Photon Emission Computed Tomography and Computed Tomography Coronary Angiography for the Assessment of Hemodynamically Significant Coronary Artery Lesions
- Anatomic-Functional Imaging by Single-Photon Emission Computed Tomography/Computed Tomography as the Cornerstone of Diagnosis and Treatment for Coronary Patients: A Glimpse Into the (Near) Future?
- Diagnostic and clinical perspectives of fusion imaging in cardiology: is the total greater than the sum of its parts?
- Noninvasive Characterization of Myocardial Molecular Interventions by Integrated Positron Emission Tomography and Computed Tomography
- Comparison of 64-Slice CT with Gated SPECT for Evaluation of Left Ventricular Function
- Quantification of Subendocardial and Subepicardial Blood Flow Using 15O-Labeled Water and PET: Experimental Validation
- Validation of 18F-Fluoro-4-Thia-Palmitate as a PET Probe for Myocardial Fatty Acid Oxidation: Effects of Hypoxia and Composition of Exogenous Fatty Acids
- PET/CT: Challenge for Nuclear Cardiology
- The Diagnosis of Coronary Artery Disease: In Search of a "One-Stop Shop"?