


Abstract
In view of the commercial success of integrated PET/CT scanners, there is an increasing interest in comparable SPECT/CT systems. SPECT in combination with CT enables a direct correlation of anatomic information and functional information, resulting in better localization and definition of scintigraphic findings. Besides anatomic referencing, the added value of CT coregistration is based on the attenuation correction capabilities of CT. The number of clinical studies is limited, but pilot studies have indicated a higher specificity and a significant reduction in indeterminate findings. The superiority of SPECT/CT over planar imaging or SPECT has been demonstrated in bone scintigraphy, somatostatin receptor scintigraphy, parathyroid scintigraphy, and adrenal gland scintigraphy. Also, rates of detection of sentinel nodes by biopsy can be increased with SPECT/CT. This review highlights recent technical developments in integrated SPECT/CT systems and summarizes the current literature on potential clinical uses and future directions for SPECT/CT in cardiac, neurologic, and oncologic applications.
Hybrid imaging techniques allow the direct fusion of morphologic information and functional information. Since its introduction to clinical medicine in 2001, PET/CT has become the fastest growing imaging modality (1,2). CT coregistration has led to definite diagnoses by PET and more acceptance of functional imaging. Recently, integrated SPECT/CT scanners have been made available. With SPECT/CT, lesions visualized by functional imaging can be correlated with anatomic structures. The addition of anatomic information increases the sensitivity as well as the specificity of scintigraphic findings (Fig. 1). SPECT/CT has an additional value in sentinel lymph node (SLN) mapping, especially in head and neck tumors and tumors draining into pelvic nodes. In addition to improved anatomic localization of scintigraphic findings, SPECT/CT offers the opportunity to add true diagnostic information derived from CT imaging. Given the growing number of studies demonstrating the added value of hybrid SPECT/CT relative to single imaging modalities, it appears likely that this promising technique will play an increasingly important role in clinical practice. The broad spectrum of existing SPECT tracers and their widespread availability suggest that SPECT/CT can be complementary to PET/CT.
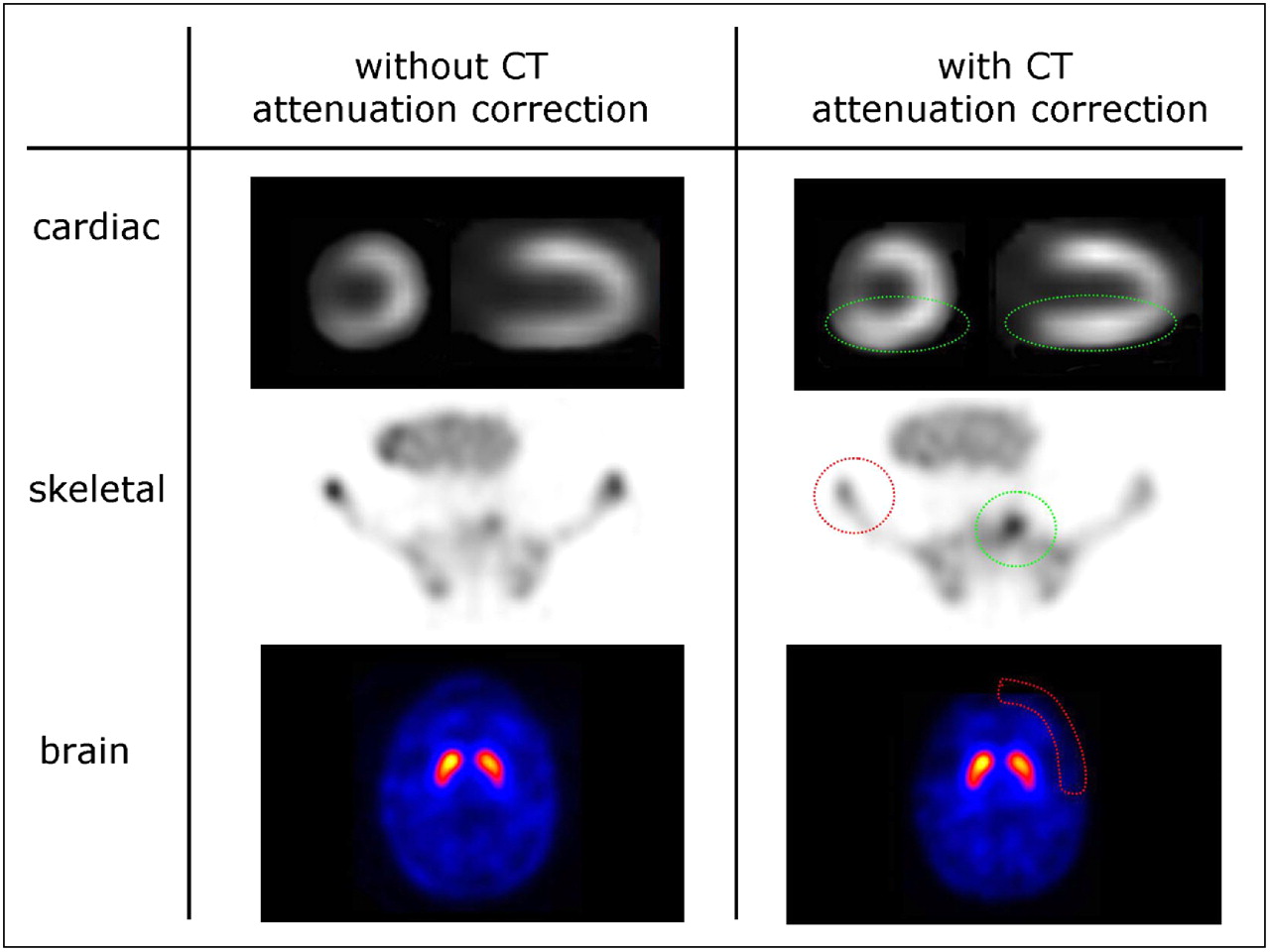
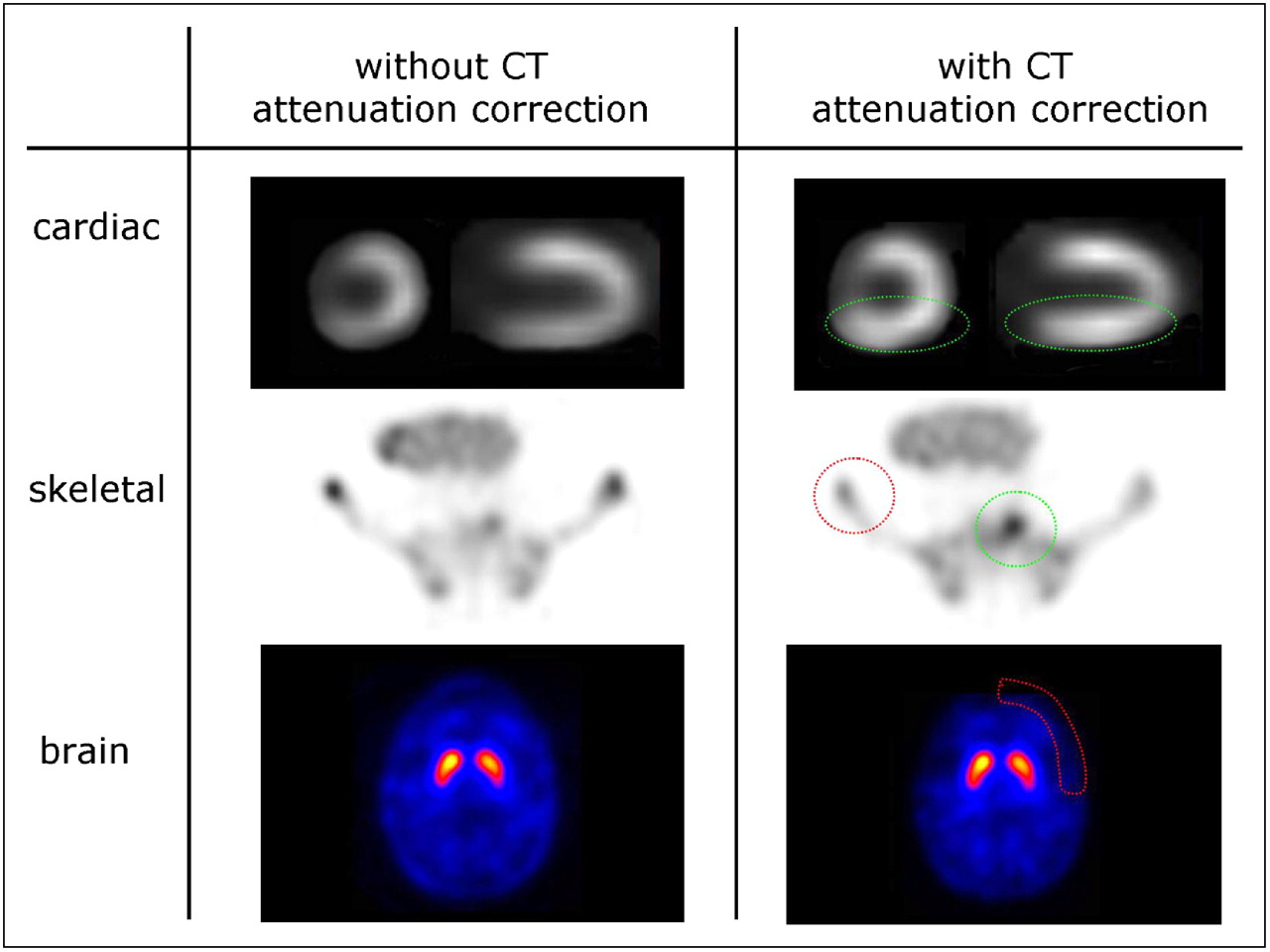
Impact of CT attenuation correction. Upper row (myocardial perfusion scintigraphy) shows attenuation of 99mTc-MIBI uptake in inferior myocardium. CT-corrected image demonstrates normal perfusion of inferior myocardium (green circles). Middle row (skeletal scintigraphy with 99mTc-hydroxymethylene diphosphonate) shows superior localization of bone metastasis in os sacrum (green circle) after CT attenuation correction. Lower row shows CT attenuation correction of brain study (99mTc-iodobenzamide SPECT). Without CT attenuation correction, background activity may be overestimated, especially in peripheral structures (red circles) and may appear with similar intensity as pathologic findings (e.g., skeletal scintigraphy, middle row).
TECHNICAL ASPECTS OF SPECT/CT
Before the introduction of dedicated SPECT/CT cameras, various software algorithms were established to allow image fusion for anatomic imaging (CT or MRI) and functional imaging (SPECT) (3). In the early 1980s, efforts were made to allow image fusion in brain studies. Current software algorithms permit highly accurate coregistration of anatomic and functional datasets. This kind of nonrigid image coregistration is therefore a regular component in daily clinical practice, such as image-guided surgery or radiation treatment planning. However, motion artifacts markedly affect image fusion in the thorax, abdomen, pelvis, or head and neck region when CT and SPECT acquisitions are obtained separately (4,5). Functional images of the thorax or the abdomen contain little or no anatomic landmarks that can be correlated with anatomic reference points. Moreover, the chest and the abdomen do not represent rigid structures. Differences in patient positioning and respiratory motion make the correct alignment of anatomic and functional images even more complicated. More recently, 3-dimensional elastic transformations or nonlinear warping has been established to further improve the accuracy of image fusion. With these modern approaches, the accuracy of software-based image coregistration is in the range of approximately 5–7 mm (6). Although software algorithms are not in widespread clinical use for image coregistration of the abdomen or the thorax, this technology will still play an important role by allowing the correction of misregistrations attributable to patient motion or breathing artifacts, which may also arise from integrated SPECT/CT cameras.
Initial work was done by Hasegawa et al., who introduced a system that is capable of simultaneous CT and SPECT acquisitions (7). This group was the first to demonstrate that CT data can be used for attenuation correction, allowing superior quantification of radiotracer uptake. This technology translated into the first commercial SPECT/CT system, Hawkeye, which was introduced by GE Healthcare (8). Here, the modalities are combined, allowing sequential CT and SPECT acquisitions with only an axial shift of the patient between measurements. An enhanced version developed by GE Healthcare contained a 4-row multidetector CT capable of acquiring four 5-mm slices instead of one 10-mm slice. Philips combined a 6- or 16-slice CT scanner with a Skylight double-head camera system (Precedence). Philips also introduced a system for scientific purposes combining SPECT with 64-slice CT. Siemens Medical Solutions combined an E-Cam dual-detector γ-camera system with optional 1-, 2-, or 6-slice CT. With both systems, slice thickness can be adjusted from 0.6 to 10 mm, and the scan speed is <30 s for a 40-cm axial field of view. With the availability of coregistered CT information for the patient, methods that include spatially dependent collimator deblurring become feasible (9). Algorithms that combine this approach with attenuation on scatter correction (both based on CT information) have been implemented in SPECT/CT systems and may enable quantitative SPECT (10).
SUGGESTED PROTOCOLS FOR SPECT/CT
Although planar imaging and SPECT are routinely performed studies and respective protocols have been documented for various clinical settings, the roles of CT coregistration and specific imaging protocols have not yet been clearly defined. In general, instead of standard protocols, combined SPECT/CT procedures should be selected on an individual basis and should reflect clinical needs. The radiation dose delivered by CT is a major issue in this regard, because diagnostic CT can increase the overall radiation dose by up to 14 mSv (11). Low-dose CT is associated with relatively low radiation doses of 1–4 mSv and should be sufficient for anatomic referencing of SPECT lesions and attenuation correction (Table 1). Usually, if a recent contrast-enhanced diagnostic CT scan is available, there is no need to perform another contrast-enhanced CT scan during SPECT/CT. Also, when SPECT/CT is performed for treatment monitoring and follow-up, low-dose CT should be sufficient. Therefore, the use of low-dose, nonenhanced spiral CT can be recommended in most cases when SPECT/CT is performed for anatomic referencing or attenuation correction. The standard protocol for integrated SPECT/CT at our institution (Siemens Symbia 6) is shown in Table 1.
Suggested CT Protocols* for Inclusion in Noncardiac SPECT/CT Protocols
When SPECT/CT is performed for tumor staging or restaging, the detection of small pulmonary nodules that may be negative on functional imaging is important. Therefore, the acquisition of an additional low-dose CT scan of the thorax during maximal inspiration should be considered for patients at risk for the presence of lung metastases (Table 1). This strategy applies especially to patients who have high-risk differentiated thyroid cancer and are undergoing radioiodine scintigraphy. In this setting, an additional 40-mA low-dose CT scan acquired during inspiration is a feasible approach, because it has been demonstrated that a reduction of the tube current to 40 mA results in satisfactory image quality and reduces overall radiation exposure (11).
Compared with PET/CT, diagnostic CT protocols including intravenous or oral contrast agent enhancement are seldom performed at SPECT/CT but may be appropriate in certain clinical situations (Tables 1 and 2). These protocols will have to be implemented and modified continually, especially with the availability of new scanners offering very high spatial resolution (64-slice CT). Potential CT protocols suitable for cardiac imaging are discussed later (Table 2).
Suggested CT Protocols for Inclusion in Cardiac SPECT/CT Protocols
SPECT/CT FOR SLN MAPPING
For patients with cancer, accurate lymph node staging is mandatory for appropriate treatment planning. A combination of lymphoscintigraphy before surgery and mapping with blue dye during surgery has been demonstrated to be a practicable approach for accurately localizing the SLN. Although most sentinel nodes can be identified during surgery with a hand-held probe, SLN identification may be impossible in certain cases. Localization with CT coregistration before surgery may facilitate surgical access and thus improve overall detection rates. The added value of CT coregistration for SLN mapping has been demonstrated by several groups. Although inguinal and lower axillary nodes can be reliably detected on planar scintigrams, anatomic coregistration represents a valuable tool for SLN detection in the pelvis, the mediastinum, or the head and neck region. For patients with melanoma of the head and neck or the trunk, a pilot study indicated that SPECT/CT enabled the detection of sentinel nodes in up to 43% of patients with negative planar scintigrams (12). For patients with early-stage cervical cancer (13) and invasive bladder cancer (14), better detection of sentinel nodes by SPECT/CT than by planar scintigrams was described. The CT portion of the examination was especially helpful for the identification of SLNs during surgery. For 20 patients with head and neck cancer, Khafif et al. reported a sensitivity of SPECT/CT of 87.5% (15). SPECT/CT further improved SLN identification and localization over those provided by planar images for 6 patients (30%). For a series of 34 patients, SPECT/CT identified sentinel nodes in 94% of patients (32/34) and identified additional nodes in 15 (47%) of those 32 patients (16). More accurate localization of SLNs in oral cavity squamous cell carcinoma was described by Keski-Santti et al. (17). Superior topographic SLN identification was described in 2 further studies of head and neck cancer or melanoma (12,18).
Husarik and Steinert examined the added value of SPECT/CT in breast cancer (Fig. 2) (19). For 41 consecutive patients, findings from planar scintigrams and SPECT/CT were identical in only 7 patients (17%); SPECT/CT indicated the correct anatomic localization in 29 patients (70%), according to the American Joint Committee on Cancer staging system (levels I–III). For 6 patients, additional SLNs were detected. For 26 patients (63%), exact anatomic localization could be derived exclusively from SPECT/CT; 3 sentinel nodes close to the injection site were not detected by SPECT but could be clearly visualized by SPECT/CT. Similar findings were described earlier by Lerman et al. (20). For 157 consecutive patients, 13% of sentinel nodes were visualized by SPECT/CT but not on planar scintigrams. Unexpected sites of drainage and non–node-related hot spots were identified for 33 patients. For a prospective series of 51 patients, sentinel nodes could be assigned to axillary levels I–III on the basis of SPECT/CT data but not on the basis of planar images (21). In a pilot study by van der Ploeg et al., SPECT/CT was superior to SPECT for SLN detection; for 4 of 31 patients, 6 additional SLNs were detected by SPECT/CT, leading to a change in management for 5% of patients because of upstaging in the axilla (22). SPECT/CT has been shown to be especially useful in overweight patients. In a prospective study of 220 patients with breast cancer, 122 patients had a body mass index of greater than 25 (23). For 49 patients (22%), planar images failed to identify a sentinel node. However, for 29 of these 49 patients (59%), sentinel nodes could be identified by SPECT/CT. Overall, the sensitivity of SPECT/CT in overweight patients was 89%. SPECT/CT was also superior to blue dye labeling during surgery and identified sentinel nodes in 75% of patients in whom the blue dye technique failed to detect sentinel nodes. Although the current literature does not indicate a major role for SPECT/CT in SLN identification in breast cancer, this modality may be helpful when the standard approach fails to identify the SLN.

Accurate anatomic localization of sentinel node in patient with breast cancer by sentinel node scintigraphy (99mTc-Nanocoll; Amersham) and CT coregistration. Correct anatomic localization of sentinel node in left axilla is illustrated by 3-dimensional projections of fused images.
SPECT/CT IN SKELETAL DISEASES
For more than 30 y, planar bone scintigraphy has been used as a valuable method for sensitively detecting or characterizing focal bone pathology; more recently, SPECT has been used in this capacity (24). Although functional bone imaging is a highly sensitive method, it lacks specificity (25). Therefore, radiography, CT, or MRI is frequently performed after bone scintigraphy to further characterize lesions evident on bone scans. Integrated SPECT/CT offers a direct correlation of focal bone pathology with anatomic structures and therefore minimizes the number of equivocal findings.
Applications in Malignant Skeletal Diseases
Screening for bone metastases and evaluation of the treatment response are the most frequent indications for bone scanning. Although the majority of bone metastases appear as hot spots, some appear as cold lesions. Benign lesions, such as hemangioma, may also appear as cold, making the differential diagnosis problematic. The differentiation of benign and malignant lesions can usually be achieved with CT coregistration and is a major advantage of SPECT/CT (Fig. 3). In addition, fused images can be used to further guide biopsies of bone lesions.

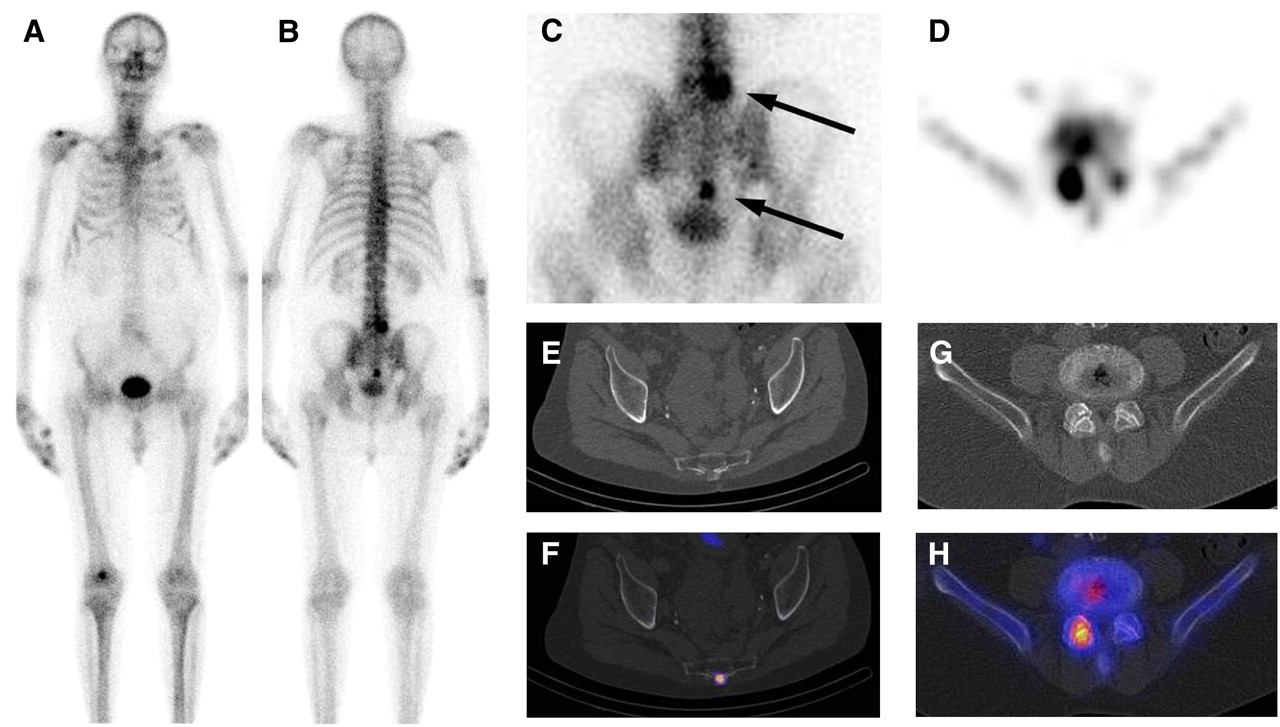
Patient with lung cancer and 2 hot spots, in lower lumbar spine and pelvis (os sacrum). (A and B) Planar scintigrams from skeletal scintigraphy (99mTc-hydroxymethylene diphosphonate). (C) Detailed view of pelvis with 2 hot spots (arrows). (D) Transverse section of upper lesion in lumbar vertebra 5. (E) Small osteolytic lesion with intense tracer uptake indicating bone metastasis in lower pelvis. (F) Fused image. (G and H) Spondylarthrosis of right facet joint with intense tracer uptake indicating degenerative lesion.
A normal tracer distribution on planar bone scans usually makes the use of SPECT/CT unnecessary. Although in many cases the correct diagnosis can be derived from planar bone scans, SPECT/CT is necessary to make the correct diagnosis in cases of undefined lesions. In particular, scintigraphic lesions in the spine or pelvis frequently may not be defined exactly, requiring the additional use of CT or MRI. Recently, image coregistration was demonstrated to be superior to planar radiographic techniques or SPECT and proved useful in further characterizing benign skeletal abnormalities. The presence of accompanying complications, such as fractures or compression of the spinal cord, can also be diagnosed in a single examination (26).
The first report demonstrating the superiority of SPECT/CT over planar imaging or SPECT was published by Römer et al. (27). In this retrospective study, SPECT-guided CT was reported to clarify more than 90% of bone lesions that were indeterminate at SPECT: 63% of indeterminate findings could be definitely assigned as benign lesions involving mostly osteochondrosis, spondylosis, or spondylarthrosis of the spine; 29% of lesions could be clearly assigned as osteolytic or osteosclerotic bone metastases; and 4 lesions (8%) remained indeterminate at SPECT/CT because of a missing anatomic correlate. The majority of these lesions were located in the ribs or scapula. Because the performance of MRI in the thorax is affected by motion artifacts, the authors concluded that even MRI might not be able to confirm or exclude bone metastases in such lesions. The study also indicated that exact matching of functional and anatomic data may be necessary, especially in small anatomic structures. Small osteolytic bone metastases were observed in close proximity to facet joints, potentially causing misinterpretation of lesions at SPECT. The concept of Römer et al. (27) included the use of SPECT data for determination of the field of view for CT, resulting in reduced additional radiation exposure. On a per-patient basis, the mean radiation exposure from additional CT was as low as 2.3 mSv. SPECT-guided CT therefore results in acceptable overall radiation exposure. The use of CT data for attenuation correction may also increase the performance of SPECT, but this issue has not been studied in detail (28,29).
Using a combination of a dual-head SPECT camera and a nondiagnostic low-dose CT scanner, Horger et al. were also able to correctly classify 85% of unclear foci; in comparison, 36% of such foci were correctly classified by SPECT alone (30). Integrated SPECT/CT also seems to be superior to side-by-side reading of SPECT and CT images. Using juxtaposed CT and SPECT scanners, Utsunomiya et al. demonstrated that fused images were superior to side-by-side reading for the differentiation of malignant from benign lesions (31).
Applications in Benign Skeletal and Infectious Diseases
Even-Sapir et al. reported recently that SPECT/CT allowed a definite diagnosis for the majority of indeterminate scintigraphic findings in nononcologic situations (32). Infectious bone lesions, such as osteomyelitis, may be diagnosed by 3-phase bone scintigraphy with 99mTc-labeled diphosphonates. This approach has high sensitivity but lacks specificity. Another option is the use of radiolabeled autologous leukocytes (WBC), still considered the gold standard for localizing an area of infection by scintigraphic procedures. A more practicable approach is the use of 99mTc-labeled monoclonal antigranulocyte antibodies directed against the CD66 antigen, which is expressed on granulocytes and macrophages. 99mTc-labeled ciprofloxacin was recently suggested to specifically detect infection through the accumulation of the radiotracer in living bacteria. CT coregistration may improve the specificity as well as the sensitivity of these scintigraphic techniques. CT is able to detect small areas of cortical destruction and to identify soft-tissue abscesses or empyema located in neighboring soft-tissue structures. CT data can be correlated with the accumulation of granulocytes or increased bone turnover, as indicated by scintigraphy, thus confirming or excluding infectious bone lesions. It is obvious that combined imaging makes the interpretation of SPECT and CT easier and more reliable.
The added value of SPECT/CT for diagnosing infections has been demonstrated by several authors (33–40). Bar-Shalom et al. recently evaluated the role of SPECT/CT in the diagnosis and localization of infections by using 67Ga- or 111In-labeled WBC (33). The patients examined had fever of unknown origin and suspected osteomyelitis, soft-tissue infection, or vascular graft infection. SPECT/CT provided additional information for the diagnosis and localization of infections in 48% of patients (39/82). For 4 patients with physiologic bowel uptake, SPECT/CT allowed the exclusion of infection, and the diagnosis based on SPECT/CT was incorrect in 2 other patients. The authors concluded that SPECT/CT with 67Ga- or 111In-labeled WBC made an incremental contribution to scintigraphy by improving the diagnosis, localization, or definition of the extent of disease. Another study evaluated the performance of SPECT/CT in 28 patients with suspected bone infection or infection of orthopedic implants. WBC planar scanning or SPECT accurately detected infections in 18 of 28 patients, with true-negative results in 10 of 28 patients; SPECT/CT provided accurate anatomic localization for all lesions. There was a significant clinical contribution of SPECT/CT in 36% of patients. For patients with osteomyelitis, SPECT/CT was also able to differentiate soft-tissue from bone involvement and allowed the correct diagnosis of osteomyelitis in patients with structural tissue alterations attributable to trauma. The superiority of SPECT/CT with 111In-labeled WBC over side-by-side reading of SPECT and CT images was also suggested by a recent pilot study (36).
The added value of integrated SPECT/CT relative to triple-phase bone scintigraphy was evaluated by Horger et al. (35). For 31 patients with pathologic results from a triple-phase bone scan, the sensitivity and the specificity of SPECT/CT were 78% and 86%; those of SPECT and planar imaging were 78% and 50%, respectively. However, a combination of SPECT and separately performed MRI, radiography, or CT returned the highest sensitivity. SPECT/CT avoided false-positive findings and reduced the number of equivocal findings, but an additional benefit beyond the benefits of separately performed imaging modalities has not been demonstrated.
SPECT/CT IN DIFFERENTIATED THYROID CANCER
In patients with differentiated thyroid carcinoma, whole-body imaging after oral administration of 131I or 123I is commonly performed to identify residual or metastatic disease. 131I scintigraphy has a higher sensitivity than morphologically based imaging modalities. However, the interpretation of 131I images may be difficult because of the absence of anatomic landmarks. Therefore, precise localization of hot spots is frequently not possible. In addition, physiologic uptake of 131I may cause false-positive findings (Fig. 4). Integrated SPECT/CT potentially allows the differentiation of physiologic, artificial, and pathologic uptake of 131I (41). In a retrospective study by Tharp et al., SPECT/CT had an incremental diagnostic value for 41 of 71 patients (58%) (42). In particular, in the neck region, SPECT/CT allowed the precise characterization of equivocal lesions for 14 of 17 patients and changed the lesion location for 5 patients. SPECT/CT also improved the characterization of indeterminate findings as definitely benign in 13% of patients (9/71) and the precise assignment of metastases to the skeleton in 17% of patients (12/71) and to the lungs versus the mediastinum in 7% of patients (5/71). SPECT/CT further optimized the assignment of 131I uptake to lymph node metastases versus remnant thyroid tissue and to lung versus mediastinal metastases. Overall, additional findings at SPECT/CT had an impact on management for 41% of patients.

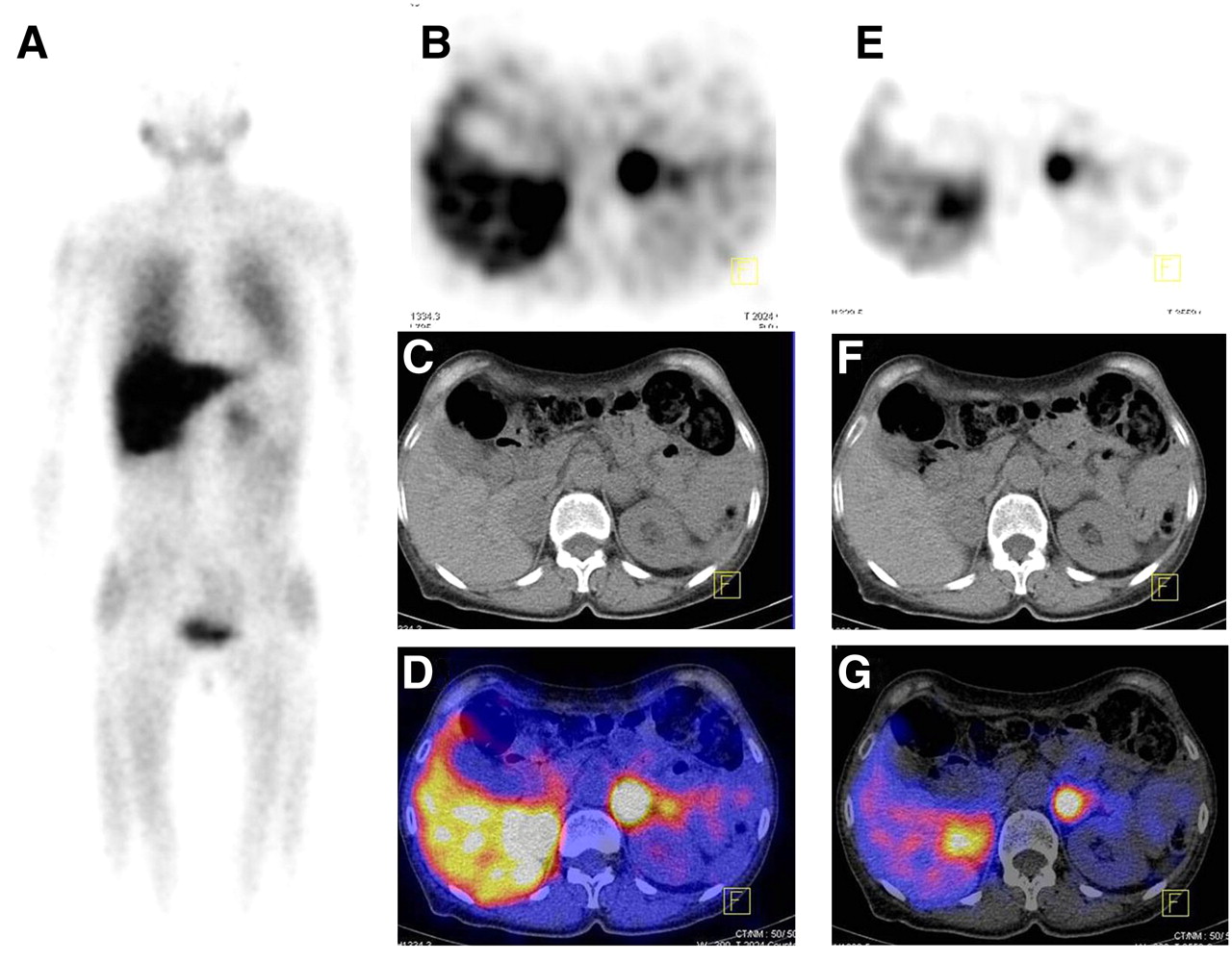
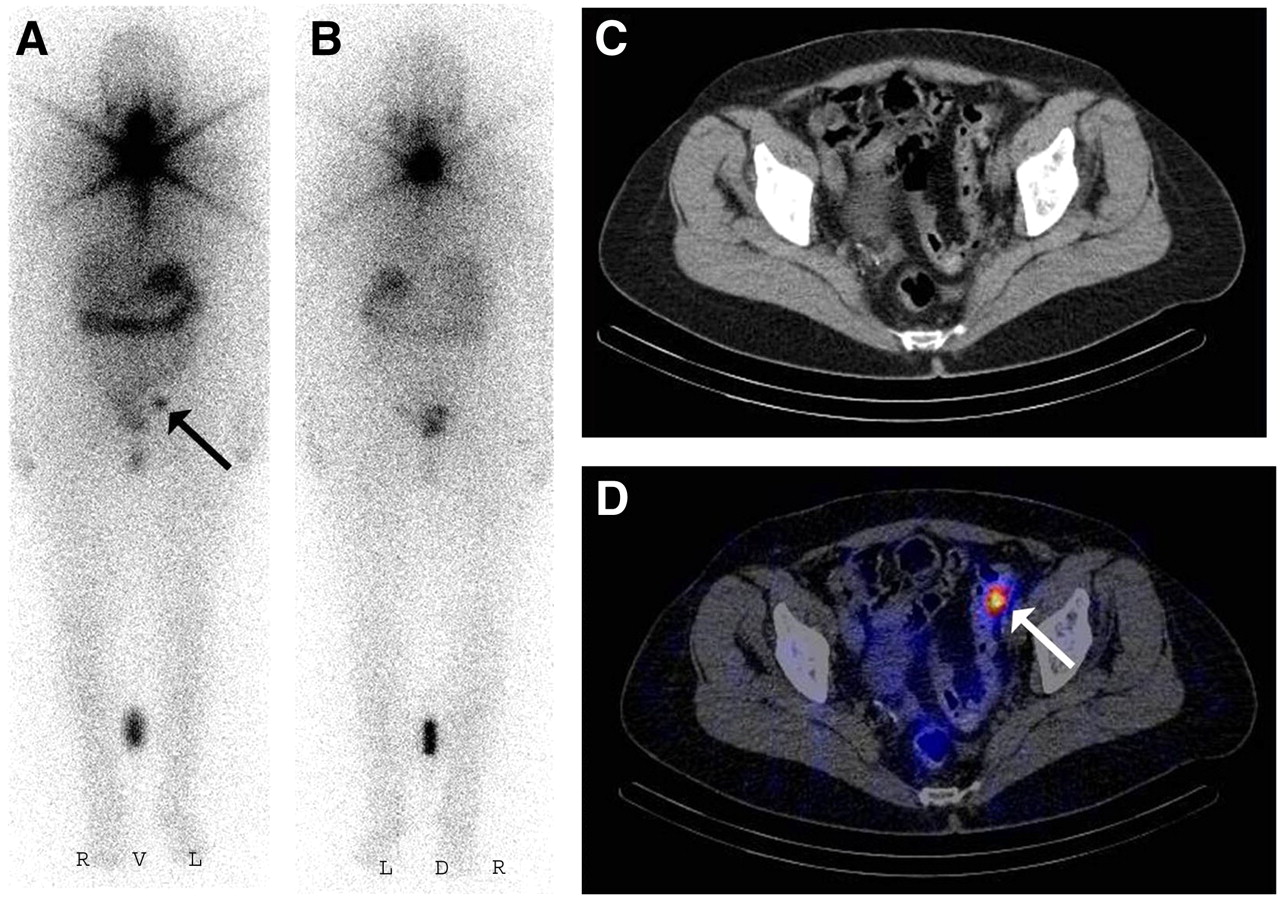
Exact delineation of focal pelvic 131I uptake in patient with differentiated thyroid cancer. (A and B) Planar 131I scintigrams (anterior view [A] and posterior view [B]) showing focal tracer uptake in left pelvic region (arrow). Lesion cannot be definitely assigned as benign or solitary bone metastasis. (C and D) Corresponding CT section (C) and fused SPECT/CT image (D) demonstrating nonspecific tracer uptake in diverticulum of colon (arrow).
In a study by Yamamoto et al. of 17 patients with differentiated thyroid carcinoma, fusion of SPECT and CT images with external markers improved the diagnosis in 15 of 17 patients (88%), mainly because of better anatomic localization of scintigraphic findings and differentiation of physiologic from specific uptake (43). Fused images resulted in a change in management for 4 of 17 patients (24%). A pilot study of 25 patients undergoing ablative radioiodine treatment of the thyroid also indicated an added value of SPECT/CT image fusion. Using an integrated SPECT/CT camera, Ruf et al. reported superior anatomic localization of 44% of suspected lesions (17/39) (44). The findings returned by fused images influenced therapeutic management for 25% of patients (6/24).
SPECT/CT IN PARATHYROID TUMORS
In primary hyperparathyroidism, 99mTc-methoxyisobutylisonitrile (MIBI) scintigraphy plays a minor role, because bilateral neck exploration has a success rate of up to 95%. However, with the increasing use of minimal invasive parathyroidectomy, presurgical imaging and precise localization of a parathyroid adenoma are critical for successful surgery. For a series of 110 patients, Lavely et al. compared the diagnostic performance of planar imaging, SPECT, SPECT/CT, and single- and dual-phase 99mTc-MIBI parathyroid scintigraphy (45). In this prospective study, dual-phase planar imaging, SPECT, and SPECT/CT were significantly more accurate than single-phase early or delayed planar imaging. Early-phase SPECT/CT in combination with any delayed imaging method (planar or SPECT) was superior to dual-phase planar imaging or dual-phase SPECT with regard to sensitivity, area under the curve, and positive predictive value (PPV). Sensitivity ranged from 34% for single-phase planar imaging to 73% for dual-phase studies including an early SPECT/CT scan. The PPV was as high as 86%−91% for dual-phase studies including an early SPECT/CT scan. The specificity was greater than 98% for all of the imaging techniques, and the negative predictive value was greater than 95%. Furthermore, early SPECT/CT had a higher sensitivity and a significantly higher PPV than delayed SPECT/CT. The authors therefore concluded that CT coregistration is a valuable tool for the precise delineation of parathyroid adenomas (Fig. 5).

Parathyroid scintigraphy with SPECT/CT. (A and B) Planar views of 99mTc-MIBI scintigraphy 60 min (A) and 15 min (B) after 99mTc-MIBI injection. Arrows indicate lesions. (C) Transverse section of 99mTc-MIBI SPECT showing mildly intense focal lesion in right lower neck region (arrow). (D and E) Corresponding CT section (D) and fused image (E) indicating parathyroid adenoma below right thyroid gland (arrows). (F and G) Demonstration of parathyroid adenoma (arrows) in corresponding coronal CT (F) and SPECT/CT (G) images.
Superior localization of parathyroid adenomas was also reported by Harris et al. (46). For a series of 23 patients, SPECT/CT performed well for the detection and localization of solitary adenomas (89%), but performance for the detection of multifocal disease was reduced. In a pilot study, Ruf et al. performed low-dose CT for attenuation correction and reported that the sensitivity of attenuation-corrected 99mTc-MIBI SPECT/CT was only slightly higher than that of non–attenuation-corrected SPECT (47). Also, Gayed et al. reported that SPECT/CT was only of limited value (8% of patients) (48). On the contrary, a retrospective study indicated a change in therapeutic management for 39% of patients (14/36) because of the localization of ectopic parathyroid adenomas or accurate localization in patients with distorted neck anatomy (49). Because of some inconsistent reports, a definite role of SPECT/CT in the imaging of parathyroid adenomas has not yet been indicated, and evaluations with larger patient cohorts are needed.
SPECT/CT IN TUMORS OF SYMPATHETIC NERVOUS SYSTEM AND ADRENOCORTICAL TUMORS
Morphologic imaging modalities, such as CT or MRI, offer high sensitivity for the detection of tumors of the sympathetic nervous system. The major advantages of radionuclide imaging, such as 123I-metaiodobenzylguanidine (MIBG) SPECT, 18F-l-3,4-dihydroxyphenylalanine PET, or 11C-metahydroxyephedrine (HED) PET, are high specificity, which can be used to better characterize lesions, and superior differentiation of scar tissue and residual tumor after surgery (Fig. 6) (50,51). Radionuclide imaging is also helpful for the detection of extraadrenal tumor sites. In a prospective study, Franzius et al. evaluated the clinical use of 123I-MIBG SPECT/CT in 19 patients with a variety of tumors of the sympathetic nervous system, including neuroblastoma and pheochromocytoma (52). 123I-MIBG SPECT/CT had a sensitivity (93%) similar to that (99%) achieved by PET/CT with 11C-HED as a tracer. 11C-HED PET/CT was demonstrated to show a higher spatial resolution and to return a final diagnosis within 30 min. SPECT/CT was compromised by a longer examination time and the need for delayed imaging (24 h after tracer administration). However, no superiority of PET/CT over SPECT/CT was observed. Because of the high cost and low availability of 11C, 123I-MIBG SPECT/CT seems to be appropriate for the imaging of tumors derived from the sympathetic nervous system, such as neuroblastoma, pheochromocytoma, ganglioneuroblastoma, and paraganglioma.
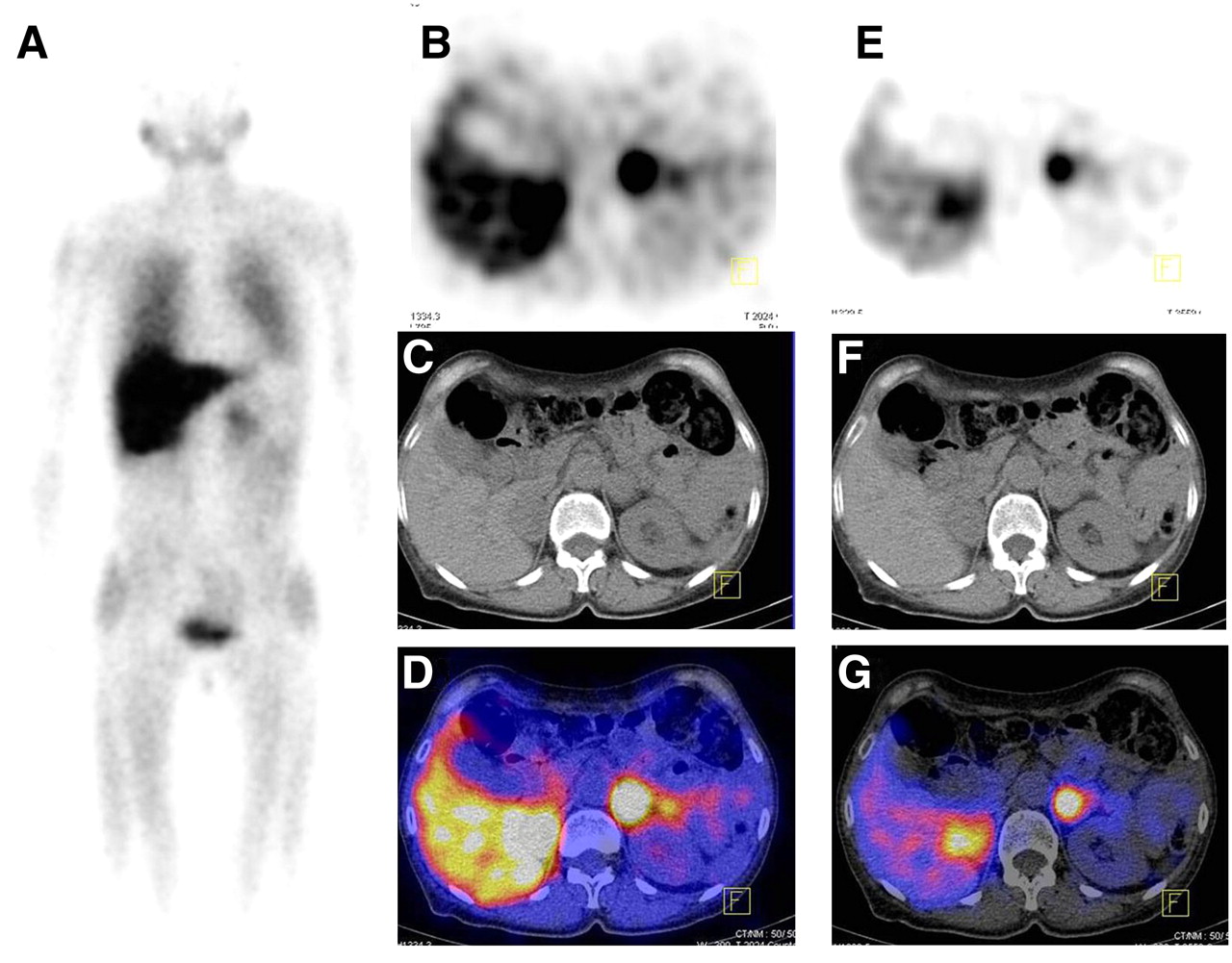
Diagnosis of pheochromocytoma with 99mTc-MIBG SPECT/CT. (A) Planar image showing mildly intense focal lesion extending to left suprarenal area. (B–D) Corresponding sections of SPECT (B), CT (C), and fused SPECT/CT (D) images showing focal uptake extending to enlarged left adrenal gland, indicating pheochromocytoma. (E–G) Corresponding transverse sections of right adrenal gland showing additional hot spot and enlargement of gland, indicating second pheochromocytoma, which was proven histologically. Lesion may be missed on planar image (A) or overexposed transaxial SPECT image (B).
Scintigraphic techniques also complement anatomically based imaging modalities for the evaluation of adrenocortical disease. The impact of hybrid SPECT/CT on the performance of functional imaging, such as 75Se-selenomethylnorcholesterol or 131I-iodocholesterol imaging, remains to be determined, because only scant data can be found in the literature. In a pilot study, Even-Sapir et al. reported a change in clinical management for a few patients undergoing 75Se-cholesterol SPECT/CT (53). Despite an obvious lack of clinical studies demonstrating the superiority of SPECT/CT over separately performed imaging modalities, it can be speculated that hybrid imaging will increase diagnostic accuracy and may lead to the more frequent use of functional imaging techniques.
SPECT/CT IN NEUROENDOCRINE TUMORS
Neuroendocrine tumors usually exhibit increased expression of somatostatin receptors (SSTR), enabling their detection through the specific binding of radiolabeled ligands, such as 111In-octreotide or 111In-pentetreotide. SSTR scintigraphy is predominantly used for the detection of primary tumors or hepatic or mesenteric metastases but can also be used for assessment of the response to treatment with somatostatin analogs. The number of publications illustrating the added value of CT coregistration for SSTR planar imaging or SSTR SPECT is limited. The largest study to date evaluated SSTR SPECT/CT in 72 patients with various neuroendocrine tumors, including 45 carcinoid tumors, medullary thyroid carcinoma, or islet cell tumors (54). No additional information beyond that provided by planar imaging or SPECT was achieved for 48 patients, whereas SPECT/CT improved the localization of scintigraphic findings for 23 patients (32%) and changed clinical management for 14% of patients. For a series of 27 patients with various neuroendocrine tumors, Even-Sapir et al. demonstrated increased accuracy of detection of lesions by 131I, 123I-MIBG, 75Se-cholesterol, or 111In-penetreotide SPECT/CT (53). For one third of patients, a change in clinical management occurred. A significant impact of SPECT/CT on therapeutic management was also demonstrated by Hillel et al. for 29 patients with carcinoid or other neuroendocrine tumors (55). The addition of clinically relevant information for 40% of patients by SPECT/CT compared with SPECT was described by Gabriel et al. (56).
SPECT/CT IN CARDIAC IMAGING
As an example of the increased interest in hybrid cardiac imaging, the Society of Nuclear Medicine awarded its 2006 image of the year award to a cardiac SPECT/CT study (57). This study demonstrated a defect in the inferior myocardium together with corresponding stenosis on CT angiography (CTA). Combining function and morphology is highly attractive for several reasons: improved diagnosis and logistics as well as illustrative visualization. In this review, we focus on the methodologic perspective for hybrid SPECT/CT in nuclear perfusion imaging (Table 2), because the number of clinical procedures and research studies is still small compared with the number of studies of conventional methods. Where SPECT, CT, and SPECT/CT are positioned best in the clinical decision-making process is outside the scope of this review; discussion of this topic is ongoing and is the focus of recent reviews (58–60). Specifically, Berman et al. proposed “possible risk-based strategies through which imaging might be used to identify candidates for more intense prevention and risk factor modification strategies as well as those who would benefit from coronary angiography and revascularization” (59). We are convinced that cardiac SPECT/CT will play a prominent role in these scenarios and have compiled arguments ranging from improved attenuation correction to the assessment of complementary information with the potential of reducing radiation burden.
Use of CT for Attenuation Correction
Nonhomogeneous photon attenuation in the thorax is one of the most notable limitations of myocardial perfusion imaging. It creates the appearance of a nonuniform, regional perfusion distribution even for normal hearts, thus limiting clinical specificity. To overcome this obstacle, the correction of photon attenuation requires the assessment of attenuating tissue in the volume of interest (Fig. 1). Unfortunately, cardiac imaging poses a particular problem for attenuation correction because of respiratory and cardiac motion. Technically, SPECT attenuation correction with external sources was introduced in the early 1990s; retrospectively, however, its success appears to be rather limited. Thus, the integration of CT components in 2000 was a major step forward, with clinically relevant results being reported in larger studies (61,62).
The technical developments were summarized in recent review articles (3,63). Two different technical approaches were previously investigated. The first was a protocol with a radiation burden as low as possible (<0.5 mSv). The second was a CT examination allowing diagnostic imaging that, for cardiac imaging, would be either an assessment of coronary calcifications or, if the CT system were suitable, contrast-based angiography (typically 1–3 mSv for calcium scoring or 4–14 mSv for CTA). It is important to note that the actual doses varied substantially for the imaging hardware and the imaging protocol used and recently showed a trend toward a decrease, at least for CTA studies. For the low-dose approach and the coronary calcification scan, the contribution to the overall dose is moderate; for SPECT and CTA, the contributions are almost the same (Table 2).
PET/CT studies have already shown that very low-dose CT acquisitions are feasible for attenuation correction (64). Koepfli et al. (65) and a recent study with SPECT/CT confirmed these findings (66). However, a potential misalignment between emission and transmission data poses the risk of incomplete correction and thus artificial perfusion defects and requires careful quality control to avoid reconstruction artifacts. PET/CT (67,68) and SPECT/CT (69,70) studies have shown that the frequency of misalignment is high (≤50%) and that the consequences are clinically significant. Fortunately, a recent study with a digital phantom showed that the effects of misalignment are less severe for SPECT/CT than for PET/CT, mainly because of reduced spatial resolution (71). The alignment of SPECT and CT is usually performed manually, a process that contributes to certain variabilities. However, automated approaches for quality control are under investigation (10,72,73). It is relevant that even low-quality CT scans for attenuation correction provide clinically useful information. Goetze et al. reported that for 10% of 200 patients, noncardiac-related abnormal findings were detected (69,70). Similar data with even higher incidence rates are available from cardiac CT studies (74,75). Incidental findings may result in legal liabilities. It is clear that modifications in the clinical reading process are needed.
Cardiac SPECT Versus PET and Absolute Quantification
The superiority of cardiac PET over cardiac SPECT was demonstrated in several publications (3,58,71,76,77). However, in almost all of these reports, non–attenuation-corrected SPECT was used. Thus, assuming the availability of reliable CT-based attenuation correction for single-photon imaging and given an increased tolerance of motion artifacts, new studies should provide further insight into whether PET will remain superior. From a technical point of view, the capability of PET for absolute quantification in general and for blood flow quantification in particular is a substantial advantage. Nevertheless, through the use of animal models and a SPECT/CT system, it was shown that absolute activity values can be generated when attenuation correction and partial-volume effects are considered (78,79). For assessing absolute flow and coronary flow reserve, imaging with SPECT appears to be promising but requires large-scale validation work (80–82).
Integration of Calcium Scoring CT
In general, a trend toward the integration of low- and medium-quality CT systems—as opposed to high-end systems suitable for contrast-enhanced CT of the coronary arteries—into SPECT/CT devices has been observed. Consequently, those hybrid systems are not necessarily suitable for analysis of the vessel lumen with contrast agents but may be capable of the technically less demanding imaging of coronary calcium as a potential marker of atherosclerosis; however, this hypothesis has been debated in the last few years. It is not the aim of this review to repeat this discussion, but some selected, potential hybrid applications deserve mention.
A recent study investigated the incidence of significant calcifications in 84 patients referred for 82Rb PET with adenosine stress (83). Non–contrast-enhanced CT was used for attenuation correction. Thirty-four patients with negative calcium findings also had normal PET results (negative predictive value, 100%). The remaining 50 patients had calcifications, and a myocardial perfusion defect was detected in 13 patients (PPV, 26%; sensitivity, 100%; specificity, 48%). Using this combined approach, the investigators concluded that myocardial perfusion PET could have been obviated in 63% of patients with no smoking history and no prior myocardial infarction or coronary revascularization procedure and in 37% of the total patient cohort. Although this study was a PET/CT study, this approach might allow a nuclear scan in a resting state to be avoided, and the overall radiation dose from SPECT/CT could be markedly reduced. Similarly, Henneman et al. investigated the hypoenhancement resulting from delayed contrast agent washin in CTA studies (84). On the basis of the fact that the scar scores calculated from SPECT myocardial perfusion imaging and by CTA washin analysis corresponded well for SPECT and CTA, another approach to avoiding a resting SPECT examination could be envisioned. However, although these studies appear to be promising, the incremental value of assessing coronary calcifications or coronary morphology as part of a nuclear examination needs to be investigated in large prospective studies, and it is too early to answer the question of optimal work flow.
Myocardial Perfusion and CT Coronary Angiography
As with combined PET/CT acquisitions of perfusion and coronary morphology (85), visually very attractive displays can be created with SPECT/CT systems (86). In one of the largest studies to date, including 56 patients with a high prevalence of coronary artery disease, the authors concluded that “hybrid SPECT/CTCA imaging results in improved specificity and PPV to detect hemodynamically significant coronary lesions in patients with chest pain” (87). However, this study also showed that the total radiation burden was as high as 41.5 mSv.
It is interesting that the fusion approach is not restricted to integrated devices (88,89). In particular, for CTA studies, the integrated CT component is typically less advanced than stand-alone CT. Thus, the use of external CT is feasible and may even offer a resolution advantage. Technically, SPECT and CT studies must be spatially registered even with hybrid cameras because of differences in breathing positions (expiration vs. averaged respiratory motion). A relevant additional aspect of cardiac contrast-enhanced CT is the imaging of delayed enhancement, as in MRI. The different washout rates for contrast agents in normal myocardium and damaged myocardium are now widely used in MRI (90) and recently were used in CT (91,92). Thus, delineating scar tissue with low-dose CT after contrast agent injection appears to be feasible.
In summary, the prospects for hybrid cardiac imaging are promising, and new clinical applications are being proposed. Large, prospective, outcome-based studies for proving these concepts are lacking. In addition, economic and biologic aspects must be considered (93,94). However, reliable attenuation correction and the integration of complementary, multimodality information into an attractive display facilitating communication with cardiologists will influence the future development of nuclear cardiac imaging.
SPECT/CT IN NEUROLOGIC AND PSYCHIATRIC DIAGNOSES
So far, data on the added value of combined SPECT/CT examinations of the brain remain rather limited. However, the diagnostic value of various cerebral SPECT examinations, such as cerebral perfusion or receptor studies, might be increased, to some extent, by additional CT examinations.
In general, individual CT scan–based attenuation correction of brain SPECT data may lead to improved image quality and more accurate data evaluation (Fig. 1). These features may be particularly important for regional data analysis, such as semiquantitative region-of-interest–based image analysis, as regularly applied for the evaluation of imaging studies of presynaptic dopamine transporters with 123I-2β-carbomethoxy-3β-(4-iodophenyl)tropane (DaTSCAN; GE Healthcare) or postsynaptic dopamine receptors with 123I-iodobenzamide. These examinations are usually applied for the verification of idiopathic Parkinson's disease, respectively, the differentiation from atypical Parkinson syndromes. In both types of studies, ratios of striatal to background tracer uptake are calculated, and predefined thresholds for striatum-to-background ratios are used for the differentiation of normal uptake and pathologic findings reflecting reduced receptor or transporter density. For attenuation correction of these studies, ellipse-based calculated attenuation correction techniques, such as the procedure described by Chang (95), are usually applied and have been demonstrated to show sufficient reliability. However, it has been shown that attenuation correction based on individual CT scans produces more accurate results (96). In particular, for borderline findings, it is possible that attenuation correction has a significant influence on quantitative assessment and, thus, on the resulting clinical diagnosis. In such cases, individual CT scan–based attenuation correction may lead to a more appropriate diagnosis. In addition to optimized data quality, access to individual coregistered CT data may also improve the standardized definition and positioning of regions of interest, particularly in datasets with pathologically low uptake (97). However, a systematic analysis is required to assess differences between individually measured and conventionally calculated attenuation corrections, and clarification of whether currently applied thresholds need to be modified is also required.
In addition to individualized attenuation correction, the performance of CT scans simultaneously with SPECT examinations may offer several additional advantages. A recent study examined the additional diagnostic value of the low-dose (CT) component of a combined 99mTc-hexamethylpropyleneamine oxime SPECT/CT examination of cerebral perfusion in a large population (98). Interestingly, 25% of the low-dose CT images demonstrated abnormalities such as infarcts, cerebral atrophy, dilated ventricles, basal ganglion calcifications, and other findings, such as subdural hematoma or meningioma. The authors concluded that the CT component of cerebral perfusion SPECT/CT investigations should be routinely reported separately.
Finally, with the advent of modern SPECT/CT hybrid systems containing state-of-the-art CT scanners, it is possible, in principle, to perform high-quality diagnostic CT examinations of the brain in a single session with simultaneous SPECT examinations. This feature may offer opportunities to assess vascular pathologies, such as cerebral ischemia, stroke, or carotid stenosis, and even to diagnose brain death through the examination of cerebral perfusion with 99mTc-hexamethylpropyleneamine oxime in combination with CT assessment of vascular abnormalities (CT perfusion imaging, or CTA). The value of this type of combined examinations has not yet been sufficiently assessed and needs to be evaluated in specific clinical trials.
COMBINED SPECT/CT FOR OPTIMIZED DOSIMETRY
The complementation of scintigraphic examinations with detailed anatomic information derived from CT offers the possibility of improving organ-specific dosimetry for radiation treatment planning and radionuclide therapy. Dosimetry for treatment planning and for retrospectively ascertaining the absorbed dose delivered during treatment should be regarded as mandatory for all radionuclide therapies, such as radioiodine (131I) treatment of thyroid cancer; radioimmunotherapy of lymphoma with, for example, 90Y-ibritumomab tiuxetan; or therapy of neuroectodermal tumors, such as pheochromocytoma, neuroblastoma, or paraganglioma, with 131I-MIBG. Conventionally, dosimetry for radionuclide treatment has been performed mostly by application of a low dose of the therapeutic radionuclide used for imaging or by application of the therapeutic compound labeled with a different radiotracer more suitable for scintigraphy (e.g., 111In or 123I) followed by tracer uptake measurements in planar scintigrams. However, more accurate dosimetry may require 3-dimensional assessment, proper attenuation correction of the image data, and assessment of organ or target volumes, which can be derived from simultaneously acquired CT scans. Several studies have already demonstrated that 3-dimensional dosimetry based on anatomic information derived for regional organ volumes or masses from CT leads to superior assessments of regionally applied doses in critical organs (99–103). Integration of the data collected by multimodality imaging into complex calculation models, such as the Monte Carlo simulation, may significantly improve regional dosimetry for the spatial distribution of the absorbed dose (104).
In addition to dosimetry of critical organs at risk, evaluation by multimodality imaging with SPECT/CT may also allow accurate dosimetry of tumor targets for treatment planning and evaluation of the response to radionuclide therapy (105). This process may also be valuable for establishing a clear correlation between the absorbed dose and the biologic effect.
In summary, it appears likely that combined SPECT/CT will be highly useful for performing valid and clinically applicable dosimetry, for improving treatment planning, and for ensuring safe and effective radionuclide therapy.
Furthermore, combined SPECT/CT may also be useful for planning radiation treatment for prostate cancer. Hybrid imaging of capromab pendetide (Prostascint; Cytogen) with SPECT and CT has been demonstrated to show increased sensitivity for the identification of prostate cancer. Recently, it was proposed that this combined imaging approach be used to confine the dose escalation of radiation treatment to discrete regions of known disease, as defined by focal uptake on fused radioimmunoscintigraphic and anatomic image sets (106). It has been suggested that intensification of treatment directed to tumor targets without an increase in rectal toxicity may be achieved. Suggestions also have been extended toward guiding the implantation of radioactive seeds in brachytherapy (107). In general, it may be assumed that SPECT/CT will be equally valid for individualized planning of radiation treatment for other tumor entities, and further clinical research should be encouraged.
CONCLUSION
The role of integrated SPECT/CT is growing, especially in oncologic applications. CT coregistration results in higher specificity as well as sensitivity of scintigraphic findings and markedly reduces the number of indeterminate findings. The superiority of SPECT/CT over planar scintigraphy or SPECT has been clearly demonstrated for the imaging of benign and malignant skeletal diseases, thyroid cancer, neuroendocrine cancer, parathyroid adenoma, and mapping of SLNs in the head and neck and in the pelvic region. Studies demonstrating superiority in other clinical applications are lacking; however, pilot studies have encouraged the use of SPECT/CT in cardiac and neurologic imaging. Interesting developments occurring with less frequently used radiopharmaceuticals and imaging technologies may become clinically relevant in the near future.
Footnotes
-
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH AUGUST 2009.
-
No potential conflict of interest relevant to this article was reported.
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.
- 35.↵
- 36.↵
- 37.
- 38.
- 39.
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.
- 101.
- 102.
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- Received for publication March 26, 2008.
- Accepted for publication June 20, 2008.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- TECHNICAL ASPECTS OF SPECT/CT
- SUGGESTED PROTOCOLS FOR SPECT/CT
- SPECT/CT FOR SLN MAPPING
- SPECT/CT IN SKELETAL DISEASES
- SPECT/CT IN DIFFERENTIATED THYROID CANCER
- SPECT/CT IN PARATHYROID TUMORS
- SPECT/CT IN NEUROENDOCRINE TUMORS
- SPECT/CT IN CARDIAC IMAGING
- SPECT/CT IN NEUROLOGIC AND PSYCHIATRIC DIAGNOSES
- COMBINED SPECT/CT FOR OPTIMIZED DOSIMETRY
- CONCLUSION
- Footnotes
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Life-threatening Coagulation Disorders
- Utility of Scintigraphy in Assessment of Noninfectious Complications of Peritoneal Dialysis
- Targeting Cardiovascular Implant Infection: Multimodality and Molecular Imaging
- The Clinical Dilemma of Incidental Findings on the Low-Resolution CT Images from SPECT/CT MPI Studies
- 99mTc SPECT/CT Versus Planar Lymphoscintigraphy for Preoperative Sentinel Lymph Node Detection in Cervical Cancer: A Systematic Review and Metaanalysis
- Thyroid Cancer in Children
- SPECT-CT: applications in musculoskeletal radiology
- SNMMI/ASNC/SCCT Guideline for Cardiac SPECT/CT and PET/CT 1.0
- Indexing Severity of Diabetic Foot Infection With 99mTc-WBC SPECT/CT Hybrid Imaging
- MIRD Pamphlet No. 23: Quantitative SPECT for Patient-Specific 3-Dimensional Dosimetry in Internal Radionuclide Therapy
- The Significance of 99mTc-MAA SPECT/CT Liver Perfusion Imaging in Treatment Planning for 90Y-Microsphere Selective Internal Radiation Treatment
- Single photon emission computed tomography (SPECT)/computed tomography using Iodine-123 in patients with differentiated thyroid cancer: additional value over whole body planar imaging and SPECT
- Constrained Physical Therapist Practice: An Ethical Case Analysis of Recommending Discharge Placement From the Acute Care Setting
- Diagnosis of Prosthetic Aortic Valve Endocarditis With Gallium-67 Citrate Single-Photon Emission Computed Tomography/Computed Tomography Hybrid Imaging Using Software Registration
- Hybrid SPECT-CT and PET-CT imaging of differentiated thyroid carcinoma
- Reply: SPECT/CT
- SPECT/CT
- Nuclear Imaging and Minimally Invasive Surgery in the Management of Hyperparathyroidism