


Abstract
Selective internal radiation therapy (SIRT), a catheter-based liver-directed modality for treating primary and metastatic liver cancer, requires appropriate planning to maximize its therapeutic response and minimize its side effects. 99mTc-macroaggregated albumin (MAA) scanning should precede the therapy to detect any extrahepatic shunting to the lung or gastrointestinal tract. Our aim was to compare the ability of SPECT/CT with that of planar imaging and SPECT in the detection and localization of extrahepatic 99mTc-MAA accumulation and to evaluate the impact of SPECT/CT on SIRT treatment planning and its added value to angiography in this setting. Methods: Ninety diagnostic hepatic angiograms with 99mTc-MAA were obtained for 76 patients with different types of cancer. All images were reviewed retrospectively for extrahepatic MAA deposition in the following order: planar, non–attenuation-corrected SPECT, and SPECT/CT. Review of angiograms and follow-up of patients with abdominal shunting served as reference standards. Results: Extrahepatic accumulation was detected by planar imaging, SPECT, and SPECT/CT in 12%, 17%, and 42% of examinations, respectively. The sensitivity for detecting extrahepatic shunting with planar imaging, SPECT, and SPECT/CT was 32%, 41%, and 100%, respectively; specificity was 98%, 98%, and 93%, respectively. The respective positive predictive values were 92%, 93%, and 89%, and the respective negative predictive values were 71%, 73%, and 100%. The therapy plan was changed according to the results of planar imaging, SPECT, and SPECT/CT in 7.8%, 8.9%, and 29% of patients, respectively. Conclusion: In pre-SIRT planning, 99mTc-MAA SPECT/CT is valuable for identifying extrahepatic visceral sites at risk for postradioembolization complications.
In addition to being at risk for the development of primary carcinoma, the liver is a predominant site of metastasis from a wide variety of neoplasms, and 60%–80% of patients with a history of colorectal carcinoma, pancreatic carcinoma, breast cancer, and other tumor types will develop liver metastases (1). Radiation is tumoricidal if sufficient doses can be delivered selectively to the tumor without damaging adjacent normal tissue, considering that normal hepatocytes have a lower tolerance to the effects of radiation than does neoplastic tissue. The dose required to destroy a solid tumor, estimated at 70 Gy or more, is far greater than the liver tolerance dose of 35 Gy delivered to the whole liver in 1.8 Gy/d fractions (2).
90Y radioembolization, or selective internal radiation therapy (SIRT), is a promising catheter-based liver-directed modality approved by the Food and Drug Administration for patients with primary and metastatic liver cancer. Liver-directed SIRT provides several advantages over traditional treatment methods because of its low toxicity profile (3,4). Two microsphere products are commercially available. TheraSphere (glass microspheres; MDS Nordion) and SIR-Spheres (resin microspheres; Sirtex Medical) were approved by the Food and Drug Administration in 1999 and 2002, respectively (2). Overall, the incidence of complications after SIRT for appropriately selected patients and meticulously targeted delivery is low (5). Serious complications have been reported when microspheres were inadvertently deposited in excessive amounts in organs other than the liver. Reported complications include gastrointestinal ulceration or bleeding, gastritis or duodenitis, cholecystitis, pancreatitis, and radiation pneumonitis (1,2,6–11).
Generally, for any selected candidate for SIRT, an angiographic evaluation combined with 99mTc-macroaggregated albumin (MAA) scanning should precede the therapy to detect any extrahepatic shunting to the lung or gastrointestinal tract. Prophylactic embolization of all extrahepatic vessels, including gastroduodenal, right gastric, and other extrahepatic vessels, at the time of 99mTc-MAA assessment is recommended to avoid extrahepatic deposition of microspheres (2). Normally, only planar imaging and SPECT of the upper abdomen are performed to assess 99mTc-MAA distribution in the liver and to rule out extrahepatic shunts. Recently, hybrid SPECT/CT installations consisting of a high-end multislice CT scanner that allows for isotropic imaging by thin collimation (0.5 mm) and a dual-head γ-camera have become available, enabling high diagnostic accuracy. SPECT/CT allows direct correlation of anatomic and functional information, resulting in a better localization and definition of scintigraphic findings. In addition to anatomic referencing, the benefit of CT coregistration is based on the attenuation correction capabilities of CT (12). The positive impact of SPECT/CT in diagnosing benign and malignant diseases has been shown in different studies (13–20).
Our aim was to compare the ability of SPECT/CT with that of planar imaging and SPECT in the detection and localization of extrahepatic 99mTc-MAA accumulation and to evaluate the impact of SPECT/CT on SIRT treatment planning and its added value to angiography in this setting. The significance of SPECT/CT with regard to intrahepatic distribution of MAA was not addressed in this study.
MATERIALS AND METHODS
Patients
Ninety diagnostic hepatic angiograms combined with 99mTc-MAA scanning were obtained for 76 patients with different types of cancer (Table 1). The mean and median ages of the patients were 64 y and 65 y, respectively (range, 34–83 y; 27 women [36%], 49 men [64%]). Three patients, all with hepatocellular carcinoma, had single liver tumors, whereas the others had multiple tumors or metastases. Sixty-six patients (87%) had tumors or metastases in both liver lobes, 9 patients had tumors only in the right lobe, and tumors or metastases were limited to the left lobe in 1 patient.
Seventy-Six Patients with Different Types of Cancer Evaluated for Radioembolization Therapy
Angiogram with Selective Visceral Catheterization and Therapy Simulation with 99mTc-MAA (Test Angiogram)
Angiography was performed in the Department of Radiology to define the vascular anatomy of the liver and to assess the vascularity of hepatic tumors and metastases before SIRT. Sixty-two patients (82%) had normal vascular anatomy. To avoid extrahepatic deposition of microspheres, all visible nonhepatic arteries were embolized prophylactically at the time of MAA assessment, including arterial flow to the pulmonary, gastroduodenal, right gastric, and other extrahepatic vessels. During the angiogram and depending on the anatomy of the liver, 200–400 MBq of 99mTc-MAA (Bonn protocol) were administered intraarterially into either the hepatic artery proper or the left and right hepatic arteries separately to simulate the distribution of microspheres to the liver, lungs, and possibly extrahepatic abdominal organs. In this study, 99mTc-MAA was injected into the artery proper, the right and left hepatic arteries in 1 session, or only into the right or left hepatic artery in 39%, 42%, 13%, and 4% of cases, respectively. In 2 cases, the 99mTc-MAA was injected superselectively into segmental arteries. To avoid nonspecific tracer uptake in the abdomen due to free 99mTc, 86 angiograms were performed after oral administration of 600 mg of perchlorate. Planar, whole-body, and SPECT/CT scans were performed in the Department of Nuclear Medicine within 1 h of 99mTc-MAA injection.
Image Acquisition
Whole-body scans in anterior and posterior projections were obtained to calculate the percentage of liver-to-lung shunting and, consequently, the possibility of pulmonary side effects. Furthermore, planar scintigraphic images of the upper abdomen followed by SPECT/CT images were obtained using a dual-detector γ-camera with a mounted 2-row CT scanner (Symbia T2; Siemens Healthcare) to allow better evaluation of tracer accumulation in the liver and to rule out extrahepatic hot spots in other organs.
The acquisition parameters for SPECT were a 128 × 128 matrix with 64 frames (20 s/frame). The scan parameters for CT were 130 kV, 60 mAs, and 5-mm slices. SPECT images were corrected for attenuation and scatter. Reconstructed data were visualized in sagittal, coronal, and axial slices. Fused images were generated from the coregistered SPECT and diagnostic CT images using Syngo MMWP VE25A software 2007 (Siemens Healthcare).
Image Interpretation
All images were reviewed retrospectively for extrahepatic 99mTc-MAA deposition by 2 experienced nuclear medicine physicians using a Syngo workstation (VE25A; Siemens Healthcare). Images were read in the following order: planar, SPECT, and SPECT/CT.
Reference Standard
Retrospective review of the SPECT/CT images revealed overlooked extrahepatic accumulation of 99mTc-MAA in 6 patients, who had received the test angiogram in the first weeks of using SPECT/CT in our department. In these patients, either the responsible vessel had been found in the routine angiographic reexamination just before the commencement of the therapy or clinical side effects developed. In other patients with diagnosed extrahepatic accumulations, the angiographic scans had been reviewed in consultation with the radiologists in an effort to find the responsible aberrant vessels. Follow-ups including physical examination and laboratory testing were performed on all patients receiving SIRT on days 2, 14, 30, 60, 90, and up to 1 y (if the patients were alive) after intervention. All patients with gastrointestinal complaints underwent gastroduodenoscopy.
Contrast-enhanced MRI and metabolic imaging with PET/CT or SPECT/CT were performed for response evaluation and assessment of extrahepatic metastases on postinterventional days 30, 90, and 180.
Data Analysis
Based on the reference standard, potential gastrointestinal accumulations detected on planar imaging, SPECT, and SPECT/CT were first rated retrospectively as true-positive, true-negative, false-positive, or false-negative. Six overlooked patients (test angiogram) were rated for a second time in a separate so-called real-life condition (RLC) as false-negative. The sensitivity, specificity, positive predictive value, and negative predictive value of all imaging modalities were calculated for both conditions. The form and intensity of intrahepatic 99mTc-MAA accumulation were not considered in this study.
RESULTS
Extrahepatic accumulation was detected by planar imaging, SPECT, and SPECT/CT in 12%, 17%, and 42% of examinations, respectively. False-positive accumulation in the stomach on SPECT/CT images was detected in 4 patients (6%) who received no perchlorate before 99mTc-MAA injection, which was always in concordance with thyroid gland uptake (Supplemental Fig. 1; supplemental materials are available online only at http://jnm.snmjournals.org), and was detected in only 1 patient on SPECT and planar imaging. The number of false-negative results was 23 for planar imaging, 20 for SPECT, and in retrospective reviews zero for SPECT/CT. However, in RLC the number of false-negative results was 6 for SPECT/CT simply because of the 6 previously mentioned patients with overlooked extrahepatic accumulation of 99mTc-MAA. On the basis of these findings, the sensitivity for detecting extrahepatic shunting with planar imaging, SPECT, and SPECT/CT was 32%, 41%, and 100% (82% RLC), respectively, whereas the specificity was 98%, 98%, and 93%, respectively. The positive predictive values were 92%, 93%, and 89% (88% RLC), respectively, and the negative predictive values were 71%, 73%, and 100% (90% RLC), respectively (Table 2).
Sensitivity, Specificity, Positive Predictive Value (PPV), and Negative Predictive Value (NPV) of 99mTc-MAA Planar, SPECT, and SPECT/CT Studies in Retrospective Analysis and RLC
Altogether, the number of abnormal findings detected by planar imaging, SPECT, and SPECT/CT was 13, 18, and 52, respectively. However, exact anatomic classification was possible for only 9 and 11 abnormal findings on planar imaging and SPECT, respectively (Table 3). For 36% of the abnormal findings detected on planar imaging, the anatomic region could be determined only with SPECT/CT, corresponding to 33% in the case of SPECT. SPECT/CT detected 50% and 20% additional abnormalities in cases for which other extrahepatic shunting had already been detected by planar imaging and SPECT, respectively.
Number of Cases in Which Planar Imaging, SPECT, or SPECT/CT Was Successful in Determining Exact Anatomic Location of Extrahepatic Perfusion Abnormalities
Of 4 patients with MAA deposition in the stomach on SPECT/CT images, interpreted as free 99mTc, 1 patient treated with SIR-Spheres developed a gastric ulcer despite no noticeable problems such as reflux of resin microspheres during therapy. A surgical finding of resin spheres in the ulcer disputed the possibility that the accumulation of tracer in stomach was due to free 99mTc. This result emphasizes the importance of perchlorate administration before 99mTc-MAA injection to avoid nonspecific tracer uptake in the stomach due to free 99mTc, the finding of which can be misleading.
The therapy plan was changed in RLC according to the results of planar imaging, SPECT, or SPECT/CT in 7.8%, 8.9%, and 29% of examinations, respectively, as follows.
Accumulation in Gallbladder
Tracer deposition in the gallbladder wall was evidenced by SPECT in 1 patient and by SPECT/CT in 9 patients (12%) (Supplemental Fig. 2). To prevent the spheres from reaching the gallbladder and to avoid possible cholecystitis (1,5,21), the catheter was placed distal to the cystic artery in 6 patients, and in 1 case it was embolized. None of these patients developed cholecystitis during follow-up. One patient was not treated because of increasing bilirubin, and the other patient with a neuroendocrine tumor had an additional abnormal accumulation in the duodenum, detected only by SPECT/CT. In this patient, the aberrant vessel could not be found on review of test angiograms. Therefore, the therapy plan was changed to radioreceptor therapy to avoid gastrointestinal side effects.
Extrahepatic Abdominal Accumulation
Reviewing the test angiograms revealed the possible aberrant vessels in 5 patients with tracer deposition in the gastrointestinal system followed by a second 99mTc-MAA examination after embolization of suspected arteries (Supplemental Fig. 3). Four of these patients no longer showed abnormal extrahepatic tracer accumulation. In the other patient, who still showed some shunting in the bowel in the second examination, a third 99mTc-MAA examination was performed and the responsible aberrant artery was successfully embolized.
In 4 other patients with underlying vessels evident on test angiogram images, either the vessels were coiled or the microspheres were injected from a more distal catheter position without any further 99mTc-MAA examination.
In 2 patients, an underlying artery was found neither on reviewing the test angiograms nor on repeated angiography despite persistent extrahepatic 99mTc-MAA uptake. These patients were not treated.
Accumulation in Coil Region
In the coil region of 5 patients, SPECT/CT showed tracer accumulation not detectable by other modalities. In 3 patients, an aberrant vessel from the right hepatic artery to this region was found on reviewing test angiograms and embolized before SIRT (Supplemental Fig. 4). In the other 2 patients, the coiled vessels had not been completely embolized; the problem was discovered and corrected in the therapy session (Supplemental Fig. 5).
None of these patients experienced gastrointestinal complications.
Complications and Overlooked Cases
One patient with coil embolization of the gastroduodenal artery and 99mTc-MAA injection into both the right and the left hepatic arteries showed accumulation of 99mTc-MAA in the stomach, duodenum, abdominal wall, and gallbladder. In this patient, we performed SIRT with TheraSphere for the right liver lobe after embolization of 2 small vessels arising from the left hepatic artery to the stomach and duodenum and placement of the catheter distal to the cystic artery. Six days later, the patient experienced abdominal pain followed by abdominal bleeding. Microspheres were found in a duodenal ulcer on gastroduodenoscopy.
In 6 patients, abnormal 99mTc-MAA accumulation was detected by SPECT/CT only retrospectively after review of clinical follow-up records. Three patients showed tracer accumulation only in the duodenum, 1 in the duodenum and spleen, 1 in the coil region, and 1 in the abdominal wall. Two patients with duodenal accumulation had developed a duodenal ulcer within 4 wk after SIRT; in one of them, particles were found during gastroduodenoscopy. In the other patient, the radiologist found and embolized a vessel supplying the duodenum during the therapy session before SIRT, without any specific knowledge of extrahepatic accumulation. This patient exhibited no side effects. The patient with duodenal and splenic tracer accumulation had not received any therapy because of a high-grade lung shunt. The patient with tracer accumulation in the abdominal wall had undergone SIRT for the right lobe followed by a second therapy for the left lobe 5 wk later; this patient developed a gastric ulcer and erosive enteritis within 3 wk of the second therapy. In the patient with tracer accumulation in the coil region, the gastroduodenal artery was found to be incompletely embolized. No significant correlation between extrahepatic 99mTc-MAA uptake ratio and the severity of gastrointestinal side effects could be revealed in this study.
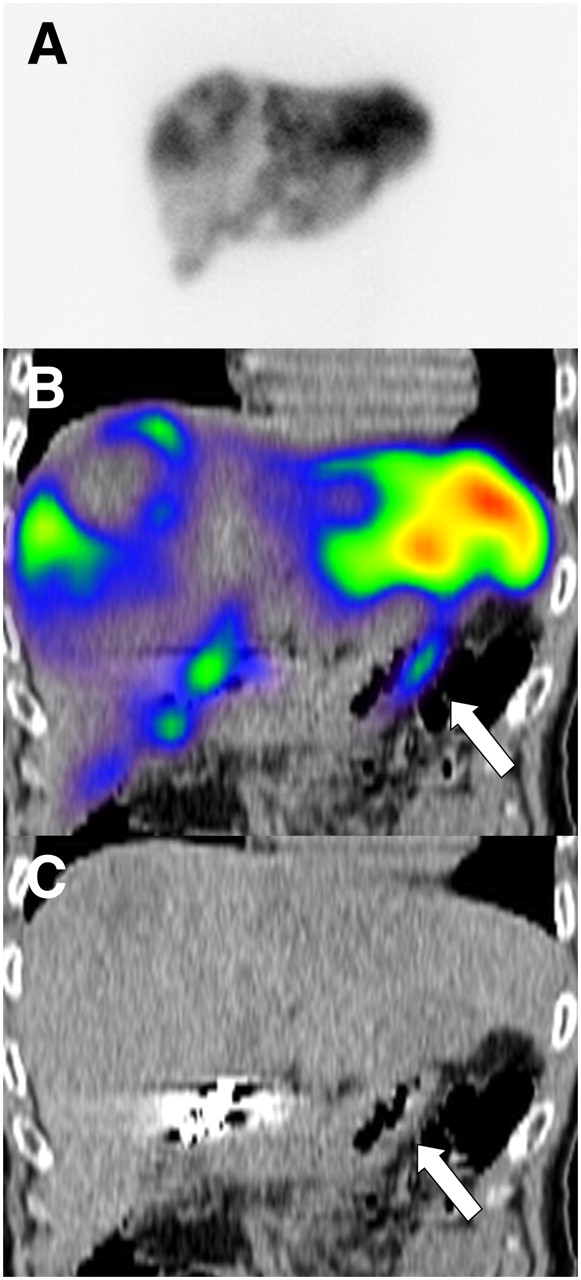
Accumulation in the duodenum could be diagnosed only by SPECT/CT and was retrospectively evident in 11 patients (14%). Because the coronal view of SPECT/CT was the most helpful for evaluating the duodenum, we named this typical appearance the “coronal gastroduodenal sign” (Fig. 1).

Duodenal accumulation (arrows) in a patient with colorectal cancer, not definable on planar images: planar scan (A), SPECT/CT coronal view (B), and CT coronal view (C).
Comparison of SPECT/CT with Angiography
In RLC, no nonembolized aberrant vessels were found on the routine reexamination angiograms of the patients without evidence of extrahepatic 99mTc-MAA accumulation on SPECT/CT, except for the 2 formerly described overlooked patients. This means that there was almost a 94% negative predictive value for SPECT/CT in RLC and a 100% negative predictive value in the retrospective analysis considering angiography as the only reference standard.
On the other hand, in 97% of patients with extrahepatic accumulation on SPECT/CT, at least an aberrant vessel—in 1 case after the third test angiogram—was found. Either the vessel was embolized or the SIRT was performed at a more distal catheter position. In 2 patients, no aberrant vessel has been found on repeated test angiograms despite extrahepatic accumulation on SPECT/CT that led to cancellation of therapy.
DISCUSSION
Microspheres can be transported into the vascular territory of the gastrointestinal organs, resulting in severe damage in less than 5% of SIRT cases. This damage can occur when the microspheres are inadvertently injected into small arteries that are misinterpreted by the radiologist as normal left-side liver arteries supplying blood to the left lobe of the liver, when in actuality these arteries are going to the gut. The main culprit is a right gastric artery originating from the left hepatic artery that is not recognized as or considered to be a small artery supplying the left lobe of the liver. Alternatively, these arteries may not have been detected by the radiologists. In about 15% of patients, vessels too small to be detected on an angiogram may pass from the liver to the gut (22). Radiation and diminished blood supply due to embolization by the spheres and subsequent hypoxia may result in ulceration and even perforation of the stomach and duodenum (10,23). 90Y-induced ulceration of the stomach or duodenum can be resistant to medical therapy, and surgery may be required (8).
SIRT requires accurate planning to ensure a good therapeutic response with as few side effects as possible. 99mTc-MAA must be administered during the preliminary examinations to evaluate a potential shunt from the liver to the lung or abdominal organs. The prophylactic embolization of all extrahepatic vessels, including gastroduodenal, right gastric, and other extrahepatic vessels, at the time of 99mTc-MAA assessment is recommended to avoid extrahepatic deposition of microspheres. These vessels and organs can revascularize quickly; therefore, the embolization should be performed close to the intended time of SIRT. In addition, a reassessment arteriogram is required just before SIRT to ensure that such revascularization has not occurred (2). Scintigraphy should be performed within 1 h of 99mTc-MAA injection to prevent false-positive extrahepatic activity due to free 99mTc. In such cases, pathologic uptake in the stomach should be ruled out before treatment. Free 99mTc is normally observed in SPECT/CT as diffuse uptake in the gastric mucosa, often in concordance with the thyroid gland on planar imaging, whereas pathologic uptake is seen as a focally increased accumulation. For the past 2 y, all patients in our department have received 600 mg of perchlorate by mouth 30 min before angiography to prevent nonspecific uptake of 99mTc-pertechnetate in the thyroid and stomach. During these 2 y, we have not observed any free 99mTc uptake in the stomach, as affirmed by SPECT/CT.
Obtaining a whole-body scan to predict possible lung damage due to liver-to-lung shunting is adequate. Detecting hot spots in other organs besides the liver with planar images is not always possible, and problems arise when these 2-dimensional images are used for more precise evaluations. Extrahepatic spots indirectly mark the possible locations of microsphere misplacement during therapy; however, planar image analysis can be difficult and lead to misinterpretation of possible extrahepatic locations because of the low spatial resolution of planar scintigraphic images. Furthermore, especially in the upper abdomen, the localization of several different organs within a relatively small region demands the analysis of tomographic images to accurately distinguish whether the 99mTc-MAA has accumulated in the liver or in some adjacent organ (24,25). Planar images cannot always make this distinction because of organ superposition. SPECT provides valuable additional information. SPECT images not only allow the lesions to be identified more accurately, and their arterial perfusion to be evaluated without superimposition, but also form a basis for image fusion with other pre- and posttherapeutic SPECT, PET, CT, and MR images. This process can be improved using SPECT/CT cameras, which avoid problems related to the interval between different studies, different positioning in different tomographs, and time-consuming software-based fusion as compared with hardware-based procedures (26).
Although SPECT or planar scanning is widely used before SIRT (2,5,27,28), the value of preradioembolization SPECT/CT has been investigated only in patients with colorectal cancer and hepatocellular carcinoma (28,29).
Denecke et al. (28) performed SPECT/CT on a small group of patients (n = 13) with colorectal cancer and found more gastrointestinal 99mTc-MAA uptake in SPECT/CT (31%) than in SPECT alone (15%). In a recently published prospective study, Hamami et al. (29) showed a sensitivity of 100% for SPECT/CT. They performed sixty-eight 99mTc-MAA examinations on 58 patients with hepatocellular carcinoma using clinical follow-up as the reference standard for proof of extrahepatic gastrointestinal perfusion abnormalities. None of the treated patients experienced gastrointestinal complications. In our study, we had more examinations and patients with different types of tumors. We found no significant difference in abdominal shunting between tumor types. Hamami et al. (29) mentioned that their study had a possible limitation in that all patients with gastrointestinal 99mTc-MAA deposition were excluded from treatment with SIRT if no causative gastrointestinal vessel was identified. Some of our patients were subject to the same limitation as those in the Hamami study. However, retrospective review of SPECT/CT images in our study revealed previously overlooked extrahepatic tracer accumulation in 3 patients who developed posttherapeutic gastrointestinal ulcers; this finding intensifies the significance and importance of this modality.
We demonstrated the different anatomic regions of extrahepatic 99mTc-MAA accumulation in detail (Table 3). An important and frequently overlooked anatomic region is the duodenum, which could be evaluated only by SPECT/CT; reviewing the coronal views of fusion scans was especially helpful. Duodenal 99mTc-MAA accumulation was present in 11 patients (14.5%), being identified as the only abnormality in 5 (Fig. 1).
Six patients (8%) showed an abnormal accumulation in the coil region, detected only on SPECT/CT images. Two reasons for this type of accumulation were small aberrant vessels ending in this region and an incompletely embolized vessel. Knowledge of the anatomic region of extrahepatic organ perfusion may help the radiologist to estimate the origin of the aberrant vessel.
SPECT/CT showed a high negative predictive value in our study. On the other hand, in 97% of patients with extrahepatic 99mTc-MAA accumulation, at least 1 aberrant vessel could be found on repeated angiograms. But as described in the “Results” section, the patients with overlooked 99mTc-MAA accumulation developed gastrointestinal ulcers despite no evident nonembolized aberrant vessels on routine angiographic reexamination, as also did 1 patient who did not undergo a second MAA examination after repeated angiography before SIRT. Thus, to increase the therapy, we recommend performing repeated test angiography and coil embolization of aberrant arteries until no extrahepatic accumulation can be detected in 99mTc-MAA SPECT/CT.
Alternatively, a superselective or lobar therapy could be done after an unremarkable superselective or lobar test angiogram. Otherwise, the therapy should be cancelled. For patients who have an extrahepatic accumulation only in the gallbladder, placement of the catheter distal to the cystic artery may be sufficient. A flowchart of the appropriate use of SPECT/CT is shown in Figure 2.

Appropriate use of 99mTc-MAA SPECT/CT in treatment planning for SIRT. *In some centers patients receive prophylactic cholecystectomy (29).
This study could also demonstrate the importance of experience in reviewing SPECT/CT scans. In the first weeks of using this modality, we overlooked extrahepatic accumulation in 6 scans or patients. Otherwise, the sensitivity, which was 82% in RLC, could be enhanced up to 100%.
The specificity of SPECT/CT was 93% in our study only because of false-positive findings as a result of free 99mTc in the stomach in 4 patients who did not have perchlorate applied before the examination. Thus, we recommend using perchlorate to improve the specificity of SPECT/CT.
CONCLUSION
99mTc-MAA SPECT/CT adds considerable value to the preprocedural planning of SIRT by identifying extrahepatic visceral sites at risk for post-SIRT complications. Experience plays an important role in reviewing SPECT/CT scans and may enhance the sensitivity. Imaging of SPECT/CT liver perfusion affected 29% of SIRTs, resulting in coil embolization of accessory vessels, infusion catheter repositioning, or procedure cancellation.
- © 2010 by Society of Nuclear Medicine
REFERENCES
- Received for publication December 30, 2009.
- Accepted for publication April 19, 2010.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- MIRD Pamphlet No. 29: MIRDy90--A 90Y Research Microsphere Dosimetry Tool
- Yttrium 90 Radioembolization for Hepatocellular Carcinoma
- A Prospective Study of Quantitative SPECT/CT for Evaluation of Lung Shunt Fraction Before SIRT of Liver Tumors
- Pharmacokinetics of 99mTc-MAA- and 99mTc-HSA-Microspheres Used in Preradioembolization Dosimetry: Influence on the Liver-Lung Shunt
- Intraarterial Hepatic SPECT/CT Imaging Using 99mTc-Macroaggregated Albumin in Preparation for Radioembolization
- Systematic Evaluation of Tumoral 99mTc-MAA Uptake Using SPECT and SPECT/CT in 502 Patients Before 90Y Radioembolization
- From the Angio Suite to the {gamma}-Camera: Vascular Mapping and 99mTc-MAA Hepatic Perfusion Imaging Before Liver Radioembolization--A Comprehensive Pictorial Review
- Image-Guided Personalized Predictive Dosimetry by Artery-Specific SPECT/CT Partition Modeling for Safe and Effective 90Y Radioembolization
- Radiodosimetric Estimates for Radioembolic Therapy of Liver Tumors: Challenges and Opportunities
- Clinical Feasibility of Fast 3-Dimensional Dosimetry of the Liver for Treatment Planning of Hepatocellular Carcinoma with 90Y-Microspheres
- Significance of Oral Administration of Sodium Perchlorate in Planning Liver-Directed Radioembolization