


Abstract
Hybrid imaging using PET in conjunction with CT-based coronary angiography (PET/CTCA) enables near-simultaneous quantification of myocardial blood flow (MBF) and anatomical evaluation of coronary arteries. CTCA is an excellent imaging modality to rule out obstructive coronary artery disease (CAD), but functional assessment is warranted in the presence of a CTCA-observed stenosis because the specificity of CTCA is relatively low. Quantitative H215O PET/CTCA may yield complementary information and enhance diagnostic accuracy. The purpose of this study was to evaluate the diagnostic accuracy of quantitative H215O PET/CTCA in a clinical cohort of patients with suspected CAD who underwent both cardiac H215O PET/CTCA and invasive coronary angiography (ICA). In addition, this study aimed to evaluate and compare the accuracy of hyperemic MBF versus coronary flow reserve (CFR). Methods: Patients (n = 120; mean age ± SD, 61 ± 10 y; 77 men and 43 women) with a predominantly intermediate pretest likelihood for CAD underwent both quantitative H215O PET/CTCA and ICA. A ≥50% stenosis at ICA or a fractional flow reserve ≤ 0.80 was considered significant. Results: Obstructive CAD was diagnosed in 49 of 120 patients (41%). The diagnostic accuracy of hyperemic MBF was significantly higher than CFR (80% vs. 68%, respectively, P = 0.02), with optimal cutoff values of 1.86 mL/min/g and 2.30, respectively. On a per-patient basis, the sensitivity, specificity, negative predictive value, and positive predictive value of CTCA were 100%, 34%, 100%, and 51%, respectively, as compared with 76%, 83%, 83%, and 76%, respectively, for quantitative hyperemic MBF PET. Quantitative H215O PET/CTCA reduced the number of false-positive CTCA studies from 47 to 6, although 12 of 49 true-positive CTCAs were incorrectly reclassified as false-negative hybrid scans on the basis of (presumably) sufficient hyperemic MBF. Compared with CTCA (61%) or H215O PET (80%) alone (both P < 0.05), the hybrid approach significantly improved diagnostic accuracy (85%). Conclusion: The diagnostic accuracy of quantitative H215O PET/CTCA is superior to either H215O PET or CTCA alone for the detection of clinically significant CAD. Hyperemic MBF was more accurate than CFR, implying that a single measurement of MBF in diagnostic protocols may suffice.
- hyperemic MBF
- coronary flow reserve
- coronary artery disease
- diagnostic accuracy
- cardiac hybrid H215O PET/CT
Accurate noninvasive assessment of coronary artery disease (CAD) and its functional consequences is a challenging task. There are several cardiac noninvasive imaging techniques, such as SPECT, stress echocardiography, MRI, and PET, for diagnosing and evaluating the extent and severity of myocardial ischemia resulting from CAD. CT coronary angiography (CTCA) has gone through a rapid development during recent years and enables visualization of the coronary artery lumen and wall and provides information about the presence and morphology of coronary artery lesions. Several studies have shown that CTCA accurately rules out obstructive CAD. However, because the positive predictive value (PPV) of CTCA is moderate, functional assessment is also needed in the presence of CTCA-graded obstructive CAD (1,2). Approximately half of the lesions deemed obstructive with CTCA are indeed hemodynamically significant as evaluated with fractional flow reserve (FFR) (3). Yet the invasive nature of conventional coronary angiography and FFR limits their broad application for initial diagnostic purposes. Therefore, the noninvasive combined assessment of coronary anatomy and perfusion can yield complementary information and may reduce the number of diagnostic invasive coronary angiographies (ICAs) by a more judicious referral of patients to the catheterization lab. The integration of anatomy and function is possible within a single scan session with the currently available cardiac PET/CT protocols (4–6). PET has the unique ability to quantify myocardial blood flow (MBF) in absolute terms, generally with less radiation exposure to the patient, as compared with SPECT (7). The quantitative nature of a dynamic PET protocol provides several parameters, such as resting and hyperemic MBF and coronary flow reserve (CFR). In a previous study, Hajjiri et al. demonstrated that hyperemic MBF might be more accurate than CFR or visual defect grading for detecting obstructive CAD (8). More recently, in a study by Kajander et al. the combination of quantitative PET (i.e., without visual qualitative grading) and CTCA (PET/CTCA) demonstrated a 95% sensitivity and a 100% specificity and offered a higher diagnostic accuracy than either CTCA or PET alone (6). Nonetheless, limited data are available on the accuracy of cardiac quantitative PET/CTCA and the value of hyperemic MBF and CFR for the evaluation of CAD. Therefore, the present study evaluated the accuracy of quantitative H215O PET/CTCA in a clinical cohort of patients suspected of CAD who underwent both cardiac H215O PET/CTCA imaging and ICA.
MATERIALS AND METHODS
Patient Population
Data were obtained from a clinical cohort of patients being evaluated for CAD and therefore referred for CTCA, coronary artery calcium (CAC) scoring, and PET MBF measurements on a PET/CT scanner (Gemini TF 64; Philips Healthcare). Patients were referred because of stable (atypical) angina or an elevated risk for CAD (presence of 2 or more risk factors) in the absence of symptoms. Hypertension was defined as a blood pressure of ≥140/90 mm Hg or the use of antihypertensive medication. Hypercholesterolemia was defined as a total cholesterol level of ≥5 mmol/L or treatment with cholesterol-lowering medication. Patients were classified as having diabetes if they were receiving treatment with oral hypoglycemic drugs or insulin. A positive family history of CAD was defined by the presence of CAD in first-degree relatives younger than 55 y in men or 65 y in women. Exclusion criteria were atrial fibrillation, second- or third-degree atrioventricular block, impaired renal function, symptomatic asthma, pregnancy, or a documented history of CAD. A history of CAD was defined as a prior percutaneous coronary intervention, coronary artery bypass graft surgery, or a previous myocardial infarction. Electrocardiography did not show signs of a previous myocardial infarction, and echocardiography showed normal left-ventricular function without wall motion abnormalities in all patients. A total of 120 patients met these criteria and underwent ICA after PET/CTCA (mean interim between studies, 70 d) without a documented cardiac event between PET/CTCA examinations. The indication for ICA was left at the discretion of the referring physician. CAD pretest likelihood was determined according to the criteria of Diamond and Forrester (9).
The need for written informed consent was waived by the institutional review board (local ethics committee) because of the nature of the study, which solely had clinical data collection.
PET
The PET/CTCA protocol is shown in Figure 1. The PET sequence has been described in detail previously (10,11). Parametric MBF images, showing MBF on the voxel level, were generated, and quantitative analysis was performed using Cardiac VUer software developed in-house (12). In short, input functions were obtained using automatic segmentation of dynamic images, after which parametric images were obtained as described previously (12). Then, parametric images of perfusable tissue fraction were used for semiautomatic heart segment definition based on the 17-segment model of the American Heart Association (13). Obtained volumes of interest were then projected onto dynamic images, and time–activity curves were extracted for each myocardial segment, for each of the 3 vascular territories (right coronary artery [RCA], left anterior descending artery [LAD], and circumflex artery [CX]), and for the entire left ventricle. Finally, segmental and global MBF was calculated using these time–activity curves and nonlinear least squares. MBF was expressed in mL/min/g of perfusable tissue. Two experienced readers masked to the ICA data reviewed all PET scans.

Cardiac H215O PET/CTCA protocol. LD CT = low-dose CT for attenuation correction.
CTCA
Patients with a stable heart rate below 65 bpm (either spontaneous or after the administration of oral or intravenous metoprolol) underwent a CT scan for calcium scoring and CTCA as previously described (11). All CT scans were analyzed with a 3-dimensional workstation (Brilliance, Philips) by an experienced radiologist and cardiologist who were masked to the ICA results.
ICA
ICA was performed according to standard clinical protocols. The coronary tree was divided into a 16-segment coronary artery model modified from the American Heart Association (14). Significant CAD was defined by a visually graded stenosis ≥ 50%. When FFR measurements were performed, visual grading was overruled by FFR, where a value ≤ 0.80 was considered significant. FFR was measured at the discretion of the interventional cardiologist performing the ICA procedure. A 0.035-cm (0.014-in) sensor-tipped guide wire (Volcano Corp.) was used, which was introduced through a 6- or 7-French guiding catheter, calibrated, and advanced into the coronary artery. Furthermore, adenosine was infused either intravenously (140 μg/kg/min) or intraarterially (120 μg) in the RCA and left coronary artery, to induce maximal coronary hyperemia. The FFR was calculated as the ratio of the mean distal intracoronary pressure measured by the pressure wire to the mean arterial pressure measured by the coronary catheter (15). All images were interpreted by at least 2 experienced interventional cardiologists who were masked to the CTCA and PET data, and subsequently a consensus reading was performed.
Interpretation of Imaging Results
The analysis was performed on both a per-patient and a per-vessel basis. The 4 main vessels—left main artery, LAD, RCA, and left CX—were assessed on CTCA, with stenoses ≥ 50% classified as significant. Comparison of CTCA with ICA or, when available, ICA plus FFR was performed on an intention-to-diagnose basis, and therefore noninterpretable segments on CTCA were considered as significant. In PET, the 3 main vessel regions (LAD, RCA, and left CX) were analyzed. The anatomic information provided by the CTCA scan was used to assess coronary dominance and to allocate a coronary lesion to its subtended vascular territory on the PET perfusion images. In addition, region analysis on a per-segment basis was performed, whereby a perfusion defect of at least 2 adjacent segments was assigned to a vascular territory. Subsequently, this regional perfusion value consisting of at least 2 adjacent segments, instead of the mean MBF of the predefined vascular territory, was used for further analyses. The optimal cutoff values for hyperemic MBF and CFR were calculated using a receiver-operating-characteristic (ROC) curve analysis. A hyperemic MBF ≤ 1.86 mL/min/g and a CFR ≤ 2.30 were considered abnormal (see the “Results” section). The results of PET/CTCA were interpreted as follows. When both CTCA and PET were normal, the vessel was considered normal. A vessel was considered significantly stenosed when a significant stenosis on CTCA was detected in combination with a perfusion abnormality in the region of the corresponding vessel. A vessel was considered nonsignificantly stenosed in the presence of a significant stenosis on CTCA and the absence of a perfusion defect. In the case of a nonsignificant stenosis on CTCA and a perfusion abnormality, the vessel was presumably affected as a result of microvascular dysfunction and was considered nonsignificantly stenosed. Combined anatomic and functional information was gained by mental integration of the information from CTCA and quantitative MBF imaging.
Statistical Analysis
Continuous variables are presented as mean values ± SD, whereas categoric variables are expressed as actual numbers. The performance of PET, CTCA, and PET/CTCA for the diagnosis of CAD, compared with ICA, or when available ICA in combination with FFR measurements, were determined with sensitivity, specificity, negative predictive value (NPV), PPV, and accuracy on a per-patient and per-vessel basis. Furthermore, a head-to-head comparison between hyperemic MBF and CFR was performed to assess the diagnostic accuracy of these PET perfusion parameters.
An ROC curve analysis was used to define optimal cutoff values for hyperemic MBF and CFR in the current study population. A McNemar nonparametric test was used to compare the diagnostic accuracy of CTCA, PET, and PET/CTCA with ICA. A P value ≤ 0.05 was considered statistically significant. All statistical analyses were performed using the SPSS software package (version 16.0; SPSS) and MedCalc (version 11.6.0.0; MedCalc Software).
RESULTS
Patient characteristics (n = 120) are shown in Table 1). In 37 patients, ICA was complemented with a FFR measurement because of the presence of an intermediate coronary lesion. No apparent significant lesion was detected on ICA in 71 patients; 20 of these 71 patients had an ICA in combination with an FFR measurement. Forty-nine patients displayed significant coronary artery stenosis (i.e., ≥50%) at ICA (17 had undergone an FFR measurement). Overall, 92 of the 360 analyzed vessels were graded significant on the basis of visual assessment or FFR measurement. Table 2 summarizes the hemodynamic characteristics. During adenosine-induced hyperemia, only heart rate increased significantly, compared with baseline, whereas no significant changes occurred with respect to blood pressures. Mean heart rate during CTCA was 57 ± 7 beats per minute, which was slightly lower than heart rate during resting perfusion imaging (61 ± 8, P < 0.01).
Patient Characteristics (n = 120)
Hemodynamic Parameters During Scan Procedure
Hyperemic MBF Versus CFR for Detecting Obstructive CAD
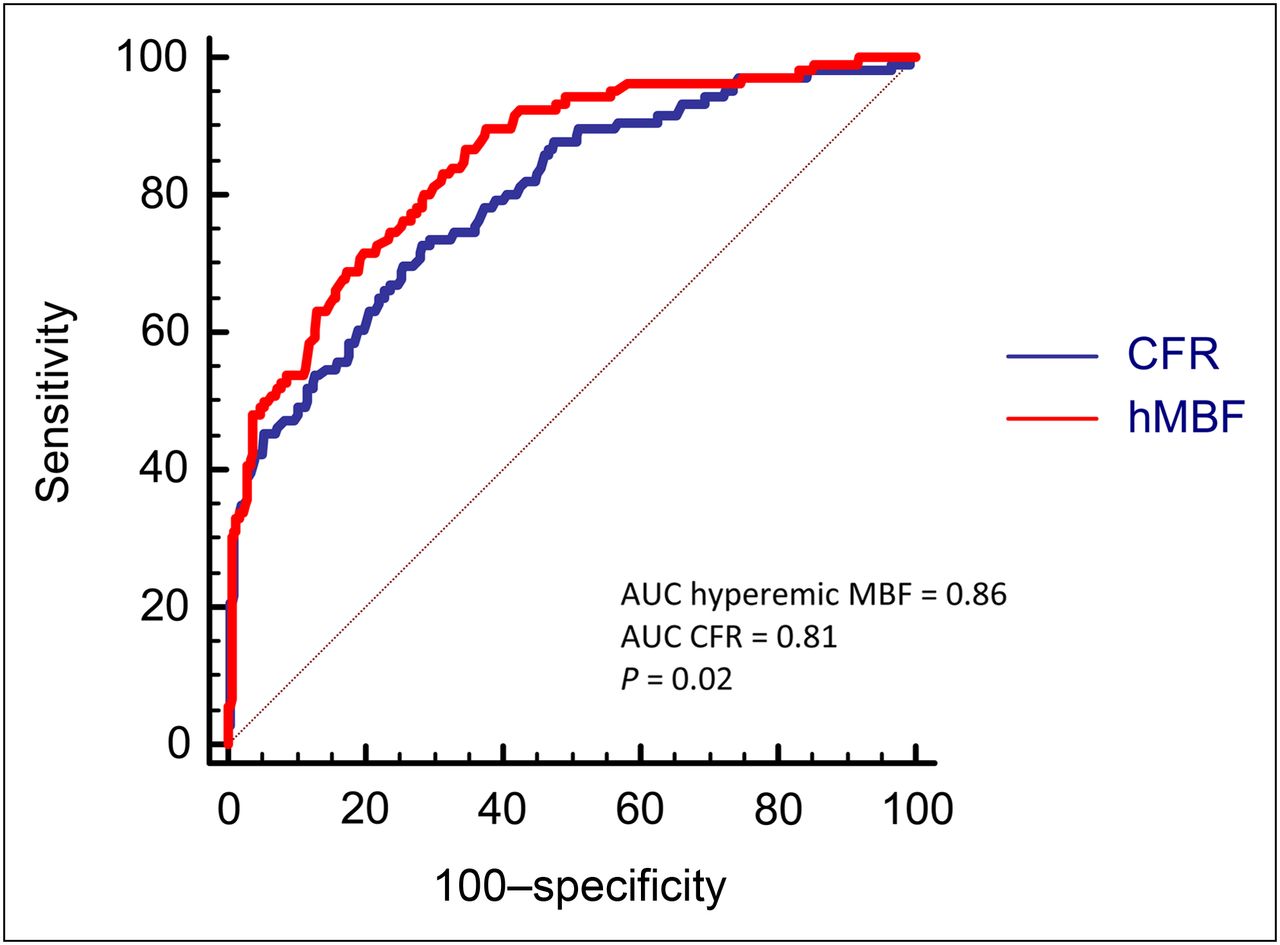
The area-under-the-ROC curve (AUC) analysis of hyperemic MBF (AUC, 0.86; 95% confidence interval [CI], 0.81–0.90) was greater than that of CFR (AUC, 0.81; 95% CI, 0.75–0.86) for the detection of obstructive CAD (P = 0.02; Fig. 2). The optimal cutoff values, which were calculated on a per-vessel basis, were ≤1.86 mL/min/g for hyperemic MBF and ≤2.30 for CFR (Fig. 2). The determination of a cutoff value only in those vessels with obstructive CAD on CTCA revealed that the optimal cutoff value for hyperemic MBF (AUC, 0.83; 95% CI, 0.77–0.89) and CFR (AUC, 0.78; 95% CI, 0.71–0.84) was similar to those obtained in the whole population.
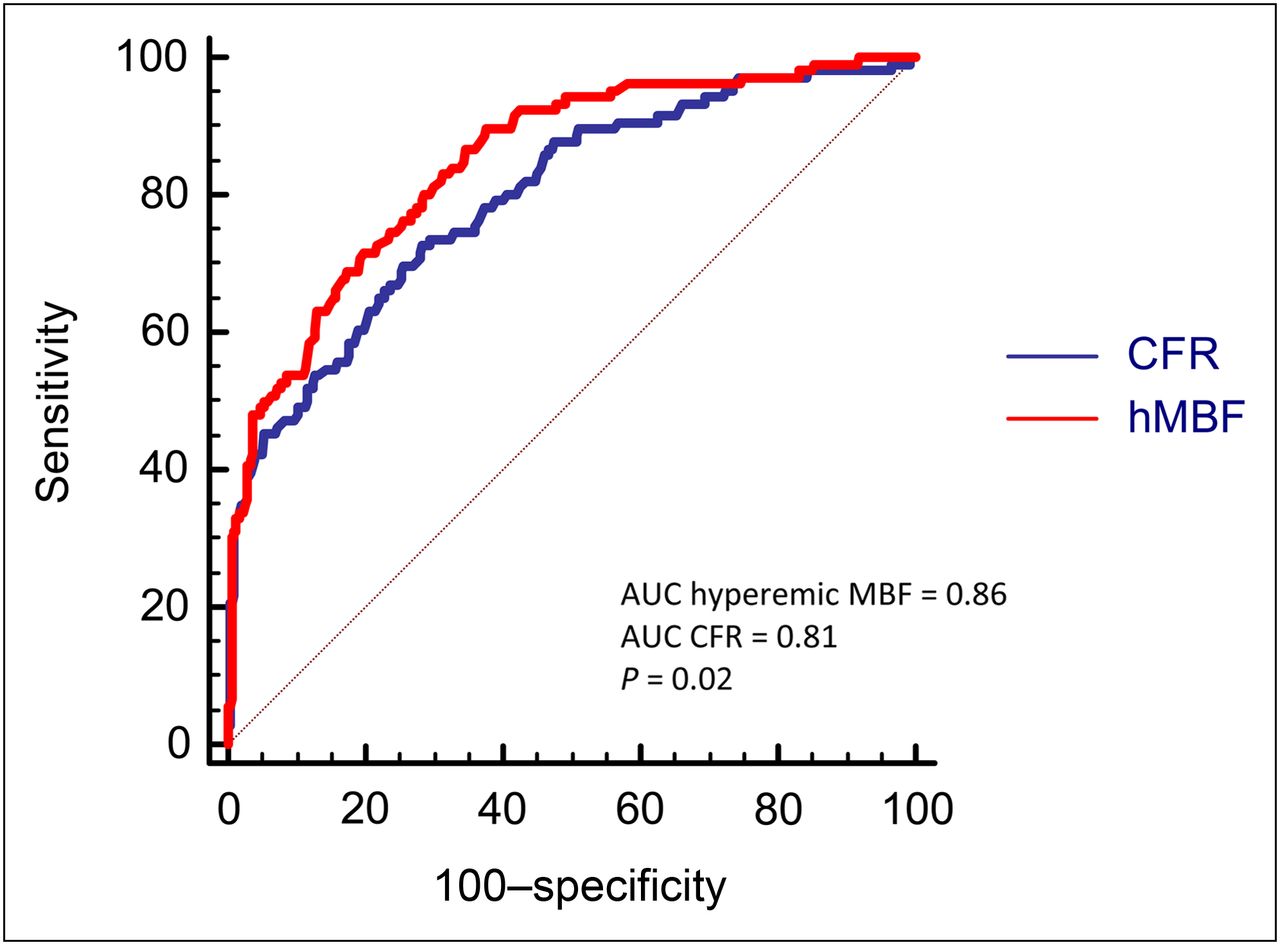
Hyperemic MBF vs. CFR for detection of CAD. ROC curves for PET parameters tested for all coronary vessels are shown. CFR = coronary flow reserve; hMBF = hyperemic myocardial blood flow.
Diagnostic Accuracy of CAC Score, 64-Slice CTCA, and Cardiac PET
The mean CAC score (±SD) in the studied population was 442 ± 711 and was significantly lower in patients without obstructive CAD than in those with obstructive CAD on ICA (359 ± 650 and 564 ± 784, respectively; P = 0.02) (Fig. 3). The diagnostic performance of CTCA alone for detecting obstructive CAD on a per-patient and per-vessel basis is displayed in Figures 4 and 5. The sensitivity and NPV of CTCA were excellent (100%), whereas specificity (34%) and PPV (51%) performed poorly in the identification of significant lesions at ICA on a per-patient basis. Similar diagnostic trends were observed on a per-vessel analysis, although specificity increased notably (72%) without an appreciable change in PPV (45%).

Log-transformed CAC score given for patients with and without obstructive CAD on ICA.

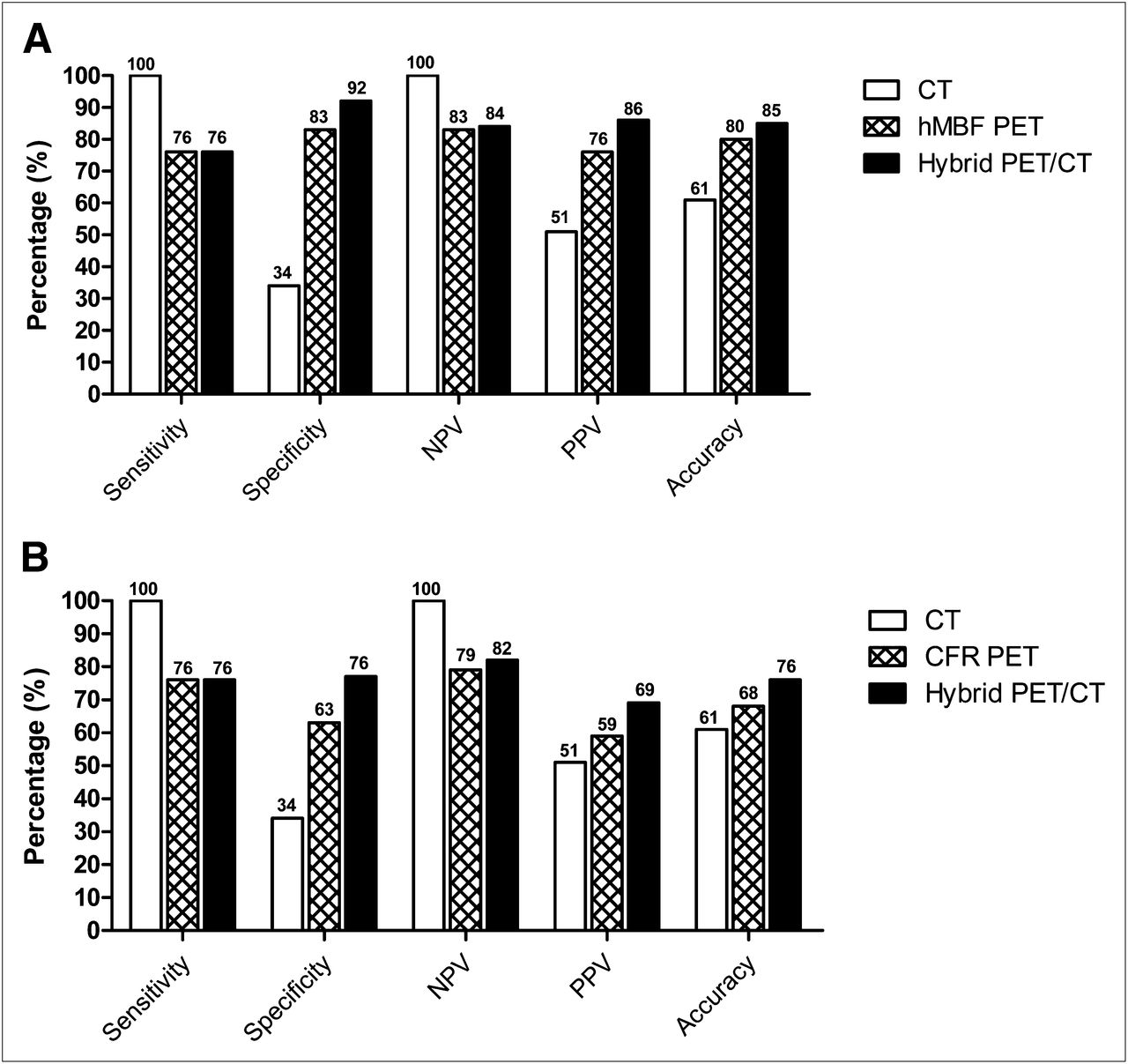
Per-patient basis: diagnostic accuracy of noninvasive cardiac imaging. Sensitivity, specificity, NPV, PPV, and accuracy of stand-alone CT, PET, and hybrid imaging. (A) Analysis using hyperemic MBF as perfusion parameter. (B) Analysis using CFR as perfusion parameter. hMBF = hyperemic myocardial blood flow.

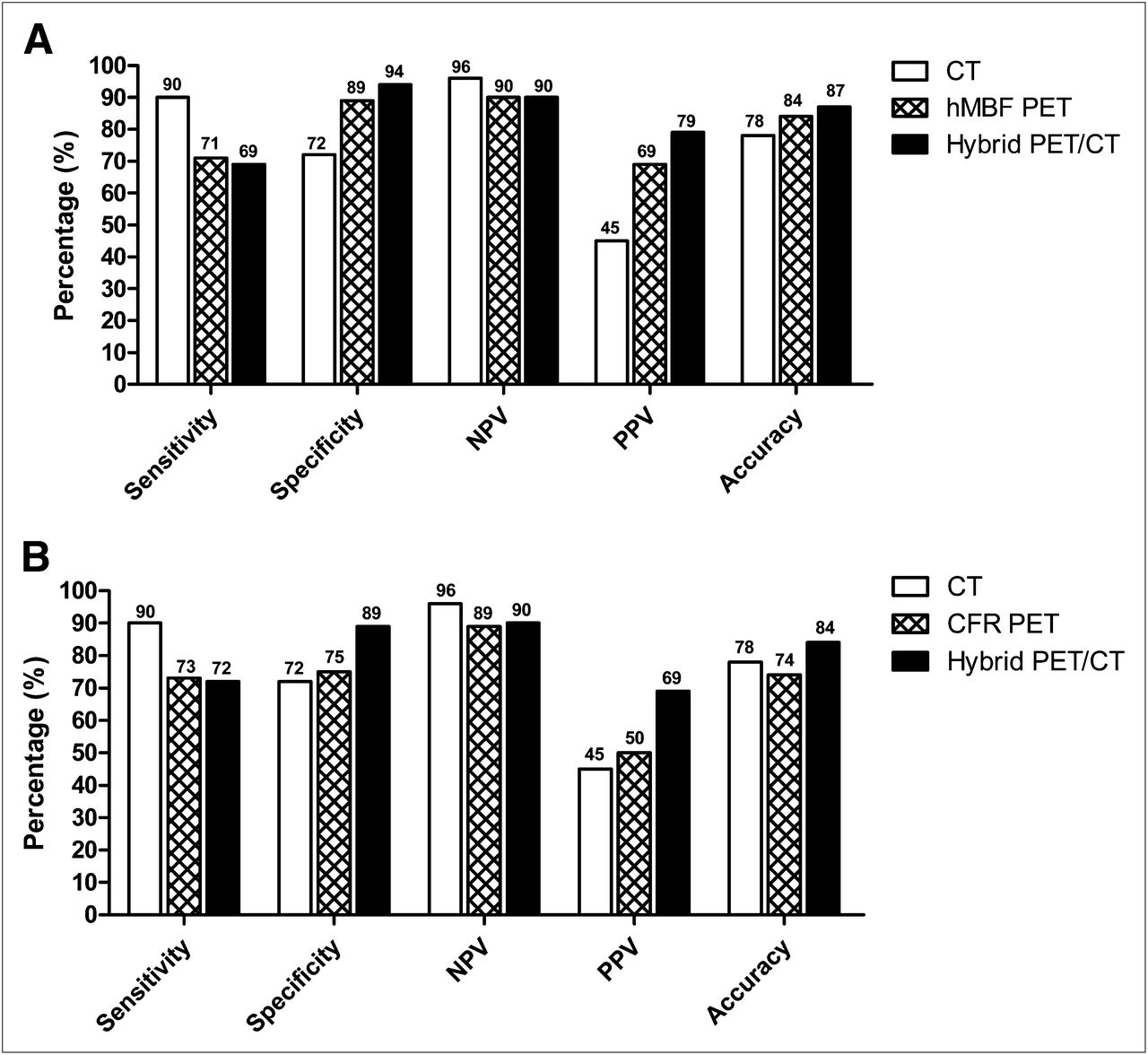
Per-vessel basis: diagnostic accuracy of noninvasive cardiac imaging. Sensitivity, specificity, NPV, PPV, and accuracy of stand-alone CT, PET, and hybrid imaging. (A) Analysis using hyperemic MBF as perfusion parameter. (B) Analysis using CFR as perfusion parameter. CFR = coronary flow reserve; hMBF = hyperemic myocardial blood flow.
Figures 4 and 5 display the diagnostic values for hyperemic MBF and CFR to detect obstructive CAD on a per-patient and per-vessel level. On a per-patient level, sensitivity (76 vs. 76%, P = 1.00) was comparable for hyperemic MBF and CFR, whereas specificity (83 vs. 63%, P < 0.01) was significantly higher for hyperemic MBF. Hence, total diagnostic accuracy was superior for hyperemic MBF (80 vs. 68%, P = 0.02). Comparable results were documented at a per-vessel analysis, as depicted in Figure 5.
Diagnostic Accuracy of Cardiac PET/CTCA
Supplemental Figures 1 and 2 (supplemental materials are available online only at http://jnm.snmjournals.org) show 2 typical examples of cases in which the anatomic lesions on CTCA were as proven functionally significant with PET, which was in concordance with ICA. As depicted in Figure 4A, the combination of CTCA and hyperemic MBF increased specificity (from 34% and 83%, respectively, to 92%; P < 0.001 and P = 0.03, respectively) and overall diagnostic accuracy (from 61% and 80%, respectively, to 85%; P < 0.01 and P = 0.03, respectively) in the hybrid protocol on a per-patient basis. However, the high sensitivity of CTCA alone was reduced by adding hyperemic MBF to the hybrid diagnostic evaluation (from 100% and 76%, respectively, to 76%; P < 0.001 and P = 1.00, respectively); NPV was also reduced (from 100% and 83%, respectively, to 84%; P < 0.001 and P = 1.00, respectively). Comparable trends were observed when CFR as the perfusion parameter was used in combination with CTCA (Fig. 4B). Overall, hybrid diagnostic accuracy, however, was highest using hyperemic MBF as the perfusion parameter, compared with CFR on a per-patient (85% vs. 76%, P = 0.04; Fig. 4) and per-vessel (87 vs. 84%, P = 0.05; Fig. 5) analysis. As also listed in Table 3, the hybrid protocol reduced the number of false-positive patients who displayed a stenosis on CTCA in the absence of a significant lesion at ICA (47/71 patients [66%]). Of these 47 patients, 41 were subsequently correctly reclassified as negative on the basis of sufficient hyperemic MBF in all vascular territories. Such a scenario is exemplified in Supplemental Figure 3. For CFR, this correct reclassification number was only 30 (from 47 to 17 patients, Table 4). On the other hand, 12 of 49 CTCA-positive patients (24%) with a least 1 significant lesion at ICA were incorrectly reclassified as negative in the hybrid approach based on (presumably) sufficient hyperemic MBF or CFR in all vascular territories. Supplemental Figure 4 illustrates such a misclassification. Tables 5 and 6 list these results on a per-vessel level, which essentially yielded comparable results.
Results per Patient Using Hyperemic MBF as Perfusion Parameter
Results per Patient Using CFR as Perfusion Parameter
Results per Vessel Using Hyperemic MBF as Perfusion Parameter
Results per Vessel Using CFR as Perfusion Parameter
DISCUSSION
The present study was conducted to evaluate the diagnostic accuracy of quantitative H215O PET/CTCA for the detection of CAD. The PET perfusion results indicate that hyperemic MBF is superior to CFR and yields a diagnostic accuracy of 80%. Furthermore, combining CTCA with hyperemic MBF in the hybrid protocol enhanced diagnostic accuracy significantly to 85%, mediated through an increase in specificity and PPV as compared with hyperemic MBF alone.
Traditionally, myocardial perfusion imaging for the detection of CAD with PET has been based on qualitative visual grading using 13NH3 and 82Rb (static) tracer uptake images. This approach conveys good diagnostic accuracy, and the pooling of data suggests that myocardial perfusion imaging with PET is superior to alternative diagnostic imaging techniques (16). Although PET additionally allows for the absolute quantification of MBF, there is a paucity of data on the diagnostic accuracy of hyperemic MBF and CFR. In the present study, hyperemic MBF was superior to CFR in the detection of CAD. Previous studies using quantitative 13NH3 PET have shown inconclusive results on this topic. In small-scaled studies, Hajjiri et al. observed a slightly higher accuracy for hyperemic MBF, whereas Muzik et al. concluded that CFR was more accurate, although the differences were small (8,17). These observations, in combination with the currently presented data, imply that a single measurement of hyperemic MBF could suffice in diagnostic imaging protocols. The optimal diagnostic cutoff value of 1.86 mL/min/g was in line with the value observed by Hajjiri et al. (1.85 mL/min/g) and somewhat higher than the best discriminatory value documented by Muzik et al. (1.52 mL/min/g), with comparable diagnostic accuracy (AUC ranging from 0.79 to 0.91, compared with 0.86 observed in the present study) (8,17). The discriminatory value of hyperemic MBF in those patients with obstructive CAD on CTCA was identical to the cutoff value of hyperemic MBF in the entire study population. In contrast, a recent study by Kajander et al., using H215O PET in 107 patients, displayed an optimal cutoff value of 2.5 mL/min/g with a markedly higher AUC at analysis (0.94) (6). Although methodologic considerations between imaging protocols and patient selection may account for some of these discrepancies, the selection of an optimal threshold to reproduce such a high diagnostic yield may prove difficult in clinical practice. Studies in patients without CAD have clearly demonstrated that the reference range of hyperemic MBF is relatively broad because of physiologic variation in minimal coronary microvascular resistance, which is related to patient characteristics such as age, sex, and CAD risk factors (11,18–20). Because hyperemic MBF is governed by the (potential) presence of an epicardial coronary lesion and microvascular resistance, a cutoff value to identify an obstructive coronary lesion will vary according to the conductance capacity of the microvascular bed in each individual patient. Indeed, animal experiments using microspheres and several quantitative PET studies using various perfusion tracers in humans have revealed that the relationship between hyperemic MBF and epicardial coronary lesion severity is characterized by considerable scatter (21–24). This physiologic variation of hyperemic MBF for a given epicardial coronary lesion hampers the discriminatory power of a single threshold to identify a hemodynamic significant stenosis. The correction of MBF reference values for specific patient subgroups (e.g., age and sex) may improve diagnostic accuracy, although further studies are obviously warranted to test this hypothesis. Although determining an optimal hyperemic MBF cutoff value is rather difficult, the absolute quantification of MBF may provide an added advantage over relative perfusion imaging, particularly in patients with triple-vessel disease or microvascular dysfunction, for whom the relative assessment of coronary perfusion may fail to uncover ischemia due to balanced hypoperfusion.
In line with previous reports, the sensitivity and NPV of CTCA were excellent. Specificity and PPV, however, were moderate and poor, respectively, yielding an overall diagnostic accuracy of 61% on a per-patient basis. Specificity and PPV—even though within the observed range of pooled analysis from multiple studies—appeared to be somewhat lower than generally reported (25). That observation was previously documented in a similar clinical cohort of patients (1,2,26). Several factors may account for these results, including relatively sensitive grading of coronary plaques at CTCA with a threshold of significance of 50% and an analysis based on an intention to diagnose for which all of the coronary segments were included in the grading, independent of image quality. These results further highlight the general consensus that CTCA is an excellent tool to rule out obstructive CAD, whereas the low PPV warrants further functional testing in the case of a positive CTCA result. In fact, roughly half of lesions deemed positive on CTCA- actually induce myocardial ischemia as documented with SPECT (27–29).
The combination of quantitative perfusion assessment with PET and coronary anatomy with CTCA significantly improved the diagnostic accuracy, compared with either imaging technique alone. The hybrid approach was particularly useful to reduce the number of false-positive CTCA findings because the addition of hyperemic MBF could assess the hemodynamic significance of CTCA-observed lesions (Supplemental Fig. 3). On the downside, the excellent sensitivity and NPV of CTCA alone were reduced by the hybrid approach. The latter is the result of an increase in false-negative hybrid scans as illustrated in Supplemental Figure 4.
Overall, these results are in line with previous studies on the diagnostic surplus value of hybrid imaging with PET/CTCA and SPECT/CTCA that consistently display particularly enhanced specificity and PPV with the addition of myocardial perfusion imaging to CTCA (6,29–32). Of these studies, only Kajander et al. used quantitative perfusion PET in the hybrid protocol, and thus their study closely resembles the imaging methodology of the current study (6). In comparison with Kajander et al., however, the current diagnostic accuracy was lower (85% vs. 98%), with a particular poorer performance regarding sensitivity (76% vs. 95%) and to a lesser extent specificity (92% vs. 100%) on a per-patient basis (6). Several methodologic issues may account for this discrepancy. First, and in contrast to Kajander et al., the current study was retrospective, leading to referral bias for which the clinical decision to subject a patient to an invasive coronary angiogram was likely based on an abnormal PET/CTCA finding. Therefore, compared with the study of Kajander et al., the lower diagnostic performance in this study may have been caused by referral bias. Nonetheless, the prevalence of obstructive CAD was similar between studies (both 41%), suggesting that the studied patient populations were comparable. Second, the cutoff values for hyperemic MBF and CFR were not defined a priori but optimized retrospectively using ROC curve analysis in the currently described study population. Prospective trials validating the obtained cutoff values are warranted. Third, FFR measurements were not routinely performed in all patients with an intermediate coronary stenosis. Because agreement between the functional severity of a stenosis as measured with FFR and visual grading may show disparities, the currently used gold standard of invasive angiography is by itself limited (33). Fourth, although care was taken to match individual coronary anatomy to perfusion territories in the evaluation of the PET/CTCA scan, software to generate fusion images of CTCA and PET was not commercially available from the manufacturer of our installed system. Some studies have demonstrated that fused hybrid imaging as compared with side-by-side analysis may slightly improve diagnostic accuracy (34–36). Finally, parametric perfusion images were generated by different software packages developed in-house in both studies (12,37). Although these packages use the same validated single-compartment model to quantify MBF, differences in, for example, arterial input definition and automated myocardial segmentation may cause a systematic bias. This may therefore be related to the observed discrepancy in optimal cutoff value (1.86 vs. 2.5 mL/min/g). Comparative studies between software packages are warranted. Finally, in the current study, H215O, which is not widely available and requires an onsite cyclotron because of its short half-life, was used as a perfusion tracer. In addition, because H215O water is metabolically inert and freely diffusible, signal-to-noise ratios and contrast between tracer concentration in the blood and in the myocardium is low, compared with other perfusion tracers such as 13N-ammonia and 82Rb. Recently, signal-to-noise ratios of H215O cardiac PET using blood-pool subtraction techniques have become more sufficient (37). Furthermore, generation of high-quality parametric perfusion images is now feasible (12). Nonetheless, relative flow imaging with H215O PET still faces many challenges, and studies investigating the additive value of quantitative MBF imaging, compared with relative flow PET are scarce (38). Clearly, more prospective studies are warranted to establish the clinical value of relative perfusion imaging with H215O as a perfusion tracer.
Irrespective of these methodologic considerations, the results from the current study confirm that quantitative perfusion PET has the ability to diagnose CAD with fairly good accuracy, and PET/CTCA further improves the diagnostic yield. Nonetheless, several important issues remain to be addressed such as whether qualitative or quantitative PET (or their combination) conveys the best results because data on this topic are scarce (8,38). The results of prospective studies further exploring the diagnostic accuracy of PET/CTCA are therefore eagerly awaited.
CONCLUSION
Absolute hyperemic MBF measurements with PET are superior to CFR for the diagnosis of obstructive CAD. The addition of CTCA with quantitative PET/CTCA improves diagnostic accuracy significantly.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Suzette van Balen, Amina Elouahmani, Judith van Es, Robin Hemminga, Femke Jongsma, Nghi Pham, and Nasserah Sais for performing the scans and Henri Greuter, Marissa Rongen, Robert Schuit, and Kevin Takkenkamp for producing 15O-water.
Footnotes
Published online Dec. 11, 2012.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication February 18, 2012.
- Accepted for publication August 6, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Determining Hemodynamically Significant Coronary Artery Disease: Patient-Specific Cutoffs in Quantitative Myocardial Blood Flow Using [15O]H2O PET Imaging
- Danish study of Non-Invasive Testing in Coronary Artery Disease 3 (Dan-NICAD 3): study design of a controlled study on optimal diagnostic strategy
- Diagnostic Performance of Hybrid Cardiac Imaging Methods for Assessment of Obstructive Coronary Artery Disease Compared With Stand-Alone Coronary Computed Tomography Angiography: A Meta-Analysis
- Clinical Quantification of Myocardial Blood Flow Using PET: Joint Position Paper of the SNMMI Cardiovascular Council and the ASNC
- Coronary CT Angiography With PET Perfusion Imaging: Hybrid or Hype?
- Prognostic Value of Coronary CT Angiography With Selective PET Perfusion Imaging in Coronary Artery Disease
- Quantitative Assessment of Coronary Microvascular Function: Dynamic Single-Photon Emission Computed Tomography, Positron Emission Tomography, Ultrasound, Computed Tomography, and Magnetic Resonance Imaging
- Myocardial Viability: Survival Mechanisms and Molecular Imaging Targets in Acute and Chronic Ischemia
- Fractional Flow Reserve Returns to Its Origins: Quantitative Cardiac Positron Emission Tomography
- Integrated Myocardial Perfusion Imaging Diagnostics Improve Detection of Functionally Significant Coronary Artery Stenosis by 13N-ammonia Positron Emission Tomography
- Integration of Quantitative Positron Emission Tomography Absolute Myocardial Blood Flow Measurements in the Clinical Management of Coronary Artery Disease
- Doppler-Derived Intracoronary Physiology Indices Predict the Occurrence of Microvascular Injury and Microvascular Perfusion Deficits After Angiographically Successful Primary Percutaneous Coronary Intervention
- Relative Flow Reserve Derived From Quantitative Perfusion Imaging May Not Outperform Stress Myocardial Blood Flow for Identification of Hemodynamically Significant Coronary Artery Disease
- Quantitative Assessment of Myocardial Perfusion in the Detection of Significant Coronary Artery Disease: Cutoff Values and Diagnostic Accuracy of Quantitative [15O]H2O PET Imaging