


Abstract
The objective of this study was to analyze the safety and efficacy of the 177Lu-labeled DOTAGA-based prostate-specific membrane antigen (PSMA) ligand 177Lu-DOTAGA-(I-y)fk(Sub-KuE) (177Lu-PSMA) in patients with metastatic castration-resistant prostate cancer (mCRPC). Methods: Fifty-six mCRPC patients underwent PSMA radioligand therapy (RLT) with 177Lu-PSMA. 68Ga-PSMA-(N,N'-bis-[2-hydroxy-5-(carboxyethyl)benzyl]ethylenediamine-N,N'-diacetic acid) (68Ga-PSMA) PET/CT was used for patient selection and follow-up after PSMA RLT. Hematologic status, renal function, and serum prostate-specific antigen levels were documented before and after therapy. Dosimetry was performed in 30 patients. Results: 177Lu-PSMA demonstrated high absorbed tumor doses (median, 3.3 mGy/MBq) compared with the levels in normal organs. Parotid glands received higher doses (1.3 mGy/MBq) than kidneys (0.8 mGy/MBq). All patients tolerated the therapy without any acute adverse effects. Except for mild reversible xerostomia in 2 patients, no long-term side effects were observed. There was a small but statistically significant reduction in erythrocyte and leukocyte counts; only the reduction in erythrocyte counts decreased slightly below the reference range. No thrombocytopenia occurred. The severity of pain was significantly reduced in 2 of 6 patients (33.3%). A decrease in prostate-specific antigen levels was noted in 45 of 56 patients (80.4%). Of 25 patients monitored for at least 6 mo after 2 or more PSMA RLT cycles, a molecular response evaluation (68Ga-PSMA PET/CT) revealed partial remission in 14, stable disease in 2, and progressive disease in 9 patients. Contrast-enhanced CT revealed partial remission in 5, stable disease in 13, and progressive disease in 7 patients. The median progression-free survival was 13.7 mo, and the median overall survival was not reached during follow-up for 28 mo. Conclusion: PSMA RLT with 177Lu-PSMA is feasible, safe, and effective in end-stage progressive mCRPC with appropriate selection and follow-up of patients by 68Ga-PSMA PET/CT through application of the concept of theranostics.
Metastatic castration-resistant prostate cancer (mCRPC) has a poor prognosis, with an estimated 27,540 prostate cancer deaths in the United States in 2015 (1). The novel agents abiraterone and enzalutamide provide limited survival benefits of 3.9 and 4.8 mo, respectively (2,3). Overall survival has been reported to improve by 3.6 mo with 223Ra-chloride, but it is indicated for patients with skeletal metastases only (4). Immunotherapy with sipuleucel-T confers a survival benefit of a few months but has no impact on the time to progression and is associated with immunologic adverse events (5).
Prostate-specific membrane antigen (PSMA) is a glutamate carboxypeptidase II overexpressed in prostate cancer (6). In 2002, Pomper et al. performed the first in vivo study with a urea-based compound targeting PSMA for diagnosis (6). Their high-affinity, urea-based inhibitor of PSMA maintained target specificity after radiolabeling with 68Ga (7). 68Ga-labeled PSMA inhibitors with N,N'-bis-[2-hydroxy-5-(carboxyethyl)benzyl]ethylenediamine-N,N'-diacetic acid as a chelator (68Ga-PSMA) have been successfully used for the imaging of prostate cancer, with high sensitivity and specificity (8,9). These small molecules penetrate solid tumors and, compared with whole antibodies, have the advantage of rapid clearance from blood. Radioimmunotherapy with PSMA antibody 177Lu-DOTA-J591 was limited by myelosuppression and nonhematologic toxicity, with a maximum tolerated activity per cycle of 2,450 MBq/m2 (10). Zechmann et al. performed endoradiotherapy of mCRPC using a PSMA small molecule labeled with 131I (11). The 68Ga-, 111In-, or 177Lu-labeled diagnostic or therapeutic PSMA ligand (DOTAGA-(I-y)fk(Sub-KuE), also called PSMA-I&T, for “imaging and therapy”) possesses a unique potential for the management of advanced prostate cancer (12–14). PSMA radioligand therapy (RLT) with PSMA-I&T could achieve high tumor-to-background ratios of mean absorbed doses (13,15).
We analyzed the safety and efficacy of the 177Lu-labeled DOTAGA-based PSMA ligand 177Lu-DOTAGA-(I-y)fk(Sub-KuE) (177Lu-PSMA) in a larger cohort of patients with mCRPC. The endpoints of our analysis, which was performed in correlation with kinetics and dosimetry, were safety, objective response, progression-free survival, and overall survival.
MATERIALS AND METHODS
Patient Characteristics
Fifty-six patients who had progressive mCRPC (median age, 72 y; median Gleason score, 8) and rising prostate-specific antigen (PSA) levels and were referred to our center underwent 125 cycles of 177Lu-PSMA RLT between May 2013 and June 2015 (1 cycle for 16 patients, 2 cycles for 15 patients, 3 cycles for 17 patients, 4 cycles for 6 patients, and 5 cycles for 2 patients). The median administered activity of 177Lu-PSMA per cycle was 5.76 GBq (range, 3.6–8.7 GBq). The patients were clinically monitored with the Karnofsky Performance Status score and the visual analog scale score for pain and for any other clinical symptoms, as documented on patient questionnaires (Tables 1 and 2). The institutional review board approved this study, and all patients signed a written informed consent form.
Patient Characteristics
Localization of Metastases
Selection of Patients and Follow-Up
PSMA expression was an essential prerequisite for 177Lu-PSMA RLT. To avoid the introduction of 2 new radiopharmaceuticals for imaging and therapy in 1 study, we used 68Ga-PSMA instead of the corresponding 68Ga-DOTAGA-(I-y)fk(Sub-KuE) for the selection of patients and therapy monitoring by means of PET/CT. The activity of 177Lu-PSMA administered and the number and interval of cycles were personalized on the basis of uptake in metastases on 68Ga-PSMA PET/CT before therapy, renal function, hematologic status, previous treatments, and Karnofsky Performance Status score. Molecular and morphologic responses were evaluated in accordance with European Organization for Research and Treatment of Cancer (EORTC) criteria (16) and RECIST 1.1 (17), respectively. The serum PSA response was documented monthly. At the time of analysis, follow-up for a median of 15 mo (range, 6–28 mo) after 2 or more therapy cycles was available for 25 patients (2 cycles for 9 patients, 3 cycles for 7 patients, and 4 cycles for 9 patients).
Ethical and Regulatory Issues
68Ga- and 177Lu-PSMA were administered in compliance with the German Medicinal Products Act (section 13, subsection 2b), the 1964 Declaration of Helsinki, and the responsible regulatory body (Government of Thuringia). All patients received PSMA RLT under the “compassionate use” clause of the German Medicinal Products Act (18). The decision to perform PSMA RLT was based on the opinion of the referring urologists and oncologists after exhaustion of all other therapeutic options. The study was performed in accordance with the regulations of the German Federal Agency for Radiation Protection.
68Ga-PSMA PET/CT Imaging
PET/CT (Biograph mCT Flow 64; Siemens Medical Solutions AG) was performed 60–80 min after intravenous administration of 68Ga-PSMA (142 ± 18 MBq [mean ± SD]). All patients received 20 mg of furosemide intravenously to accelerate renal tracer excretion. Spiral contrast-enhanced CT imaging was acquired after intravenous administration of 60–100 mL of nonionic iodinated contrast material. Imaging and reconstruction parameters were as follows: 120 kV; 160 mA; gantry rotation time, 0.3 s; slice thickness, 0.4 mm, with increments of 0.1–10 mm; 40 images/s; and 512 × 512 matrix. PET imaging was acquired from the skull through the midthigh in 3-dimensional flow motion. The reconstruction matrix was 400 × 400 (high-resolution processing), achieving an axial resolution of 4.4 mm. SUVmax was obtained by drawing circular regions of interest that were automatically adapted (40% isocontour) to a 3-dimensional volume of interest with commercial software provided by the vendor.
177Lu Radiolabeling
177Lu labeling of the DOTAGA-based PSMA ligand [DOTAGA-(I-y)fk(Sub-KuE)] was performed with previously described methods (12). In brief, the PSMA ligand was incubated with the required radioactivity of 177Lu-Cl3 at 90°C for 30 min in sodium acetate buffer (0.4 M, pH 5.5). To this buffer, 5–10 mg of gentisic acid were added to prevent radiolysis. After sterile filtration and quality control, the radiochemical purity was more than 97% in all cases—mostly greater than 99%.
Hydration and Administration of Therapeutic Activity
Each patient received 1.6 L of 5% lysine HCl and 10% l-arginine HCl (amino acid solution) intravenously over 4 h, starting 30 min before radiopharmaceutical administration (19). The radiopharmaceutical was coadministered over 10–15 min with a dedicated second infusion pump system for radionuclide therapy.
Safety
All patients were clinically monitored during therapy and for 2–4 d thereafter as inpatients for possible side effects (such as nausea, vomiting, breathlessness, and fatigue). Vital parameters were recorded during therapy. A structured questionnaire was used to document any delayed complication (such as xerostomia). Laboratory analysis was performed before and after PSMA RLT (Table 3). Toxicity was recorded in accordance with Common Terminology Criteria for Adverse Events (CTCAE), version 4.03 (20).
Laboratory Parameters Monitored After PSMA RLT
Dosimetry
Dosimetry was performed in 30 patients in accordance with our protocol established from more than 1,000 neuroendocrine neoplasm patients undergoing peptide receptor radionuclide therapy (21). Time-dependent activity in organs and tumors was determined by drawing regions of interest on serial 177Lu-PSMA whole-body scans after therapy. The time–activity curves of source regions were fitted to exponential functions of the first or second order to determine the time-integrated activity. The mean absorbed doses were estimated with OLINDA/EXM software (22).
Blood sampling was performed in 6 patients to estimate the mean absorbed dose to the red marrow. Venous blood samples were obtained at various time points after injection of the radiopharmaceutical. The radioactivity was measured with a high-purity germanium detector (MBq/mL) and was plotted against time. The curves were fitted to bi- or triexponential functions to determine the radioactivity in blood. Cumulative radioactivity in bone marrow was calculated as previously described (23).
Whole-body scintigraphy after therapy was performed with a SPIRIT DH-V dual-head γ-camera (Mediso Medical Imaging Systems), a medium-energy general-purpose collimator, a 15% energy window, a peak at 208 keV, and a scan speed of 15 cm/min. Whole-body scintigraphy was acquired at 5 time points from 0.5 to 118 h after injection. SPECT/CT imaging was obtained between 45 and 118 h after injection.
Statistics
Statistical analysis was performed with OriginPro 8.1G software (OriginLab). After the skewed distribution of all variables was proved with the Kolmogorov–Smirnov test, quantitative data were described in terms of median and range. Nonparametric sign tests were used for determination of the significance of differences between hematologic and renal parameters before and after therapy; P values of less than or equal to 0.05 were considered significant. Survival analysis was performed with Kaplan–Meier curves.
RESULTS
177Lu-PSMA Scintigraphy After Therapy
Excellent uptake of 177Lu-PSMA was noted in metastases and in residual or recurrent prostate cancer (n = 10) on planar and SPECT/CT images after therapy (Figs. 1 and 2). Physiologic uptake was seen in the lacrimal and salivary glands, small intestine, and kidneys, and a relatively lower level of uptake was seen in the liver and spleen. The radiopharmaceutical was predominantly excreted through the kidneys. No uptake was seen in the lungs or brain. Delayed whole-body images (up to 118 h after therapy) revealed long-term retention of 177Lu-PSMA in metastases and relatively rapid clearance from normal organs.
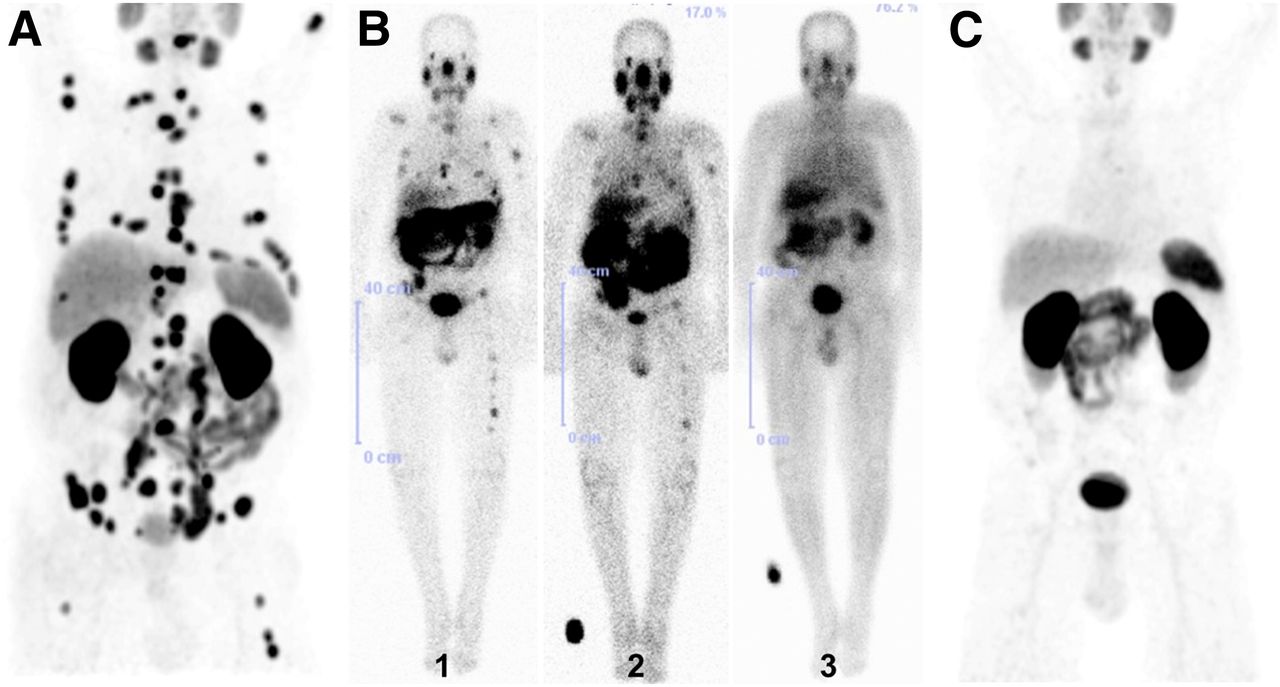
76-y-old patient after external-beam radiation therapy to bone metastases and hormone therapy. (A) 68Ga-PSMA PET/CT revealed progressive bone and lymph node metastases. (B) 177Lu-PSMA scintigraphy demonstrated resolution of metastases after first (1), second (2), and third (3) RLT cycles. (C) 68Ga-PSMA PET/CT showed excellent molecular response (RECIST 1.1 and EORTC criteria), with disappearance of most PSMA-avid metastases, after 3 PSMA RLT cycles.
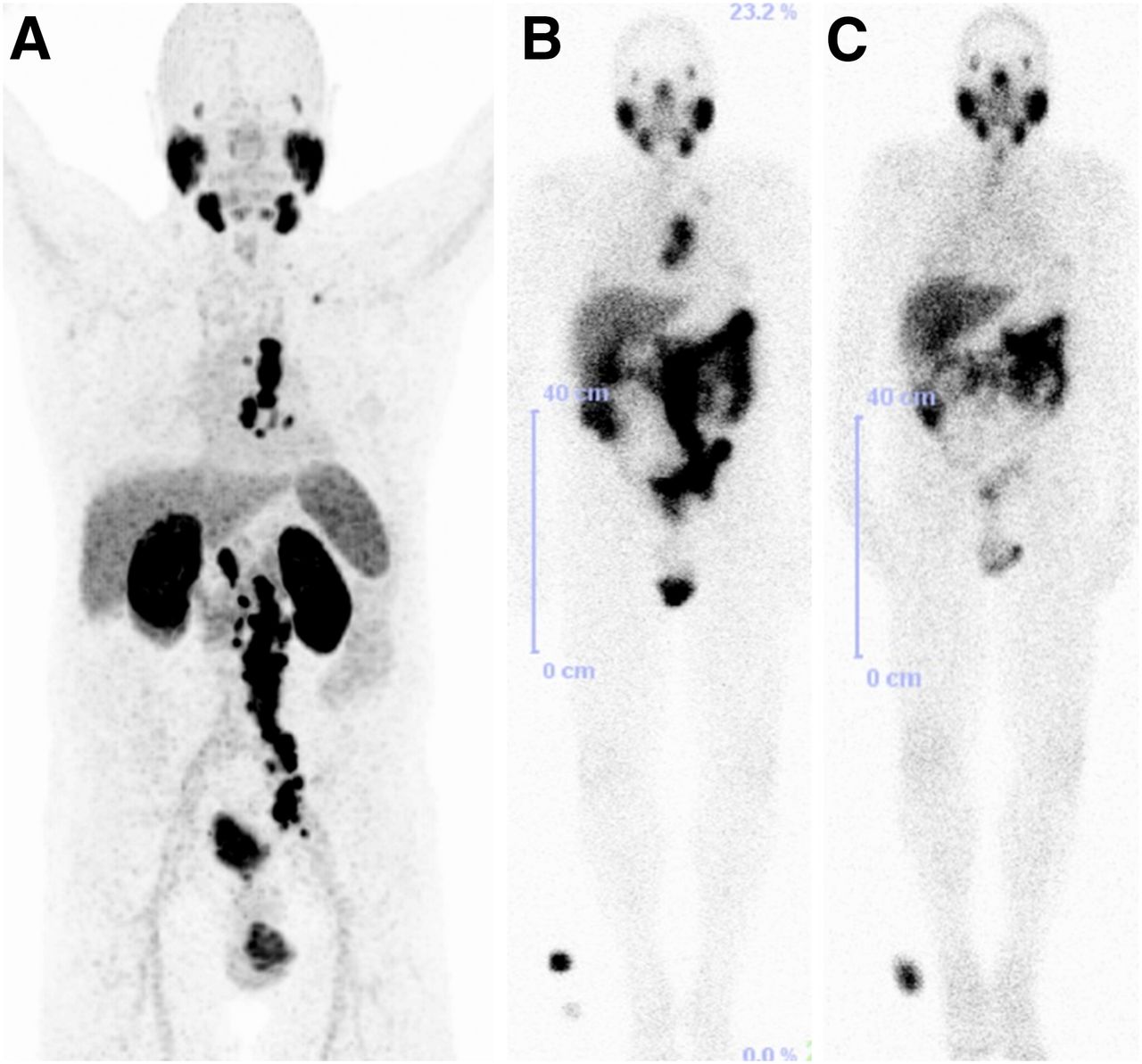
70-y-old patient with PSMA-avid lymph node metastases on 68Ga-PSMA PET/CT before therapy (A) and on 177Lu-PSMA scintigraphy after first PSMA RLT (B), with remarkable reduction in uptake after second PSMA RLT (C). Results were consistent with excellent therapy response.
Dosimetry
Blood sampling revealed fast kinetics of 177Lu-PSMA, especially for the first of the 3 exponential functions. The mean absorbed dose to the red marrow in 6 patients varied from 0.01 to 0.04 mGy/MBq (Table 4). The effective half-life in tumor lesions was higher than those in the whole body, kidneys, and parotid glands, resulting in the delivery of higher mean absorbed doses to tumors (Fig. 3; Table 5). The maximum absorbed dose delivered to a paraaortic lymph node metastasis that exhibited the highest SUVmax (187.5) before therapy was 468 Gy.
Blood Kinetics and Absorbed Dose to Red Marrow in 6 Patients

Kinetics, effective half-lives, and mean absorbed doses (median) in normal organs and tumor lesions. IA = injected activity.
Effective Half-Lives and Mean Absorbed Doses in Whole Body, Kidneys, Parotid Glands, and Tumor Lesions
Safety
177Lu-PSMA therapy was well tolerated by all patients. No clinically significant adverse effects were reported by any patient during hospitalization for therapy or follow-up for 28 mo. Two patients reported mild xerostomia after receiving 3 and 4 cycles, with spontaneous resolution within 3 mo.
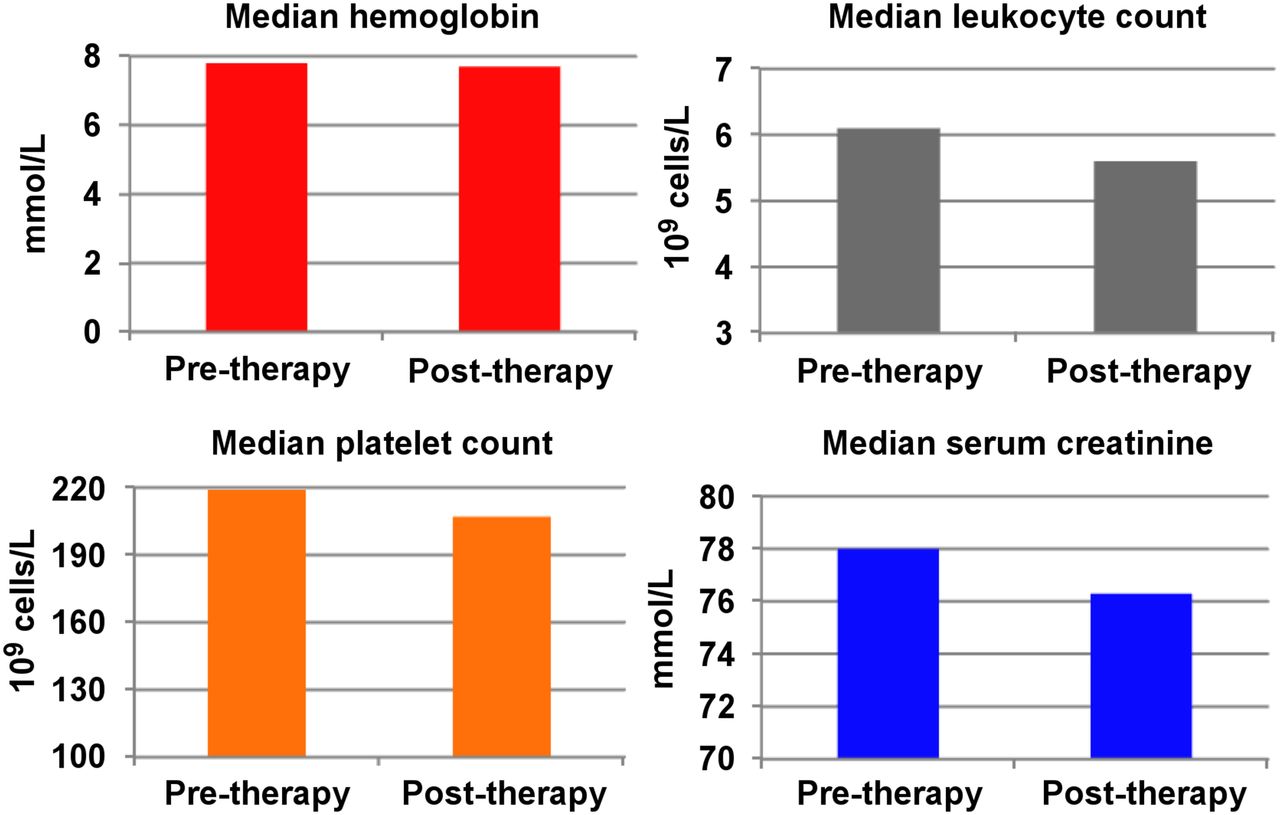
No significant change in hemoglobin (median ± SD; before therapy: 7.8 ± 1.1 mmol/L; after therapy: 7.7 ± 1.2 mmol/L; P > 0.05) was observed after therapy (Fig. 4). Three anemic patients required packed red cell transfusions before PSMA RLT. There were statistically significant decreases in erythrocyte counts (before therapy: 4.3 ± 0.6; after therapy: 4.0 ± 0.5; P < 0.05) and leukocyte counts (from 6.1 ± 1.4 to 5.6 ± 1.6; P < 0.05), although the absolute differences were minimal and clinically insignificant. Platelets remained within the reference range (before therapy: 219 ± 51; after therapy: 207 ± 49; P > 0.05). Grade 1 or 2 leukocytopenia occurred in 9 patients who had received long-term chemotherapy. Remarkably, patients with low blood cell counts before therapy did not exhibit a decrease in blood cell counts after 177Lu-PSMA therapy (Table 6).
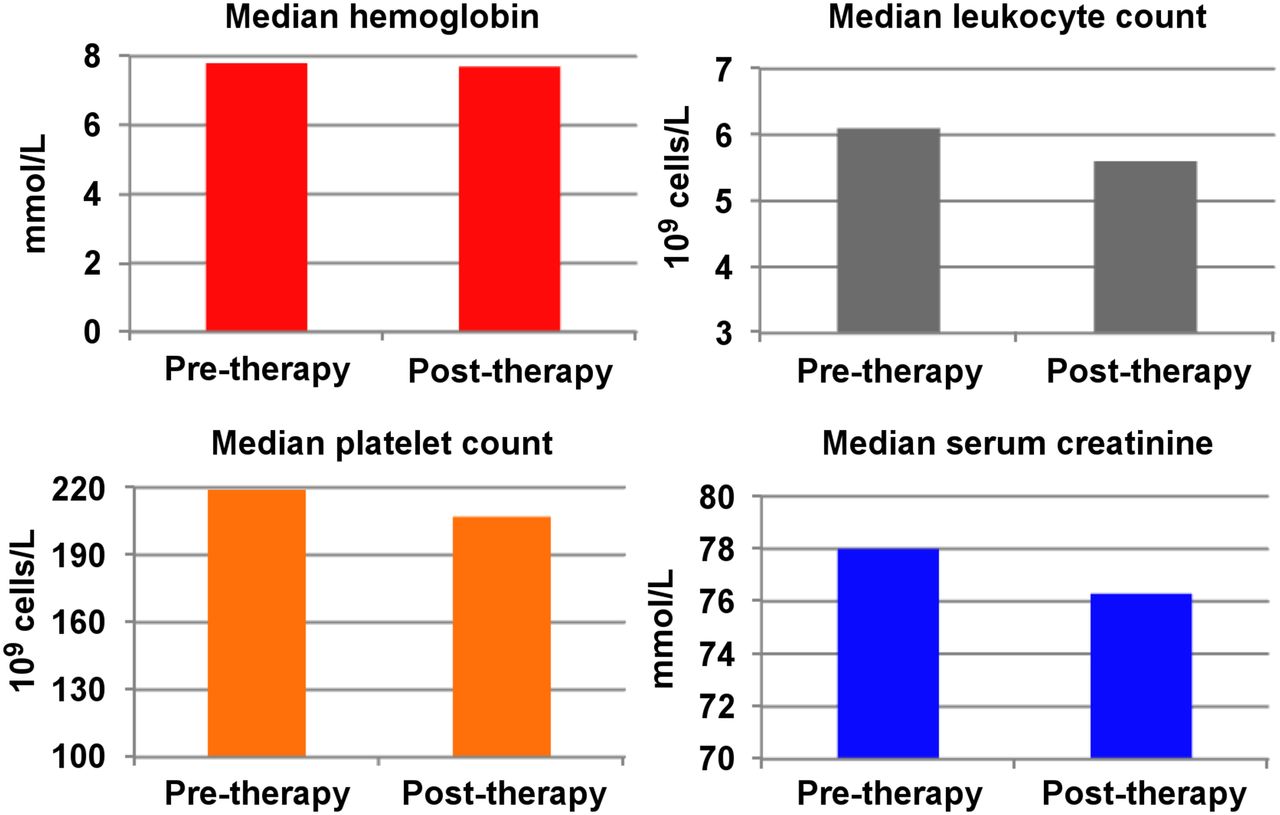
Comparison of median laboratory parameters before and after PSMA RLT, revealing no significant hematotoxicity or nephrotoxicity.
No Evidence of Hematotoxicity After PSMA RLT*
There was no evidence of nephrotoxicity (Fig. 4). One patient with previous grade 1 renal insufficiency did not experience worsening of renal function. There was no statistically significant change in serum creatinine levels (before therapy: 81.9 ± 22.4 mmol/L; after therapy: 80.9 ± 23.7 mmol/L; P > 0.05).
Efficacy of 177Lu-PSMA RLT
Improvement in Clinical Symptoms
Pain significantly decreased in severity in 2 of 6 patients (33.3%), with a reduction in visual analog scale scores from 8 and 6 before PSMA RLT to 4 and 3 after PSMA RLT, respectively. The pain intensity remained unchanged in 4 patients, requiring constant use of analgesics. The Karnofsky Performance Status score improved in several patients, and no worsening was observed in any patient after therapy.
PSA Response
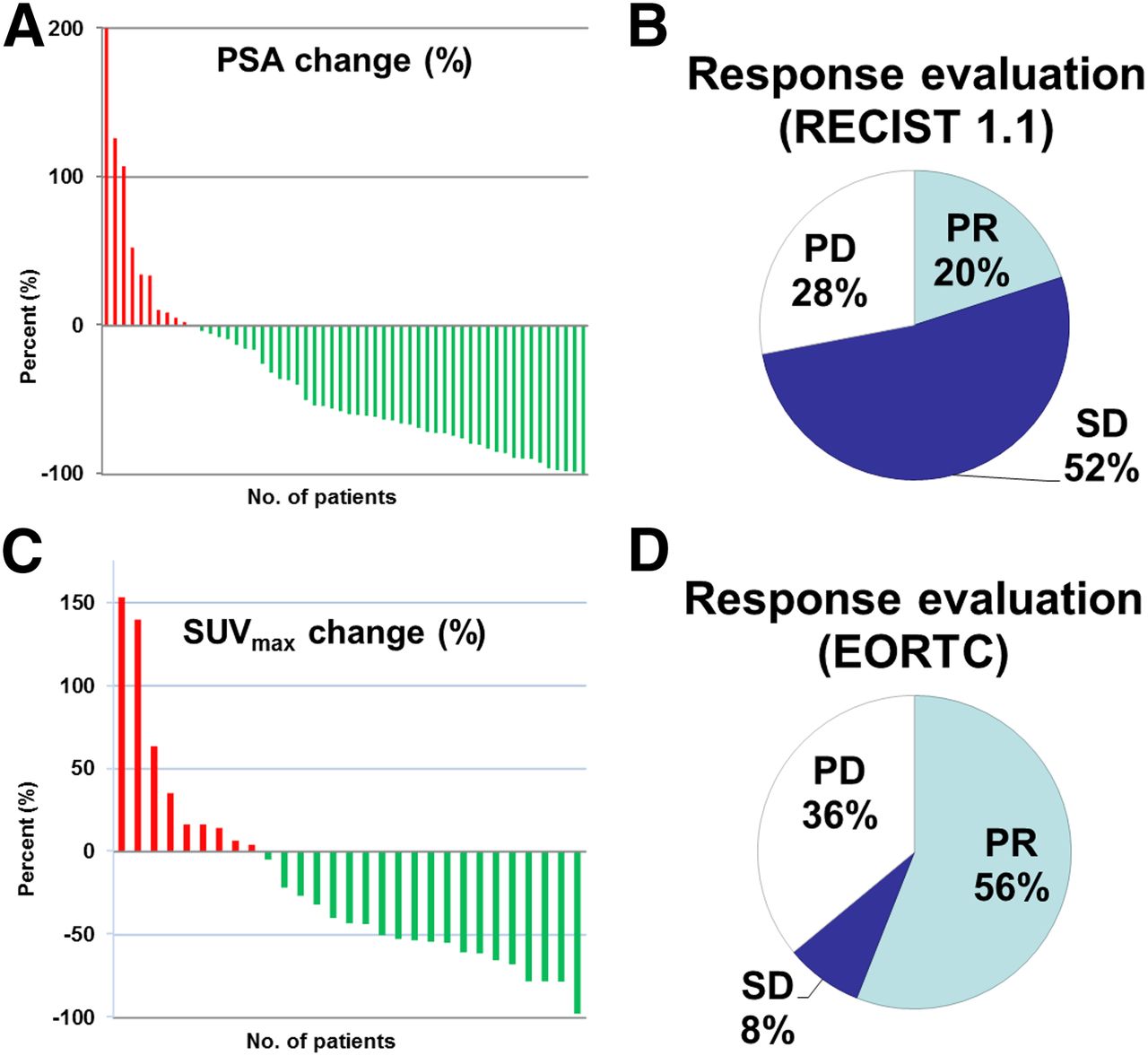
Of 56 patients, 45 (80.4%) demonstrated a reduction in PSA levels (Fig. 5). The median PSA level at the first presentation was 43.2 ng/mL (range, 0.05–2,848 ng/mL), and the level decreased to 23.8 ng/mL (range, 0.01–2,227 ng/mL) after therapy. A decline in the PSA level by greater than 80% was seen in 13 patients (23.2%), a decline by greater than 50% was seen in 33 patients (58.9%), and a decline by greater than 30% was seen in 37 patients (66.1%). The best PSA response was a decline from 29.12 to 0.23 ng/mL (99.2%) after therapy. A PSA increase of greater than 25% was noted in 6 patients (10.7%) with progressive disease (24).

PSA, SUVmax, and response assessment. (A and C) Percentage changes in baseline serum PSA levels (A) and in baseline SUVmax during follow-up period. (B and D) Response assessment in 25 patients after at least 2 PSMA RLT cycles with RECIST 1.1 (B) and EORTC criteria (D). PD=progressive disease; PR=partial remission; SD=stable disease.
Objective Response
Analysis was performed in 25 patients monitored for at least 6 mo after 2 or more 177Lu-PSMA RLT cycles (Fig. 5).
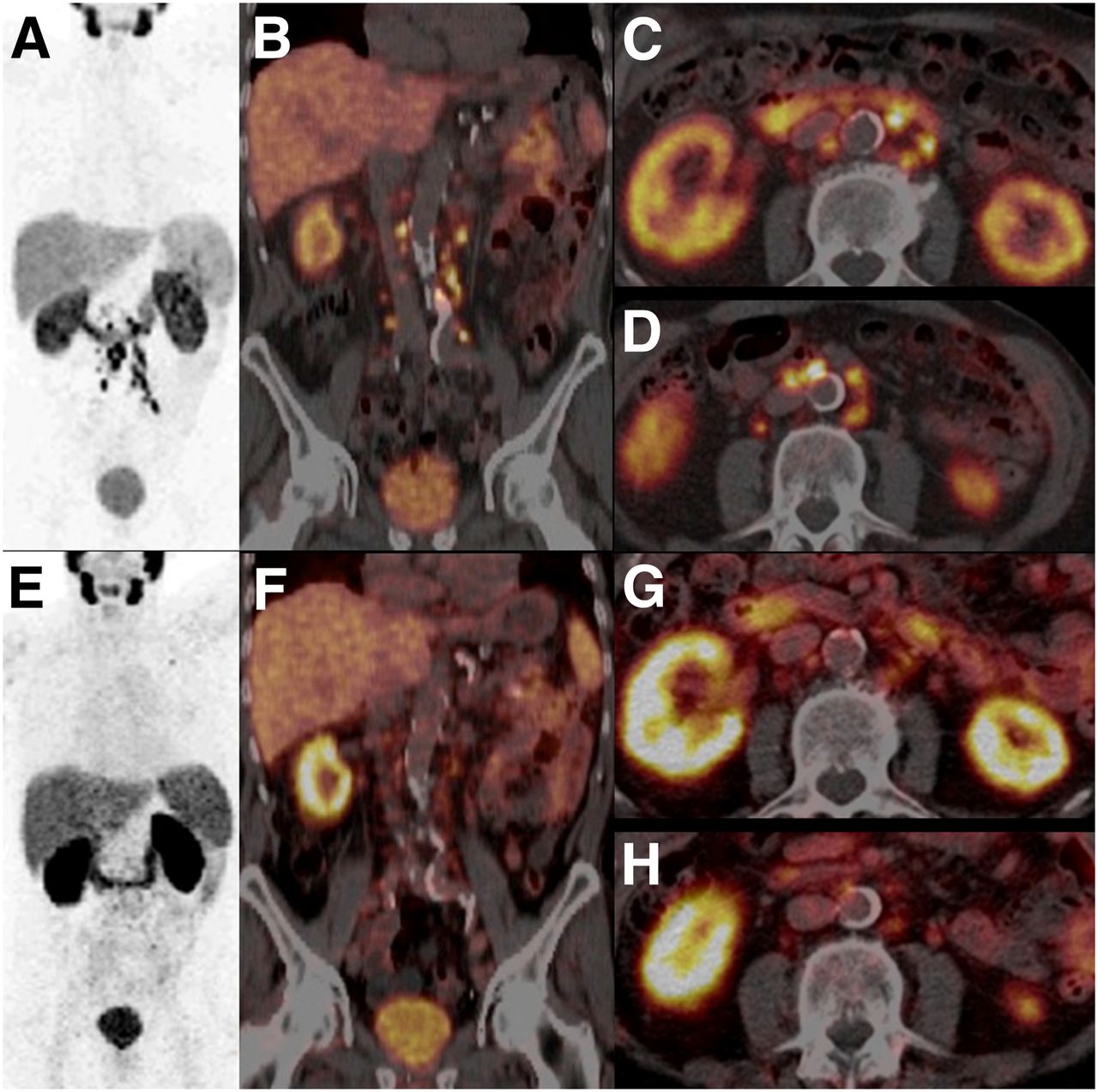
A morphologic response assessment (RECIST 1.1) by contrast-enhanced CT documented partial remission in 5 patients (20%), stable disease in 13 patients (52%), and progressive disease in 7 patients (28%). Of the patients exhibiting an objective response, 4 had lymph node metastases only, and 1 had multiple lymph node and bone metastases, with only the target lymph node lesion demonstrating a significant decrease in size (Figs. 1 and 6).

76-y-old patient after prostatectomy, external-beam radiation therapy to bone metastases, hormone therapy, and chemotherapy. (A–D) Patient had multiple PSMA-avid lymph node metastases, as revealed by 68Ga-PSMA PET/CT. (E–H) Excellent response to therapy (according to both RECIST 1.1 and EORTC criteria) after 2 cycles of 177Lu-PSMA RLT was demonstrated by 68Ga-PSMA PET/CT, with greater than 50% decrease in serum PSA level (from 15 to 6 ng/mL).
On 68Ga-PSMA PET/CT (EORTC criteria), the median SUVmax of the target lesion before PSMA RLT was 37.5 (range, 15–187.5), and that after PSMA RLT was 15.7 (range, 1.7–75.3). A molecular response evaluation revealed partial remission in 14 patients (56%), stable disease in 2 patients (8%), and progressive disease in 9 patients (36%). Objective responses were also observed in 9 patients with either only or predominantly bone metastases. There was a 90% reduction in the SUVmax (from 187.5 to 15.9) in the paraaortic lymph node metastasis receiving an absorbed dose of 468 Gy.
Survival
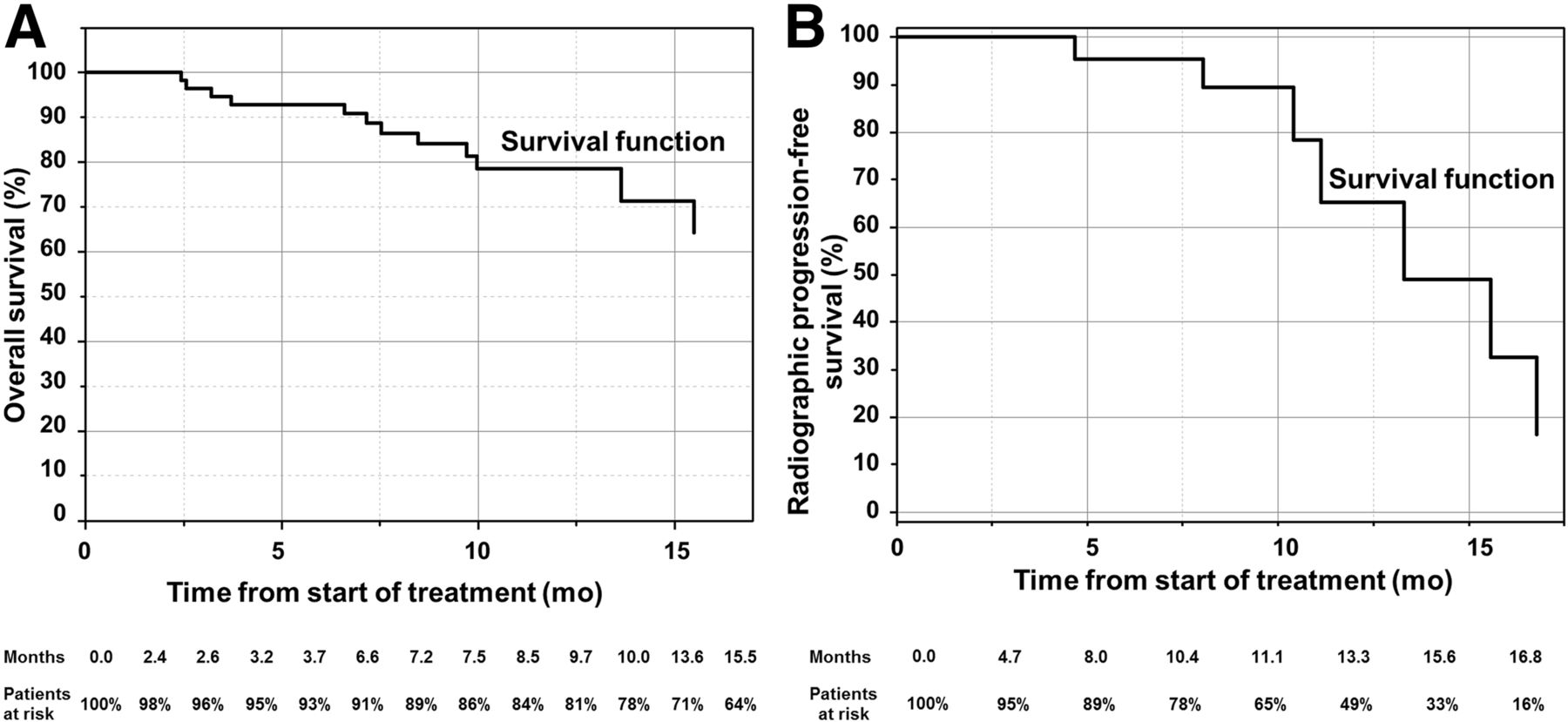
During a follow-up period of 28 mo, 12 patients died (21.4%). The median overall survival (last assessed 15.5 mo after PSMA RLT) was not reached (Fig. 7A). Survival after 28 mo was 78.6%. The median progression-free survival was 13.7 mo (Fig. 7B).

Survival function. (A) Overall survival (months). (B) Progression-free survival (months), according to RECIST 1.1.
DISCUSSION
177Lu PSMA RLT involves selective tumor targeting with the objectives of maximizing tumor dose and sparing normal tissue. 177Lu-PSMA showed high, specific, and rapid uptake in prostate cancer metastases. The long effective half-lives in both skeletal and soft-tissue metastases, approaching the physical half-life of 177Lu, resulted in high mean absorbed tumor doses; the maximum doses obtained in bone and lymph node metastases were 260 and 468 Gy, respectively. Our patient group was heterogeneous, with wide variations in the SUVmax before PSMA RLT, in tumor load, and in the distribution of metastases (Table 2). The excellent tumor response was attributable to the high doses delivered to metastases, as indicated by specific 177Lu-PSMA tumor uptake (25,26).
PSMA RLT has a distinct advantage over radioimmunotherapy with 177Lu-labeled PSMA antibodies. The mean absorbed doses of 177Lu-PSMA delivered to the whole body, red marrow, and kidneys (0.02, 0.014, and 0.8 mGy/MBq, respectively) were found to be significantly lower than those of 177Lu-DOTA-J591 (0.19, 0.32, and 1.40, respectively) (10). The larger size of the antibody results in slower clearance from the circulation, thereby resulting in the delivery of much higher doses to normal organs. The mean absorbed dose of 177Lu-DOTA-J591 delivered to the red marrow was 20-fold higher than that of 177Lu-PSMA in the present study (10).
The theranostic approach encompasses the use of molecular targeting vectors (e.g., peptides and ligands), which can be labeled with distinct radionuclides for diagnosis and therapy (27). In the present study, the essential selection criterion was the confirmation of PSMA expression in the metastases on 68Ga-PSMA PET/CT. The theranostic approach also aids in the early and accurate assessment of the response to therapy (28). The disease burden can be accurately quantified by the SUV with 68Ga-PSMA PET/CT, making follow-up in mCRPC patients undergoing PSMA RLT easy.
In the present study, an objective response evaluation after radiolabeled PSMA small-molecule therapy was systematically performed for the first time (to our knowledge). A significant reduction in the size of the target lesion was noted in 5 patients with lymph node metastases. The discrepancy in the evaluation of remission in 9 patients classified as responders by PET/CT could be explained by the lower sensitivity of stand-alone CT in the assessment of skeletal lesions.
On the basis of the SUVs of the target lesions before and after therapy, the disease progressed after 2 cycles in 9 patients who had extensive lymph node and osseous metastases. The discordance in 2 patients with extensive disease—that is, progressive disease on 68Ga-PSMA PET/CT and stable disease on CT—could be explained by the higher sensitivity of PET/CT (particularly for small lymph node lesions) and by the fact that a molecular response (as defined by a change in the SUV) occurs earlier than a change in size (28,29).
There was a decrease in serum PSA levels in 45 of 56 patients (80.4%) and a decrease by greater than 50% in 33 patients (58.9%), similar to the results reported earlier (11). The major route of excretion of 177Lu-PSMA is through the kidneys, similar to that of 177Lu-DOTATATE (19). The high level of renal uptake may have been due to PSMA expression in renal tissue, which was better visualized on 177Lu-PSMA images early after therapy (30). Blocking of specific PSMA binding in kidney tissues by the PSMA inhibitor 2-(phosphonomethyl)pentanedioic acid has been validated in preclinical studies; however, there is a lack of availability of this compound for clinical use, and its use may concurrently block uptake within tumors (31). The patients were hydrated with a combination of positively charged amino acids, as for peptide receptor radionuclide therapy with somatostatin analogs. There was no evidence of nephrotoxicity after PSMA RLT. However, the role of nephroprotection needs to be further investigated. The rapid washout of 177Lu-PSMA resulted in a relatively low mean absorbed dose despite the high initial level of renal uptake. Dosimetry ensured that the maximum mean absorbed renal dose of 23 Gy, extrapolated from external-beam radiotherapy, was not exceeded (32).
A higher incidence of hematotoxicity (40%) was reported in a smaller study of 10 patients treated with 177Lu-DKFZ-617; 1 patient had grade 3 or 4 hematologic toxicity (33). This finding could be explained by more compromised bone marrow in those patients before PSMA RLT. Grade 1–3 hematologic toxicity was reported with 131I-labeled PSMA ligands (11). There was a mild but statistically significant decrease in mean leukocyte counts in our patient cohort. However, 17 patients had preexisting grade 1 or 2 anemia and leukocytopenia before PSMA RLT, without worsening of blood counts after therapy (Table 6). Leukocytopenia of grade 1 or 2 was present in 9 of 25 patients (36%) who had received chemotherapy before PSMA RLT. No thrombocytopenia occurred. There was no grade 3 or 4 hematologic toxicity in any of the patients in the present study, despite the high administered radioactivity (up to 8.7 GBq).
The uptake in salivary glands and in the proximal small intestine could be explained by PSMA expression (30). The mean absorbed dose to the parotid glands was found to be greater than that to the kidneys. This finding was also noted in a recent preclinical dosimetry study of 177Lu-DKFZ-617 (34). None of the patients in the present study experienced significant xerostomia. Intense accumulation of 131I-MIP-1095 in the salivary glands reportedly led to xerostomia in 7 patients and mucositis in 1 patient (11). The high dose delivered to the salivary glands by 131I-MIP-1095 was probably due to prolonged retention. Because 177Lu-PSMA—unlike 131I-MIP-1095—did not give rise to salivary gland toxicity, the fates of the labels in the salivary glands over time are assumed to be different and should be investigated. No short- or long-term side effects from the therapy (such as nausea, vomiting, and diarrhea) were observed in any patient despite the accumulation of the radiopharmaceutical in the small bowel and the significant elimination of activity by the intestine.
The morphologic response was better appreciated in lymph node metastases than in bone lesions, primarily because of the better delineation of lymph nodes on CT. A significant advantage of 177Lu-PSMA over bone-targeting radiopharmaceuticals—notably, 223Ra-chloride—is the utility in patients with mCRPC and not only osseous but also soft-tissue metastases. Twelve of the patients in the present study had lymph node metastases only, and 8 of them responded to PSMA RLT—not only according to molecular, morphologic, and biochemical (reduction in PSA level) criteria but also clinically, as noted by a significant decrease in inguinal pain in 1 patient. Further clinical trials comparing 177Lu-PSMA and 223Ra-chloride with regard to objective response, pain management, and adverse effects on bone marrow in patients with skeletal metastases are needed.
Objective responses to 177Lu-PSMA were noted even in patients who had relapsed despite maximum hormonal therapy. There is no evidence suggesting that hormonal agents affect PSMA expression in metastases. Therefore, we postulate that these drugs should not be stopped during or after PSMA RLT.
Our single-center prospective clinical study had some limitations. There were no strict pretest criteria for the selection of patients, and the patients were a heterogeneous group. However, PSMA RLT was a rational therapeutic option, given that it was applied as a systematic individualized theranostic approach comprising 68Ga-PSMA PET/CT for the selection of patients, 177Lu-PSMA–based therapy, and 68Ga-PSMA PET/CT–based response evaluation. The decision to treat was made by the referring oncologists and urologists after the exhaustion of all standard therapeutic options. The median progression-free survival (13.7 mo) obtained in the present study is at least comparable to that observed with newer therapies for mCRPC (2–5). Progression-free survival was retained in many patients despite the fact that they received currently available therapy options, including chemotherapy, which potentially limited the amount of radioactivity that could be applied for PSMA RLT.
CONCLUSION
177Lu-PSMA radioligand therapy for end-stage progressive mCRPC is safe and effective. The avidity of the tumor target that defined the achievable tumor dose was demonstrated before therapy with 68Ga-PSMA PET/CT and a theranostic approach. PET/CT was applied to monitor the tumor response and to guide decisions about further personalized treatment. This novel therapy achieved objective responses with minimal toxicity in patients whose prostate cancer had progressed despite all standard treatments.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Hans-Jürgen Wester is a shareholder of Scintomics, Fürstenfeldbruck, Germany. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Karin Niepsch, database manager, and colleagues Dr. Manal Sayeg and Dr. Mostafa Shahinfar, the nursing staff, and the nuclear medicine technologists of isotope therapy ward D3 for patient management. We thank J. Harvey Turner for critically reading the manuscript.
Footnotes
↵* Contributed equally to this work.
Published online Jan. 21, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication October 17, 2015.
- Accepted for publication December 15, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Mathematic Modeling of Tumor Growth During [177Lu]Lu-PSMA Therapy: Insights into Treatment Optimization
- Preclinical Evaluation of 177Lu-OncoFAP-23, a Multivalent FAP-Targeted Radiopharmaceutical Therapeutic for Solid Tumors
- Dosimetry of [177Lu]Lu-PSMA-Targeted Radiopharmaceutical Therapies in Patients with Prostate Cancer: A Comparative Systematic Review and Metaanalysis
- PSMAx-Guided PROTAC Degraders for Tumor-Specific Protein Degradation in Prostate Cancer
- Unraveling the Impact of 177Lu-PSMA Radioligand Therapy on Renal Impairment: Distinguishing Causation from Correlation
- Prediction of Response to 177Lu-PSMA Therapy Based on Tumor-to-Kidney Ratio on Pretherapeutic PSMA PET/CT and Posttherapeutic Tumor-Dose Evaluation in mCRPC
- Toward Single-Time-Point Image-Based Dosimetry of 177Lu-PSMA-617 Therapy
- Prostate-Specific Membrane Antigen Radioligand Therapy Using 177Lu-PSMA I&T and 177Lu-PSMA-617 in Patients with Metastatic Castration-Resistant Prostate Cancer: Comparison of Safety, Biodistribution, and Dosimetry
- Pretherapeutic Comparative Dosimetry of 177Lu-rhPSMA-7.3 and 177Lu-PSMA I&T in Patients with Metastatic Castration-Resistant Prostate Cancer
- The Impact of Monosodium Glutamate on 68Ga-PSMA-11 Biodistribution in Men with Prostate Cancer: A Prospective Randomized, Controlled Imaging Study
- Comparative Preclinical Biodistribution, Dosimetry, and Endoradiotherapy in Metastatic Castration-Resistant Prostate Cancer Using 19F/177Lu-rhPSMA-7.3 and 177Lu-PSMA I&T
- Feasibility of Single-Time-Point Dosimetry for Radiopharmaceutical Therapies
- First Clinical Results for PSMA-Targeted {alpha}-Therapy Using 225Ac-PSMA-I&T in Advanced-mCRPC Patients
- Cytoplasmic Localization of Prostate-Specific Membrane Antigen Inhibitors May Confer Advantages for Targeted Cancer Therapies
- 177Lu-EB-PSMA Radioligand Therapy with Escalating Doses in Patients with Metastatic Castration-Resistant Prostate Cancer
- JHU-2545 Selectively Shields Salivary Glands and Kidneys during PSMA-Targeted Radiotherapy
- Long-Term Follow-up and Outcomes of Retreatment in an Expanded 50-Patient Single-Center Phase II Prospective Trial of 177Lu-PSMA-617 Theranostics in Metastatic Castration-Resistant Prostate Cancer
- Theranostics: Leveraging Molecular Imaging and Therapy to Impact Patient Management and Secure the Future of Nuclear Medicine
- 177Lu-PSMA-617 Radioligand Therapy in Metastatic Castration-Resistant Prostate Cancer Patients with a Single Functioning Kidney
- Is the Vision of Radioligand Therapy for Prostate Cancer Becoming a Reality? An Overview of the Phase III VISION Trial and Its Importance for the Future of Theranostics
- Effect of External Cooling on 177Lu-PSMA Uptake by the Parotid Glands
- Clinical Outcomes of 177Lu-PSMA Radioligand Therapy in Earlier and Later Phases of Metastatic Castration-Resistant Prostate Cancer Grouped by Previous Taxane Chemotherapy
- Albumin-Binding PSMA Ligands: Implications for Expanding the Therapeutic Window
- A Single Dose of 225Ac-RPS-074 Induces a Complete Tumor Response in an LNCaP Xenograft Model
- Preserving Preclinical PET Quality During Intratherapeutic Imaging in Radionuclide Therapy with Rose Metal Shielding Reducing Photon Flux
- Dosimetry of 177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer: Correlations Between Pretherapeutic Imaging and Whole-Body Tumor Dosimetry with Treatment Outcomes
- Detection Threshold and Reproducibility of 68Ga-PSMA11 PET/CT in a Mouse Model of Prostate Cancer
- Salivary Gland Toxicity of PSMA Radioligand Therapy: Relevance and Preventive Strategies
- A Perspective on the Evolving Story of PSMA Biology, PSMA-Based Imaging, and Endoradiotherapeutic Strategies
- The Effect of Total Tumor Volume on the Biologically Effective Dose to Tumor and Kidneys for 177Lu-Labeled PSMA Peptides
- Imaging of Nonprostate Cancers Using PSMA-Targeted Radiotracers: Rationale, Current State of the Field, and a Call to Arms
- Targeted {alpha}-Therapy of Metastatic Castration-Resistant Prostate Cancer with 225Ac-PSMA-617: Swimmer-Plot Analysis Suggests Efficacy Regarding Duration of Tumor Control
- Why Targeting PSMA Is a Game Changer in the Management of Prostate Cancer
- PSMA Ligands for PET Imaging of Prostate Cancer
- Dual-Target Binding Ligands with Modulated Pharmacokinetics for Endoradiotherapy of Prostate Cancer
- Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy
- 177Lu-PSMA Radioligand Therapy for Prostate Cancer
- Acceleration of PSMA-Targeted Theranostics to the Clinic: Can Common Sense Prevail?
- 68Ga-PSMA-11 PET as a Gatekeeper for the Treatment of Metastatic Prostate Cancer with 223Ra: Proof of Concept
- Predictors of Response to Radioligand Therapy of Metastatic Castrate-Resistant Prostate Cancer with 177Lu-PSMA-617
- 68Ga-PSMA-11 PET Imaging of Response to Androgen Receptor Inhibition: First Human Experience
- From NETTER to PETTER: PSMA-Targeted Radioligand Therapy
- Targeted {alpha}-Based Treatment of Metastatic Castration-Resistant Prostate Cancer: Revolutionizing Systemic Radiotherapy?
- Nuclear Medicine in Cancer Theranostics: Beyond the Target
- PSMA-Based Radioligand Therapy for Metastatic Castration-Resistant Prostate Cancer: The Bad Berka Experience Since 2013
- Prostate-Specific Membrane Antigen-Targeted Radiohalogenated PET and Therapeutic Agents for Prostate Cancer
- The Rise of PSMA Ligands for Diagnosis and Therapy of Prostate Cancer
- Perspective on 177Lu-PSMA Therapy for Metastatic Castration-Resistant Prostate Cancer