


Abstract
177Lu-prostate-specific membrane antigen (PSMA) radioligand therapy (RLT) using inhibitors of PSMA is a novel therapeutic option in patients with metastatic castration-resistant prostate cancer. The current literature suggests that this therapy is well tolerated and effective. On the basis of clinical need and current evidence, the therapy is being implemented in a growing number of centers worldwide. Here, we review important aspects of 177Lu-PSMA RLT, including patient stratification, the therapy protocol, concomitant medication, and follow-up, to inform medical staff involved in the RLT and care of patients with metastatic castration-resistant prostate cancer.
Metastatic spread and disease progression under androgen deprivation therapy define the onset of metastatic castration-resistant prostate cancer (mCRPC), the lethal form of the disease. Despite recent advances in the treatment of mCRPC, the disease eventually progresses and patients are expected to survive less than 20 mo (1). The development of 177Lu-labeled small ligands for prostate cancer was triggered by the great need for effective mCRPC therapy and by the success of RLT in patients with metastatic neuroendocrine tumors (2).
After previous promising results with 131I-labeled prostate-specific membrane antigen (PSMA) ligands, 177Lu-PSMA RLT was introduced by the German Cancer Research Center at the University Hospital Heidelberg in 2015 (3). 177Lu-PSMA RLT targets PSMA, which is expressed at high levels on the surface of prostate cancer cells (4). PSMA expression remains high in metastases even after multiple lines of therapy (5,6), enabling systemic RLT by repeated intravenous applications of the radioligand (7).
Because there is an urgent clinical need in mCRPC patients, and the first data found RLT to be safe and effective in reducing tumor burden, clinical use of 177Lu-PSMA RLT has been widely adopted in German and international sites, with likely more than a thousand therapy cycles performed (7–18). Given this fast implementation, vast retrospective evidence of dosimetry, safety, and efficacy has been reported, guiding current clinical protocols. Here, we review key findings to summarize the current status of 177Lu-PSMA RLT for mCRPC and to inform the reader on patient selection criteria, the treatment protocol, application, toxicity, and follow-up.
TARGET
PSMA, also termed folate hydrolase I or glutamate carboxypeptidase II, is expressed at high levels on the cells of prostatic adenocarcinoma (19,20). The degree of PSMA expression positively correlates with tumor stage (19,21) and early recurrence (22,23). Normal human tissues, including prostate epithelium, small intestine, renal tubules, and salivary glands, demonstrate considerably lower levels of PSMA expression than prostate cancer (4).
PSMA is a type II transmembrane protein with 2 monomers and corresponding intracellular, transmembrane, and extracellular domains (24). The protein is enzymatically active in its homodimeric form. On ligand binding, PSMA undergoes clathrin-mediated endocytosis (25). Identification of the substrate and binding site stimulated the development of urea-based high-affinity PSMA inhibitors with favorable biodistribution and high tumor-to-background uptake ratios (26–28).
LIGANDS
Currently, 2 PSMA ligands are predominantly reported for clinical 177Lu-based RLT: 177Lu-PSMA-617, first characterized by the Heidelberg group (29), has been implemented in most centers (9–12,14,16–18); 177Lu-PSMA I&T (imaging and therapy) was first reported by Wester’s group (30). Both ligands demonstrate nanomolar affinity for PSMA, with strong and prolonged accumulation in lesions of prostate cancer. Biodistribution, characterized by high uptake in the kidneys, lacrimal glands, salivary glands, and proximal small bowel, is comparable for both ligands (Fig. 1).

Anterior planar scintigrams of 2 patients 18 h after intravenous application of 6.0 GBq of 177Lu-PSMA-617 (A) and 24 h after intravenous application of 7.4 GBq of 177Lu-PSMA I&T (B). Both patients had minimal residual disease after prior RLT, not visible on scintigraphy.
Organs at risk for a critical radiation dose are the kidneys (0.5–0.8 Gy/GBq; conservative dose limit, 23 Gy (31)) and the lacrimal and salivary glands (0.6–1.4 Gy/GBq; dose limit not clearly established (31)) (8,10–12,17,32). The radiation dose to the bone marrow (<0.05 Gy/GBq (8,11,12,17)) and the liver and spleen (each < 0.5 Gy/GBq (12,17,32)) is considerably below critical thresholds.
A review of the literature indicated no clinical advantage of one ligand over the other; however, a head-to-head comparison has not been performed yet. 177Lu-PSMA-617 and 177Lu-PSMA I&T are henceforth summarized as 177Lu-PSMA.
INDICATION
177Lu-PSMA RLT is not approved by the U.S. Food and Drug Administration or the European Medicines Agency, and thus formal criteria for patient inclusion have not been defined. Therapy is currently performed either under a clinical trial (e.g., NCT03042312, NCT03042468, and ACTRN12615000912583) or under local regulations for unproven interventions for patients having exhausted all therapy options. Potential criteria for patient selection outside clinical trials were outlined in a consensus recommendation by nuclear medicine specialists involved in RLT at 12 high-volume centers in Germany (33). The criteria were derived from retrospective evidence (7), expert opinion, and recommendations for 177Lu-DOTATATE/DOTATOC therapy (34).
In summary, 177Lu-PSMA RLT may be considered in patients who have mCRPC progressive after exhaustion of approved therapies; who have confirmed PSMA expression of tumor and metastases, ideally by baseline PSMA-directed imaging (PET or SPECT); who have a sufficient bone marrow reserve as defined by a white blood cell count lower than 3,000/μL and a platelet count lower than 75,000/μL; who have a serum creatinine level lower than 2 times the upper limit of normal; who have liver transaminase levels lower than 5 times the upper limit of normal; and who have discontinued potentially myelosuppressive therapy for more than 6 wk.
Patients should undergo blood tests, including a comprehensive metabolic panel and a complete blood count, within 2 wk before RLT. Renal scintigraphy should be performed before each cycle in patients with a known or suspected renal or urinary disorder. Urinary tract obstruction increases the risk for an excessive radiation dose to the kidneys, as observed in an earlier trial for 111In-pentetreotide (35), and poses a relative contraindication for RLT.
The indication should be confirmed by an interdisciplinary tumor board.
RLT PROTOCOL
Most sites repeat RLT at 8- to 12-wk intervals (8,12,14–18). The experience with 177Lu-DOTATATE indicates that an interval of 8 wk between RLT applications allows for evaluation of a potential blood count nadir after each cycle (2). Between RLT cycles, a complete blood count should be obtained every 2–4 wk to evaluate for potential hematotoxicity (14). A proposed timeline for repeated RLT is shown in Figure 2.

Proposed protocol for repeated 177Lu-PSMA RLT. RLT is performed by repeated application of 177Lu-PSMA at 8-wk intervals, with follow-up assessment at 4-wk intervals. PSMA-directed PET/CT is performed at baseline and after 2 cycles of therapy. (Adapted with permission of (33).)
Maximum tolerable activity has not been evaluated yet. Most sites use a clinically practical standard activity of 6.0 or 7.4 GBq per cycle and have found low rates of serious, mostly hematologic, adverse events (≤10% (7)). The duration of RLT, and therefore the cumulative activity, should be guided by individual response and tolerability. Dosimetry can be used to monitor the cumulative radiation dose to the kidneys and salivary glands. Up to 6 cycles of RLT have been applied without activity-limiting toxicity to the kidneys (36); up to 4 cycles have been applied without salivary-gland toxicity of grade 3 or higher (7). However, long-term clinical follow-up has not been reported yet. Given the average life expectancy in patients with mCRPC, the current dose thresholds derived from external radiation therapy (31) should not preclude an individual need for effective therapy.
177LU-PSMA APPLICATION
Before the start of therapy, intravenous or oral hydration should be initiated if needed, according to the individual’s cardiovascular condition. RLT is started by intravenous application of 177Lu-PSMA, either as a slow injection by hand or via an infusion pump. Use of medication during application should be considered (33): diuretics in cases of urinary flow disorders and laxatives in cases of constipation to support rapid clearance of unbound 177Lu-PSMA; icepacks for the salivary glands to potentially reduce blood flow and 177Lu-PSMA uptake during the blood pool phase, until approximately 4 h after the start of RLT (37); prophylactic antiemetic therapy such as ondansetron; and corticosteroids in cases of cerebral, spinal, or other metastases with risk of swelling and mechanical obstruction.
CONCOMITANT THERAPY
In one multicenter study, serious hematologic adverse events occurred in 12% of patients undergoing 177Lu-PSMA RLT (7). Potentially myelosuppressive therapy should therefore be discontinued at least 6 wk before the start of RLT (33). Basic androgen-deprivation therapy is recommended for mCRPC patients (38). Furthermore, preclinical and clinical studies have indicated that inhibition of the androgen receptor pathway may potentially increase PSMA expression (39,40). Thus, in the literature reports, a considerable proportion of the patients undergoing 177Lu-PSMA RLT received concomitant androgen-deprivation therapy, and acceptable safety was documented for this combination (7,8,12,14–17,41). The current evidence indicates that patients may stay on androgen-deprivation therapy during RLT. However, combination therapy, especially with regard to second-line androgen-deprivation therapy or chemotherapy, has not yet been prospectively assessed.
SAFETY
The safety of 177Lu-PSMA RLT has been assessed by multiple groups (7,8,12,14–17,41). The largest evidence comes from a retrospective multicenter trial in which 145 patients with mCRPC received a median of 2 RLT cycles (range, 1–4) at 12 nuclear medicine clinics in Germany (7). Most patients received 3.5–7.5 GBq (median, 6.0 GBq) per cycle. Physicians reported potentially related or unrelated adverse events based on a standard template. In addition, toxicity was determined by baseline and follow-up findings for serum creatinine level, transaminase level, white blood cell count, hemoglobin count, and platelet count for 121 (83%) of the 145 patients. No treatment-related deaths were reported. Grade 3–4 anemia occurred in 15 patients (10%), and grade 3–4 thrombocytopenia occurred in 5 patients (4%).
A low blood count at baseline and diffuse bone marrow involvement pose a risk for serious hematotoxicity (7,9,12). However, in one multicenter study, few patients undergoing RLT demonstrated a blood count decline of more than one grade, and the rate of grade 3–4 events was low for all other categories (0–3 patients; 0%–2%) (7). A low rate of serious adverse events is consistent with smaller trials outside the multicenter initiative (8,15,16). Rates for serious hematologic adverse events after 177Lu-PSMA (3%–10%) were similar to those reported for mCRPC patients treated with placebo (1%–14%) or 223Ra (3%–13%) within the ALSYMPCA trial (42). Retrospective data thus indicate a favorable safety profile for 177Lu-PSMA RLT for doses of up to 7.5 GBq per cycle. Hematotoxicity occurs in only a small number of patients, similar to 177Lu-DOTATATE RLT (2).
EFFICACY
Efficacy after 177Lu-PSMA RLT was assessed by Rahbar et al. (7), who recorded serial prostate-specific antigen (PSA) levels at baseline and follow-up for 99 of 145 patients (68%). Response was determined in these 99 patients as percentage change in serum PSA from baseline to the lowest PSA level measured at follow-up and at least 8 wk after the start of RLT (best PSA response). Over the entire follow-up period, 45% of patients demonstrated a PSA decline of at least 50% and were considered biochemical responders. A PSA decline of any amount occurred in 60% of patients. Most responders had already demonstrated a PSA decline of at least 50% after the first cycle. The presence of visceral metastases or a serum alkaline phosphatase of 220 U/L or higher, indicating more advanced bone involvement, was a predictor of poor outcome.
A decline of any amount after the first cycle was associated with prolonged survival in a recent retrospective study by Ahmadzadehfar et al. (43). In another retrospective study, overall survival was longer in patients undergoing 177Lu-PSMA therapy than in a historic best-supportive-care group (18). However, survival data from prospective studies are not yet available.
68Ga-PSMA PET/CT follow-up was obtained for 47 patients and found a partial response in 45% and stable disease in 28% (7). A reduction in tumor burden was confirmed in 2 single-center studies by applying the RECIST criteria (12,17).
Patient-reported outcome was assessed in 4 retrospective trials (8,15–17): 177Lu-PSMA RLT led to pain relief in 33%–70% of mCRPC patients, an improved quality of life in 60%, and an improved performance status in 74%.
In summary, a biochemical response after repeated RLT is expected in more than half of all patients, and a partial response by imaging in more than a third.
FOLLOW-UP
Clinical examination and blood tests should be performed at 2- to 4-wk intervals for evaluation of toxicity and response (7). A complete blood count, a comprehensive metabolic profile, and serum creatinine or clearance tests should be included in the routine bloodwork. Coagulation screening and dipstick testing may be added, depending on the comorbidity and risk profile.
For response assessment, PSA levels should be obtained after each cycle. Imaging—for example, CT or PSMA-directed PET/CT—should be performed after every 2 cycles (Fig. 3). Response criteria for 177Lu-PSMA RLT have not been established yet. The criteria of the Prostate Cancer Clinical Trials Working Group 3 may serve as a reasonable framework for response assessment (44); however, decisions on repeated RLT should be guided by individual responses also, including clinical symptoms and quality of life (16,17).
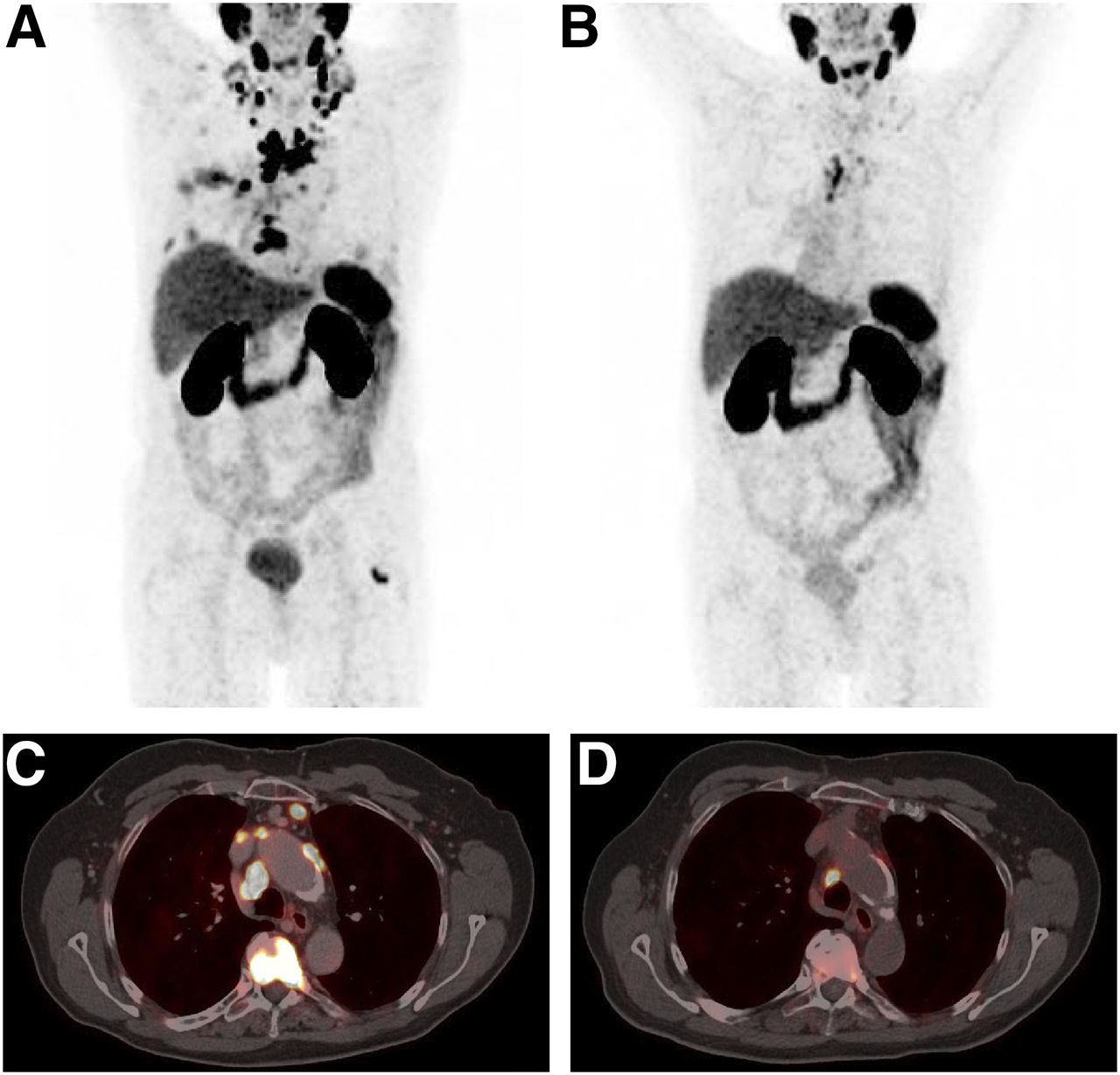
68Ga-PSMA-11 PET/CT at baseline and after 2 cycles of 177Lu-PSMA-617 in 78-y-old patient with mCRPC. Whole-body 68Ga-PSMA-11 PET maximum-intensity projections (A and B) and axial PET/CT scans (C and D) of thorax are shown at baseline (A and C) and after therapy (B and D). 68Ga-PSMA-11 PET demonstrates considerable reduction of PSMA-expressing metastases in lymph nodes and bone after 2 cycles, each with 6.0 GBq of 177Lu-PSMA-617. Serum PSA level decreased from 11.5 to 1.2 ng/mL.
FUTURE PERSPECTIVE
Several prospective trials are under way to establish dosimetry, safety, efficacy, and risk factors for patient stratification (e.g., NCT03042312, NCT03042468, and ACTRN12615000912583). These trials will assess clinical endpoints such as PSA progression-free survival, radiographic progression-free survival, overall survival, pain, and quality of life. For approval and widespread clinical implementation, a NETTER-1–like phase 3 randomized trial will be needed (45).
α-therapy using 225Ac-labeled PSMA-617 has induced promising response rates in patients whose disease progressed under 223Ra or 177Lu-PSMA treatment (46,47). Short-range high-energy α-radiation may yield improved treatment efficacy and reduced hematotoxicity in patients with diffuse bone marrow involvement.
SUMMARY
RLT by repeated intravenous application of 177Lu-PSMA appears safe and effective for reducing PSA and tumor burden in patients with mCRPC. On the basis of promising yet preliminary evidence, RLT is now offered at multiple sites worldwide within clinical trials or under local regulations for new therapies. Several prospective trials are under way to support future implementation of 177Lu-PSMA RLT in the management of mCRPC.
Footnotes
Published online Jun. 29, 2017.
Learning Objectives: On successful completion of this activity, participants should be able to (1) identify potential candidates for 177Lu-prostate-specific membrane antigen (PSMA) radioligand therapy, (2) explain the concept and clinical workflow of PSMA-directed radioligand therapy, and (3) summarize prostate-specific antigen response rates and common adverse events after 177Lu-PSMA radioligand therapy.
Financial Disclosure: University Hospital Muenster has received consulting fees from ABX Advanced Biochemical Compounds for Kambiz Rahbar. Wolfgang Fendler is a consultant/advisor to Ipsen. The authors of this article have indicated no other relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA category 1 credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, SAM, and other credit types, participants can access this activity through the SNMMI website (http://www.snmmilearningcenter.org) through August 2020.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 27, 2017.
- Accepted for publication June 20, 2017.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- SPECT/CT in Early Response Assessment of Patients with Metastatic Castration-Resistant Prostate Cancer Receiving 177Lu-PSMA-617
- [177Lu]Lu-PSMA-617 Therapy in a Patient with Chronic Kidney Disease
- Tumor Control Probability and Small-Scale Monte Carlo Dosimetry: Effects of Heterogenous Intratumoral Activity Distribution in Radiopharmaceutical Therapy
- The Impact of Peptide Amount on Tumor Uptake to Assess PSMA Receptor Saturation on 68Ga-PSMA-11 PET/CT in Patients with Primary Prostate Cancer
- Radionuclide Therapies: An Overview of Applications
- Molecular Imaging of Prostate Cancer Targeting CD46 Using ImmunoPET
- Investigating PSMA-Targeted Radioligand Therapy Efficacy as a Function of Cellular PSMA Levels and Intratumoral PSMA Heterogeneity
- JHU-2545 Selectively Shields Salivary Glands and Kidneys during PSMA-Targeted Radiotherapy
- Effect of External Cooling on 177Lu-PSMA Uptake by the Parotid Glands
- Multimodality Imaging of Prostate Cancer
- A Perspective on the Evolving Story of PSMA Biology, PSMA-Based Imaging, and Endoradiotherapeutic Strategies
- EBONI: A Tool for Automated Quantification of Bone Metastasis Load in PSMA PET/CT
- The Utility of PET/CT in the Planning of External Radiation Therapy for Prostate Cancer
- More {alpha} Than {beta} for Prostate Cancer?