


Abstract
Prostate-specific membrane antigen (PSMA)–targeted radioligand therapy is increasingly used in metastatic castration-resistant prostate cancer. We aimed to estimate the absorbed doses for normal organs and tumor lesions using 177Lu-PSMA I&T (I&T is imaging and therapy) in patients undergoing up to 4 cycles of radioligand therapy. Results were compared with pretherapeutic Glu-NH-CO-NH-Lys-(Ahx)-[68Ga(HBEDCC)] (68Ga-PSMA-HBED-CC) PET. Methods: A total of 34 cycles in 18 patients were analyzed retrospectively. In 15 patients the first, in 9 the second, in 5 the third, and in 5 the fourth cycle was analyzed, respectively. Whole-body scintigraphy was performed at least between 30–120 min, 24 h, and 6–8 d after administration. Regions of interest covering the whole body, organs, and up to 4 tumor lesions were drawn. Organ and tumor masses were derived from pretherapeutic 68Ga-PSMA-HBED-CC PET/CT. Absorbed doses for individual cycles were calculated using OLINDA/EXM. SUVs from pretherapeutic PET were compared with absorbed doses and with change of SUV. Results: The mean whole-body effective dose for all cycles was 0.06 ± 0.03 Sv/GBq. The mean absorbed organ doses were 0.72 ± 0.21 Gy/GBq for the kidneys; 0.12 ± 0.06 Gy/GBq for the liver; and 0.55 ± 0.14 Gy/GBq for the parotid, 0.64 ± 0.40 Gy/GBq for the submandibular, and 3.8 ± 1.4 Gy/GBq for the lacrimal glands. Absorbed organ doses were relatively constant among the 4 different cycles. Tumor lesions received a mean absorbed dose per cycle of 3.2 ± 2.6 Gy/GBq (range, 0.22–12 Gy/GBq). Doses to tumor lesions gradually decreased, with 3.5 ± 2.9 Gy/GBq for the first, 3.3 ± 2.5 Gy/GBq for the second, 2.7 ± 2.3 Gy/GBq for the third, and 2.4 ± 2.2 Gy/GBq for the fourth cycle. SUVs of pretherapeutic PET moderately correlated with absorbed dose (r = 0.44, P < 0.001 for SUVmax; r = 0.43, P < 0.001 for SUVmean) and moderately correlated with the change of SUV (r = 0.478, P < 0.001 for SUVmax, and r = 0.50, P < 0.001 for SUVmean). Conclusion: Organ- and tumor-absorbed doses for 177Lu-PSMA I&T are comparable to recent reports and complement these with information on an excellent correlation between the 4 therapy cycles. With the kidneys representing the critical organ, a cumulative activity of 40 GBq of 177Lu-PSMA I&T appears to be safe and justifiable. The correlation between pretherapeutic SUV and absorbed tumor dose emphasizes the need for PSMA-ligand PET imaging for patient selection.
Prostate cancer (PC) is the second most common cancer in men worldwide (1). About 30% of men experience biochemical recurrence often followed by progression to metastatic castration-resistant PC (mCRPC). Despite several treatment options for these patients, more than 250,000 men are still dying from PC worldwide each year (1). Most recently, prostate-specific membrane antigen (PSMA) is gaining significant interest as a target for imaging as well as radionuclide therapy (2,3). Its expression correlates with the malignancy of the disease, being further increased in mCRPC (4). A variety of PSMA ligands for radioligand therapy (RLT) have been developed in recent years (5). Several studies using 131I- or 177Lu-labeled PSMA ligands for RLT reported reductions in tumor volume and serum prostate-specific antigen (PSA) levels (3,6–10). For the assessment of a new radiopharmaceutical, dosimetry is essential to aim for the optimal therapeutic response with limited side effects. Beside the high and specific uptake of PSMA ligands in PC tissue, different normal organs (e.g., kidney, salivary glands, proximal intestine) exhibit tracer accumulation. Recently published studies using the theranostic DOTA-conjugated PSMA ligand 177Lu-PSMA-DKFZ-617 reported results for both posttherapeutic dosimetry (9,11,12) and pretherapeutic dosimetry (13).
DOTAGA-(I-y)fk(Sub-KuE), termed PSMA I&T for imaging and therapy, is another PSMA ligand (6). It also allows the use of 68Ga- and 177Lu-labeled compounds as theranostic twins. Our initial experiences in antitumor effect and side effects in heavily pretreated patients using this agent have been published recently (10). Similar results on clinical efficacy were reported by Baum et al. with additional data on dosimetry (7). In peptide receptor radionuclide therapy for neuroendocrine tumors, high tumor uptake in pretherapeutic PET and high tumor-absorbed dose are regarded to be predictive of the therapeutic success (14). The SUV may serve as indicator for later-achieved absorbed dose (15–17). Presumably, also in mCRPC the decision for or against RLT may be influenced and eventually potentially based on pretherapeutic PET.
Thus, the purpose of this study was to estimate the absorbed doses for 177Lu-PSMA I&T in normal organs and in tumor lesions in a considerable number of patients with mCRPC undergoing up to 4 cycles with a reference activity of 7.4 GBq. In addition, we aimed to investigate the relationship of pretherapeutic SUV of Glu-NH-CO-NH-Lys-(Ahx)-[68Ga(HBEDCC)] (68Ga-PSMA-HBED-CC) PET and subsequently achieved tumor-absorbed dose and tumor response by PET.
MATERIALS AND METHODS
Patients and 68Ga-PSMA-HEBD-CC PET/CT
Between January 2015 and March 2016, 18 patients (Table 1) with mCRPC and PSMA-avid lesions on pretherapeutic PET underwent 34 cycles of 177Lu-PSMA I&T (n = 15 for first, n = 9 for second, n = 5 for third, n = 5 for fourth cycle) using a reference activity of 7.4 GBq combined with a dedicated protocol for posttherapy dosimetry. The institutional review board of the Technische Universität München approved this study, and all subjects signed a written informed consent form.
Effective Dose for Whole Body in Sv/GBq and Absorbed Doses for Normal Organs in Gy/GBq
177Lu-PSMA I&T RLT and Posttherapy Scintigraphy
The mean applied activity for all cycles was 7.3 ± 0.30 GBq (range, 6.47–7.83 GBq), 7.3 ± 0.32 GBq (range, 6.47–7.78 GBq) for the first cycle, 7.3 ± 0.34 GBq (range, 6.47–7.73 GBq) for the second cycle, 7.5 ± 0.22 GBq (range, 7.30–7.83 GBq) for the third cycle, and 7.3 ± 0.24 GBq (range, 6.95–7.60 GBq) for the fourth cycle. Whole-body scintigraphy was performed at least between 30–120 min, 24 h, and 6–8 d after administration of 177Lu-PSMA I&T. In some cycles (n = 8), patients also underwent whole-body scintigraphy 48 and 72 h after the tracer injection. In detail, 26 cycles were analyzed with 3, 2 cycles with 4, and 6 cycles with 5 posttherapy scintigraphies, respectively. Details on the synthesis, application, and posttherapy scintigraphy of 177Lu-PSMA I&T is given in the supplemental materials (supplemental materials are available at http://jnm.snmjournals.org).
Image Analysis
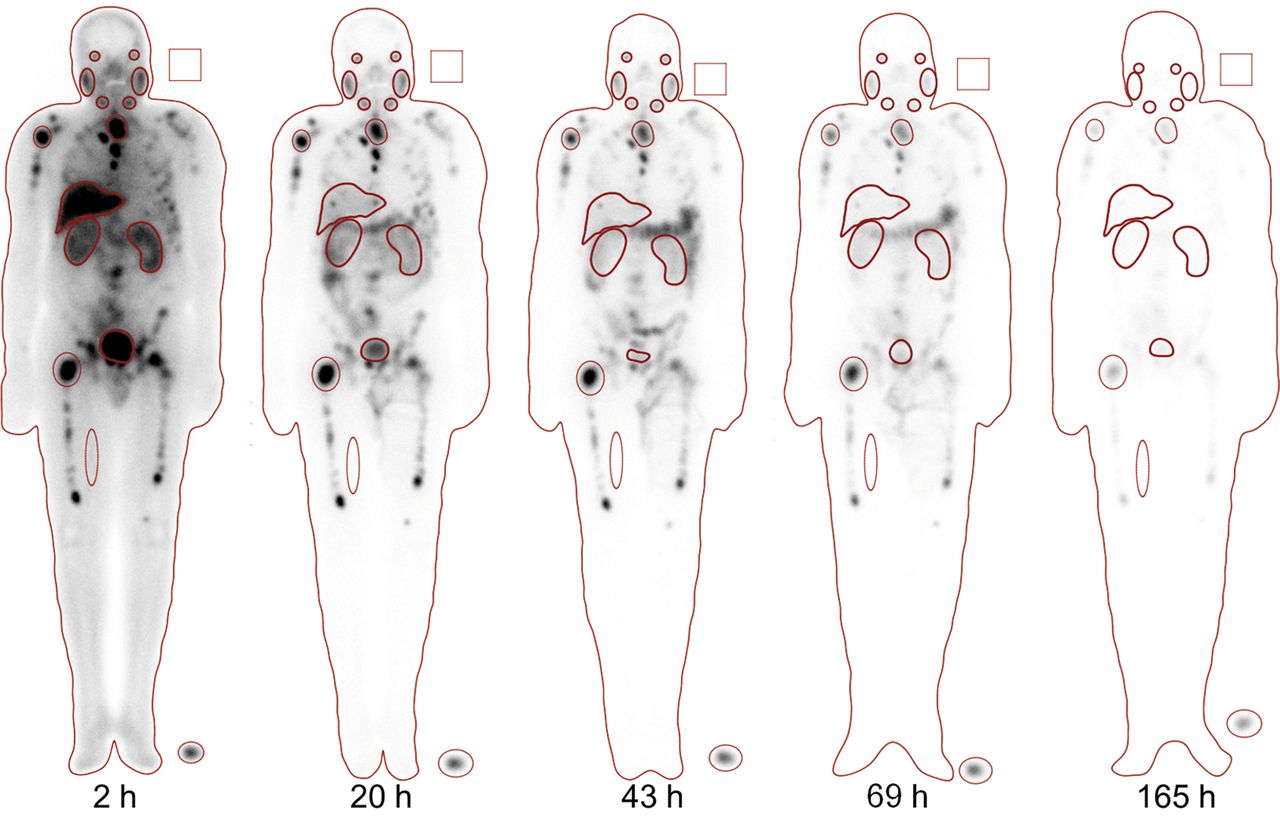
Individual patient absorbed doses for the whole body; kidneys; liver; and parotid, submandibular, and lacrimal glands were estimated based on the MIRD scheme and as recommended in the European Association of Nuclear Medicine Dosimetry Committee Guidelines (18,19). Regions of interest on the whole body; kidneys; liver; parotid, submandibular, and lacrimal glands; and up to 4 tumor lesions were delineated manually on the anterior and posterior whole-body images at 24 h after injection by 2 experienced nuclear medicine physicians and then manually relocated on the previous and subsequent scans (Fig. 1). The volumes of normal organs and tumor lesions were calculated using the CT dataset of the corresponding pretherapeutic 68Ga-PSMA-HBED-CC PET/CT. A total of 93 representative lesions were analyzed (74 bone, 8 lymph node, 8 liver, 3 lung metastases; the assignment to the different cycles is shown in Table 2). Details on the regions of interest for scintigraphy and volume calculation in CT are given in the supplemental materials.

177Lu-PSMA I&T whole-body scintigraphy images obtained at 2, 20, 43, 69, and 165 h after administration. Regions of interest were drawn on liver, kidneys, parotid glands, submandibular glands, lacrimal glands, and lesions in right humerus, thoracic vertebrae, and right femur.
Absorbed Dose for Tumor Lesions in Gy/GBq
Statistical Analysis
All continuous data reported are expressed as mean, SD, and range. Two-sample t tests were used to evaluate differences between individual groups. Correlations between SUVs, change of SUV between pre- and posttherapeutic PET (ΔSUV), and absorbed dose in tumor lesions were assessed using Spearman rank correlation coefficient. A significance level of α = 5% was used. Statistical analyses were conducted using MedCalc (version 13.2.0, 2014; MedCalc).
RESULTS
Qualitative 177Lu-PSMA I&T Distribution on Posttherapeutic Scintigraphy
Physiologic uptake was seen in lacrimal, parotid, and submandibular glands; kidneys; small intestine; and less pronounced in the liver and spleen. Uptake in excess of background was also seen for multiple tumor lesions with progressive accumulation up to 24–48 h after injection (Fig. 1). Delayed whole-body images (up to 6–8 d after therapy) exhibited long-term retention of 177Lu-PSMA I&T in the metastases, with nearly no residual uptake in normal organs.
Dosimetry for Normal Organs
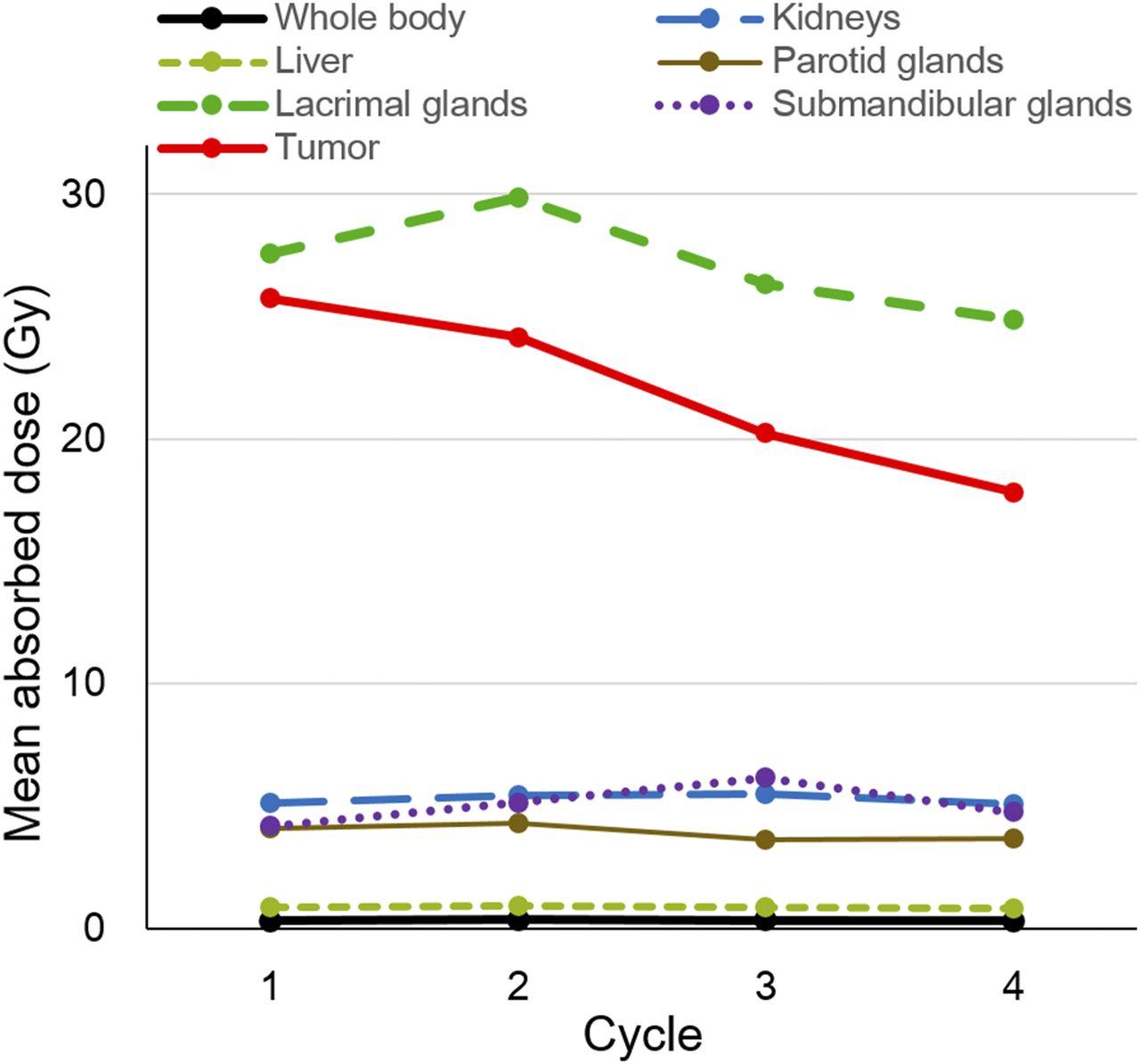
The mean whole-body effective dose for all cycles was 0.41 ± 0.18 Sv (0.06 Sv/GBq). The mean absorbed organ doses were 5.3 ± 1.6 Gy (0.72 Gy/GBq) for the kidneys; 0.89 ± 0.42 Gy (0.12 Gy/GBq) for the liver; and 4.0 ± 1.1 Gy (0.55 Gy/GBq) for the parotid, 4.8 ± 2.8 Gy (0.64 Gy/GBq) for the submandibular, and 27 ± 10 Gy (3.8 Gy/GBq) for the lacrimal glands. The values (mean, SD, and ranges) for the corresponding absorbed doses per GBq are presented in Table 1. No substantial difference for absorbed doses of normal organs were observed when comparing them with respect to cycle number (Table 1; Fig. 2). The mean organ masses underlying these absorbed dose estimates were 1,595 ± 307 g (range, 1,165–2,373 g) for the liver, 153 ± 29.9 g (range, 88.4–218.7 g) for the kidneys, 19.1 ± 5.7 g (range, 8.0–35.6 g) for the parotid, 8.2 ± 1.9 g (range, 4.2–14.3 g) for the submandibular, and 0.45 ± 0.12 g (range, 0.25–0.78 g) for the lacrimal glands. For paired organs, masses from both sides were summed.

Absorbed doses for normal organs and tumors at respective cycle.
Dosimetry for Tumor Lesions
In total, all lesions received a mean dose per cycle of 23 ± 20 Gy (3.3 Gy/GBq). Mean absorbed dose for bone, lymph node, liver, and lung metastases were 26 ± 20 Gy (3.4 Gy/GBq), 24 ± 16 Gy (3.2 Gy/GBq), 8.5 ± 4.7 Gy (1.28 Gy/GBq), and 13 ± 7.4 Gy (1.7 Gy/GBq). The values (mean, SD, and range) for the corresponding absorbed doses per GBq are presented in Table 2. Figure 2 shows the mean absorbed dose in all tumor lesions with respect to the specific therapy cycle. Figure 3 shows a representative example of a patient with a histologically proven lung metastasis and multiple bone metastases. There is a clear trend toward a lower absorbed dose with an increasing number of the cycle. Mean absorbed dose per lesion was 26 ± 21 Gy (3.5 Gy/GBq) for the first, 24 ± 19 Gy (3.3 Gy/GBq) for the second, 20 ± 18 Gy (2.7 Gy/GBq) for the third, and 18 ± 17 Gy (2.4 Gy/GBq) for the fourth cycle. A similar trend can be seen for the subgroup of bone metastases. No reliable comparison is possible for lymph node, liver, and lung metastases because of a low sample number.

A 64-y-old patient with metastasis in lung (black arrow) and bone (white arrows). (A) Absorbed dose for lung metastasis for first, second, and third cycle were 20.9, 9.7, and 6.9 Gy, respectively. (B) SUVmax and SUVmean on pretherapeutic PET at each cycle were 21.2, 9.9, and 3.7 and 13.8, 6.6, and 2.5, respectively.
Correlation of SUV and Absorbed Doses in Tumor Lesions
The mean SUVmax and mean SUVmean of all lesions in pretherapeutic PET were 22 ± 14 (range, 3.5–64.8) and 15 ± 10 (range, 2.4–46.8), respectively (Supplemental Table 2). The mean change in SUV (ΔSUV) was 4.8 ± 8.2 (range, −7.2–34.8) for SUVmax and 3.3 ± 5.7 (range, −4.8–24.1) for SUVmean. SUVmax and SUVmean moderately correlated with absorbed dose for all lesions (r = 0.442, P < 0.001 and r = 0.433, P < 0.001, respectively; Supplemental Table 2; Supplemental Fig. 1). Change of SUVmax and SUVmean (ΔSUV) for all lesions showed a moderate and highly statistically significant correlation to the pretherapeutic SUV (r = 0.468, P < 0.001 for SUVmax; r = 0.498, P < 0.001 for SUVmean; Supplemental Table 3). No correlation could be found between the change of SUVmax and SUVmean (ΔSUV) for all lesions and the absorbed dose (r = 0.163, P = 0.129 for SUVmax; r = 0.153, P = 0.154 for SUVmean; Supplemental Table 4). Details for both correlations on the subgroups of bone and soft-tissue lesions are shown in Supplemental Tables 2, 3, and 4.
DISCUSSION
We present data for radiation dosimetry for normal organs and tumor lesions using 177Lu-PSMA I&T RLT in 18 patients and a total of 34 cycles. Our results for normal organs are comparable to recent clinical work on the safety and efficacy on 177Lu-PSMA I&T including results on dosimetry (7) and data reported for 177Lu-PSMA-DKFZ-617 (9,11,12). The kidneys are one of the critical organs, with a mean absorbed dose of 0.72 Gy/GBq and glandular tissue with high PSMA ligand uptake (lacrimal gland, 3.8 Gy/GBq; parotid gland, 0.55 Gy/GBq; and submandibular gland, 0.64 Gy/GBq). The long-term retention in tumor lesions resulted in a high mean absorbed tumor dose of 3.2 Gy/GBq, with a maximum of 12 Gy/GBq. In addition, high pretherapeutic SUV of a tumor lesion on PET may serve as rough indicator for a high absorbed dose, emphasizing the importance of pretherapeutic PSMA PET imaging for patient selection.
Data on the dosimetry are essential during the evaluation of new radiopharmaceuticals for radionuclide therapy to assess the risk of potential toxicity and response probability. There are common radiation tolerance limits as guiding values derived from external-beam radiation therapy. Thus, to some extent dose escalation studies can be omitted and dosing of new radiopharmaceuticals can be based on dosimetry. Qualitative judgment of the distribution of 177Lu-PSMA I&T showed physiologic tracer uptake in the abdominal organs, especially the kidneys, as well as the lacrimal and salivary glands (20). Besides the high number of patients and total number of cycles included, a further strength of this study is the availability of a late (6–8 d after injection) time point for posttherapeutic scintigraphy. Baum et al. also included late scintigraphy for their 177Lu-PSMA I&T dosimetry; however, only up to 5 d after injection (7). For 177Lu-PSMA-DKFZ-617 it has been shown that (mainly) overestimation of doses is present when omitting the late time point (mean, 9.8% for whole body; 22.0% for kidney; 19.4% for salivary glands; 10.6% for lacrimal glands) (12).
In several radio-receptor therapies, the kidney is regarded as the dose-limiting organ (21). Our results for kidneys (mean, 0.72 Gy/GBq) are well comparable to a recent publication using the same radiopharmaceutical (kidney: median, 0.8 Gy/GBq) (7). For 177Lu-PSMA-DKFZ-617, 3 recent reports state mean absorbed doses between 0.53 and 0.75 Gy/GBq for kidneys (9,11,12). These values are relatively comparable to that for the treatment of neuroendocrine tumors (for 177Lu-DOTATATE, for example, 0.6 Gy/GBq (22)).
The whole-body absorbed dose determined in our study (mean, 0.06 Sv/GBq; median, 0.03 Sv/Gy) was slightly different from that found by Baum et al. (7) (median, 0.02 Gy/GBq), with only a higher maximum range. This is potentially based on a higher overall tumor burden in our patient cohort (median PSA, 354.5 ng/mL) as compared with Baum et al. (median PSA, 43.2 ng/mL). Because 15 of 18 patients in our study demonstrated extensive bone involvement, red marrow cross-doses might have been high. However, therapy-induced myelosupression was not noted on clinical follow-up.
Other organs at risk are salivary and lacrimal glands. For parotid and submandibular glands, the organ doses (mean, 0.55 and 0.64 Gy/GBq) derived from our study are lower than in the recent report for 177Lu-PSMA I&T (median, 1.3 Gy/GBq) (7) and in the published data for 177Lu-PSMA-DKFZ-617 (mean, 0.72–1.4 Gy/GBq) (9,11,12). The main reason is most likely variations of the volumes used for dose estimation. For salivary glands, for example, Hohberg et al. (12) used 85 g based on International Commission on Radiologic Protection 23 data whereas Delker et al. (11) used 38 g based on individual organ masses. Because of the high intraindividual size variation, we also aimed to use individual values based on CT images, with a mean volume for both sides of 54 g. In addition, further variation is possible due to different tracer distribution, different time points of posttherapy scintigraphy, and different overall tumor burden. Finally, the effect of cooling of salivary glands and posttherapeutic stimulation of saliva production is still unclear. Currently data are too sparse to estimate the potential benefit of the latter.
For the lacrimal glands, potential discrepancies are even more pronounced when performing dosimetry because of their small size on the lacrimal glands. So far, only Hohberg et al. evaluated the organ dose for lacrimal glands using 177Lu-PSMA-DKFZ-617, with a mean of 2.8 Gy/GBq. Our calculations resulted in a mean organ dose of 3.8 Gy/GBq. However, we most likely underestimated the size of the lacrimal glands (mean of 0.8 g) in CT compared with Hohberg et al. using a mass assumption of 1.4 g based on MR data (12). With a mean underestimation of volumes in our calculation (∼42%), both results are quite comparable. However, despite the relatively high absorbed doses for salivary and lacrimal glands in clinical practice, they do not represent critical organs at risk. In our experience, despite the application of up to 30 GBq of 177Lu-PSMA I&T, so far only sporadic cases of reversible xerostomia and no considerable complaints on dry eyes were noted (10). Hey et al., for example, using external-beam radiation therapy, reported that a dose to the parotid glands below 26 Gy allowed complete recovery of pretherapeutic salivary flow rates (23).
The absorbed doses (especially for the critical organs) showed an excellent correlation between the 4 therapy cycles. Delker et al. reported an overall Pearsons ρ of 0.97 when comparing the first and second cycle in 5 patients using 177Lu-PSMA-DKFZ-617 (11). Similar results have been found for peptide receptor radionuclide therapy using up to 5 cycles (24). This might allow the prediction of the absorbed dose of the following therapy cycle with sufficient accuracy and the possibility of potential adaptation of the activity for the next cycle.
Our results for absorbed dose on tumor lesions (mean, 3.2 Gy/GBq) are comparable with data by Delker et al. (11) and Kratochwil et al. (9) for 177Lu-PSMA-DKFZ-617 and with Baum et al. (7) for 177Lu-PSMA I&T. In addition, we also analyzed and observed that the absorbed dose on the tumor was decreasing with the cycle number (Fig. 2; Table 2). In peptide receptor radionuclide therapy, this has also been reported for the use of 177Lu-ocreotate (25). Compared with leukemia, most lymphomas and germ cell tumors and epithelial tumors such as neuroendocrine tumors and PC are only moderately radiosensitive and require a significantly higher dose of radiation. The reason for a decreasing absorbed dose remains unclear. Potential explanation could be prior therapy effect with reduced target expression (in later cycles predominantly patients were included with reasonable prior response). An indirect sign for this is the considerable drop of the PSA value in these patients, indicating therapy response with potential decreased presence of the target in the next cycle.
The highly significant and moderate correlation between pretherapeutic SUV and absorbed dose of 177Lu-PSMA I&T (SUVmax: κ = 0.44, SUVmean: κ = 0.43) stresses the importance of pretherapeutic PET imaging. Similar results are known for peptide receptor radionuclide therapy (17). Our initial data are a preliminary basis for estimating therapeutic efficacy (or feasibility) of PSMA RLT. The highly significant moderate correlation between pretherapeutic SUV and change of SUV (ΔSUV) fits into the concept that with a higher target expression a higher molecular response can be expected. Nevertheless, the missing correlation between absorbed dose and change of SUV (ΔSUV) indicates that besides target expression other factors of tumor biology are present for determination of therapy response. In addition, it has to be considered that more sophisticated approaches exist, which can be used to predict the therapeutic biodistribution. For example, Hardiansyah et al. recently presented a so-called physiologically based pharmacokinetic model that aims for individualization of treatment planned and integrates a variety of patient-specific data (e.g., weight, tumor volume, and glomerular filtration rate) (26).
With the kidneys being the relevant critical organ, our data indicate that on average a cumulative activity of 40 GBq of 177Lu-PSMA I&T is safe when 28 Gy (50% probability of developing severe late kidney damage within 5 y) is the dose limit (27). With respect to the average life expectancy of mCRPC patients, this approach seems to be justifiable. This would allow at least 5 cycles using 7.4 GBq of 177Lu-PSMA I&T (standard activity at our institution), achieving relevant absorbed doses on tumor lesions and offering the possibility of several cycles for midterm tumor control. These findings are in line with data presented by Kabaskal et al. using pretherapeutic dosimetry for 177Lu-PSMA-DKFZ-617 and who calculated a maximum activity of 30 GBq to achieve a 23-Gy kidney dose (13). Nevertheless, these absorbed dose limits are based on the conventionally fractionated external-beam therapy and cannot necessarily be directly applied to low-dose-rate radiation (28). Patients without risk factors for kidney disease might tolerate a renal biologic equivalent dose up to 40 Gy, based on experience in NET (29).
There are several limitations of our study. First, the different peptides used for PET on one hand (PSMA-HBED-CC) and therapy on the other (PSMA I&T) are noteworthy. Second, one principal bias of dosimetry studies is the selection of tumor lesions that show better delineation from the surrounding healthy tissue and thus a relatively high absorbed dose. Numerous factors can impair the accuracy of PET and planar dosimetry and can lead to decreased correlation of the 2 modalities. Overlay in planar scintigraphy can lead to an overestimation of dose (11,20). SPECT should be the method of choice to avoid overlap with physiologic uptake and tumor uptake. Potential additional errors can occur both for volumetric assessment and for measurement of SUV for the tumor lesions. We tried to minimize this error, by adjusting a volume of interest using information from PET to the anatomic configuration of the lesions. However, especially for bone lesions, the anatomic delineation can be difficult. On the other hand, SUVmax (as compared with SUVmean) is a highly reproducible metric, with small expected error for quantification in the range of up to 10% (30,31). Third, we have not applied any sophisticated model in this study to aim for individual treatment planning. Fourth, it has to be stressed that the data comparing absorbed doses in different treatment cycles are not based on the same patients.
CONCLUSION
Organ- and tumor-absorbed doses for 177Lu-PSMA I&T for RLT are comparable to recent reports using the same ligand as well as 177Lu-PSMA-DKFZ-617. The kidneys represent the critical organ, with a mean absorbed dose of 0.72 Gy/GBq. Kidney-absorbed dose is relatively similar across different studies and is constant across several cycles in the same patient. When established dose limits from radiation oncology are used, up to 40 GBq of 177Lu-PSMA I&T appear feasible, with limited risk of radiation-induced side-effects on normal organs given the average life expectancy for mCRPC patients. The preliminary correlation between pretherapeutic SUV and absorbed tumor dose emphasizes the need for initial PSMA ligand PET imaging for appropriate patient selection. Nevertheless, more data need to be collected from larger series to confirm and validate these initial findings.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 18, 2016.
- Accepted for publication August 30, 2016.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Characterization of Effective Half-Life for Instant Single-Time-Point Dosimetry Using Machine Learning
- Preclinical Evaluation of 177Lu-rhPSMA-10.1, a Radiopharmaceutical for Prostate Cancer: Biodistribution and Therapeutic Efficacy
- Safety, Dosimetry, and Feasibility of [68Ga]Ga-PSMA-R2 as an Imaging Agent in Patients with Biochemical Recurrence or Metastatic Prostate Cancer
- Mathematic Modeling of Tumor Growth During [177Lu]Lu-PSMA Therapy: Insights into Treatment Optimization
- Dosimetry of [177Lu]Lu-PSMA-Targeted Radiopharmaceutical Therapies in Patients with Prostate Cancer: A Comparative Systematic Review and Metaanalysis
- First Safety and Efficacy Data with the Radiohybrid 177Lu-rhPSMA-10.1 for the Treatment of Metastatic Prostate Cancer
- Renal and Multiorgan Safety of 177Lu-PSMA-617 in Patients with Metastatic Castration-Resistant Prostate Cancer in the VISION Dosimetry Substudy
- An Intrapatient Dosimetry Comparison of 177Lu-rhPSMA-10.1 and 177Lu-PSMA-I&T in Patients with Metastatic Castration-Resistant Prostate Cancer
- Lesion Dosimetry for [177Lu]Lu-PSMA-617 Radiopharmaceutical Therapy Combined with Stereotactic Body Radiotherapy in Patients with Oligometastatic Castration-Sensitive Prostate Cancer
- Prediction of Response to 177Lu-PSMA Therapy Based on Tumor-to-Kidney Ratio on Pretherapeutic PSMA PET/CT and Posttherapeutic Tumor-Dose Evaluation in mCRPC
- Antihormonal-Treatment Status Affects 68Ga-PSMA-HBED-CC PET Biodistribution in Patients with Prostate Cancer
- Albumin-Binding and Conventional PSMA Ligands in Combination with 161Tb: Biodistribution, Dosimetry, and Preclinical Therapy
- Synthesis and Preclinical Evaluation of 177Lu-Labeled Radiohybrid PSMA Ligands for Endoradiotherapy of Prostate Cancer
- Prostate-Specific Membrane Antigen Radioligand Therapy Using 177Lu-PSMA I&T and 177Lu-PSMA-617 in Patients with Metastatic Castration-Resistant Prostate Cancer: Comparison of Safety, Biodistribution, and Dosimetry
- Pretherapeutic Comparative Dosimetry of 177Lu-rhPSMA-7.3 and 177Lu-PSMA I&T in Patients with Metastatic Castration-Resistant Prostate Cancer
- Kidney Doses in 177Lu-Based Radioligand Therapy in Prostate Cancer: Is Dose Estimation Based on Reduced Dosimetry Measurements Feasible?
- Tumor Sink Effect in 68Ga-PSMA-11 PET: Myth or Reality?
- Dosimetry in Clinical Radiopharmaceutical Therapy of Cancer: Practicality Versus Perfection in Current Practice
- Normal-Tissue Tolerance to Radiopharmaceutical Therapies, the Knowns and the Unknowns
- The Impact of Monosodium Glutamate on 68Ga-PSMA-11 Biodistribution in Men with Prostate Cancer: A Prospective Randomized, Controlled Imaging Study
- Comparative Preclinical Biodistribution, Dosimetry, and Endoradiotherapy in Metastatic Castration-Resistant Prostate Cancer Using 19F/177Lu-rhPSMA-7.3 and 177Lu-PSMA I&T
- Low-dose targeted radionuclide therapy renders immunologically cold tumors responsive to immune checkpoint blockade
- Radiation Dosimetry in 177Lu-PSMA-617 Therapy Using a Single Posttreatment SPECT/CT Scan: A Novel Methodology to Generate Time- and Tissue-Specific Dose Factors
- Long-Term Follow-up and Outcomes of Retreatment in an Expanded 50-Patient Single-Center Phase II Prospective Trial of 177Lu-PSMA-617 Theranostics in Metastatic Castration-Resistant Prostate Cancer
- Patients Resistant Against PSMA-Targeting {alpha}-Radiation Therapy Often Harbor Mutations in DNA Damage-Repair-Associated Genes
- First Clinicopathologic Evidence of a Non-PSMA-Related Uptake Mechanism for 68Ga-PSMA-11 in Salivary Glands
- Early Experience of Rechallenge 177Lu-PSMA Radioligand Therapy After an Initial Good Response in Patients with Advanced Prostate Cancer
- Dosimetry of 177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer: Correlations Between Pretherapeutic Imaging and Whole-Body Tumor Dosimetry with Treatment Outcomes
- Modeling and Predicting Tumor Response in Radioligand Therapy
- The Effect of Total Tumor Volume on the Biologically Effective Dose to Tumor and Kidneys for 177Lu-Labeled PSMA Peptides
- Repeated 177Lu-Labeled PSMA-617 Radioligand Therapy Using Treatment Activities of Up to 9.3 GBq
- Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy