


Abstract
Current treatment protocols for 177Lu-labeled PSMA-617 therapies were cautiously derived from dosimetry data, but their practical appropriateness has not yet been proven clinically. We retrospectively report our clinical observations using 4 different treatment activities. Methods: Forty patients with advanced prostate cancer and positive uptake in prostate-specific membrane antigen (PSMA) imaging were treated with 4 GBq of 177Lu activity/80 nmol of precursor, 6 GBq of 177Lu activity/120 nmol of precursor, 7.4 GBq of 177Lu activity/150 nmol of precursor, or 9.3 GBq of 177Lu activity/150 nmol of precursor (10 patients per group) every 2 mo. Safety was checked every 2 wk by laboratory tests, the prostate-specific antigen response was checked every 4 wk, and other effects were assessed by anamnesis. Results: The initial prostate-specific antigen response showed no correlation with treatment activity. However, 2 of 10, 4 of 10, 4 of 10, and 7 of 10 patients receiving doses of 4, 6, 7.4, and 9.3 GBq, respectively, were in partial remission 8 wk after completing all 3 cycles. This finding would be in line with but—because of low patient numbers—would not prove a positive dose–response relationship. Acute hematologic toxicity was also not correlated with treatment activity, and no more than 1 patient per group had grade 3/4 toxicity. Nevertheless, in contrast to the findings for the other groups, the mean platelet count in the 9.3-GBq group decreased chronically over time. Conclusion: If patients with diffuse red marrow infiltration and extensive chemotherapeutic pretreatments are excluded, then treatment activities of up to 3 injections of 9.3 GBq of 177Lu-PSMA-617 every 2 mo are tolerated well. Further dose escalation should be conducted with care, as the highest dose seems to be close to the maximum tolerable dose.
Approximately 85%–90% of prostate cancer relapses occurring after curative intended primary therapy have a prostate-specific membrane antigen (PSMA)–positive tumor phenotype (1). It has also been reported that invasive growth, metastasis, and hormone independence are associated with an overexpression of PSMA histologically (2–4). Therefore, most patients with metastasized castration-resistant prostate cancer might be suitable for radioligand therapy (RLT) targeting PSMA (PSMA-RLT). The Glu-urea–based ligand PSMA-617 was preclinically optimized for low kidney uptake and improved ligand-induced cellular internalization. Coupling with DOTA enabled labeling with several diagnostic and therapeutic radionuclides (5). Different centers (6–8) reported favorable dosimetry for 177Lu-PSMA-617 which—with regard to the kidney dose (∼0.6 Gy/GBq) and the red marrow dose (∼0.03 Gy/GBq)—outperformed a 177Lu-labeled PSMA antibody (9), an 131I-labeled small-molecule PSMA ligand (10), and the RLT reference compound 177Lu-DOTATATE (11). On the basis of the available dosimetry data, the 177Lu-PSMA-617 activities used for the first PSMA-RLTs were chosen cautiously. However, even these very first reports demonstrated promising antitumor activity (8,12). Nevertheless, tolerance limits for normal organs reported in the literature were based on external-beam radiotherapy and were only extrapolated to RLT using radiobiologic models, which themselves have manifold limitations, as reviewed recently (13). Thus, dosimetry in nuclear medicine can only provide guidance about doses in RLT; the optimal treatment regimen still must be refined clinically.
In this retrospective analysis, we report our clinical experience with doses of 4, 6, 7.4, and 9.3 GBq of 177Lu-PSMA-617 repeated every 2 mo.
MATERIALS AND METHODS
Patients
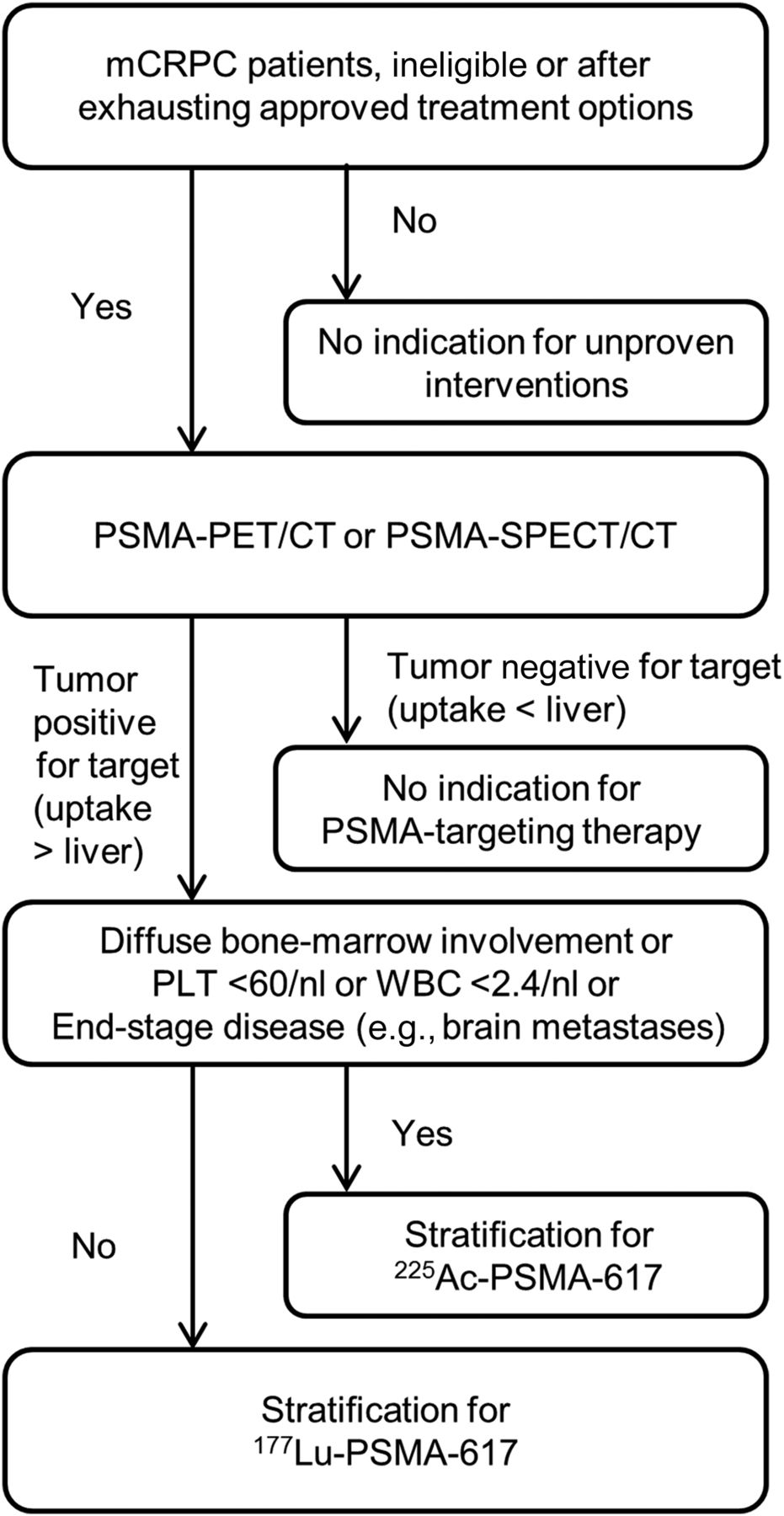
RLT with 177Lu-PSMA-617 was performed under the conditions of the updated Declaration of Helsinki (item 37 [unproven interventions in clinical practice]) and in accordance with the Pharmaceuticals Act [§13(2b)] as a salvage therapy for patients who had metastasized castration-resistant prostate cancer (which had to be resistant to or ineligible for approved options) and progressive disease. Patient selection is outlined in Figure 1. For patients stratified to receive 177Lu-PSMA-617, each dose level was administered to 10 consecutive patients. If toxicities were comparable to those in the placebo group of the ALSYMPCA trial (14), then individual dose escalations for nonresponders were considered ethically justified; this approach resulted in a short learning phase using heterogeneous dose regimens between respective dose escalation groups. Data from patients in these heterogeneous interim groups were not suitable for this kind of systematic evaluation; however, some are available in other publications (8,15). The chronology of how the dose escalation was embedded into clinical practice is summarized in Figure 2. Patient characteristics are summarized in Table 1. All patients were informed about the experimental character of the therapy and signed written informed consent forms. The clinical data are reported retrospectively with approval of the Ethics Committee of the Medical Faculty of Heidelberg University (Permit S-321).

Clinical standard operating procedure for selection of patients to receive 177Lu-PSMA-617 therapy. mCRPC = metastasized castration-resistant prostate cancer; PLT = platelets.

Flowchart demonstrating how dose escalation was embedded in clinical practice, resulting in chronological separation of patients into dose groups. ITT = intention to treat; PD = progression of disease; SAEs = serious adverse events; SOP = standard operating procedure.
Baseline Characteristics of Patients
Radiopharmaceuticals
The good manufacturing practices–grade precursor for PSMA-617 was obtained from ABX Advanced Biochemical Compounds and labeled with 177Lu, which was obtained from either iTG or Perkin–Elmer, as described previously (8). The molar activity was 1 GBq of 177Lu per 20 nmol of precursor, with a maximum amount of 150 nmol of injected substance. Quality control of the drug was performed by reverse-phase high-performance liquid chromatography and instant thin-layer chromatography pretherapeutically and always revealed labeling yields of greater than 99%.
Treatment Protocol
According to the German Radiation Protection Ordinance, patients were treated as inpatients for 48 h and discharged when the γ-emission from the patients was less than 3.5 μSv/h at a 2-m distance. On the therapy day, laboratory tests and anamnesis were performed. The therapy solution was injected manually over 30–60 s via a low-protein-binding sterile filter (Filtropur S 0.2; Sarstedt). Patients received concomitant intravenous hydration (2,000 mL; started 30 min before application of the therapy solution). The intention-to-treat protocol was a 3-cycle PSMA therapy, with cycles administered every 2 mo. Radiologic restaging was planned for 2 mo after the third cycle but was done earlier in cases of clinical and biochemical progression.
Follow-up
Laboratory tests were performed every 2 wk for 8 wk after each cycle. Blood cell counts were checked every 2 wk; serum creatinine, blood urea nitrogen, alkaline phosphatase, liver enzyme, and prostate-specific antigen (PSA) levels were checked every 4 wk. Hematologic toxicity was translated into a grading scale according to the Common Terminology Criteria for Adverse Events Version 4.0 (16). Clinical side effects at each treatment cycle were assessed by anamnesis.
RESULTS
Clinical Findings
The administration of each treatment cycle was tolerated well by all patients. No serious nonhematologic side effects were observed, and grade 4 hematologic toxicity was observed in only 1 patient (in the 9.3-GBq group). Especially after the first cycle and irrespective of dose group, patients with symptomatic bone metastases reported a transient increase in pain (flare-up) in the known metastases in the first 1–4 d after treatment and then a decrease in pain symptoms to below the baseline.
Hematologic Toxicity
Data from 8 wk of follow-up were available for all patients in each group. The mean counts of platelets and white blood cells (WBCs) over time are shown in Figure 3. In the 4-, 7.4-, and 9.3-GBq groups, platelets showed a nadir at week 4, but this trend was very moderate; this pattern was not demonstrated in the 6-GBq group. WBC counts typically dropped during the first 2 wk; later, they were undulant over serial time points. For patients who completed 3 cycles, including the respective follow-up, the courses of platelet and WBC counts over the complete 24-wk period (i.e., 6 mo) are shown in Figure 3. In the 9.3-GBq group, a chronic decrease in platelet counts during follow-up was observed; however, in most patients, the absolute counts were still in the reference range.

Hematologic toxicity over 8 wk (A and C) and 24 wk (B and D) of 177Lu-PSMA-617 RLT. (A and B) Platelet counts (/nL); reference range is 150–440/nL. (C and D) WBC counts (/nL); reference range is 4–10/nL.
After the first cycle, 1 patient in the 4-GBq group had grade 3 thrombocytopenia (38 platelets/nL), and 2 patients in this group had grade 2 leukopenia (WBC counts decreased from 2.46/nL at baseline to 2.3/nL at week 8 in 1 patient and from 3.63/nL at baseline to 2.7/nL at week 8 in the other patient). In the 6-GBq group, only 1 patient had grade 1 thrombocytopenia, and no pathologic leukopenia was observed. In the 7.4-GBq group, 1 patient had grade 2 leukopenia (WBC counts decreased from 3.3/nL at baseline to 2.8/nL at week 8) and 1 patient had grade 3 leukopenia (WBC counts decreased from 4.35/nL at baseline to 1.9/nL at week 6 but recovered to 2.54/nL at week 8) accompanied by grade 1 thrombocytopenia. In the 9.3-GBq group, blood cell counts worsened by only 1 toxicity grade and no grade 3/4 result was observed after the first therapeutic injection.
During the 24-wk regimen, we additionally observed 1 patient with grade 1 thrombocytopenia (a platelet count of 85/nL at week 8 recovered to 218/nL at week 12) and 1 patient with grade 2 leukopenia (a WBC count of 2.57/μL at week 10 recovered to 4.38/μL at week 24) in the 6-GBq group. In the 7.4-GBq group, only 1 patient had grade 1 leukopenia after the second cycle (a WBC count of 3.0/μL at week 10). In the 9.3-GBq group, 1 patient had grade 4 thrombocytopenia (a platelet count of 21/nL at week 20), 1 patient had grade 1 leukopenia, and 2 patients had grade 2 leukopenia. The patient with grade 4 thrombocytopenia and concurrent grade 2 leukopenia received a dose reduction to 6 GBq for the third cycle to reduce hematologic side effects.
Like the mean cell count data, a small number of patients in all dose regimens developed a worsening of cell blood counts by more than 1 grade. In all affected patients, intratherapeutic 177Lu emission scans indicated red marrow infiltration and progression in comparison with pretherapeutic PSMA imaging; these patients also shared a history of chemotherapy.
Response
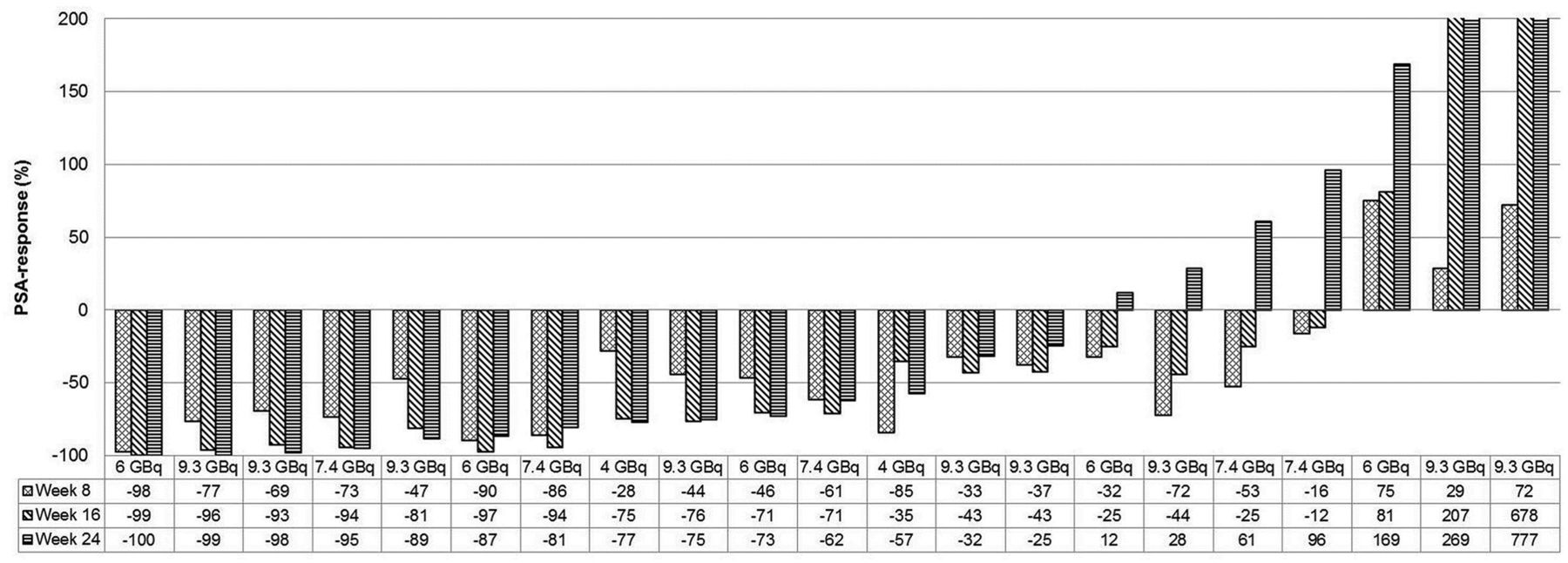
The PSA response at 8 wk after the first treatment cycle, as shown graphically in waterfall graphs (Fig. 4), demonstrated no major differences among the 4 dose groups. Any decline in the PSA level was observed in 90%, 70%, 70%, and 80% of patients in the 4 dose groups. A decline in the PSA level of greater than 50% was observed in 40%, 30%, 50%, and 30% of patients in the 4-, 6-, 7.4-, and 9.3-GBq groups, respectively.

Waterfall graphs of initial (week 8) PSA responses for 4-GBq group (A), 6-GBq group (B), 7.4-GBq group (C), and 9.3-GBq group (D).
Because of biochemical progression or delayed recovery of blood cell counts, only 21 of 40 patients completed the treatment as planned. From the population receiving the intention-to-treat protocol, 2 of 10 patients (4-GBq group), 5 of 10 patients (6-GBq group), 5 of 10 patients (7.4-GBq group), and 9 of 10 patients (9.3-GBq group) completed the 3 cycles of RLT in accordance with the protocol. An objective radiologic response at week 24 was demonstrated for 2 of 10 patients (4-GBq group), 4 of 10 patients (6-GBq group), 4 of 10 patients (7.4-GBq group), and 7 of 10 patients (9.3-GBq group). Except for 1 patient who experienced 61% PSA progression but had radiologically “stable disease,” the imaging-based restaging correlated well with the PSA response. The PSA follow-up data for patients who completed the treatment in accordance with the protocol are summarized in Figure 5.
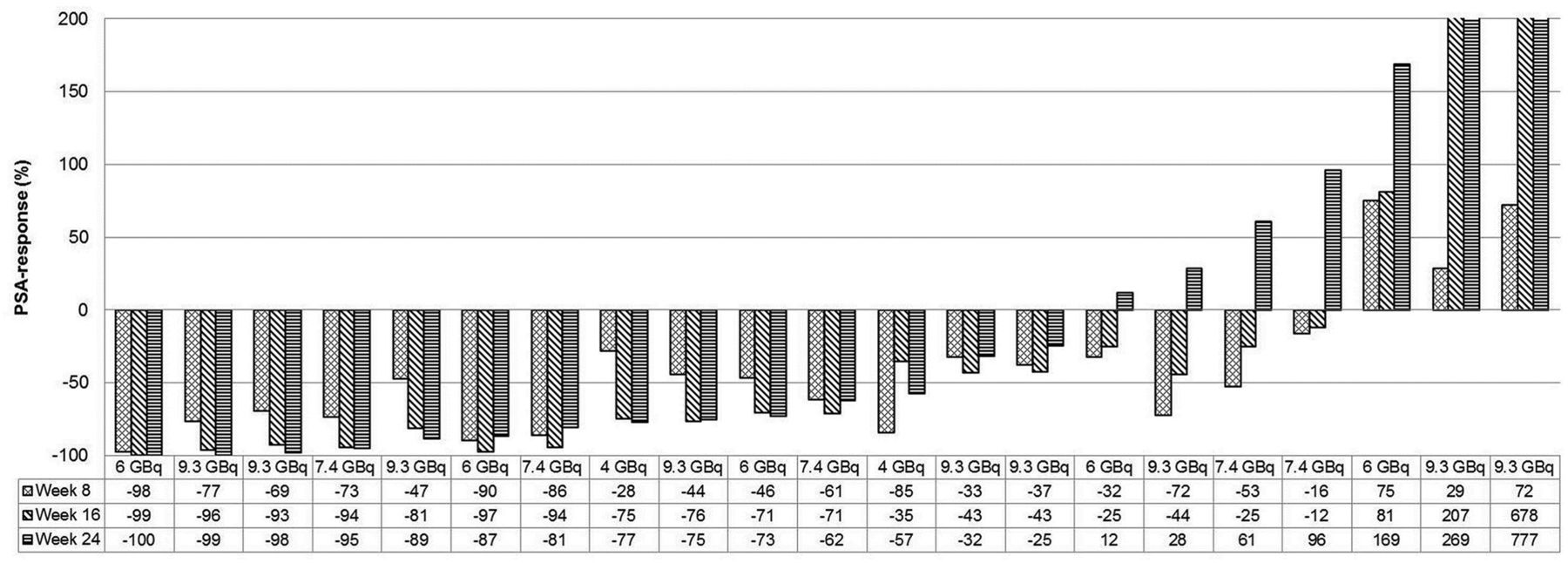
Longitudinal follow-up of PSA levels during 3 cycles of 177Lu-PSMA-617. Changes in PSA levels are presented as percentages (comparison of PSA level at particular week to PSA level at baseline).
DISCUSSION
Here, we retrospectively report our clinical experience with various treatment activities of 177Lu-PSMA-617 during salvage therapy of 40 patients with metastasized castration-resistant prostate cancer.
The first clinical application of PSMA-RLT was done in 2011–2012 using a 131I-labeled PSMA ligand. The treatment activity was chosen after 124I PET-based dosimetry, taking into account a 1-Gy red marrow tolerance dose; hematologic toxicities were mild (10). During repeated treatments, grade 3/4 hematologic toxicities remained rare (16). Any PSA response was demonstrated in 84% (21/25) of the patients (10); a PSA decline of greater than 50% after the first treatment cycle was achieved in 70.6% of 34 patients (17). PSMA-RLT based on 177Lu has practical advantages, and the PSMA-617 ligand even has refined pharmacokinetics and radiation dosimetry (5,8). Thus, theoretically, 177Lu-PSMA-617 should improve the therapeutic range of PSMA-RLT. Nevertheless, until now, the reported PSA response rates commonly have been remarkably lower; the largest multicenter investigation of 177Lu-PSMA-617 reported only a 40% biochemical response rate after the first treatment cycle (17). Therefore, a critical discussion about currently used treatment protocols seems warranted.
Dosimetry studies of 177Lu-PSMA-617 have been performed with variable methodologies at different centers, but all investigators have reported similar results (6–8,18,19). The essential organs red marrow (∼0.03 Gy/GBq) and kidneys (∼0.6 Gy/GBq) should be considered dose-limiting organs (6–8,18,19). Given a red marrow tolerance dose of 1 Gy, single-cycle activities of up to 30 GBq of 177Lu could be proposed (7). Taking into account the concept of a biologic effective dose during low-dose-rate radionuclide therapy, a kidney tolerance dose of 28–40 Gy was suggested for 177Lu-radiopharmaceuticals (20), theoretically making a cumulative treatment activity of 50 GBq of 177Lu-PSMA-617 reasonable. No grade 3/4 renal toxicity was observed in 55 patients treated with 3 doses of 6 GBq of 177Lu-PSMA-617 (21). However, the high prevalence of bone metastases, the use of approved chemotherapeutic options before salvage therapy, and the fact that the patients were elderly introduced some doubt about whether the tolerance doses of red marrow and other organs reported in the literature were still valid for the patient cohort. Thus, it was reasonable that 177Lu-PSMA-617 RLT treatment regimens were initially introduced with caution.
Recent publications predominantly focused on a treatment activity of 6 GBq administered every 2 mo (22–28), and the results were in agreement with each other. All authors reported few cases of grade 3/4 toxicity—that is, in the same dimension as the incidence of tumor-related adverse events observed in the placebo arm of the ALSYMPCA trial (14)—and, despite moderate xerostomia, there was no evidence of relevant treatment-related toxicity. However, the treatment activities used were remarkably lower than the projected maximum tolerance dose, according to dosimetry estimates: a red marrow dose of only 0.2 Gy (6 GBq × 0.03 Gy/GBq). Simultaneously, the PSA response rates were lower than older 131I-PSMA RLT data obtained with the full 1-Gy red marrow tolerance limit (10,16). Surprisingly, none of the authors (22–28) discussed the possibility that the escalation of 177Lu treatment activity to an estimated red marrow absorbed dose of 0.2–1.0 Gy should still be tolerated well and should offer the chance to further improve antitumor activity because a positive dose–response relationship is normally expected in radiotherapy. Therefore, after the clinical introduction of 177Lu-PSMA-617, for us it seemed ethically mandatory to increase treatment activity until either tolerable grade 1/2 toxicity appeared or patients achieved enduring remission.
Because of limited numbers of patients, it is statistically not reasonable and not in the scope of the present report to draw a final conclusion about which dosing regimen provides the optimal therapeutic range. It was already reported that PSA and objective radiologic responses to PSMA-RLT correlated poorly with individual tumor absorbed doses (29). For individual patients, the respective radiosensitivity of the particular tumor and other clinical factors (30) seem to be relevant for determining response probability. It is possible that even high doses of 177Lu-PSMA-617 cannot achieve the same response rates as 131I-MIP1095 because this older ligand was used in the preabiraterone/preenzalutamide era and current patients have more previous therapies than these historical controls. Thus, an efficacy analysis cannot be based on a case series of serially treated patients but requires a group comparison after random assignment. For such a purpose, a prospective phase 2 study would be needed.
Up to the highest treatment activity (9.3 GBq), we did not observe increasing numbers of dose-limiting grade 3/4 toxicities. However, in contrast to a formal clinical trial, salvage therapy must be conservative. Thus, we made the clinical decision to stop dose escalation once we observed an incomplete recovery of blood cell counts to the baseline, even before critical absolute numbers were reached. Because there was no randomization (which would define the study as “medical research” and which is not possible during “unproven interventions in clinical practice”), simply by chance the 9.3-GBq group contained the most patients with previous chemotherapy and the highest alkaline phosphatase and PSA levels—which might be a sufficient explanation for the reduced red marrow reserve. Thus, the dose-limiting effects attributed to the 9.3-GBq activity might have been an accidental observation caused by patient selection, and even higher activities might be possible for well-selected patients. However, our aim was to establish a reasonable standard operating procedure appropriate for patients currently scheduled to receive PSMA-RLT and without the routine need for sophisticated pretherapeutic dosimetry to identify statistical outliers in advance. The good tolerability observed in our patient series is well in line with the dosimetry-based expectation. The estimated average red marrow dose of 0.3 Gy/cycle (9.3 GBq × 0.03 Gy/GBq) is far below the accepted red marrow tolerance limit of 1 Gy and, with a ratio of 0.3:1 Gy, there are enough safety margins for individual patient variability to warrant the application of standard doses.
It should be noted that for patients with diffuse red marrow infiltration, we use 225Ac-PSMA-617 targeted α-therapy (Fig. 1) whenever this radionuclide is available. These types of challenging patients might have been underrepresented in our patient cohort. Modeling of red marrow absorbed doses normally neglects the contribution of β-particles that are emitted from bone metastases to the surrounding healthy red marrow. For 177Lu, the 1.5-mm maximum β-range in water corresponds to approximately 30 cell layers; this routinely neglected factor might be relevant in patient with very advanced disease. Thus, individual dose reductions should be considered for patients with diffuse red marrow infiltration.
CONCLUSION
For patients without extensive red marrow involvement, repeated applications of 7.4–9.3 GBq of 177Lu-PSMA-617 per cycle are associated with moderate acute hematologic toxicity and other nonhematologic side effects. The incomplete platelet recovery observed in the 9.3-GBq group might imply that the potential for further dose escalations is limited. However, there is still a high demand for prospective controlled clinical trials to evaluate the fractionation regimen that enables the longest duration of tumor control and survival.
DISCLOSURE
Uwe Haberkorn and Klaus Kopka benefit from a patent for PSMA-617, which is held by their respective affiliations. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 10, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 18, 2017.
- Accepted for publication July 12, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Deescalated 225Ac-PSMA-617 Versus 177Lu/225Ac-PSMA-617 Cocktail Therapy: A Single-Center Retrospective Analysis of 233 Patients
- 177Lu-PSMA Therapy
- Dosimetry in Clinical Radiopharmaceutical Therapy of Cancer: Practicality Versus Perfection in Current Practice
- A Microdosing Study with 99mTc-PHC-102 for the SPECT/CT Imaging of Primary and Metastatic Lesions in Renal Cell Carcinoma Patients
- 177Lu-EB-PSMA Radioligand Therapy with Escalating Doses in Patients with Metastatic Castration-Resistant Prostate Cancer
- Dosimetry Estimate and Initial Clinical Experience with 90Y-PSMA-617
- Predictive Factors of Response and Overall Survival in Patients with Castration-Resistant Metastatic Prostate Cancer Undergoing 177Lu-PSMA Therapy