


Abstract
The intense accumulation of prostate-specific membrane antigen (PSMA) radioligands in salivary glands is still not well understood. It is of concern for therapeutic applications of PSMA radioligands, because therapeutic radiation will damage these glands. A better understanding of the uptake mechanism is, therefore, crucial to find solutions to reduce toxicity. The aim of this study was to investigate whether the accumulation of PSMA-targeting radioligands in submandibular glands (SMGs) can be explained with PSMA expression levels using autoradiography (ARG) and immunohistochemistry (IHC). Methods: All patients gave written informed consent for further utility of the biologic material. The SMG of 9 patients, pancreatic tissue of 4 patients, and prostate cancer (PCA) lesions of 9 patients were analyzed. Tissue specimens were analyzed by means of PSMA-IHC (using an anti–PSMA-antibody and an immunoreactivity score system [IRS]) and ARG using 177Lu-PSMA-617 (with quantification of the relative signal intensity compared with a PSMA-positive standard). The SUVmax in salivary glands, pancreas, and PCA tissues were quantified in 60 clinical 68Ga-PSMA-11 PET scans for recurrent disease as well as the 9 primary tumors selected for ARG and IHC. Results: PCA tissue samples revealed a wide range of PSMA staining intensity on IHC (IRS = 70–300) as well as in ARG (1.3%–22% of standard). This variability on PCA tissue could also be observed in 68Ga-PSMA-11 PET (SUVmax, 4.4–16) with a significant correlation between ARG and SUVmax (P < 0.001, R2 = 0.897). On IHC, ARG, and 68Ga-PSMA-11 PET, the pancreatic tissue was negative (IRS = 0, ARG = 0.1% ± 0.05%, SUVmax of 3.1 ± 1.1). The SMG tissue displayed only focal expression of PSMA limited to the intercalated ducts on IHC (IRS = 10–15) and a minimal signal on ARG (1.3% ± 0.9%). In contrast, all SMG showed a high 68Ga-PSMA-11 accumulation on PET scans (SUVmax 23.5 ± 5.2). Conclusion: Our results indicate that the high accumulation of PSMA radioligands in salivary glands does not correspond to high PSMA expression levels determined using ARG and IHC. These findings provide evidence, that the significant accumulation of PSMA radioligands in SMG is not primarily a result of PSMA-mediated uptake.
- prostate cancer
- prostate-specific membrane antigen
- 177Lu-PSMA-617
- 68Ga-PSMA-11
- positron emission tomography
- immuno-histochemistry
- autoradiography
The prostate-specific membrane antigen (PSMA) is upregulated in prostate cancer (PCA), whereas only a few normal organs and tissue show physiologic expression (1–3). Currently, 68Ga-PSMA-11 is widely used as a primary imaging tool for PCA restaging using PET at biochemical recurrence (4,5). It enables a high detection rate of small soft-tissue and bone lesions even at low prostate-specific antigen (PSA) values (6). The high and specific tumor uptake of 68Ga-PSMA-11 prompted researchers to develop PSMA ligands with a DOTA-chelator (e.g., PSMA-617), for labeling with 177Lu for therapeutic applications (7,8). Off-target uptake of PSMA radioligands was commonly detected in the kidneys, duodenum and small bowel, and lacrimal and major salivary glands (9). First dosimetry studies of 177Lu-PSMA-617 revealed a significantly higher mean absorbed dose in salivary glands (1.4 Gy/GBq) than in kidneys (0.75 Gy/GBq) (10). This is in concordance with first results obtained after 177Lu-PSMA-617 therapy, where no early nephrotoxicity, but some transient xerostomia in 8%–20% of the patients was observed (7,11). High salivary gland uptake is of particular concern when PSMA ligands are applied with α-particle emitters, such as 225Ac, since this resulted in irreversible xerostomia and, hence, dose-limiting toxicity (12,13).
It was previously reported that PSMA is physiologically expressed on normal prostate epithelial cells, in the small intestine, renal tubular cells, and the salivary glands, however, at much lower levels than in PCA tissue (13–15). Other publications reported on immunohistochemical investigations, which showed no PSMA expression in salivary glands (2,16,17). These findings were in agreement with the fact that PSMA-specific radioimmunoconjugates, such as 111In-J591 and 177Lu-J591, did not accumulate in salivary glands (18).
A previous comment on the importance of salivary gland toxicity in PSMA-targeted radionuclide therapy stated the lack of sufficient data and understanding of the high uptake of PSMA ligands (19).
Published mouse experiments do not reveal high accumulation of PSMA-targeting radioligands in salivary gland tissue (20,21). Therefore, such models are not suitable to investigate radiotherapy-related side effects to the salivary glands or methods to reduce salivary gland uptake of PSMA-targeting ligands.
The aim of this study was to compare the in vivo accumulation of 68Ga-PSMA-11 in the PCA tissue, salivary glands, and pancreas of patients with the PSMA expression levels on PCA patient tissue, as well as to benign salivary gland and pancreatic tissue using immunohistochemistry (IHC) and in vitro autoradiography (ARG).
MATERIALS AND METHODS
Patients for IHC and ARG
Patients undergoing neck dissections including tumor-free submandibular glands (SMGs) were prospectively selected. Tissues of patients who underwent pancreas resection were included for the analysis of benign pancreatic tissue. All patients with prostatectomy for PCA and preoperative 68Ga-PSMA-11 PET/MRI available were screened, and cases with tumor in the apex were selected, as fresh frozen tissue after standard prostatectomy was only available from the apex. For PET quantification in normal tissue, patients, referred to a 68Ga-PSMA-11 PET for biochemical recurrence, were included. All patients gave written informed consent to further analysis of their data and biologic material within biobank protocols approved by the local ethics committee (BASEC no. 2016-00778, 2017-01319, KEK-StV-Nr: 40/08 and KEK-ZH-Nr. 06/08). The direct comparison to 68Ga-PSMA-11 PET images was only possible for the PCA specimens. To determine the uptake of 68Ga-PSMA-11 in PCA relative to the uptake in salivary glands and pancreas, an additional cohort of 60 patients who previously underwent 68Ga-PSMA-11 PET for biochemical recurrence was included in a retrospective analysis (Fig. 1).

Overview of selected patients for tissue collection for ARG and IHC (SMG 01–09), pancreas (PANC 01–04), and primary PCA (PCA 01–09), as well as PSMA PET quantification, including the 9 patients with primary PCA (PCA 01–09) and 60 patients referred for restaging for the analysis of average uptake on salivary glands, pancreas, spleen, liver, and PCA metastasis.
Tissue Preparation, PSMA IHC, and Evaluation
Fresh tissue of all types, obtained from the resection specimens immediately after surgery, was snap frozen. The remaining tissue was formalin-fixed, paraffin-embedded, and examined on 2-μm-thick hematoxylin & eosin (H&E)–stained sections. Both tissue types were compared microscopically to be representative. Immunohistochemical staining for PSMA (DAKO, M3620, clone 3E6, 1:25) was performed as described previously (22). PSMA expression was evaluated using a 3-tiered system (1+ weak, 2+ moderate, 3+ strong), and the area covered by staining was estimated in the following scale (1%, 2%, 5%, 10% followed by further 10% steps). Immunoreactivity score (IRS) was calculated as IRS = IHC expression score multiplied by the area covered (23). The area fraction covered by carcinoma and Gleason scores were determined by an experienced genitourinary pathologist after digitalization of the slides (Nanozoomer NDP digital slide scanner C9600-12) using the Hamamatsu NDP.view 2.6.8 Software.
In Vitro PSMA ARG
PSMA-617 (ABX GmbH) was labeled with no-carrier-added 177Lu (ITG GmbH) under standard labeling conditions as previously reported (20). In vitro ARG was performed on frozen sections of patient tissue and mouse xenografts (highly PSMA-positive PC-3 PIP and PSMA-negative PC-3 flu tumors). In brief, buffer-treated sections were incubated with a solution of 177Lu-PSMA-617 (1.5 MBq/mL in Tris-HCl buffer containing 1% bovine serum albumin) with or without blocking agent (200 μM 2-(phosphonomethyl)-pentandioic acid [2-PMPA; Sigma]) for 60 min at room temperature. Afterward, the sections were washed twice in cold Tris-HCl buffer (with 0.25% bovine serum albumin), twice in pure Tris-HCl buffer, and finally rinsed with cold distilled water. The air-dried sections were exposed to a phosphor imaging screen (Super Resolution; Perkin Elmer, USA) that was developed using a radiometric phosphor imager (Cyclone Plus Storage Phosphor System; Perkin Elmer). The signal intensity on the autoradiographic images was quantified using the OptiQuant Acquisition software (version 5.0; Perkin Elmer). PC-3 PIP and PC-3 flu tumor xenograft sections were used as a positive or negative control, respectively. It is important to recognize that PSMA-transduced PC-3 (PC-3 PIP) tumors express PSMA reproducibly at levels much higher than pathophysiologic PSMA expression levels on human PCA (24). The percentage signal intensity relative to the PC-3 PIP section (set to 100%) was calculated. The images were arranged for visual display using Adobe Photoshop (version CS6; Adobe Systems, USA).
68Ga-PSMA-11 PET/MRI
The 9 patients with primary PCA with corresponding tissue analysis underwent 68Ga-PSMA-11 PET for staging of high-risk PCA between June 2016 and August 2017. For the second cohort of patients for PSMA PET image quantification, 60 consecutive patients referred for 68Ga-PSMA-11 PET for biochemical recurrence were selected. All patients underwent a clinical routine whole-body PET/MRI 60 min after injection of 68Ga-PSMA-11 using a hybrid scanner (SIGNA PET/MR; GE Healthcare) as reported previously (25). To quantify 68Ga-PSMA-11 uptake, a standardized volume of interest (VOI) was positioned in the regular tissue of the parotid, submandibular, lacrimal, and sublingual glands, as well as pancreatic, hepatic, and splenic tissue to assess the maximum and mean SUV (SUVmax and SUVmean, respectively). For patients with PSMA-positive local recurrence or metastasis, a VOI was placed over the most active lesion.
To quantify PSMA uptake on 68Ga-PSMA-11 PET images in the 9 primary tumors, VOIs were placed into the apical quadrant positive for cancer on histopathology that was selected for further ARG and IHC analysis.
Statistical Analysis
Statistical analysis was performed with SPSS 25.0.0.0 software (IBM). Descriptive statistics was used to display patient data as median, SD, or number (percentage). The average activity or intensity on IHC, ARG, and PET imaging was correlated with the values obtained for SMG, pancreas, and PCA using Pearson correlation. A P value lower than 0.05 was considered to indicate statistical significance. Linear regression was used between the signal intensity on ARG and the uptake on PSMA PET to estimate the relation between PSMA expression and tracer uptake on 68Ga-PSMA-11 PET images.
RESULTS
Patient samples for analysis of PSMA expression on SMG were isolated from 9 consecutive patients, for pancreatic tissue from 4 patients, and for PCA tissue from 9 patients with cancer in the apex. In 60 patients undergoing 68Ga-PSMA-11 PET for restaging, the activity accumulation was determined in the lacrimal, parotid, submandibular, and sublingual gland, as well as in pancreatic, splenic, and hepatic tissue and in PCA lesions (Fig. 1; Table 1). In 31 patients, 68Ga-PSMA-11–positive metastases were clearly localized. The mean uptake in the SMG was not different between patients with or without 68Ga-PSMA-11–positive lesions with an SUVmax 23.5 ± 5.2 versus 23.3 ± 5.1 (P = 0.875), respectively.
Patient Characteristics
PCA
Frozen tissue sections of the apex were analyzed in 9 patients with apical PCA confirmed on H&E staining. The area fraction covered by adenocarcinoma on the slides ranged from 3% to 33% and included Gleason scores from 3 + 3 to 4 + 4. The corresponding paraffin-embedded tissue stained with an anti-PSMA antibody indicated PSMA expression ranging from low (1+) to strong (3+), covering 70%‒100% of the tumor tissue with IRS values between 70 and 300 (Table 2).
Comparison of the 9 Primary Prostate Tumors on Histology, ARG, and PSMA PET
In analogy to the IRS score, the signal intensity on ARG images of PCA tissue relative to PC-3 PIP tumor xenograft sections showed a heterogeneous pattern with a mean signal intensity of 8.5% ± 6.8% and a range between 1.3% and 22% (Fig. 2A). The pattern of signal intensity on frozen sections corresponded well with the tumor region on H&E histology.
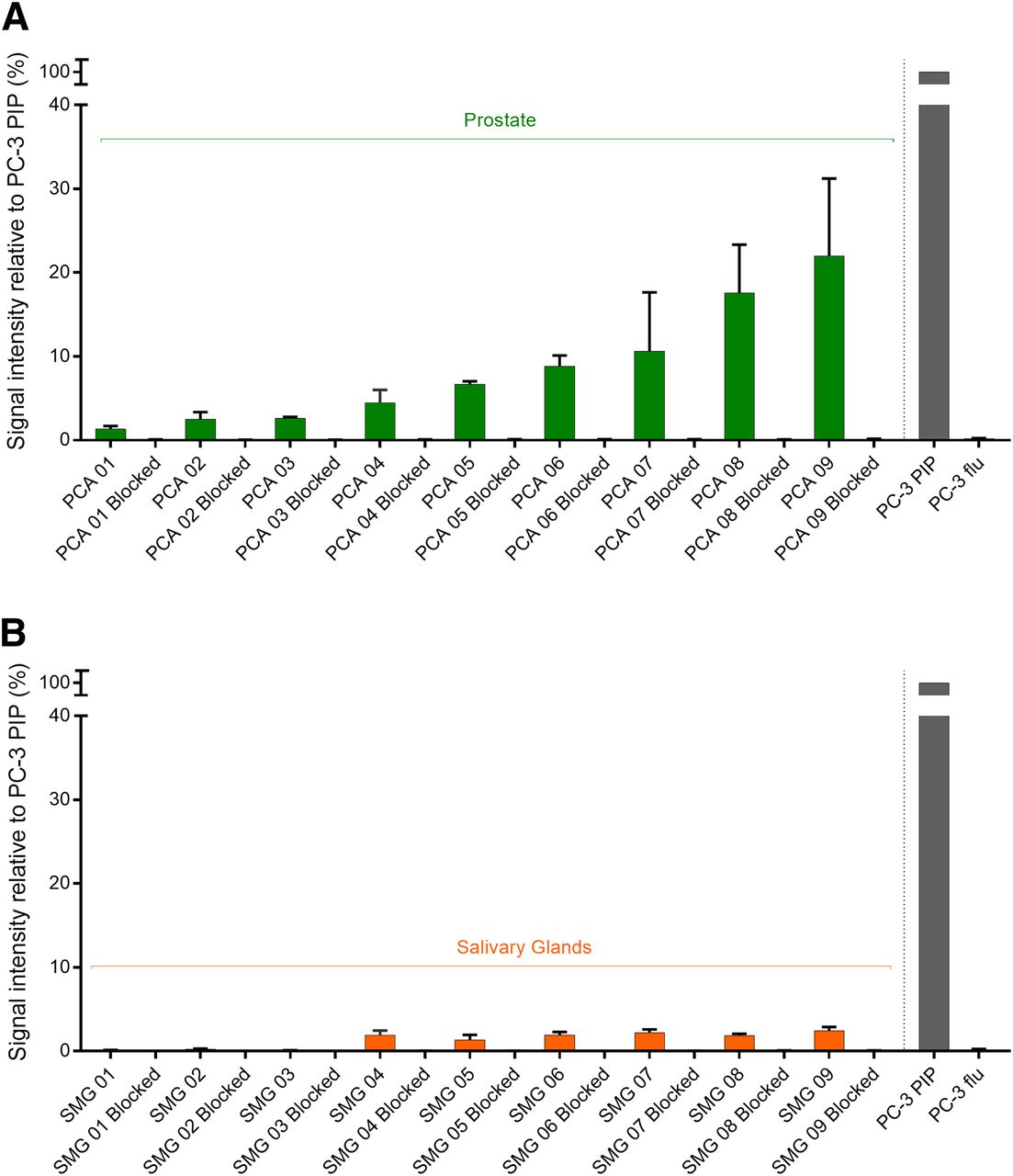
(A) ARG quantification of signal intensity of human primary PCA tissue relative to PC-3 PIP (high PSMA expression, set to 100%) and PC-3 flu (low PSMA expression) mouse tumor xenograft sections after application of 177Lu-PSMA-617. Data shown for unblocked and 2-PMPA–blocked tissue sections. Heterogeneous pattern of signal intensity on ARG was observed, with mean of 8.5% ± 6.8% and range of 1.33%–21.98%, compared with PC-3 PIP tumor tissue. (B) Same ARG quantification for human salivary gland sections. SMG 01–03 with atrophy showed only minimal signal intensity (0.14% ± 0.10%) and SMG 04–09 with normal histology showed low signal intensity (1.94% ± 0.32%).
Also, the in vivo 68Ga-PSMA-11 accumulation determined on PET scans showed a heterogeneous SUVmax ranging from 4.4 to 16.0 in the areas of the investigated primary prostate adenocarcinoma corresponding to the signal seen on ARG (Table 2; Fig. 3).
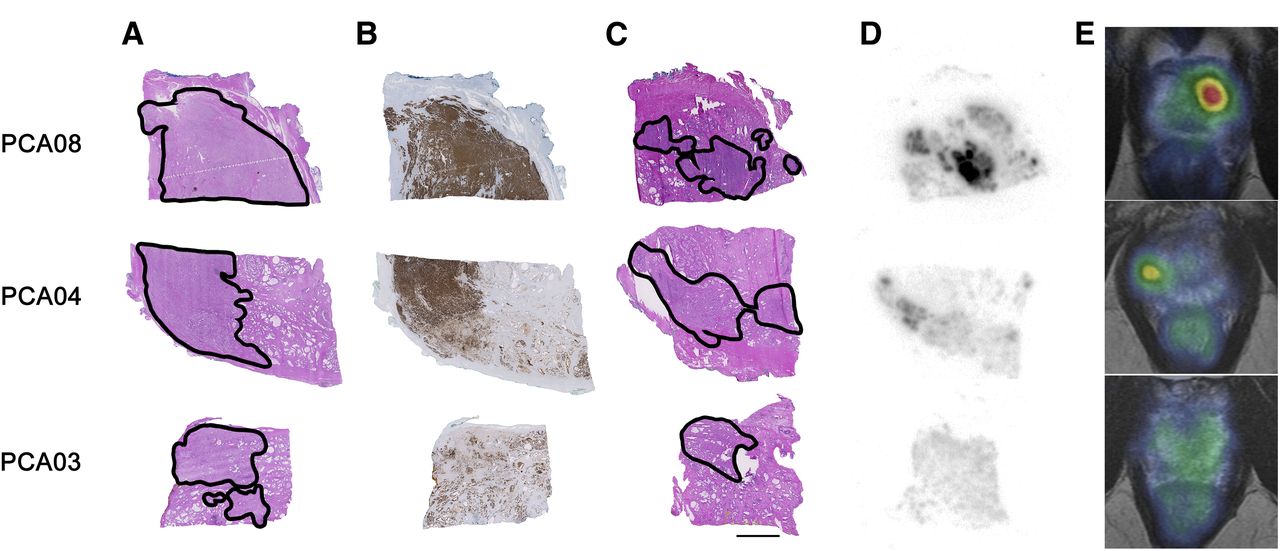
Comparison of 3 selected examples of prostate carcinomas (line by line) regarding hematoxylin & eosin (H&E) histology, PSMA IHC, in vitro ARG, and in vivo PET. Encircled carcinoma areas in formalin-fixed tissue (A), respective corresponding PSMA IHC (B), and selected encircled carcinoma areas in fresh frozen tissue (scale bar 5 mm) (C). D shows corresponding in vitro ARG with high (PCA08, GS 4 + 4), moderate (PCA04, GS 3 + 4), and low (PCA03, GS 3 + 3) normalized signal intensity on ARG, whereas E shows corresponding axial slice through apex of prostate on PSMA PET/MR. GS = Gleason score.
Pancreatic Tissue
The healthy pancreatic tissue (PANC) was negative for PSMA on IHC in all 4 cases, even in the intercalated ducts (IRS 0; Table 3). The average signal intensity of the ARG performed on the pancreatic tissue was minimal in relation to PC-3 PIP tumor xenograft sections (0.1% ± 0.05%, Supplemental Fig. 1 [supplemental materials are available at http://jnm.snmjournals.org]), as was the case for the 68Ga-PSMA-11 accumulation on 68Ga-PSMA-11 PET scans that was low as well (SUVmax of 3.1 ± 1.1) (Table 4).
Comparison of the 9 Salivary Gland and 4 Pancreatic Tissues
Quantification of 68Ga-PSMA-11 Accumulated in Different Tissues Based on PSMA PET
Salivary Glands
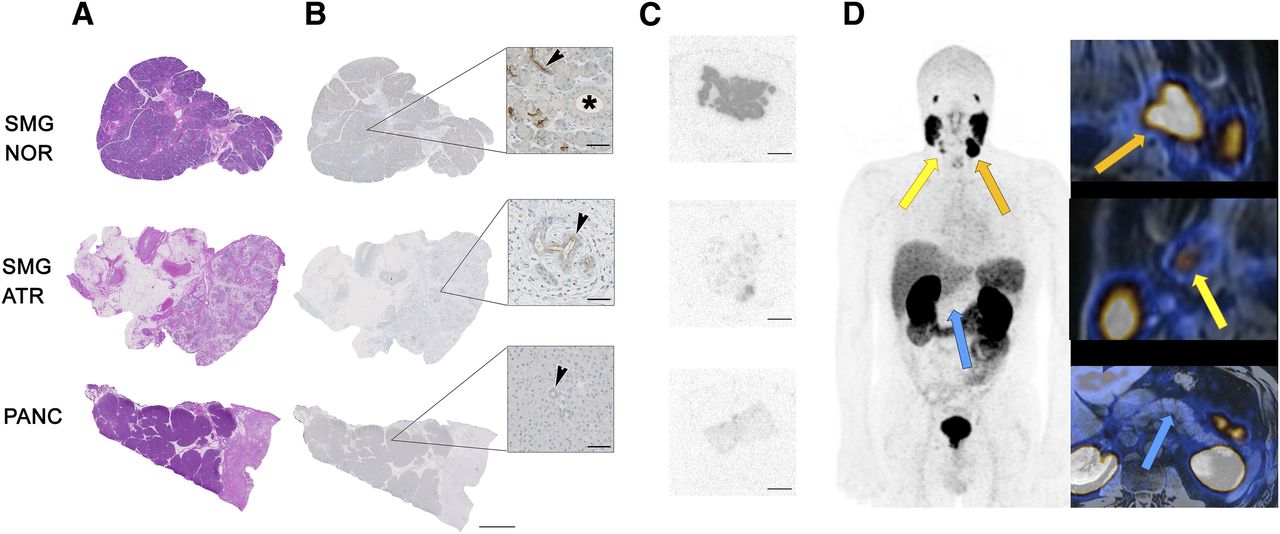
Three SMG were atrophic with signs of chronic inflammation, whereas 6 glands had a normal histology without inflammatory changes. IHC of PSMA expression showed distinct PSMA staining intensity (2 to 3+) that was limited in extent (5% of the tissue) and typically confined to the intercalated ducts of normal SMG, yielding an IRS of 10–15. Atrophic SMG showed a similar pattern, but markedly reduced staining intensity (1+), as well as decreased coverage (IRS of 2–5; Table 3; Figs. 4A and 4B). A minor, opaque and inconsistent staining of the mucinous glands was regarded as an unspecific artifact.
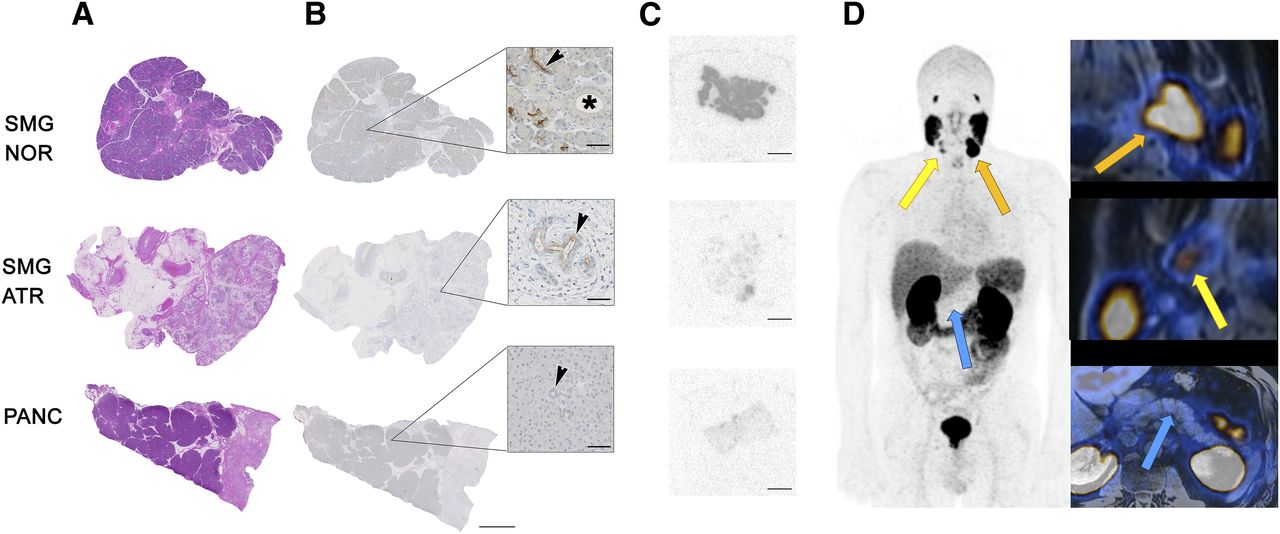
Comparison of normal and atrophic submandibular salivary gland tissue (SMG NOR and ATR), and pancreatic tissue (PANC) regarding hematoxylin & eosin (H&E) histology, PSMA IHC, and in vivo PET. (A) H&E histology of these 3 tissue types. (B) Moderate but focal PSMA expression in intercalated ducts (inset, arrow), whereas striated ducts (inset, asterisk) are PSMA-negative and intercalated ducts of atrophic salivary gland tissue show less expression. In pancreatic tissue, no PSMA expression is noted (inset, arrow shows negative intercalated duct). Scale bar 5 mm, and 100 μm (insets). (C) In vitro ARG with normalized signal intensity for normal and atrophic SMG besides normal pancreatic tissue. Scale bar 5 mm. (D) PSMA PET scan of patient showing high PSMA accumulation in left SMG (orange arrow, SUVmax 33), lower uptake in atrophic right SMG (yellow arrow, SUVmax 11), and only minimal uptake in pancreas (blue arrow, SUVmax 3) (magnification in insets).
The average relative signal intensity on ARG images of SMG was 1.34% ± 0.89%. The 3 atrophic glands showed reduced signal intensity on ARG (0.14% ± 0.1%) compared with the 6 glands with normal histology (1.94% ± 0.32%) (Fig. 2B). Given that most PCA patients do not have atrophic salivary glands, further comparison was performed by considering only the average uptake of healthy SMG (Table 3).
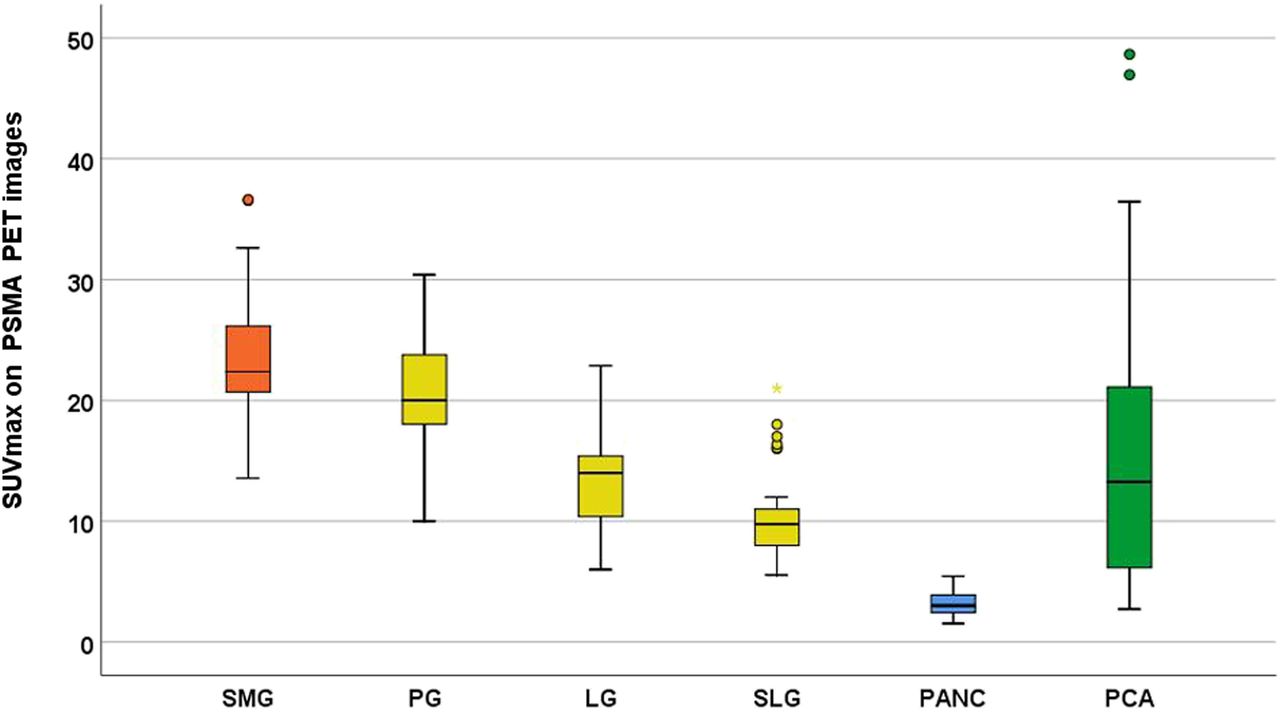
In contrast to the low IRS on IHC and the minimal signal intensity on ARG, all SMG on 68Ga-PSMA-11 PET scans revealed a strong accumulation of the tracer with a mean SUVmax of 23.5 ± 5.2 (range, 13.6–36.6) (Table 4; Fig. 5).
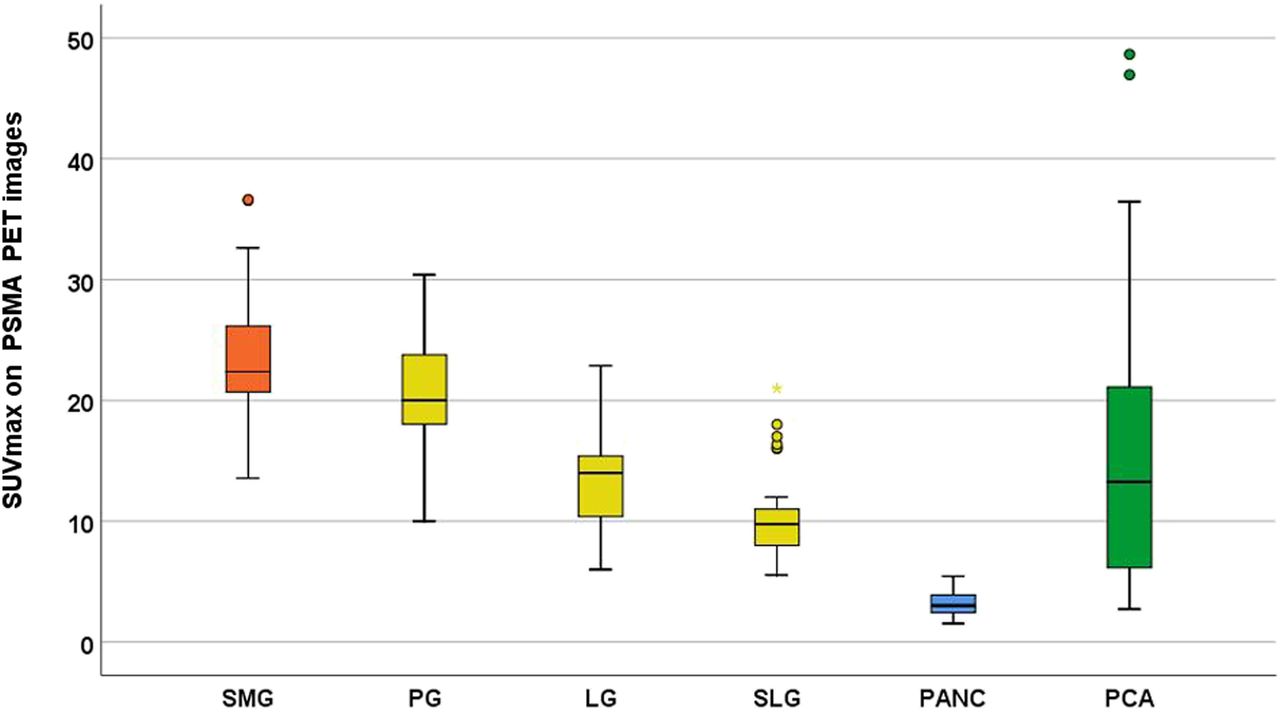
Box plots illustrating PSMA PET activity distribution for 60 consecutive patients imaged for PCA recurrence. High accumulation of 68Ga-PSMA-11 60 min after injection can be measured in salivary glands of head and neck area, with a maximum in SMGs (orange), followed by parotid gland (PG), lacrimal gland (LG), and sublingual gland (SLG). Only minimal uptake was determined in pancreatic tissue (PANC, blue). Average 68Ga-PSMA-11 uptake in SMGs was higher than uptake in PCA metastasis (PCA, green).
Correlation Between IHC, ARG, and PET
The IRS evaluated by IHC and the ARG intensity showed a significant correlation (R2 = 0.642, P = 0.009), visualizing the areas of PSMA-positive prostate adenocarcinoma. Furthermore, the ARG intensity correlated well with the accumulation of 68Ga-PSMA-11 in the apical quadrant of the prostate as determined on PET images (R2 = 0.897, P < 0.001) (Fig. 6).

Scatterplot with linear regression fit for quantification of relative signal intensity on ARG images and corresponding quantification of in vivo uptake of 68Ga-PSMA-11 on PET images (SUVmax) for PCA specimens (green, circle), with a linear regression fit (R2 = 0.897, P < 0.001, y = 1.46*× −3.9). Average ARG signal intensity for salivary glands (SMGnor, 1.94%) in relation to average SUVmax on 60 PSMA PET scans (SUVmax 23.5) is shown in orange (square) and ARG signal intensity for pancreases (PANC; 0.1%) in relation to average SUVmax on 60 PSMA PET scans (SUVmax 3.1) in blue (triangle).
In addition, SMG and pancreatic tissue displayed a significant correlation between the low IRS (mean SMG, 8.7 ± 4.9 and mean PANC, 0.0 ± 0.0) and the low ARG signal intensity (mean SMG, 1.3% ± 0.9% and mean PANC, 0.1% ± 0.1%, R2 = 0.739, P < 0.001). In vivo accumulation of 68Ga-PSMA-11 was strong in SMG, with a mean SUVmax of 23.5 ± 5.2 even surpassing the highest uptake detected in primary prostate adenocarcinoma (SUVmax 16.0 in PCA 09) (Fig. 6).
When a linear fit algorithm for ARG signal intensity and SUVmax was applied, over the 9 PCA cases, the following equation would result in (ARG %) = 1.46* (SUVmax) − 3.9. Assuming a similar perfusion between SMG tissue and PCA tissue, the same function should be applicable for ARG signal intensity and SUVmax on SMG. As a consequence, a mean 68Ga-PSMA-11 uptake of SUVmax 23.5 determined on PET scans would correspond to an average signal intensity of 30% ((1.46 × 23.5) − 3.9) on ARG images. This would, however, be a 15-fold increased value as compared with the actual signal intensity of 1.9% determined for ARG images of normal SMG in our study.
DISCUSSION
The presented data support a mainly non–PSMA-related radioligand uptake in salivary glands, in contrast to a significant correlation of PSMA mediated radioligand uptake in primary PCA. IHC analysis showed a patchy and focal PSMA expression limited to the intercalated ducts in SMG, whereas serous acinar cells and striated ducts did not show PSMA expression.
On the SMG specimens with chronic sialadenitis and atrophy, the IHC staining pattern was similar but overall less intense. These data were confirmed by ARG analysis, which showed low signal intensity on SMG tissue. The pancreatic tissue, which has a histology similar to that of the SMG, did not show any expression of PSMA on IHC and ARG, respectively. The main structural difference between pancreatic tissue and SMG are the striated ducts (26). The substantial difference of PSMA radioligand uptake between these tissues may be attributed to the striated ducts. However, this would be most likely PSMA-unrelated, as no PSMA expression is observed in the striated ducts.
The consistently high uptake of PSMA radioligands in all seromucous glands of the head and neck was also confirmed by Klein Nulent et al. with a retrospective analysis of 30 patients (27). Together with previous observations of minimal to patchy PSMA expression on IHC (2,16,28), this supports the hypothesis that the accumulation of small-molecule PSMA-targeting radioligands is largely nonspecific (19).
This could also explain why the injection of botulinum toxin into the salivary glands, which leads to a transient reduction in salivary gland function, reduces the PSMA radioligand accumulation up to 64% (29). Some clinicians suggested local cooling to reduce radioligand accumulation; however, the reduction of SUVmax by this measure was only 15%, so that further investigation is needed before consideration of clinical routine use (30). The approach of using inhibitors of PSMA (e.g., 2-PMPA) was found to be more successful in view of protecting the kidney from radiation damage (31), rather than the SMG, which was another finding supporting the hypothesis that the uptake of PSMA ligands in salivary glands is mostly PSMA-unrelated.
The sink effect in patients with high tumor burden is a phenomenon that led to a reduced radioligand accumulation in salivary glands (32); however, in the patients selected for this study referred for staging or early biochemical recurrence, the tumor burden was not high enough to affect the radioactivity uptake in the salivary glands.
A potential limitation of the present study may be that a direct comparison of the accumulation of PSMA radioligands in vivo, determined by PET examinations and in vitro using ARG of the same specimens for salivary gland and pancreatic tissue, is not possible. Given the consistent results for both pancreatic and normal SMG tissue regarding ARG and IHC, as well as the consistently high PSMA radioligand accumulation in salivary glands of the head and neck and low radioligand uptake in the pancreas, we believe that the indirect comparison as presented in this study is conclusive to confirm our hypothesis.
CONCLUSION
Our data strongly suggest that accumulation of PSMA-targeting radioligands in salivary gland tissue is mainly nonspecific. Further studies will be necessary to investigate the exact mechanism of radioligand accumulation to develop new strategies to reduce radiotracer uptake in this dose-limiting tissues. This is in particular critical for radionuclide therapy using α-particle emitters with high linear energy transfer.
DISCLOSURE
Irene A. Burger has received research grants from GE Healthcare and Swiss Life and a speaker honorarium from GE Healthcare, Bayer Health Care, and Astellas Pharma AG. The Department of Nuclear Medicine holds an institutional research contract with GE Healthcare. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is the high accumulation of PSMA-targeting radioligands in salivary glands due to a high PSMA expression?
PERTINENT FINDINGS: In this prospective study autoradiography (ARG, 117Lu-PSMA-617) and immunohistochemistry (IHC, anti–PSMA-antibody) were performed on fresh frozen tissue from submandibular glands, pancreatic tissue, and prostate cancer. The correlation between SUVmax on 68Ga-PSMA-11 PET and IHC PSMA expression and ARG signal intensity was very high (R2 = 0.897) for prostate cancer whereas submandibular glands had only very limited PSMA expression on IHC and very low ARG signal intensity but a general high uptake on 68Ga-PSMA-11 PET.
IMPLICATIONS FOR PATIENT CARE: We showed that the high accumulation of PSMA radioligands in salivary glands is not primarily a PSMA-mediated mechanism; therefore, other pathways and potential blocking methods need to be investigated to reduce the toxicity of PSMA radioligand therapy.
Acknowledgments
We thank the Sick legat and the Iten-Kohaut foundation for their financial support. We acknowledge the technicians Marlena Hofbauer, Miguel Porto, Sofia Kaltsuni, and Sabrina Epp for their work on high quality PET/MR scans. We thank Susanne Dettwiler, Fabiola Prutek, and Christiane Mittmann for tissue processing and immunohistochemical stainings.
Footnotes
Published online Feb. 8, 2019.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 13, 2018.
- Accepted for publication January 13, 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.