


Visual Abstract

Abstract
PET scans using 18F-FDG and somatostatin receptor imaging agents are both used in imaging of neuroendocrine neoplasms (NENs). We have suggested the “NETPET score,” using uptake of both PET tracers, as a prognostic biomarker in NENs. The name NETPET score was suggested previously to capture the score's intent to summarize information from dual PET imaging in neuroendocrine tumors. We previously demonstrated the effectiveness of the NETPET score in gastroenteropancreatic NENs (GEPNENs). Its prognostic relevance in bronchial NENs remains undetermined. Methods: This is a retrospective multicenter study (2011–2018) assessing patients who had advanced bronchial NEN and who underwent both 18F-FDG and 68Ga-DOTATATE PET within 60 d of each other. The NETPET score was assigned by experienced nuclear medicine physicians and compared with other clinical data such as World Health Organization grade. The primary outcome was overall survival; NETPET score and other prognostic variables were analyzed using univariate and multivariate analyses by the Cox proportional-hazards model. Results: Thirty-eight patients were included for review. The NETPET score and histology were significantly correlated with overall survival in univariate analyses (P = 0.003, P = 0.01). On multivariate analysis, only the NETPET score remained significant (P = 0.03). The NETPET score was significantly associated with histologic grade (P = 0.006, χ2 test). Conclusion: The NETPET score is a prognostic biomarker in bronchial NENs as well as GEPNENs. Although it needs to be validated in prospective studies, it holds significant promise as a biomarker for a wide range of NENs.
Neuroendocrine neoplasms (NENs) are a heterogeneous group of tumors that may secrete bioactive peptides. Although uncommon, they are increasing in incidence (1,2). They can arise in different parts of the body, most commonly in the gastrointestinal tract, pancreas, and lung. Although they vary considerably in biologic behavior, surgical resection is the only cure, and patients with high-grade metastatic NEN have a very guarded prognosis (3). Tumors in the gastrointestinal tract and pancreas are known collectively as gastroenteropancreatic NENs (GEPNENs). Bronchial NENs are often considered separately and have a different classification system from GEPNENs (4,5). Bronchial NENs have a differing genetic basis from GEPNENs and may also exhibit different clinical behavior, with a median overall survival comparable to pancreatic NENs but inferior to that of small-bowel NENs (6–8). Treatment for patients with advanced bronchial NENs tends to be extrapolated from GEPNENs because of a lack of prospective trials in this subgroup. For instance, the only systemic treatment for bronchial NENs supported by phase III trial evidence is everolimus (9), whereas such evidence exists in various GEPNENs for somatostatin analogs, everolimus, sunitinib, and peptide receptor radionuclide therapy (PRRT) (10–13).
Clinicians find it challenging to predict prognosis and select optimal systemic therapies in metastatic NEN because of the widely variant biologic aggressiveness of different NENs. Although histologic grade can predict disease behavior to some extent, grade may be inaccurately measured in small biopsies, may vary in different metastatic sites, and may also evolve over time. Tissue- and blood-based biomarkers have been suggested, but few have been validated prospectively (14). PET imaging has been increasingly used to image NENs and even to guide the optimal choice of systemic therapies. It is recognized that somatostatin receptor–based radiotracers (such as 68Ga-DOTATATE PET) highlight well-differentiated NEN cells that express the somatostatin receptor. Conversely, avidity on 18F-FDG PET as well as high metabolic tumor volume predicts aggressive tumor biology and poorer prognosis (15–18). The distribution and intensity of somatostatin receptor expression measured by 68Ga-DOTATATE PET, together with the absence of sites of discordant 18F-FDG–avid disease, also provides a theranostic role by confirming suitability for treatment with PRRT. In a similar fashion to NEN treatment, much of the data regarding PET imaging in NENs has been extrapolated from publications concerning GEPNENs.
Given the different roles of these 2 scans, we proposed a system to interpret the complementary findings of the 2 scans—the “NETPET score” (19). This name was suggested in the original study to capture the score's intent to summarize information from dual PET imaging in neuroendocrine tumors. This score was investigated in a group of predominantly GEPNEN patients, showed prognostic significance independent of histologic grade, and was subsequently validated in 2 other patient cohorts (20,21). As the prognostic impact of the NETPET score had not been formally investigated in bronchial NENs, we aimed to measure this impact in a retrospective study.
MATERIALS AND METHODS
This was a multicenter retrospective study conducted in Australia (Royal North Shore Hospital, Sydney, and Royal Brisbane and Women’s Hospital, Brisbane) and the United States (Memorial Sloan Kettering Cancer Center, New York, New York). Subjects aged 18 y or above with histologically confirmed, advanced (unresectable or metastatic) NENs originating from the lung were eligible. All NEN histologies (typical carcinoid, atypical carcinoid, large cell and small cell neuroendocrine carcinoma) were included. Other pathologies (e.g., adenocarcinoma and squamous cell carcinoma) were excluded.
Searches of each site’s nuclear medicine database were conducted. All patients fulfilling the above criteria who underwent 68Ga-DOTATATE and 18F-FDG PET imaging within 60 d of each other with no local or systemic therapy between the 2 scans were included. In the case of multiple pairs of eligible scans in the same individual, the earliest pair acquired after diagnosis of advanced disease was chosen.
Imaging
Image data were acquired on PET/CT scanners at each institution. All image data were acquired on current-generation PET/CT scanners with time-of-flight, scatter correction, and point-spread function resolution recovery (UltraHD) capabilities (Royal North Shore Hospital: Biograph mCT.S/64 PET/CT scanner [Siemens Healthcare]; Royal Brisbane and Women’s Hospital: Biograph mCT.S/128 PET/CT scanner [Siemens Healthcare]; Memorial Sloan Kettering Cancer Center: 690 or 710 PET/CT scanner [GE Healthcare]). Data were typically acquired as whole-body scans (top of skull to mid thigh), usually requiring 6–8 bed positions in step-and-shoot mode.
For the 68Ga-DOTATATE PET scans, the patients were injected with 120–200 MBq of 68Ga-DOTA-(Tyr3)-octreotate; imaging commenced approximately 45–60 min after injection, with whole-body low-dose CT followed by the PET acquisition of 120–180 s/bed position. Subjects were advised to cease somatostatin analogs 4 wk before the scan.
For the 18F-FDG scans, the patients were required to fast for at least 6 h before the scan, and blood glucose levels were checked to ensure they were within the range of 4–11 mmol/L. Subjects were administered 18F-FDG in the range of 250–450 MBq according to standard institutional protocols (Royal North Shore Hospital: 250 MBq if patient weight under 90 kg and 300 MBq if over 90 kg; Royal Brisbane and Women’s Hospital: 4.5 MBq/kg up to a maximum of 350 MBq; Memorial Sloan Kettering Cancer Center: 444 MBq [±10%]). At approximately 60 min after injection of the 18F-FDG, scanning commenced with whole-body low-dose CT followed by the PET acquisition of 120–150 s/bed position.
Image Analysis
Scans were graded subjectively by visual interpretation on dedicated nuclear medicine reporting workstations. Interpretation was undertaken by experienced nuclear medicine physicians at each site. Both scans were displayed simultaneously in transverse, coronal, and sagittal planes accompanied by a maximal-intensity projection of the PET data, with both image sets anatomically coregistered. The scans were initially windowed with preset SUVs of 0–15 for 68Ga-DOTATATE PET and 0–7 for 18F-FDG PET, as these were the values used for reporting in clinical practice. The readers had full access to all software tools in the reporting software. Positivity on 18F-FDG and 68Ga-DOTATATE scans was defined as uptake greater than that regarded as physiologic for the organ or tissue in question on the respective scan.
All readers underwent initial training with a standardized dataset of 10 NEN cases (taken from the initial NETPET study (19)) before commencing grading. According to our prior study, scoring was focused on the most discordant lesion on dual PET (Fig. 1). A score of P5 was assigned if there was significant disease that was 18F-FDG–avid but not 68Ga-DOTATATE–avid. A score of P2–P4 corresponded to the presence of 18F-FDG–avid, 68Ga-DOTATATE–avid disease in any of the lesions, with the exact score dependent on the relative avidity on 18F-FDG and 68Ga-DOTATATE PET. P1 denoted 68Ga-DOTATATE but not 18F-FDG avidity in all lesions; P0 denoted neither 68Ga-DOTATATE nor 18F-FDG avidity (Table 1).
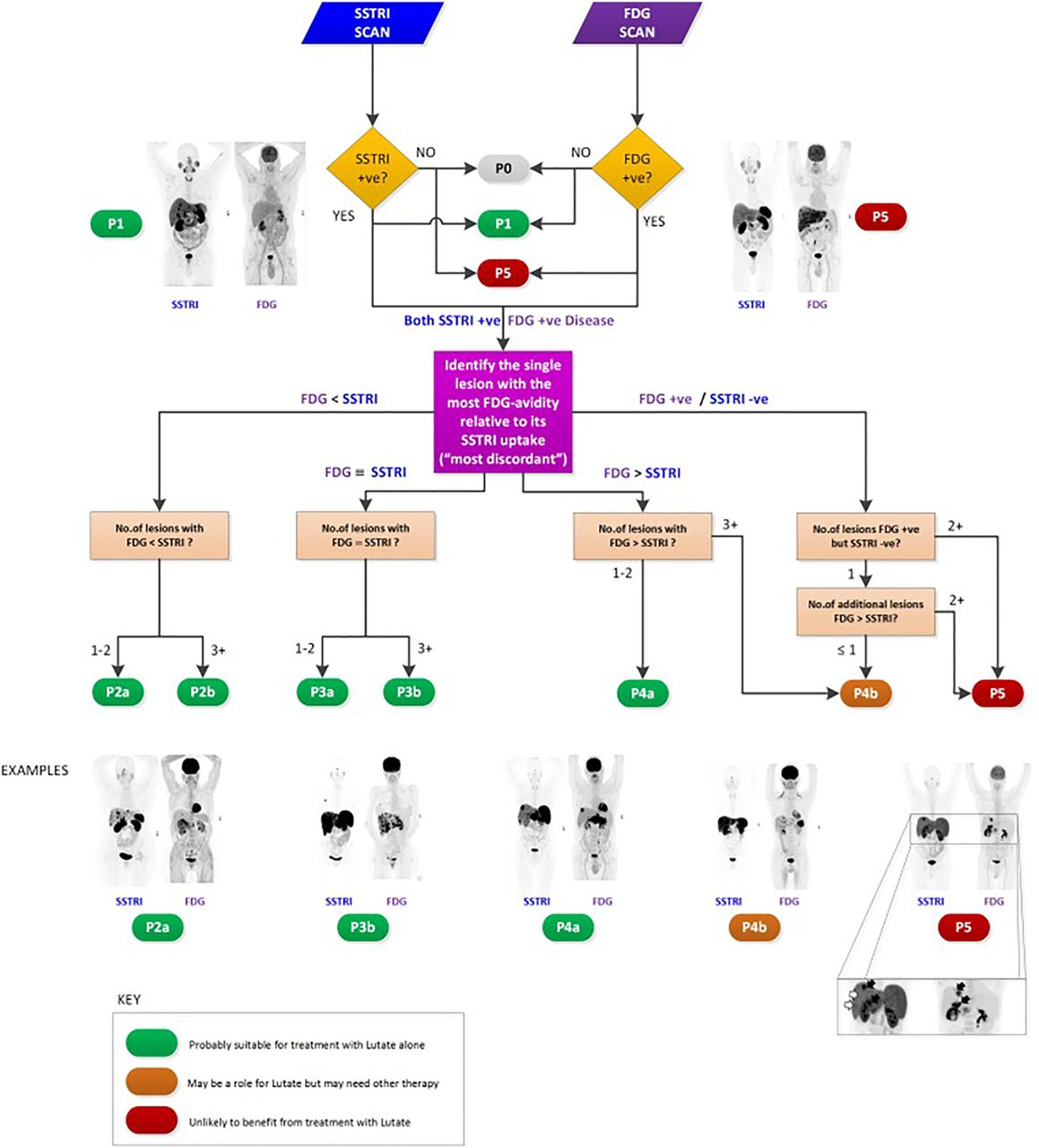
Original NETPET schema. SSTRI = somatostatin receptor imaging. (Reproduced from (19).)
Simplified Schematic of Relationship Between NETPET Score and Dual PET Avidity
Clinicopathologic Data
The included patients’ charts were reviewed to extract demographic and prognostic data (including primary site and histologic grade). Outcomes included overall survival (OS) and progression-free survival (PFS), defined as a composite of RECIST-defined radiologic progression, commencement of another systemic therapy after the index scan, and death (22). The primary outcome was OS, measured in days from the latter of the 2 paired PET scans to the date of death or last follow-up.
Statistical Analysis
Patient demographics are presented descriptively. For survival analysis, the included patients were separated into 3 cohorts—P1, P2–P4, and P5—in the same fashion as the original NETPET study (19). Patients with P2, P3, and P4 findings were grouped together as there is no consensus on the exact quantitative cutoffs to separate patients who have lesions exhibiting more 68Ga-DOTATATE than 18F-FDG avidity from those with more 18F-FDG than 68Ga-DOTATATE avidity. Patients with P0 disease were noted but excluded from this analysis (the authors considered that this was an uncommon finding from their clinical experience). Survival outcomes in the different cohorts were compared using the log-rank test. Univariate and multivariate regression was performed using the Cox proportional-hazards model with the following variables: age, presence or absence of distant extrahepatic disease, histologic grade, and NETPET score. Histologic grade was divided into 3 groups: typical carcinoid, atypical carcinoid, and large cell/small cell neuroendocrine carcinoma. Other potential prognostic markers (most pertinently the mitotic count and Ki-67 index) were not included in multivariate analysis because of the potential for introducing collinear factors into multivariate analysis. We conducted sensitivity analyses to determine the value of replacing histologic grade by the Ki-67 index for OS analyses. Finally, the correlation between NETPET score and histologic grade (as well as NETPET score and Ki-67 index) was analyzed using the χ2 test.
Ethics Approval
This study was approved by the Northern Sydney Local Health District Human Research Ethics Committee, 2019/ETH09817, and relevant local ethics committees for each participating site. The requirement to obtain informed consent for this retrospective study was waived.
RESULTS
Thirty-eight patients were included in this study from 3 sites. Female patients comprised 61% of the cohort, and the median age was 66 y (Table 2). The median time from histologic diagnosis to PET imaging was 13 mo (range, 1–151 mo). Treatments before PET imaging included SSAs (18% of patients), chemotherapy (26%), and PRRT (5%). Treatment after PET imaging included SSAs (24%), chemotherapy (45%), and PRRT (37%). The median follow-up for patients was 18.5 mo.
Demographics of Study Cohort (n = 38)
When the NETPET scoring system was applied to the included patients, more than half the patients (61%) had disease that was both 68Ga-DOTATATE–avid and 18F-FDG–avid (Table 3). The distribution of scores did not significantly differ among the participating institutions (χ2 test, P = 0.27). Eight percent of patients had a NETPET score of P1 (denoting purely 68Ga-DOTATATE–avid disease), and 26% of patients had a score of 5, denoting the presence of significant 18F-FDG–avid, 68Ga-DOTATATE–negative discordant disease. Two patients (5%) had disease that was scored as P0 (i.e., all lesions were negative on both 68Ga-DOTATATE and 18F-FDG PET). In all, 16 of the 38 included patients (42%) underwent PRRT at some point of their disease journey (14/16 after the dual PET scans). These patients had NETPET scoring as follows: P1, 1/16 (6%); P2–P4, 13/16 (81%); and P5, 2/16 (13%).
Distribution of NETPET Scores
OS
Death had occurred in 10 of the 38 patients (26%) at the time of censoring. The median OS was not reached but was estimated at 53 mo. An increasing NETPET score was associated with poorer median OS (P1, not reached; P2–P4, 49.1 mo; P5, 14.5 mo [P = 0.003, log-rank test]) (Fig. 2). On univariate analysis, OS was associated with NETPET score (P = 0.003) and histology (P = 0.01). On multivariate analysis, only NETPET score remained significant as a prognostic factor (P = 0.03), with histology no longer significant (P = 0.39) (Table 4).
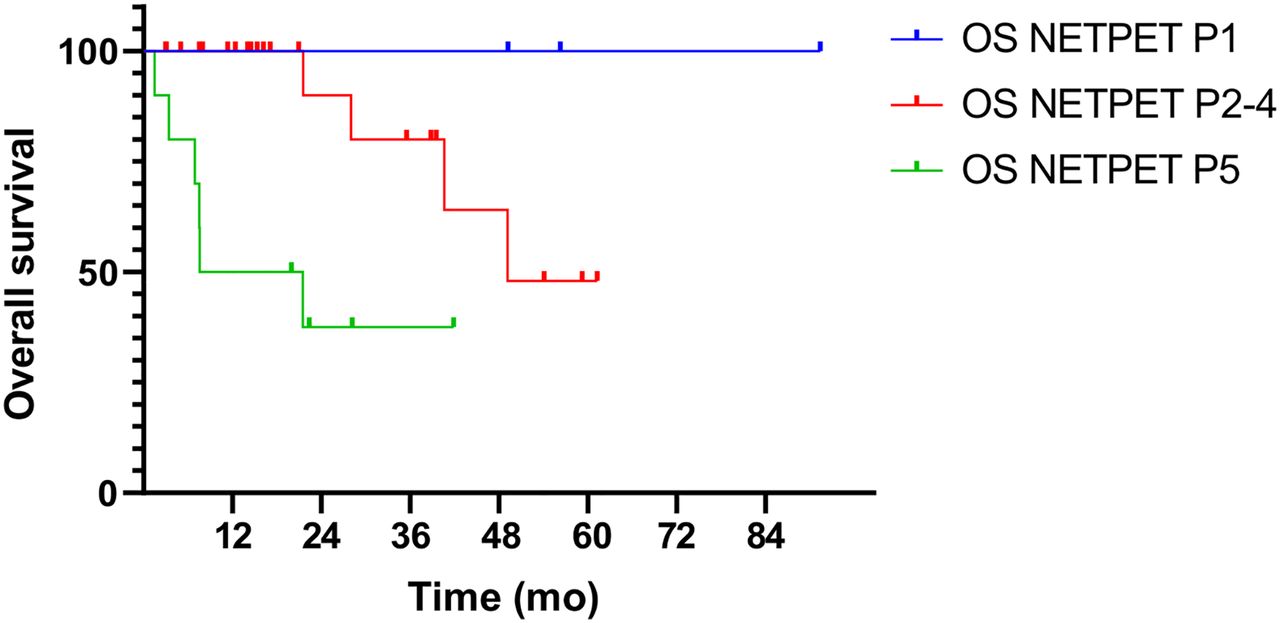
OS by NETPET score.
Univariate and Multivariate Analyses for OS
PFS
Of the included patients, 29 of 38 (76%) had progressed at the time of censoring, with a median PFS of 12.9 mo. Median PFS was not reached in patients grouped as P1. In those grouped as P2–P4, it was 14.1 mo, and in those grouped as P5, it was 4.8 mo (P < 0.0001, log-rank test) (Fig. 3).
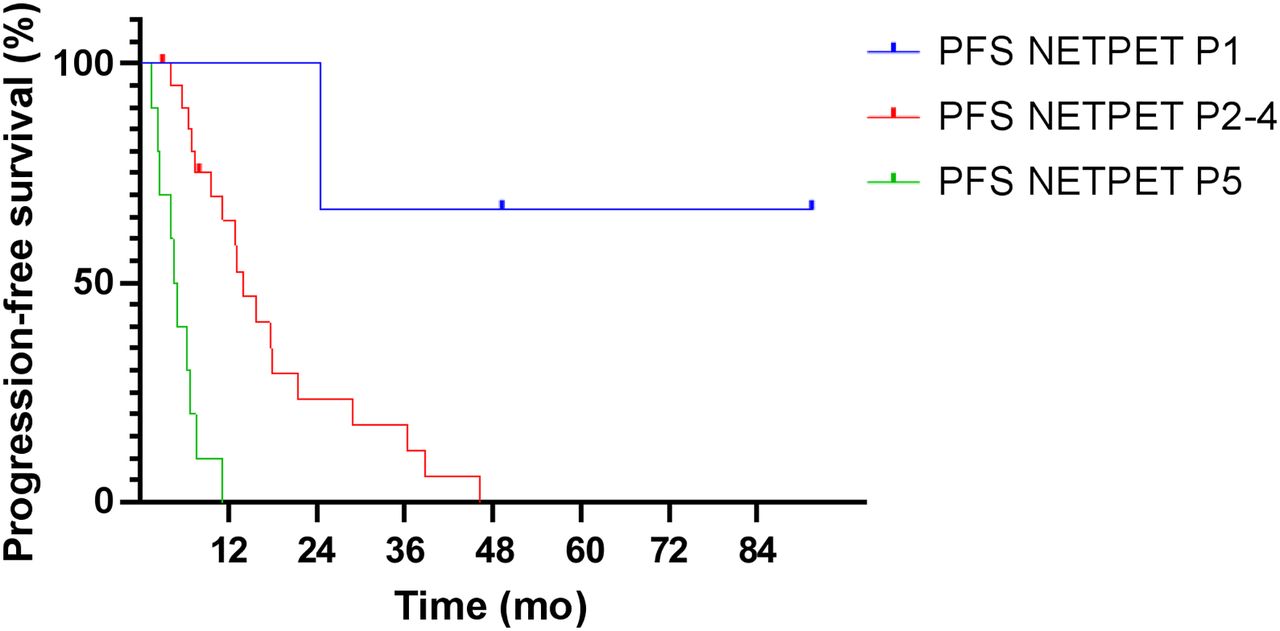
PFS by NETPET score.
On univariate analysis, PFS was significantly associated with NETPET score (P < 0.00001) and histologic grade (P = 0.04) but not age (P = 0.88) or the presence of extrahepatic disease (P = 0.68). On multivariate analysis, only NETPET score remained a significant predictor of PFS (P < 0.00001) (Table 5). Finally, NETPET score was significantly associated with histologic grade (P = 0.006, χ2 test).
Univariate and Multivariate Analyses for PFS
Sensitivity Analyses
We performed sensitivity analyses to investigate the impact of substituting histologic grade with Ki-67 index. On univariate analysis, Ki-67 index was also associated with OS (P = 0.004, log-rank test). This association remained significant on multivariate analysis (P = 0.034). The NETPET classification was not significantly associated with OS after adjustment for Ki-67 index (P = 0.08). Finally, the NETPET score was associated with the Ki-67 index (P = 0.01 by ANOVA).
DISCUSSION
The current project and indeed the NETPET score proposal arose from the hypothesis that 68Ga-DOTATATE and 18F-FDG PET provide complementary information about tumor biology. 68Ga-DOTATATE assesses the presence and extent of somatostatin receptors, whereas 18F-FDG uptake reflects glucose metabolism, with avidity typically highest in more aggressive and less well differentiated tumors. The NETPET score divides patients into 3 main groups: those who only had 68Ga-DOTATATE avidity on dual PET (favorable), those with 18F-FDG–avid, 68Ga-DOTATATE–negative discordant disease (unfavorable), and those with at least one 18F-FDG–avid, 68Ga-DOTATATE–avid lesion on dual PET without any discordance (intermediate). This NETPET score was a significant prognostic biomarker in the original study, which mainly investigated GEPNENs (19). This multicenter study demonstrated that the NETPET scoring system has a similar prognostic ability in bronchial NENs.
In the current study, we extended the findings of the original study of NETPET score to patients with bronchial NENs. Previously suggested factors such as histologic grade, age, and presence or absence of extrahepatic disease had less prognostic value in the current study. Although histologic grade and the NETPET score were associated with OS and PFS in univariate analyses, the NETPET score was the only predictor for both OS and PFS in multivariate analyses. The fact that histologic grade is a recognized predictor of outcome further highlights the potential of the NETPET score (23). The lack of OS difference between typical and atypical carcinoids in the current study (compared with the cited reference) may be due to the smaller size of our cohort. However, this lack of difference only serves to show the ability of the NETPET score to reflect the most aggressive lesion on dual PET, particularly relevant in the presence of metastatic heterogeneity. In contrast, histology samples only one unselected site of known disease and is also affected by sample size (needle biopsies may underestimate grade because of the paucity of tumor tissue). These data support a potential role for dual PET in addition to biopsy to determine tumor aggressiveness and optimal therapy in a patient with bronchial NEN. In addition, as PET is a noninvasive modality, the NETPET score may also highlight changes in disease biology over time without the risks incurred with repeated tissue biopsies.
To our knowledge, our findings confirm the prognostic value of the NETPET score in bronchial NENs for the first time, extending the findings from previous GEPNEN studies (20,21). Although a similar analysis in bronchial NENs has recently been published and demonstrated a significant proportion of patients with discordant lesions, a different scoring system was used, and the impact of dual PET scoring on OS was not reported (24). This study suggests that patients with no avidity on PET with either tracer (analogous to P0) and patients with significant disease that is 18F-FDG–avid but not 68Ga-DOTATATE–avid (analogous to P5) should not receive PRRT, as is concordant with our clinical experience. Further investigations into a molecular imaging–led paradigm for treatment selection may impact care for patients with bronchial NEN (e.g., a score of P1 leading to the use of somatostatin analogs, and a score of P5 arguing more for the use of systemic chemotherapy).
We acknowledge limitations in the current study. The relatively small numbers in this study reflect the uncommon nature of bronchial NENs. As such, the study should be regarded as hypothesis-generating at this point while awaiting additional confirmatory data. Because dual PET for bronchial NENs is not routinely practiced (because of the paucity of data regarding its utility to date), there is also a possibility of selection bias, as clinicians may order both PET examinations for patients with more aggressive disease, as reflected in the high proportion of patients with atypical carcinoids rather than typical carcinoids. This bias may also explain the relatively small number of patients with P1 grading. The retrospective nature of this study meant that the PET scans were not performed on the same day, raising the possibility that there may have been changes in tumor size or characteristics between the time of the 2 PET scans. We restricted inclusion to patients whose scans were done within 60 d of each other to minimize this potential issue. The current findings (particularly the interplay between Ki-67, NETPET score, and prognosis) should ideally be confirmed by a prospective study. Finally, we note that we included bronchial NENs of all histologies (from typical carcinoid to small cell neuroendocrine carcinoma), as opposed to a recent study that enrolled only patients with typical and atypical carcinoid (24). This inclusion allowed us to demonstrate the value of dual PET imaging and its correlation to high-grade histologies; our results remained significant for NETPET score alone on restriction of the cohort to typical and atypical carcinoid histologies (data not shown).
Future research from this study might include investigation of dual PET as a predictive biomarker for PRRT (i.e., one that predicts for differential efficacy from PRRT as opposed to just predicting for poorer prognosis per se). However, ideally this needs to be done in the context of a prospective clinical trial. The best systemic therapy for each NETPET score and the relative importance of this compared with histologic grade need to be determined. The current study treats the P2–P4 group (patients with lesions that are both 68Ga-DOTATATE–avid and 18F-FDG–avid) as a single group, meaning that subtle differences in relative 68Ga-DOTATATE and 18F-FDG avidity have not been shown to be of significance to date; the P2/P3/P4 classes may be refined into separate prognostic subgroups with larger studies and quantitative evaluation of 68Ga-DOTATATE and 18F-FDG metrics. Further research may show a link between different dual PET imaging phenotypes and molecular changes in bronchial NENs (25). Finally, the etiology and significance of disease that is nonavid on both 68Ga-DOTATATE and 18F-FDG PET remain to be determined (24).
This study also raises some intriguing possibilities for further preclinical investigation. Relatively little is known about the interplay between the molecular bases of NENs and PET findings. Recent studies investigating gene expression profiles of bronchial NENs have implicated multiple abnormalities involving the NF-KB (nuclear factor-κB) and ERK/MAPK (extracellular-signal-regulated kinase/mitogen-activated protein kinase) pathways and also demonstrated significant differences between small cell lung cancer and typical or atypical carcinoids (26,27). The upregulation of these pathways may lead to metabolic reprogramming in favor of increased glycolytic rates and more aggressive behavior. Further understanding of these molecular pathways may shed light on the dual PET findings observed in the current study and also lead to the development of new imaging tracers to better define disease biology.
CONCLUSION
Dual PET divides patients into 4 groups: purely 68Ga-DOTATATE–avid disease (P1); dual 68Ga-DOTATATE and 18F-FDG avidity (P2–P4); 18F-FDG–avid, 68Ga-DOTATATE–negative disease (P5); and dual negative disease (P0). The NETPET score predicts OS in patients with metastatic bronchial NEN, even after adjustment for known prognostic variables such as histologic grade. If confirmed by prospective studies, this finding would confirm the role of the NETPET score as a prognostic biomarker above that of histologic grade alone in predicting disease aggressiveness and guiding best care.
DISCLOSURE
David Chan has received a National Health and Medical Research Council investigator grant to fund this research in part (APP1175788). Dale Bailey is supported in part by Sydney Vital, which receives its funding from a Translational Cancer Research Centre program grant from the Cancer Institute of New South Wales. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the prognostic significance of the proposed NETPET scoring system for dual 18F-FDG and 68Ga-DOTATATE PET imaging in patients with metastatic bronchial NEN?
PERTINENT FINDINGS: In a multicenter retrospective study of 38 patients, increasing NETPET score (signifying 18F-FDG avidity and loss of 68Ga-DOTATATE avidity) was associated with worsened OS on univariate and multivariate analysis.
IMPLICATIONS FOR PATIENT CARE: The NETPET score holds significant promise as a biomarker in patients with advanced bronchial NENs.
Acknowledgments
We acknowledge Dr. Elizabeth Bernard (Royal North Shore Hospital) for her assistance in image analysis.
Footnotes
Published online February 12, 2021.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 18, 2020.
- Revision received January 3, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.