


Visual Abstract

Abstract
The objective of this retrospective study was to determine the role of 18F-FDG PET/CT in a large cohort of 495 patients with metastatic neuroendocrine neoplasms (NENs) who were treated with peptide receptor radionuclide therapy (PRRT) with a long-term follow-up. Methods: The 495 patients were treated with 177Lu- or 90Y-DOTATOC/DOTATATE PRRT between February 2002 and July 2018. All subjects received both 68Ga-DOTATOC/TATE/NOC and 18F-FDG PET/CT before treatment and were followed 3–189 mo. Kaplan–Meier analysis, log-rank testing (Mantel–Cox), and Cox regression analysis were performed for overall survival (OS) and progression-free survival (PFS). Results: One hundred ninety-nine patients (40.2%) presented with pancreatic NENs, 49 with cancer of unknown primary, and 139 with midgut NENs, whereas the primary tumor was present in the rectum in 20, in the lung in 38, in the stomach in 8, and in other locations in 42. 18F-FDG PET/CT was positive in 382 (77.2%) patients and negative in 113 (22.8%) before PRRT, whereas 100% were 68Ga-DOTATOC/TATE/NOC–positive. For all patients, the median PFS and OS, defined from the start of PRRT, were 19.6 mo and 58.7 mo, respectively. Positive 18F-FDG results predicted shorter PFS (18.5 mo vs. 24.1 mo; P = 0.0015) and OS (53.2 mo vs. 83.1 mo; P < 0.001) than negative 18F-FDG results. Among the cases of pancreatic NENs, the median OS was 52.8 mo in 18F-FDG–positive subjects and 114.3 mo in 18F-FDG–negative subjects (P = 0.0006). For all patients positive for 18F-FDG uptake, and a ratio of more than 2 for the highest SUVmax on 68Ga-somatostatin receptor (SSTR) PET to the most 18F-FDG–avid tumor lesions, the median OS was 53.0 mo, compared with 43.4 mo in those patients with a ratio of less than 2 (P = 0.030). For patients with no 18F-FDG uptake (complete mismatch imaging pattern), the median OS was 108.3 mo versus 76.9 mo for an SUVmax of more than 15.0 and an SUVmax of 15.0 or less on 68Ga-SSTR PET/CT, respectively. Conclusion: The presence of positive lesions on 18F-FDG PET is an independent prognostic factor in patients with NENs treated with PRRT. Metabolic imaging with 18F-FDG PET/CT complements the molecular imaging aspect of 68Ga-SSTR PET/CT for the prognosis of survival after PRRT. High SSTR expression combined with negative 18F-FDG PET/CT results is associated with the most favorable long-term prognosis.
Neuroendocrine neoplasms (NENs) are a heterogeneous group of neoplasms and typically have a wide range of cellular differentiation with variable biologic aggressiveness and clinical outcome (1). The clinical course of NENs can be quite heterogeneous, with a variable response to the same treatment despite similar tumor characteristics. In principle, the choice of therapy depends on individual tumor characteristics and ranges from complete eradication to a watch-and-wait approach (2–4). NENs, especially those of the pancreas and intestine, are frequently identified at a late stage at which there is advanced metastatic disease.
Most well-differentiated NENs are characterized by a high level of expression of the somatostatin receptors (SSTRs), allowing the use of radiolabeled somatostatin analogs for SSTR-targeted imaging (i.e., 111In-octreotide scintigraphy or 68Ga-SSTR PET) as well as peptide receptor radionuclide therapy (PRRT) using 177Lu- or 90Y-labeled somatostatin analogs (DOTATATE or DOTATOC). PRRT has been established as an efficient and well-tolerated treatment for patients with unresectable or metastatic progressive well-differentiated SSTR-positive neuroendocrine tumors (5) and is shown to be highly efficacious in terms of progression-free survival (PFS) and response rates compared with other treatment modalities (6–8). Quality of life is also significantly improved after PRRT (7,9,10). The significant benefit of PRRT over cold somatostatin analog therapy demonstrated by the landmark randomized phase III clinical trial (NETTER-1) (7) led to the approval of 177Lu-DOTATATE (Lutathera; Advanced Accelerator Applications) by both the European Medicines Agency and the U.S. Food and Drug Administration for the treatment of gastroenteropancreatic neuroendocrine tumors.
With the growing importance of PRRT in treating NENs, the relevant outcome predictors are becoming increasingly significant to optimize the application of PRRT. Several prognostic factors of NENs after PRRT have been described, including gene cluster expression (11), site of the primary tumor (12,13), presence of metastases (13), resection of the primary tumor (14), grade of differentiation (13,15–17), proliferation index (Ki-67 index) (13,18–20), serum biomarkers (18,21), presence of SSTRs (22,23), tumor stage (24), and treatment modality (18,25,26). However, several of these factors are difficult to assess, especially in the setting of multifocal metastatic disease. One such example is the most commonly used proliferation index, Ki-67. The histopathology of a certain small part of the tumor from biopsy or resected specimens may not be representative of the entire tumor burden; therefore, whole-body noninvasive alternatives may offer significant advantages (27).
SSTR imaging (PET or scintigraphy) represents an estimation of the SSTR status for planning of PRRT and for evaluation of response to the treatment. 18F-FDG PET/CT is used to assess glycolytic metabolism, characterized by the potential for malignancy. SSTR imaging seems like a promising alternative to repeated tissue sampling for the determination of the aggressiveness of tumors, since the results have been found to be associated with tumor aggressiveness and are highly prognostic in a variety of tumors (28–31). The diagnostic value of 18F-FDG PET in lower-grade (1, II, and IIIa) NENs is limited since they represent the slowly proliferating tumors with lower glycolytic activity. 18F-FDG PET/CT or PET/MRI is not used for diagnosis of NENs and currently is not a routine diagnostic for NENs before PRRT.
The aim of our study was to evaluate the role of baseline 18F-FDG PET/CT in predicting the PFS and overall survival (OS) of a large cohort of patients with metastatic NENs treated with PRRT with a long-term follow-up.
MATERIALS AND METHODS
Patients
From February 2002 to July 2018, a retrospective data analysis was performed for a total of 495 patients with advanced NENs who received PRRT at Zentralklinik Bad Berka and underwent PET/CT imaging with both 68Ga-SSTR and 18F-FDG at baseline before therapy. Patients with histopathologically confirmed metastatic NENs and a high level of SSTR expression, that is, tumor uptake greater than or equal to normal liver parenchyma uptake on 68Ga-SSTR PET imaging, were included. Disease progression was documented within 3–6 mo before the start of PRRT. The study was approved by the institutional review board, and written informed consent was obtained from each patient. The baseline demographics of the patients are shown in Table 1.
Demographics of Patients with NENs (n = 495)
PRRT Regimen
The DOTA-conjugated somatostatin analogs DOTATOC, DOTANOC, and DOTATATE were labeled with 68Ga for SSTR PET imaging and either 177Lu or 90Y for PRRT, in accordance with good-manufacturing-practice regulations. PRRT regimens conformed with the published practical guidelines for PRRT (32). The labeling of DOTA-conjugated peptides with 177Lu and 90Y was performed according to a previously published method (16,33). High-performance liquid chromatography was used for quality control. Radiochemical purity was always higher than 98%. An in-house–produced amino acid infusion (1,600 mL of 5% lysine HCl and 10% l-arginine HCl) was administered for nephroprotection during each PRRT cycle (34). Additional nephroprotection using an intravenous infusion of 4% Gelofusine (B. Braun Melsungen AG) adjusted to patients’ weight (infusion as a bolus of 1 mL/kg of body weight over 10 min before therapy and followed by 0.02 mL/kg/min over 3 h after radiopeptide infusion) was applied in cases of impaired renal function (glomerular filtration rate < 60 mL/min) and in patients treated with 90Y (16,32). The infusion was started at least 30 min before administration of the radiopharmaceutical and lasted for 4 h afterward. The radiopharmaceutical was coadministered over 10–15 min using a second infusion pump system. The administrated radioactivity was individually calculated on the basis of the Bad Berka Score (8,16,34).
Response Assessment
The treatment response was evaluated on CT or MRI according to RECIST 1.1 (35) and by PET imaging according to the criteria of the European Organization for Research and Treatment of Cancer (36,37). Imaging was performed before each PRRT cycle and at restaging. Restaging was performed every 3–4 mo after PRRT, and every 6 mo for stable disease or remission (complete or partial) after initial follow-up, until disease progression. PRRT was resumed if progression occurred after a therapy interval of more than 6 mo (the so-called next treatment phase of PRRT) (10,16). A decision on whether to use a salvage approach considering PRRT after progression was made by internal or external tumor boards. SSTR PET/CT and 18F-FDG PET/CT (until January 2014 with Biograph and since then with Biograph mCT Flow 64; Siemens Medical Solutions) was performed in all cases 45–90 min after the intravenous injection of 46–260 MBq of 68Ga-DOTANOC, 68Ga-DOTATOC, or 68Ga-DOTATATE and 45–90 min after the intravenous injection of 350–600 MBq of 18F-FDG, respectively. PET/CT images were acquired from the skull to the middle part of the thigh. Contrast-enhanced CT (spiral CT using a Biograph mCT Flow 64) was acquired after the intravenous administration of 60–100 mL of nonionic iodinated contrast agent. SUVmax was obtained by drawing circular regions of interest (ROIs), which were automatically adapted (40% isocontour) to a 3-dimensional volume of interest using commercial software provided by the vendor. Images were evaluated by 2 experienced nuclear medicine specialists. MRI was performed in selected cases (allergy to iodinated contrast agent or poor detectability of liver metastases on CT), and routine sonography was performed for additional diagnostic evaluation.
Data Analysis
Data were collected in the following categories: patient characteristics, tumor characteristics, prior treatments, baseline 68Ga-SSTR PET/CT results, baseline 18F-FDG PET/CT results, PRRT radionuclide, PRRT cycle, cumulative activity, all completed 68Ga-SSTR and 18F-FDG PET/CT results, and follow-up. Progression was determined on the basis of RECIST or the criteria of the European Organization for Research and Treatment of Cancer. The categories of tumor uptake and tumor burden on 68Ga-SSTR and 18F-FDG PET/CT are listed in Table 2.
Baseline 68Ga-SSTR and 18F-FDG PET Imaging of Patients with NENs
Statistical Analysis
The primary and secondary endpoints of this study were the duration of OS and PFS, respectively, defined from the start of PRRT. Survival curves for PFS and OS were estimated by Kaplan–Meier analysis, and significance was tested by the log-rank test. Univariate analysis was conducted for each prognostic factor using the log-rank test. Multivariate analysis (Cox proportional-hazards model) was performed to estimate hazard ratios (HRs) and 95% confidence intervals (95% CIs) for the potential prognostic factors. Quantitative data were denoted as mean ± SD. The statistical analysis was 2-tailed and conducted by SPSS software (IBM). A P value of less than 0.05 was considered statistically significant.
RESULTS
Patient Characteristics
The characteristics of the 495 patients (299 men, 196 women; median age at first treatment, 59.0 ± 10.7 y; range, 19–80 y) are shown in Tables 1 and 2. Primary tumors were localized in the pancreas in 199 (40.2%) patients, midgut in 139 (28.1%), lung in 38 (7.7%), rectum in 20 (4.0%), stomach in 8 (1.6%), and other locations in 42 (8.5%); 49 (9.9%) patients had cancer of unknown primary. Most patients (117 and 245, respectively) had well-differentiated NENs of grade 1 (23.6%) or grade 2 (49.5%). At baseline, 382 patients (77.2%) were 18F-FDG–positive, and 113 (22.8%) were 18F-FDG–negative. The number of treatment cycles and the cumulative administered radioactivity are listed in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org). Four hundred fifteen (83.8%) patients received dual PRRT, that is, a combination of 177Lu and 90Y; 60 (12.1%) received 177Lu as monotherapy, and 20 (4.0%) received 90Y as monotherapy. The mean cumulative administered radioactivity for all patients was 25.7 ± 10.8 GBq (range, 3.9–60.7 GBq).
Univariate and Multivariate Analysis for OS and PFS
The results of univariate and multivariate analysis of possible prognostic factors for OS and PFS are listed in Tables 3–6. Over a median follow-up of 94 mo for all patients (range, 3–189 mo), 319 patients (64.4%) died and 136 patients (27.5%) progressed. The median OS and PFS of the entire cohort were 58.7 mo (95% CI, 52.8–64.6) and 19.6 mo (95% CI, 17.6–21.7), respectively (Fig. 1).
Univariate and Multivariate Analyses of Potential Factors Contributing to OS, Part 1
Univariate and Multivariate Analyses of Potential Factors Contributing to OS, Part 2
Univariate and Multivariate Analyses of Potential Factors Contributing to PFS, Part 1
Univariate and Multivariate Analyses of Potential Factors Contributing to PFS, Part 2

Kaplan–Meier curves of OS and PFS for all patients (n = 495). (A) Median OS was 58.7 mo (95% CI, 52.8–64.6). (B) Median PFS was 19.6 mo (95% CI, 17.6–21.7).
Tumor grading was an independent predictor for both OS (P = 0.012) and PFS (P = 0.039). A higher tumor grade was associated with worse prognosis. The median OS in grades 1, 2, and 3 was 78.5 mo (95% CI, 66.2–90.8), 55.4 mo (95% CI, 46.9–63.9), and 33.2 mo (95% CI, 18.8–47.6), respectively. When compared with grade 1, grade 2 had a 1.4-fold increase in the risk of death (95% CI, 1.0–2.0; P, 0.038), whereas grade 3 was associated with a 2.5-fold increase (95% CI, 1.3–4.5; P = 0.004). The median PFS in grades 1, 2, and 3 was 23.0 mo (95% CI, 15.9–30.2), 18.9 mo (95% CI, 15.2–22.6), and 7.5 mo (95% CI, 0.0–20.1), respectively. When compared with grade 1, grade 2 tumors had a 1.2-fold increase in the risk of progression (95% CI, 0.9–1.5; P = 0.150), whereas G3 was associated with a 2.1-fold increased risk of progression (95% CI, 1.3–3.4; P = 0.003).
Primary tumor site was an independent predictor of OS (P = 0.004). The median OS of patients with pancreas, midgut, and lung NENs was 54.4 mo (95% CI, 49.3–59.6), 77.8 mo (95% CI, 61.0–94.6), and 46.2 mo (95% CI, 34.1–58.3), respectively. The median PFS was 25.8 mo (95% CI, 21.8–29.8), 22.6 mo (95% CI, 17.2–28.0), and 10.6 mo (95% CI, 5.0–16.1), respectively.
18F-FDG Uptake Status Related to Survival
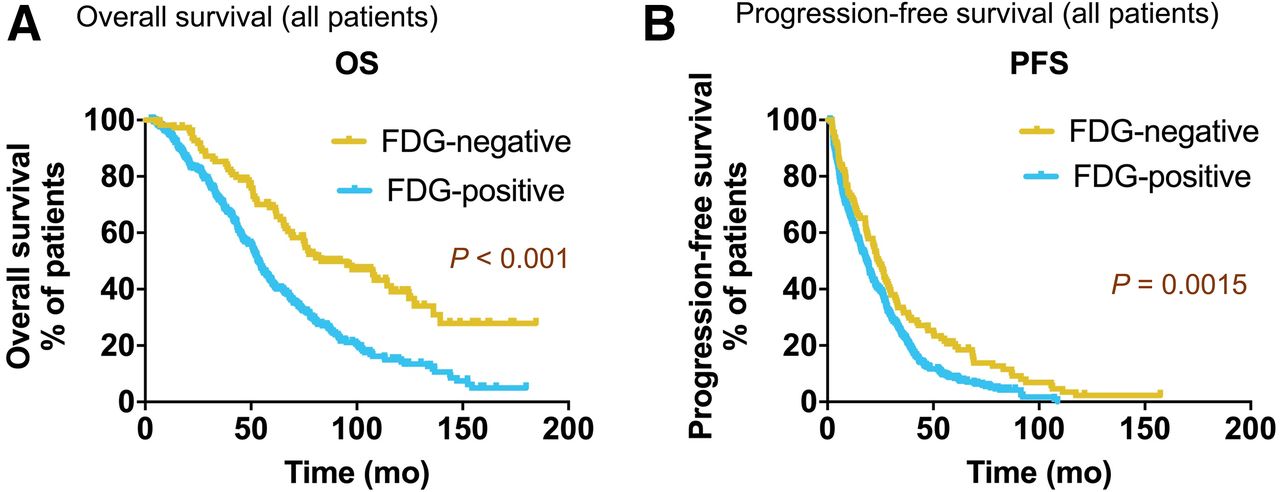
In all patients, median OS and PFS were significantly higher in the 18F-FDG–negative group than in the 18F-FDG–positive group. The benefit in OS was 83.1 mo (95% CI, 57.0–109.2) versus 53.2 mo (95% CI, 49.4–57.0; P < 0.001), respectively, and in PFS, 24.1 (95% CI, 19.9–28.3) versus 18.5 mo (95% CI, 15.9–21.1; P < 0.002), respectively (Fig. 2). 18F-FDG–negative status was an independent prognostic factor for OS, with a 0.5-fold decrease in the risk of death (HR, 0.5; 95% CI, 0.3–0.8; P = 0.002), as well as for PFS, with a 0.7-fold decrease in the risk of progression (HR, 0.7; 95% CI, 0.5–0.9; P = 0.007). 18F-FDG–positive lymph node and liver tumor burden was an independent predictor for OS (P = 0.035 and P = 0.034, respectively), whereas 18F-FDG–avid bone tumor burden (metastases) was an independent predictor for PFS (P = 0.001).
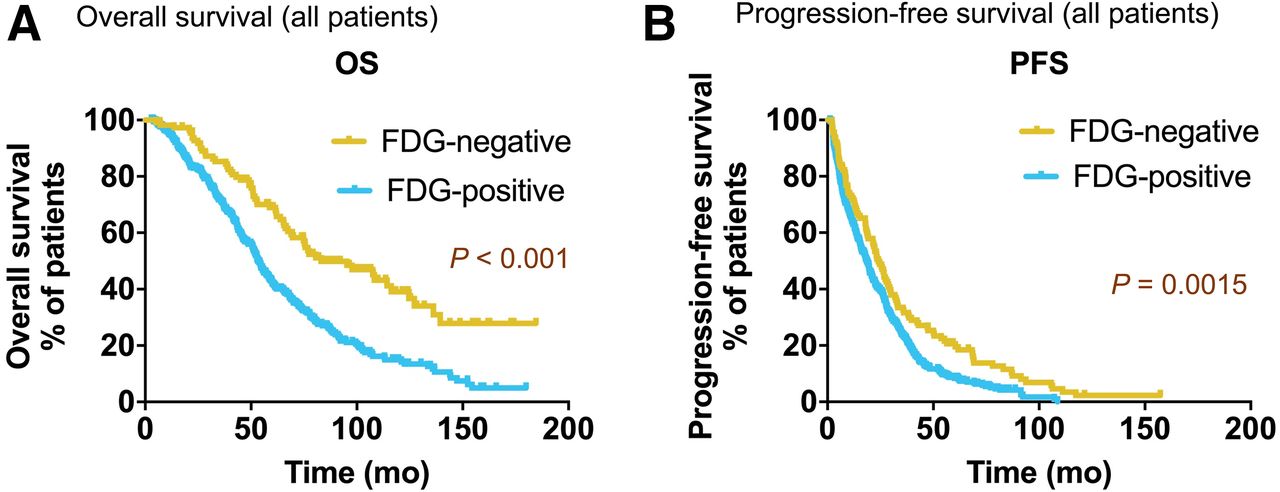
Kaplan–Meier survival analysis of all NEN patients (n = 495) stratified by baseline 18F-FDG status. Patients with 18F-FDG–negative lesions had significantly higher median OS (A) (83.1 mo vs. 53.2 mo, P < 0.001) and higher median PFS (B) (24.1 mo vs. 18.5 mo, P < 0.002) than patients with 18F-FDG–positive lesions.
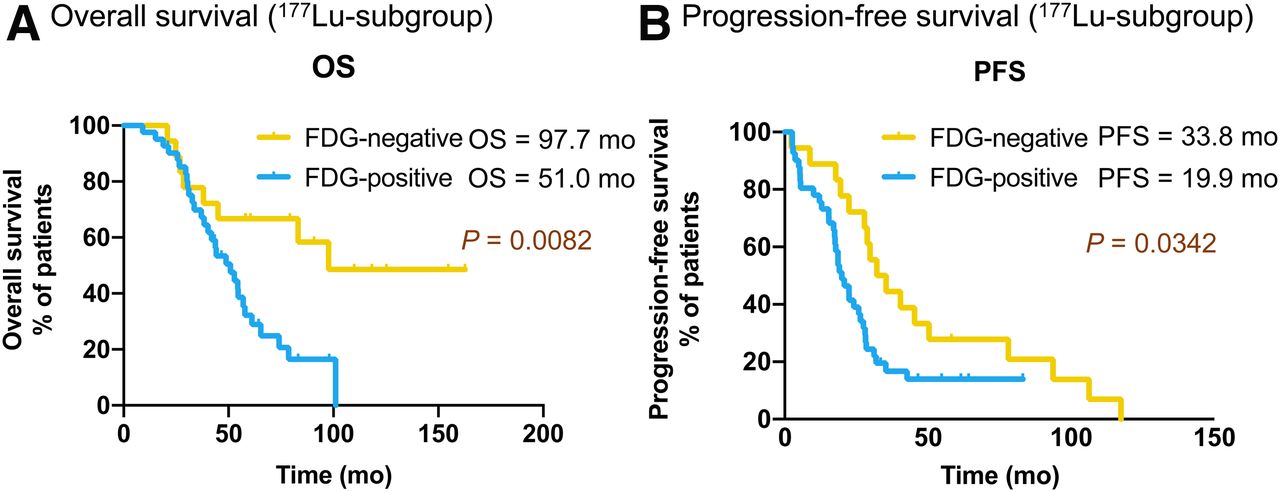
In the 177Lu-PRRT subgroup, median OS and PFS were significantly higher in the 18F-FDG–negative group than in the 18F-FDG–positive group (median OS, 97.7 mo vs. 51.0 mo [P < 0.01]; median PFS, 33.8 mo vs. 19.9 mo [P < 0.05]) (Fig. 3).

Kaplan–Meier curves of OS (A) and PFS (B) for 177Lu subgroup (n = 60) stratified by baseline 18F-FDG status.
In the pancreatic NEN subgroup, median OS and PFS were significantly higher in the 18F-FDG–negative than in the 18F-FDG–positive group (median OS, 114.3 mo vs. 52.8 mo; median PFS, 36.9 mo vs. 22.4 mo [P < 0.001 for both]) (Fig. 4).
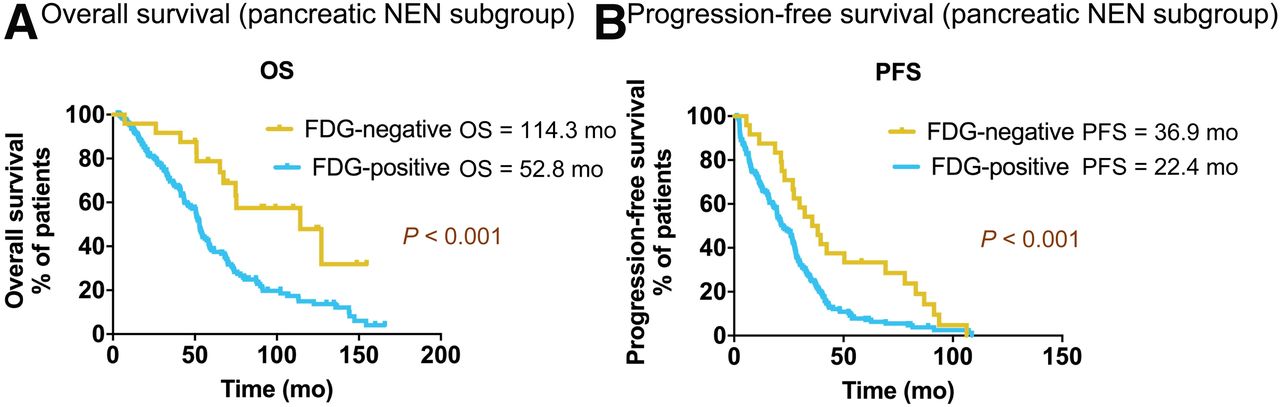
Kaplan–Meier survival of OS (A) and PFS (B) for pancreatic NEN subgroup (n = 199) stratified by baseline 18F-FDG status.
In the midgut NEN subgroup, the median OS was 95.3 mo in the 18F-FDG–negative group and 62.1 mo in the 18F-FDG PET–positive group. The median PFS was 36.1 mo in the 18F-FDG–negative group and 29.0 mo in the 18F-FDG PET–positive group.
68Ga-SSTR PET Imaging Related to Survival
68Ga-SSTR uptake in the primary tumor was an independent predictor of OS (P = 0.011) and PFS (P = 0.003). In multivariate analysis, compared with level 1 liver tumor burden in 68Ga-SSTR PET, level 2 had a significant decreased risk of progression, with an HR of 0.5 (95% CI, 0.3–0.7; P = 0.001), but levels 3 and 4 had no significant decrease in risk (level 3: HR, 0.9; 95% CI, 0.5–1.5 [P = 0.664]; level 4: HR, 0.9; 95% CI, 0.6–1.1 [P = 0.256]).
The statistical analysis revealed that the highest SUVmax of all target (SSTR-positive) lesions on 68Ga-SSTR PET for each patient was not significant in terms of OS or PFS, and there was no direct correlation between OS and the highest SUVmax of all target tumor lesions (P > 0.05). The analysis of OS showed no significant difference between patients with an SUVmax of less than 15 and patients with an SUVmax of more than 15 on 68Ga-SSTR PET imaging, including those from the midgut NEN subgroup and the 18F-FDG–negative group. For 18F-FDG–positive patients with a ratio of more than 2 for maximum SSTR to 18F-FDG (the highest SUVmax among all target lesions on 68Ga-SSTR PET to the most 18F-FDG–avid tumor lesions for each patient), the median OS was 53.0 mo, compared with 43.4 mo for patients with a ratio of less than 2 (P = 0.030). For 18F-FDG–negative patients, the median OS was 108.3 mo, versus 76.9 mo for an SUVmax of more than 15.0 and an SUVmax of 15.0 or less on 68Ga-SSTR PET, respectively.
DISCUSSION
To the best of our knowledge, to date this study represents the largest cohort of metastatic NEN patients treated with personalized PRRT in which long-term prognosis was evaluated on the basis of initial dual PET tracer imaging (68Ga-SSTR PET/CT and 18F-FDG PET/CT). All patients were followed up until death (64.4% of the patients) or the study cutoff date (end of 2018). The follow-up (median, 94 mo; range, 3–189 mo) in this patient cohort is the longest among all published relevant studies (16).
SSTR PET/CT imaging with 68Ga-labeled somatostatin analogs has excellent sensitivity and specificity for diagnosing and staging NENs (38,39). 18F-FDG PET is widely used in oncology, but its use in neuroendocrine tumors has been a matter of controversy (40). Several studies have demonstrated the association of 18F-FDG PET with treatment response and PFS after PRRT in NENs. In a study with 98 NEN patients, an 18F-FDG SUVmax of more than 3 was found to be the only independent predictor of PFS, and an 18F-FDG SUVmax of more than 9 was strongly correlated with a greater risk of mortality, although median OS was not reached (27). Sansovini et al. reported a phase II trial of 177Lu-DOTATATE PRRT in 60 patients with locally advanced or metastatic well-differentiated grade 1 or 2 pancreatic neuroendocrine tumors who completed the scheduled 5 cycles of PRRT. The median PFS was 21.1 mo in 18F-FDG–positive patients (58%) and 68.7 mo in the 18F-FDG–negative group regardless of the total activity administered (P < 0.0002) (41), but the uptake on SSTR imaging, before and after therapy, was not significant in terms of PFS (42). Chan et al. reported a NETPET grading scheme for dual SSTR and 18F-FDG PET/CT imaging in a study with 62 NEN patients. The NETPET grade divided subjects into solely SSTR-positive, SSTR-positive/18F-FDG–positive, and SSTR-negative/18F-FDG–positive subgroups and introduced a 0–5 categoric scale based largely on the characteristics of the single initial lesion, showing promise as a prognostic imaging biomarker in neuroendocrine tumors (43). Our group also has demonstrated that PET/CT imaging with 18F-FDG along with SSTR helps to stratify patients with World Health Organization grade 3 NENs (16).
The median OS of the current study after PRRT was 58.7 mo, which is within the range reported in the literature (18). The median PFS was 19.6 mo, which was shorter than in other studies, as the treatment response was evaluated according to both RECIST and molecular imaging criteria. Moreover, the current study included 128 patients who received up to 3 cycles of PRRT only, which may have influenced the prognosis. Meanwhile, this study included not only grade 1 and 2 NENs but also high-risk grade 3 NENs, as well as patients with variable primary tumor sites. In this study, both tumor grade and primary tumor site were found to be independent predictors for OS. Patients with midgut NENs had the longest median OS, 77.8 mo; whereas, median OS was 55.4 mo in the rectal NEN group, 54.4 in the pancreatic NEN group, and 46.2 mo in the lung NEN group.
Our results demonstrated that an 18F-FDG–negative tumor status was an independent prognostic factor for OS of PRRT, with a 0.5-fold decrease in the risk of death. Although not generally used for the diagnosis of NENs, 18F-FDG PET/CT was able to classify NEN patients into different prognostic categories for PRRT. A very high SUV on 18F-FDG PET would at least lead to reconsideration of the decision to perform PRRT as the first-line procedure. We would suggest that the decision to perform 18F-FDG PET/CT be based on personalized medicine criteria, especially the grade, time course of the disease, speed of progression, total tumor mass, and other criteria as previously published regarding the Bad Berka score (8,16,34).
SSTR imaging is a positive prognostic factor for demonstrating the abundance of SSTR expression, which is intensely related to well-differentiated tumor and therefore used for evaluating the possibility of treatment with cold and radiolabeled somatostatin analogs (44). In this study, 68Ga-SSTR uptake in the primary tumor was an independent predictor of OS and PFS, as agrees with other studies. However, the prognostic value of 68Ga-SSTR PET imaging was lower than that of 18F-FDG PET. There was no direct correlation between the single highest SUVmax of 68Ga-SSTR PET and OS. For all patients with 18F-FDG uptake (NETPET SSTR-positive/18F-FDG–positive disease) and a ratio of more than 2 for the highest SUVmax on 68Ga-SSTR PET to the most 18F-FDG–avid tumor lesion, the median OS was higher than in patients with a ratio of less than 2 (P = 0.030).
One of the limitations of this study is that it was a retrospective analysis (however, with prospective data sampling using a structured database). There were variations in radioisotopes and SSTR affinities because different radiopharmaceuticals were used. Another limitation was the lack of availability of the exact Ki-67 index in 104 (21%) patients; however, these patients were referred from other centers with histopathologically confirmed NENs without reporting the Ki-67 index, and relevant tissue specimens were not available for reevaluation. Furthermore, concerning the value of SSTR uptake for predicting survival after receiving PRRT, this study analyzed only the single highest SUVmax among all target lesions on 68Ga-SSTR PET for each patient. Analysis of the metastatic tumor burden score on 68Ga-SSTR PET, the further genomic signature, and the association between survival and comprehensive individual evaluation of SSTR expression remains warranted.
CONCLUSION
18F-FDG PET/CT demonstrating glycolytic activity, or lack thereof, is an independent prognostic factor in patients with NENs treated with PRRT. 18F-FDG–negative NENs demonstrated better OS and PFS than 18F-FDG–positive NENs, particularly in pancreatic NENs. High uptake on 68Ga-SSTR PET/CT combined with negative 18F-FDG PET/CT findings is associated with a comparatively prolonged PFS and OS.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is 18F-FDG PET an independent prognostic factor in patients with NENs treated with PRRT and useful in NEN patients after PRRT?
PERTINENT FINDINGS: This large cohort study revealed the presence of positive lesions on 18F-FDG PET to be an independent prognostic factor in patients with NENs treated with PRRT. A significant difference was found in both PFS and OS between 18F-FDG–positive and 18F-FDG–negative patients.
IMPLICATIONS FOR PATIENT CARE: Metabolic imaging with 18F-FDG PET/CT complements the molecular imaging aspect of 68Ga-SSTR PET/CT for the prognosis of survival in NEN patients after PRRT.
Acknowledgments
We thank the patients who participated in this study, as well as all research support staff, radiopharmacists, radiochemists, physician colleagues, nursing staff, and nuclear medicine technologists, past and present, at Zentralklinik Bad Berka, for their support.
Footnotes
↵* Contributed equally to this work.
Published online Mar. 13, 2020.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 24, 2019.
- Accepted for publication March 5, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Dual Somatostatin Receptor/18F-FDG PET/CT Imaging in Patients with Well-Differentiated, Grade 2 and 3 Gastroenteropancreatic Neuroendocrine Tumors
- Discordance Between Histopathologic Grading and Dual-Tracer PET/CT Findings in Metastatic NETs and Outcome of 177Lu-DOTATATE PRRT: Does In Vivo Molecular PET Perform Better from the Viewpoint of Prediction of Tumor Biology?
- Dual PET Imaging in Bronchial Neuroendocrine Neoplasms: The NETPET Score as a Prognostic Biomarker
- 18F-FDG PET is Superior to WHO Grading as a Prognostic Tool in Neuroendocrine Neoplasms and Useful in Guiding PRRT: A Prospective 10-Year Follow-up Study