


Article Figures & Data
Figures
- FIGURE 1.
Kaplan–Meier curves of OS and PFS for all patients (n = 495). (A) Median OS was 58.7 mo (95% CI, 52.8–64.6). (B) Median PFS was 19.6 mo (95% CI, 17.6–21.7).
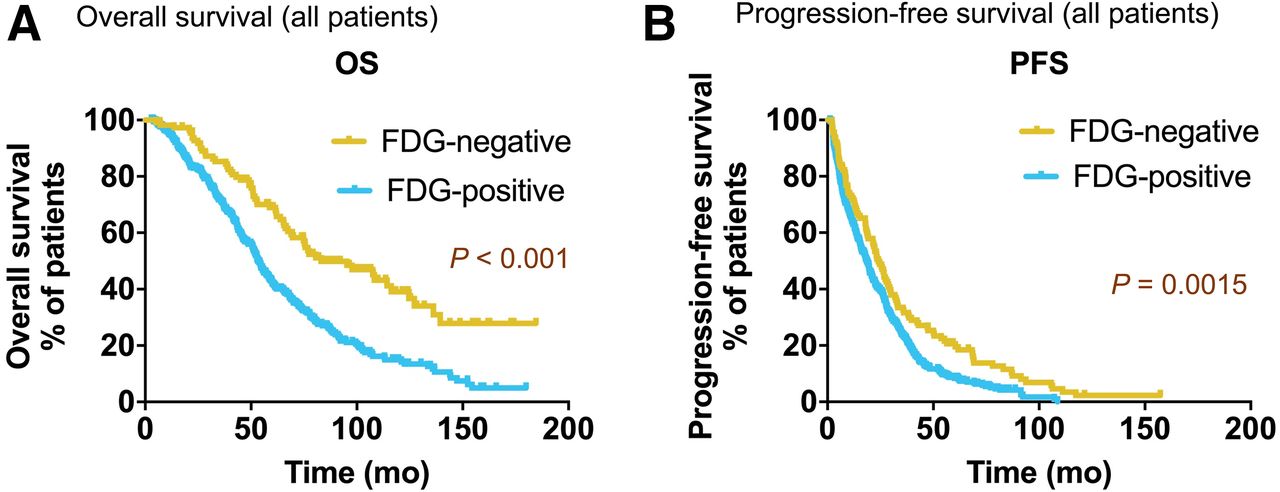
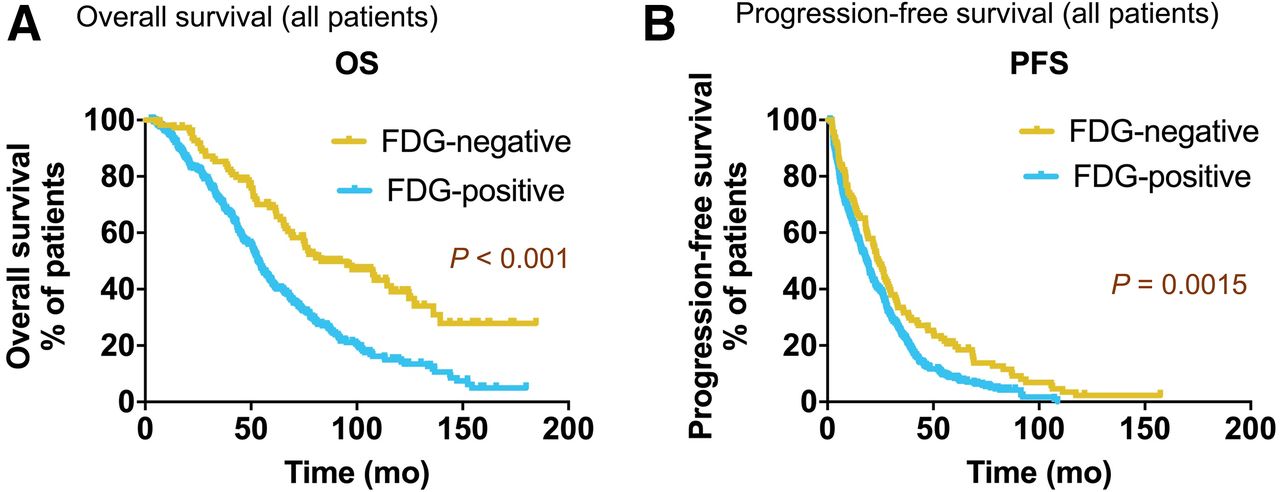
- FIGURE 2.
Kaplan–Meier survival analysis of all NEN patients (n = 495) stratified by baseline 18F-FDG status. Patients with 18F-FDG–negative lesions had significantly higher median OS (A) (83.1 mo vs. 53.2 mo, P < 0.001) and higher median PFS (B) (24.1 mo vs. 18.5 mo, P < 0.002) than patients with 18F-FDG–positive lesions.
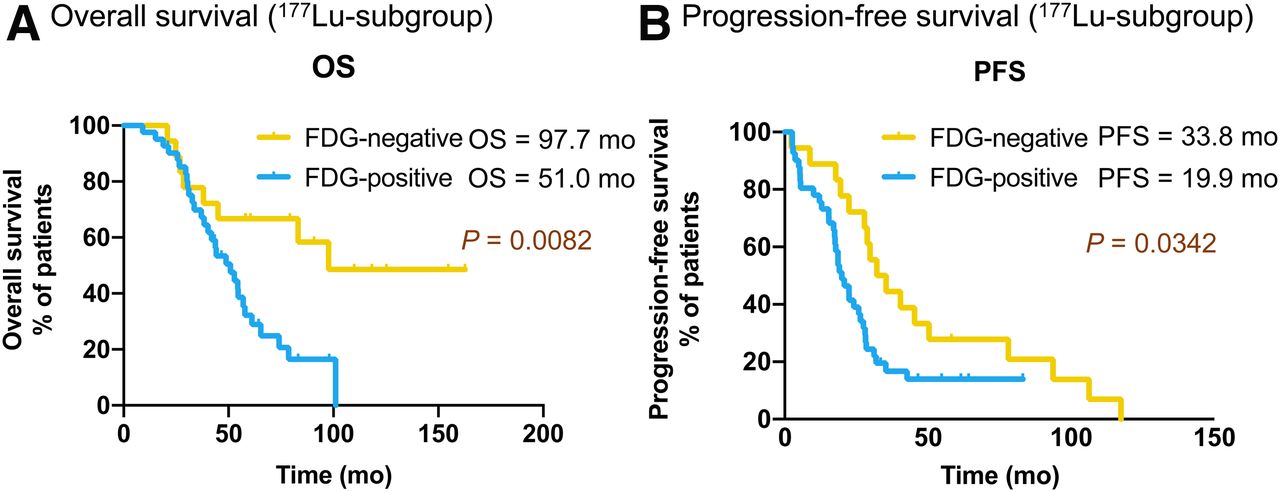
- FIGURE 3.
Kaplan–Meier curves of OS (A) and PFS (B) for 177Lu subgroup (n = 60) stratified by baseline 18F-FDG status.
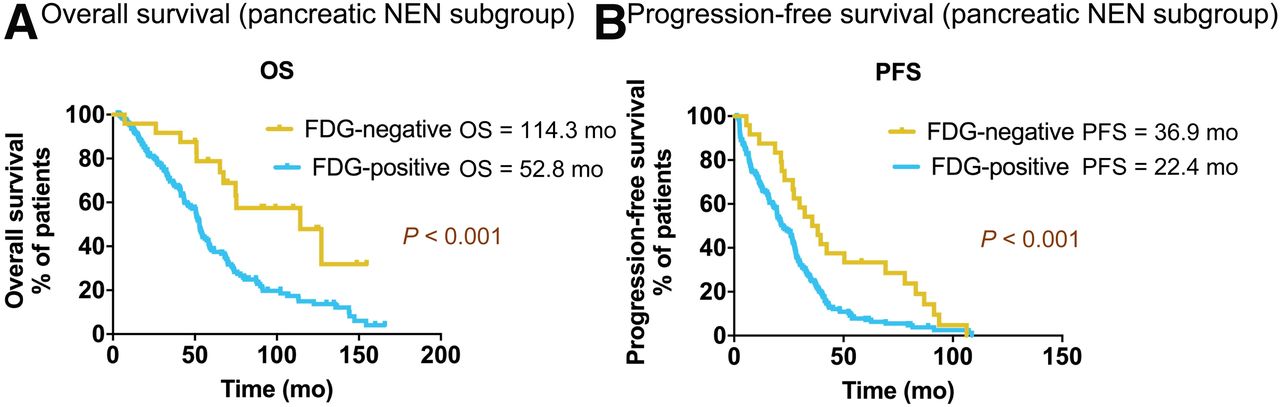
- FIGURE 4.
Kaplan–Meier survival of OS (A) and PFS (B) for pancreatic NEN subgroup (n = 199) stratified by baseline 18F-FDG status.



Tables
Demographic Data Sex Male 299 (60.4) Female 196 (39.6) Age (y) Median 59.0 ± 10.7 y ≤50 111 (22.4) 50< y ≤60 146 (29.5) 60< y ≤70 165 (33.3) 70< y ≤80 73 (14.7) Primary tumor site Cancer of unknown primary 49 (9.9) Lung 38 (7.7) Midgut 139 (28.1) Others 42 (8.5) Pancreas 199 (40.2) Rectum 20 (4.0) Stomach 8 (1.6) Ki-67 index grading G1 (Ki-67 < 3%) 117 (23.6) G2 (Ki-67 = 3%–20%) 245 (49.5) G3 (Ki-67 > 20%) 29 (5.9) Not assessed 104 (21.0) Qualitative data are numbers followed by percentages in parentheses; continuous data are medians.
Parameter Data 68Ga-SSTR uptake 495 (100.0) SUVmax = liver (level 1) 3 (0.6) Liver<SUVmax≤15 (level 2) 161 (32.5) 15<SUVmax≤20 (level 3) 106 (21.4) SUVmax>20 (level 4) 225 (45.5) 18F-FDG uptake 495 (100.0) Positive 382 (77.2) Negative 113 (22.8) Primary tumor uptake on 18F-FDG PET No uptake (level 1) 376 (76.0) SUVmax≤10 (level 2) 87 (17.6) 10<SUVmax≤15 (level 3) 16 (3.2) SUVmax>15 (level 4) 16 (3.20) Primary tumor uptake on 68Ga-SSTR No uptake (level 1) 262 (52.9) SUVmax≤15 (level 2) 102 (20.6) 15<SUVmax≤20 (level 3) 37 (7.5) SUVmax>20 (level 4) 94 (19.0) Liver tumor burden on 18F-FDG PET 0 lesions (level 1) 239 (48.3) 1 lesion (level 2) 49 (9.9) 2 to ≤5 lesions (level 3) 126 (25.5) >5 lesions (level 4) 77 (15.6) Not assessed 4 (0.8) Bone tumor burden on 18F-FDG PET 0 lesions (level 1) 409 (82.6) 1 lesion (level 2) 29 (5.9) 2 to ≤5 lesions (level 3) 36 (7.3) >5 lesions (level 4) 19 (3.8) Not assessed 2 (0.4) Lymph node tumor burden on 18F-FDG PET 0 lesions (level 1) 362 (73.1) 1 lesion (level 2) 55 (11.1) 2 to ≤5 lesions (level 3) 58 (11.7) >5 lesions (level 4) 13 (2.6) Not assessed 7 (1.4) Lung tumor burden on 18F-FDG PET 0 lesions (level 1) 463 (93.5) 1 lesion (level 2) 22 (4.4) 2 to ≤5 lesions (level 3) 6 (1.2) >5 lesions (level 4) 4 (0.8) Liver tumor burden on 68Ga-SSTR PET 0 lesions (level 1) 76 (15.4) 1 lesion (level 2) 32 (6.5) 2 to ≤5 lesions (level 3) 153 (30.9) >5 lesions (level 4) 234 (47.3) Liver tumor 68Ga-SSTR uptake No uptake (level 1) 77 (15.6) SUVmax≤15 (level 2) 117 (23.6) 15<SUVmax≤20 (level 3) 90 (18.2) SUVmax>20 (level 4) 211 (42.6) Data are numbers followed by percentages in parentheses.
- TABLE 3
Univariate and Multivariate Analyses of Potential Factors Contributing to OS, Part 1
OS (mo) Multivariate analysis Factors Median 95% CI Univariate analysis (P) HR and 95% CI P All patients 58.7 52.8–64.6 Sex Male 53.7 47.6–59.8 0.040 Female 66.1 54.4–77.8 Age (y) y ≤50 69.8 61.7–77.8 0.024 50< y ≤60 61.6 51.5–71.7 60< y ≤70 53.0 49.8–56.3 70< y ≤80 49.0 39.6–58.5 Grading Grade 1 78.5 66.2–90.8 <0.001 0.012 Grade 2 55.4 46.9–63.9 1.4 (1.0–2.0) 0.038 Grade 3 33.2 18.8–7.6 2.5 (1.3–4.5) 0.004 Not assessed 54.1 48.3–59.9 1.6 (1.1–2.2) 0.009 18F-FDG PET uptake Positive 53.2 49.4–57.0 <0.001 0.002 Negative 83.1 57.0–109.2 0.5 (0.3–0.8) Primary tumor site Cancer of unknown primary 65.1 47.4–82.7 0.007 0.004 Lung 46.2 34.1–58.3 0.3 (0.1–0.7) 0.004 Midgut 77.8 61.0–94.6 0.7 (0.3–1.6) 0.344 Others 65.7 31.3–100.1 0.3 (0.1–0.7) 0.008 Pancreas 54.4 49.3–59.6 0.4 (0.2–1.0) 0.041 Rectum 55.4 50.3–60.4 0.5 (0.2–1.0) 0.063 Stomach 46.9 33.3–60.5 0.6 (0.2–1.5) 0.239 - TABLE 4
Univariate and Multivariate Analyses of Potential Factors Contributing to OS, Part 2
OS (mo) Multivariate analysis Factors Median 95% CI Univariate analysis (P) HR and 95% CI P Liver tumor burden on 18F-FDG PET 0 lesions 75.6 65.5–85.6 <0.001 0.034 1 lesion 55.4 36.9–73.9 1.7 (0.6–5.2) 0.338 2 to ≤5 lesions 47.1 40.5–53.7 1.2 (0.4–3.8) 0.712 >5 lesions 43.7 35.4–52.0 2.2 (0.7–6.4) 0.157 Not assessed 54.6 33.7–75.5 2.3 (0.8–7.0) 0.127 Bone tumor burden on 18F-FDG PET 0 lesions 61.6 54.9–68.3 0.004 1 lesion 56.0 29.6–82.4 2 to ≤5 lesions 41.9 25.1–58.8 >5 lesions 43.4 19.2–67.7 Not assessed 32.6 — Lymph node tumor burden on 18F-FDG PET 0 lesions 63.8 56.3–71.4 0.006 0.035 1 lesion 51.6 34.6–68. 5 1.4 (0.5–4.1) 0.540 2 to ≤5 lesions 46.2 37.2–55.3 1.7 (0.6–5.2) 0.344 >5 lesions 37.4 10.0–64.7 1.8 (0.6–5.4) 0.293 Not assessed 86.6 23.7–149.6 4.4 (1.3–15.3) 0.018 Grading of PRRT 2 to ≤3 cycles 33.27 25.0–41.3 <0.001 <0.001 4 to ≤5 cycles 51.6 44.5–58.7 7.9 (3.9–15.9) <0.001 6 to ≤7 cycles 68.9 61.8–76.1 4.7 (2.6–8.4) <0.001 8 to ≤10 cycles 122.5 84.8–160.3 3.0 (1.8–5.0) <0.001 Cumulative activity (GBq) Activity ≤15 26.0 13.8–38.2 <0.001 0.038 15< activity ≤25 52.7 45.4–59.9 1.1 (0.6–2.0) 0.745 25< activity ≤35 61.1 54.9–67.3 0.7 (0.4–1.1) 0.084 Activity >35 77.8 66.0–89.6 0.8 (0.6–1.2) 0.379 - TABLE 5
Univariate and Multivariate Analyses of Potential Factors Contributing to PFS, Part 1
PFS (mo) Multivariate analysis Factors Median 95% CI Univariate analysis (P) HR and 95% CI P All patients 19.6 17.6–21.7 Age y ≤50 25.0 19.4–30.5 0.281 50< y ≤60 18.4 12.8–23.9 60< y ≤70 17.9 15.1–20.7 70< y ≤80 22.4 16.8–28.0 Grading Grade 1 23.0 15.9–30.2 0.003 0.039 Grade 2 18.9 15.2–22.6 1.2 (0.9–1.5) 0.150 Grade 3 7.5 0.0–20.1 2.1 (1.3–3.4) 0.003 Not assessed 19.8 13.8–25.7 1.1 (0.9–1.5) 0.426 18F-FDG PET uptake Positive 18.5 15.9–21.1 0.002 0.007 Negative 24.1 19.9–28.3 0.7 (0.5–0.9) Primary tumor site Cancer of unknown primary 11.4 6.5–16.2 0.011 Lung 10.6 5.0–16.1 Midgut 22.6 17.2–28.0 Others 9.1 2.7–15.5 Pancreas 25.8 21.8–29.8 Rectum 19.9 11.8–27.9 Stomach 24.6 18.9–30.4 - TABLE 6
Univariate and Multivariate Analyses of Potential Factors Contributing to PFS, Part 2
PFS (mo) Multivariate analysis Factors Median 95% CI Univariate analysis (P) HR and 95% CI P Liver tumor burden on 18F-FDG PET 0 lesions 20.8 17.4–24.1 0.034 1 lesion 27.8 20.9–34.7 2 to ≤5 lesions 16.2 11.5–20.9 >5 lesions 17.9 14.1–21.7 Not assessed 28.2 0.0–58.7 Bone tumor burden on 18F-FDG PET 0 lesions 22.4 19.3–25.5 <0.001 0.001 1 lesion 13.3 1.4–25.1 1.0 (0.2–4.1) 0.982 2 to ≤5 lesions 10.5 8.4–12.5 1.7 (0.4–7.4) 0.479 >5 lesions 11.5 0.0–24.9 2.2 (0.5–9.4) 0.304 Not assessed 12.0 — 1.2 (0.3–5.2) 0.848 Lymph node tumor burden on 18F-FDG PET 0 lesions 21.6 18.6–24.7 <0.001 0.050 1 lesion 17.9 10.9–25.0 1.2 (0.5–3.1) 0.587 2 to ≤5 lesions 15.4 12.3–18.6 1.3 (0.5–3.4) 0.552 >5 lesions 6.5 4.5–8.5 1.3 (0.5–3.3) 0.563 Not assessed 37.2 7.1–67.3 3.5 (1.2–10.1) 0.019 Lung tumor burden on 18F-FDG PET 0 lesions 19.9 17.5–22.3 <0.001 1 lesion 18.4 16.5–20.3 2 to ≤5 lesions 3.7 0.0–21.3 >5 lesions 5.3 1.5–9.2 Grading of PRRT 2 to ≤3 cycles 13.6 8.6–18.5 0.907 4 to ≤5 cycles 18.0 15.2–20.8 6 to ≤7 cycles 25.0 20.9–29.2 8 to ≤10 cycles 26.8 16.7–36.8
Supplemental Data
Files in this Data Supplement:





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Dual Somatostatin Receptor/18F-FDG PET/CT Imaging in Patients with Well-Differentiated, Grade 2 and 3 Gastroenteropancreatic Neuroendocrine Tumors
- Discordance Between Histopathologic Grading and Dual-Tracer PET/CT Findings in Metastatic NETs and Outcome of 177Lu-DOTATATE PRRT: Does In Vivo Molecular PET Perform Better from the Viewpoint of Prediction of Tumor Biology?
- Dual PET Imaging in Bronchial Neuroendocrine Neoplasms: The NETPET Score as a Prognostic Biomarker
- 18F-FDG PET is Superior to WHO Grading as a Prognostic Tool in Neuroendocrine Neoplasms and Useful in Guiding PRRT: A Prospective 10-Year Follow-up Study