


Abstract
A quantitative imaging biomarker is desirable to provide a comprehensive measure of whole-body tumor burden in patients with metastatic prostate cancer, and to standardize the evaluation of treatment-related changes. Therefore, we evaluated whether prostate-specific membrane antigen (PSMA) ligand PET/CT may be applied to provide PSMA-derived volumetric parameters for quantification of whole-body tumor burden. Methods: One hundred one patients who underwent 68Ga-PSMA I&T PET/CT because of increasing prostate-specific antigen (PSA) levels after radical prostatectomy were included in this retrospective analysis. Tracer uptake was quantified using SUVs. Volumetric parameters, that is, PSMA-derived tumor volume (PSMA-TV) and total lesion PSMA (TL-PSMA), were calculated for each patient using a 3-dimensional segmentation and computerized volumetry technique and compared with serum PSA levels. In a group of 10 patients, volumetric parameters were applied for treatment monitoring. Results: Volumetric parameters, that is, whole-body PSMA-TV and whole-body TL-PSMA, demonstrated a statistically significant correlation with PSA levels (P < 0.0001) as a surrogate marker of tumor burden, whereas SUVmax (P = 0.22) or SUVmean (P = 0.45) did not. Treatment response and treatment failure were paralleled by concordant changes in both whole-body PSMA-TV and whole-body TL-PSMA (P = 0.02), whereas neither the change in SUVmax (P = 1.0) nor the change in SUVmean (P = 1.0) concordantly paralleled changes in PSA levels. Conclusion: PSMA-derived volumetric parameters provide a quantitative imaging biomarker for whole-body tumor burden, capable of standardizing quantitative changes in PET imaging of patients with metastatic prostate cancer and of facilitating therapy monitoring.
Prostate-specific membrane antigen (PSMA) has recently gained interest as a molecular target for both clinical imaging and radionuclide therapy of prostate cancer (1–6). PET/CT imaging using 68Ga-PSMA ligands is a highly sensitive method for detection of primary tumors as well as locally recurrent or metastatic lesions after primary prostate cancer treatment (1,4). Accordingly, several PSMA ligands are in routine clinical use (2,5–7). 68Ga-PSMA imaging and therapy (I&T) has recently been demonstrated to localize primary prostate cancer and to provide high detection rates in recurrent prostate cancer (8–10). PSMA I&T can be labeled with either 68Ga or 177Lu for theranostic purposes (6).
PSMA ligand PET images may be semiquantitatively analyzed using SUVs (1). However, treatment-related changes in individual lesion SUV may be inadequate to determine the overall response. There is a need for precise assessment of overall tumor burden, especially in the context of monitoring therapeutic efficacy. The secretion of prostate-specific antigen (PSA) by cancer cells is highly variable and does not correlate with size or grade of prostate tumor lesions (11,12), such that serum PSA is a suboptimal biomarker for assessment of changes in tumor burden. In morphologic imaging, the RECIST allow for assessment of treatment, based on selection of representative individual tumor lesions (13). PET allows sensitive and direct assessment of whole-body tumor burden (14). Therefore, volumetric parameters derived from 18F-FDG PET/CT such as metabolic tumor volume (MTV) and total lesion glycolysis (TLG) have recently gained prominence for prognostic studies and for treatment monitoring in a variety of cancers, because they provide a direct estimation of whole-body tumor load (14–17). However, 18F-FDG PET/CT has limited value for assessment of prostate cancer. The preferred method for detecting skeletal metastases from prostate cancer is whole-body bone scintigraphy (18,19). However, this method is not specific to tumor cells, does not evaluate extraosseous disease, and does not readily provide volumetric parameters. In addition, the flare phenomenon may be misinterpreted as progression of disease. For all these reasons, a tumor-specific imaging biomarker of whole-body tumor burden would represent a major advance. To our knowledge, the concept of whole-body MTV or TLG assessment has not yet been applied in prostate cancer using PSMA ligands.
Therefore, the aim of this study was to evaluate PSMA ligand PET/CT to assess volumetric parameters as a measure of whole-body tumor burden, in comparison with other image-based parameters and PSA levels as a surrogate marker of tumor load.
MATERIALS AND METHODS
Study Population
The study population of this retrospective study consisted of 101 men (69.1 ± 6.8 y; age range, 49.9–82.6 y) who were referred for 68Ga-PSMA I&T PET/CT for detection of biochemical recurrence or PSA persistence after radical prostatectomy for prostate cancer between November 2014 and March 2016. Patients were selected according to the following inclusion and exclusion criteria. Inclusion criteria were detectable PSA level after radical prostatectomy for primary prostate cancer, detectable lesions on the 68Ga-PSMA I&T PET/CT scan, and available clinical history including initial Gleason score and PSA levels at the time of PET/CT. Exclusion criteria included external-beam radiation therapy or (combined) brachytherapy for primary treatment, local therapy without complete resection of prostate (transurethral resection of the prostate, cryosurgical ablation of the prostate, high-intensity focused ultrasound, irreversible electroporation), and more than 10 PSMA-positive lesions on the 68Ga-PSMA I&T PET/CT scan; the analysis was restricted to patients with 10 or fewer lesions, because nonautomated measurement of tumor volumes (TVs) is time- and labor-intensive.
Details on patient characteristics are summarized in Table 1. All studies were performed during the clinical diagnostic workup of patients. 68Ga-PSMA I&T was administered in compliance with the Declaration of Helsinki, §37, and the German Medicinal Products Act, AMG §13.2b. The institutional review board approved this retrospective study.
Characteristics of Study Population (n = 101)
Preparation of PSMA-Targeting Ligand
68Ga-PSMA I&T (5,6) was synthesized by a fully automated, good manufacturing practice–compliant procedure (20) using a good radiopharmaceutical practice module (SCINTOMICS GmbH) connected to a 68Ge/68Ga generator (1.11-GBq Obninsk Generator; Eckert & Ziegler EUROTOPE GmbH) and equipped with a disposable single-use cassette kit (ABX). A standardized labeling sequence with 22.5 μg (15 nmol) of unlabeled PSMA I&T (SCINTOMICS GmbH) was used. For quality control, 68Ga-PSMA I&T was analyzed by analytic high-performance liquid chromatography according to the monographs 2462 (gallium chloride) and 2482 (gallium edotreotide) of the European Pharmacopoeia. Radioanalytic high-performance liquid chromatography was performed on a ProStar high-pressure gradient system (Varian) equipped with an ultraviolet-visible detector (ProStar 335; Varian) and a radiodetector (Berthold LB 3800-20 with LB 6657 probe) using an RP-18 column (Gemini C18 5μ 110A, 250 x; Phenomenex). The eluent had a linear gradient from 100% solvent A (phosphate buffer/acetonitrile, 85:15) to 100% solvent B (phosphate buffer/acetonitrile, 65:35) over 25 min at a flow of 0.6 mL/min.
PET/CT Acquisition and Image Reconstruction
All studies were acquired using a dedicated PET/CT system (Biograph mCT 128 Flow; Siemens), equipped with an extended field-of-view PET component, a 128-slice spiral CT component, and a magnetically driven table optimized for continuous scanning. Patients received an intravenous injection of 96 ± 28 MBq of the 68Ga-PSMA ligand. Imaging started with a low-dose nonenhanced helical CT (120 kV, mA modulated, pitch of 1.2, reconstructed axial slice thickness of 5.0 mm) for attenuation correction. Whole-body PET images were subsequently acquired using continuous bed motion at a speed of 0.9 mm/s for chest and abdomen and 2.1 mm/s for legs at 1 h after injection after voiding of the bladder. All studies were reconstructed using Ultra HD, an iterative algorithm combined with time-of-flight and point-spread function information (Siemens Healthcare; 2 iterations, 21 subsets; matrix, 200; zoom, 1.0; gaussian filter, 5.0). No contrast material was administered.
Image Analysis and Calculation of Volumetric Parameters
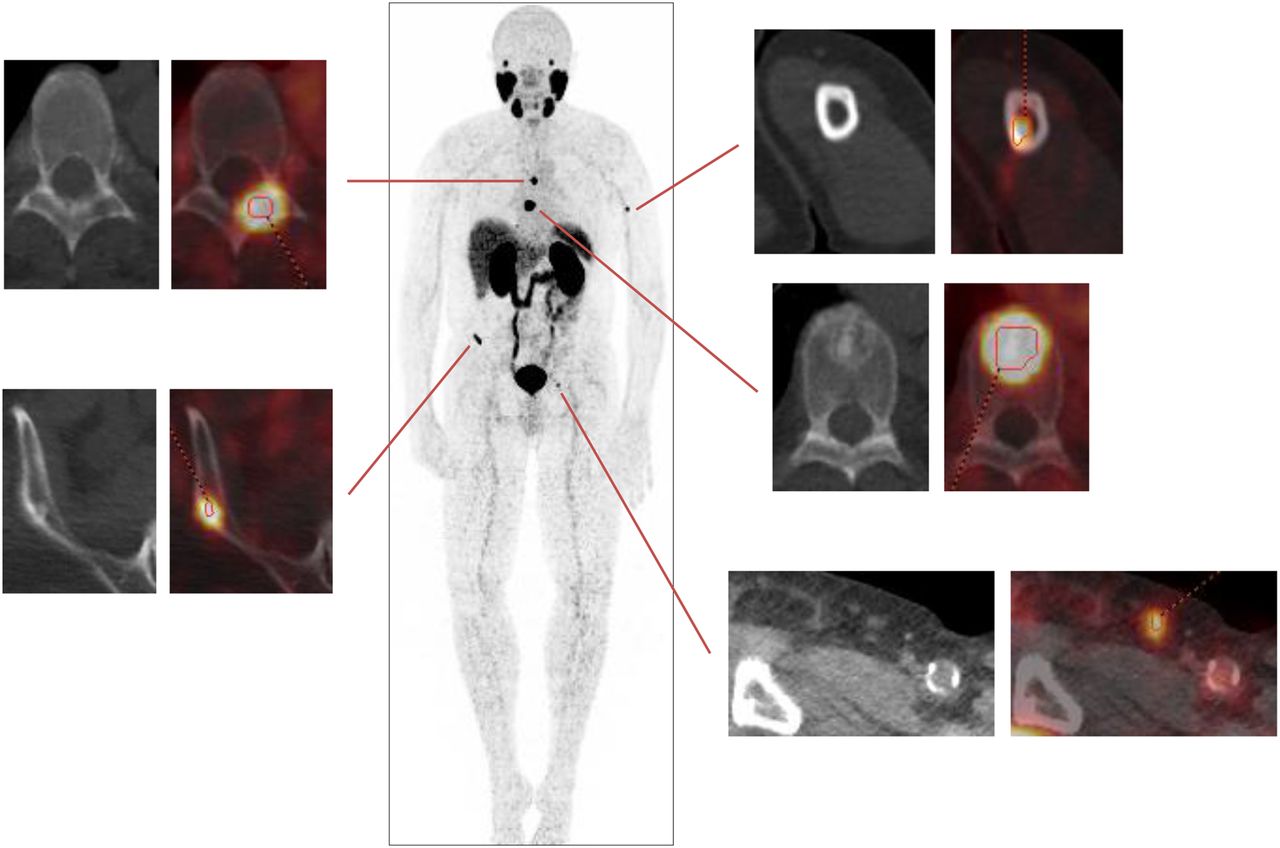
PET/CT images were analyzed using a dedicated workstation equipped with a commercial software package (syngo.via; V10B; Siemens Healthcare), allowing simultaneous and fused review of PET and CT data. All lesions suggestive for recurrent prostate cancer were noted, and their localization (e.g., local recurrence, lymph node metastases, bone metastases) was recorded (1). For PET images, focal uptake of 68Ga-PSMA I&T higher than background was judged as tissue suspected of malignancy. The number of detected metastases per patient was recorded. To calculate volumetric parameters, an isocontour volume of interest including all voxels above 45% of the maximum was created (Fig. 1) using a 3-dimensional segmentation and computerized volumetric technique, as performed recently in similar studies (9,21). This measurement yielded a PSMA-derived TV (PSMA-TV), similar to the MTV investigated in previous studies (14–17). Next, PSMA-TV was multiplied by SUVmean of the lesion, yielding the total lesion PSMA (TL-PSMA), comparable to the TLG as previously reported (14–17). In addition, SUVmean and SUVmax were measured within all volumes of interest. The SUVmax threshold of 45% was determined experimentally in 5 representative patient scans by varying the cutoff at 40%, 45%, and 50% to obtain agreement with the contour of the lesions on CT, compensating for activity spill-over. No significant differences were observed concerning PSMA-TV (P = 0.91), TL-PSMA (P = 0.64), SUVmax (P = 0.51), and SUVmean (P = 0.96) between these 5 scans and the total study population.

Volumetric assessment of whole-body tumor burden using 68Ga-PSMA I&T PET. Maximum-intensity projection showing several metastases (central panel). Volume of each individual tumor lesion (left and right panels) is segmented and summed up for calculation of whole-body PSMA-TV. In this patient with a PSA level of 15.88 ng/mL, PSMA-TV is 4.8 cm3 and TL-PSMA is 96.89 cm3.
The feasibility of volumetric therapy response assessment was investigated in 10 patients who underwent both a baseline and a follow-up 68Ga-PSMA I&T PET/CT scan. Relative changes in PSA levels were compared with relative changes in SUVs, PSMA-TV, and TL-PSMA.
Statistical Analysis
Categoric variables are presented with absolute and relative frequencies. Continuous variables are expressed as mean ± SD and range. Pearson correlation was used to explore the association of imaging findings with PSA levels. A 1-way ANOVA with a Tukey multiple-comparison test was performed to analyze the association between volumetric parameters and Gleason scores. Stepwise multiple-regression analysis was performed to identify independent variables for PSMA-TV and TL-PSMA. Statistical significance was established for P values of 0.05 or less. Statistical analysis was performed using GraphPad Prism (version 6.0 for Windows; GraphPad Software) or MedCalc (version 17.2; MedCalc Software).
RESULTS
The evaluation of 68Ga-PSMA I&T PET/CT scans including assessment of PSMA-TV and TL-PSMA was feasible in all patients. Relevant patient characteristics are shown in Table 1.
68Ga-PSMA I&T Imaging Findings and Volumetric Parameters
A total of 304 lesions were detected in 101 patients. A total of 202 lymph node metastases were found in 74 (73.3%) patients, 73 bone metastases in 31 (30.7%) patients, 17 local recurrences in 17 (16.8%) patients, and 12 other metastases in 6 (5.9%) patients. On average, 3.0 ± 2.6 lesions (range, 1–10) were found in an individual 68Ga-PSMA I&T PET/CT–positive patient. Detailed data on PSMA-TV, TL-PSMA, and intensity of tracer uptake are shown in Table 2.
Volumetric 68Ga-PSMA I&T PET Parameters (PSMA-TV and TL-PSMA) and Intensity of Tracer Uptake of Study Population
Serum PSA Levels Are Associated with Whole-Body PSMA-TV
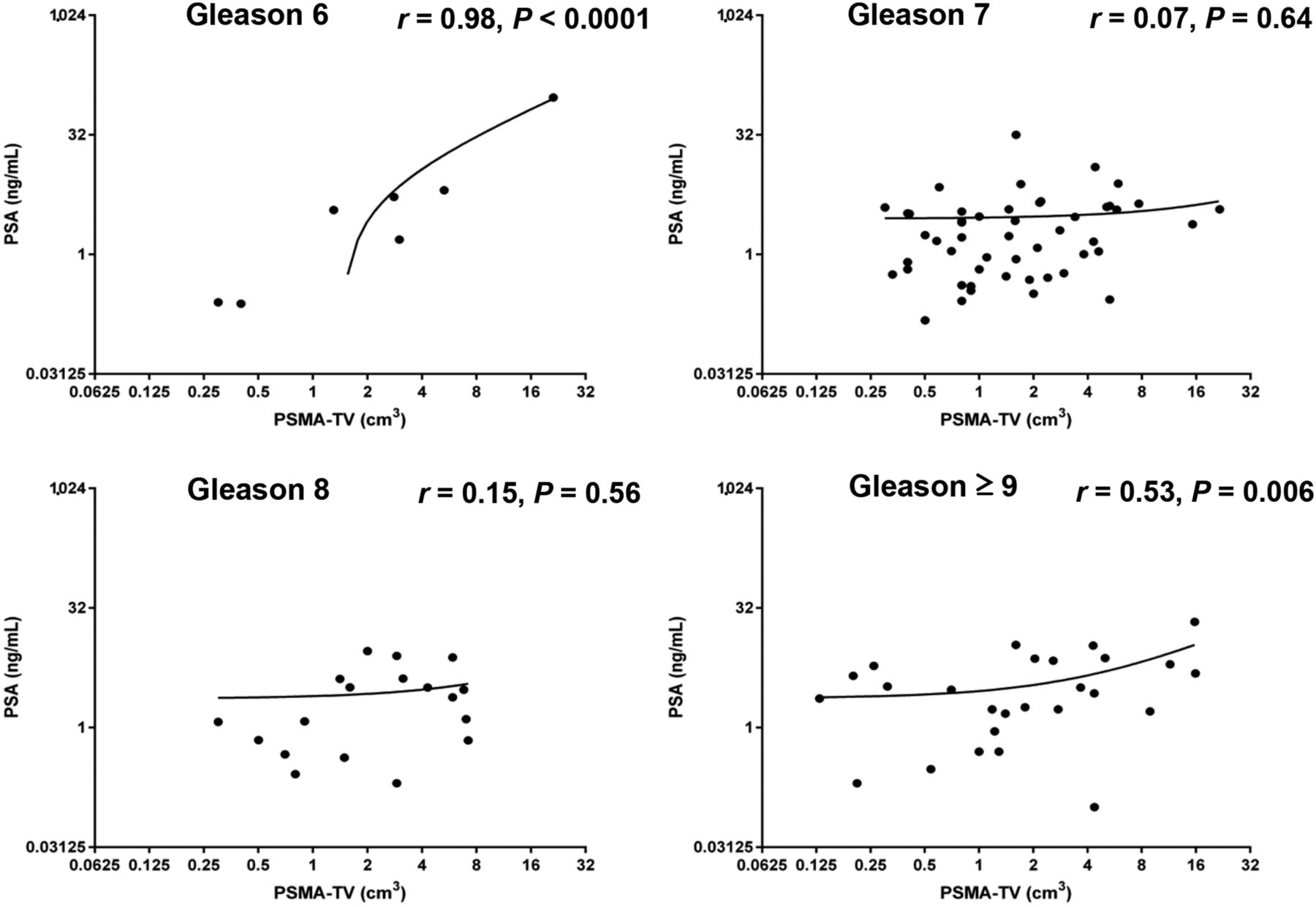
Whole-body PSMA-TV demonstrated a statistically significant correlation with PSA levels (r = 0.48, P < 0.0001). The correlation was statistically significant for both well-differentiated tumors (Gleason 6, r = 0.98, P < 0.0001) and poorly differentiated tumors (Gleason ≥ 9, r = 0.53, P = 0.006), but not for Gleason 7 and 8 tumors.
When whole-body PSMA-TV was analyzed using primary Gleason scores (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org), differences among PSMA-TV means were not statistically significant (1-way ANOVA, P = 0.32), meaning that metastatic TV did not depend on primary Gleason score. In multiple-regression analysis, PSA levels (rpartial = 0.48, P < 0.0001), but not initial Gleason score, were independently associated with PSMA-TV. The relation between whole-body PSMA-TV, PSA levels, and Gleason scores is illustrated in Figures 2 and 3.
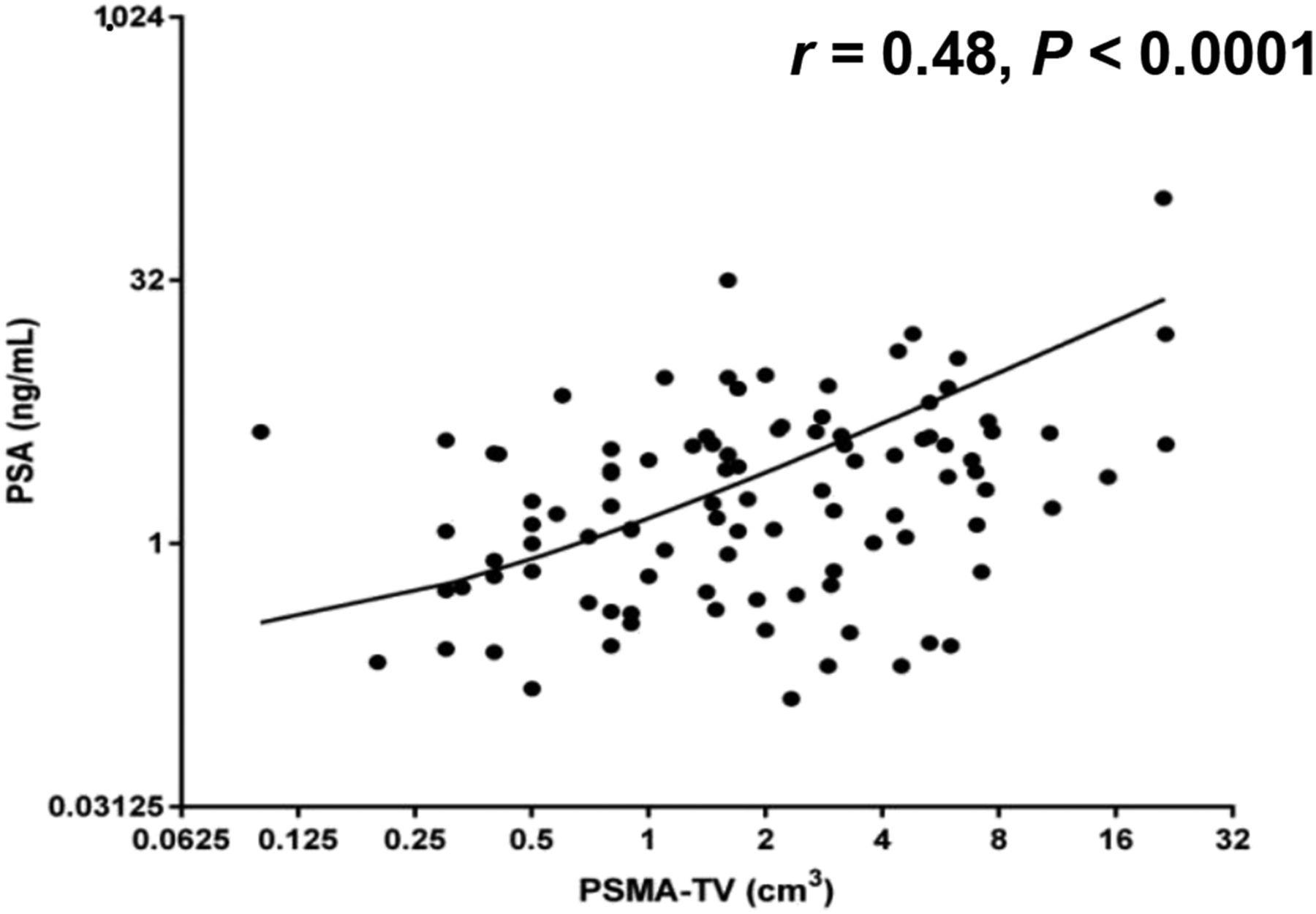
PSMA-TV for volumetric assessment of whole-body tumor burden using 68Ga-PSMA I&T PET. PSMA-TV demonstrates significant correlation with PSA levels (r = 0.48, P < 0.0001).

PSMA-TV for volumetric assessment of whole-body tumor burden using 68Ga-PSMA I&T PET. In subgroup analysis, correlation was statistically significant for Gleason 6 and Gleason ≥ 9 tumors, but not for Gleason 7 and 8 tumors.
Serum PSA Levels Are Associated with Whole-Body TL-PSMA
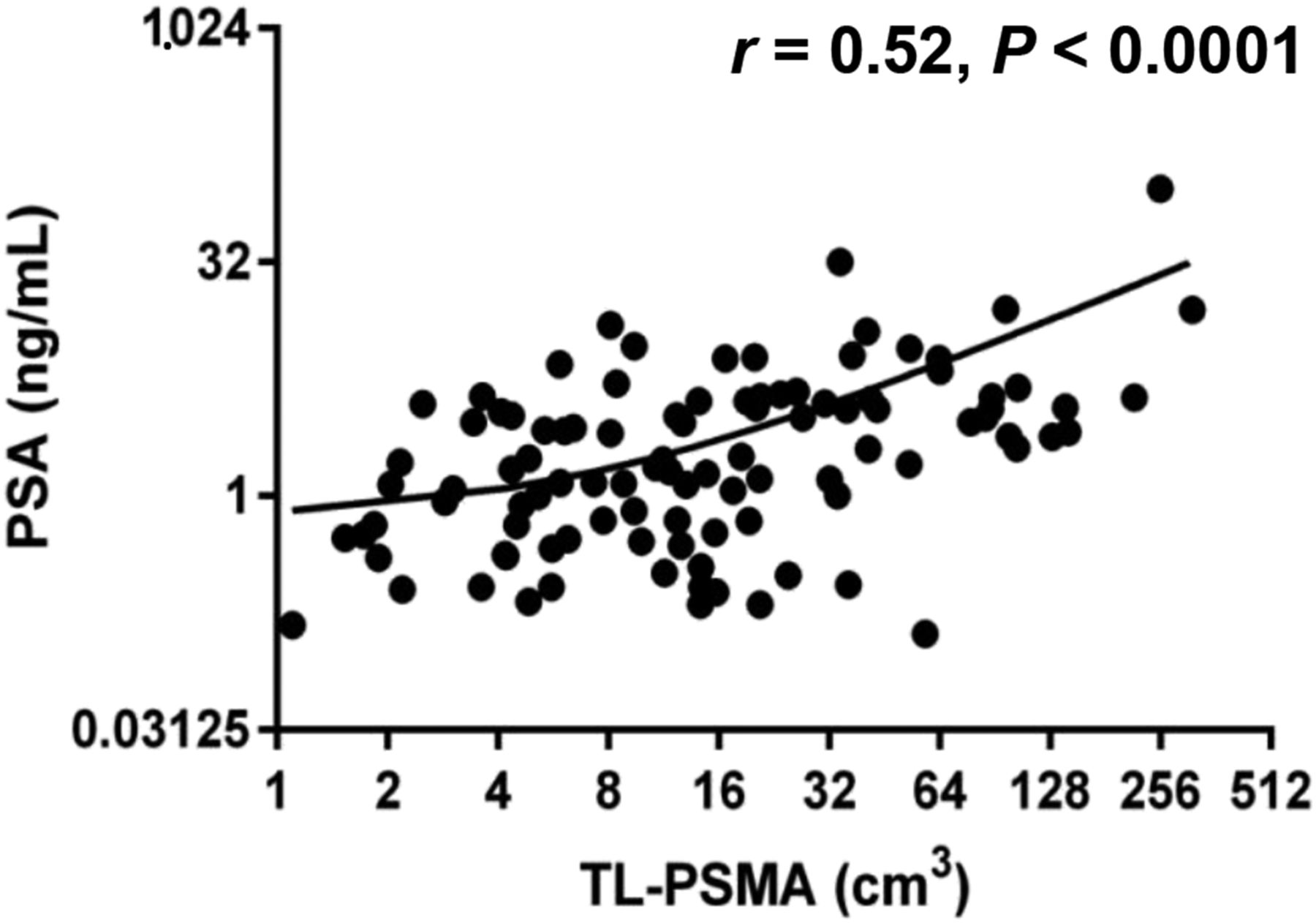
Whole-body TL-PSMA demonstrated a statistically significant correlation with PSA levels (r = 0.52, P < 0.0001). The correlation was statistically significant for both well-differentiated tumors (Gleason 6, r = 0.98, P < 0.0001) and poorly differentiated tumors (Gleason ≥ 9, r = 0.59, P = 0.002), but not for Gleason 7 and 8 tumors.
When whole-body TL-PSMA was analyzed using primary Gleason scores (Supplemental Fig. 2), differences among TL-PSMA means were statistically significant (1-way ANOVA, P = 0.01), meaning that metastatic TL-PSMA depends on primary Gleason score. Specifically, TL-PSMA was significantly higher in patients with a Gleason score of 9 or more compared with Gleason 7 (56.2 ± 14.5 vs. 18.9 ± 4.0, P = 0.002). Differences among other Gleason scores were not statistically significant. In multiple-regression analysis, PSA (rpartial = 0.57, P < 0.0001) and initial Gleason score (rpartial = 0.33, P < 0.001) were independently associated with TL-PSMA. The relation between whole-body TL-PSMA, PSA levels, and Gleason scores is illustrated in Figures 4 and 5.
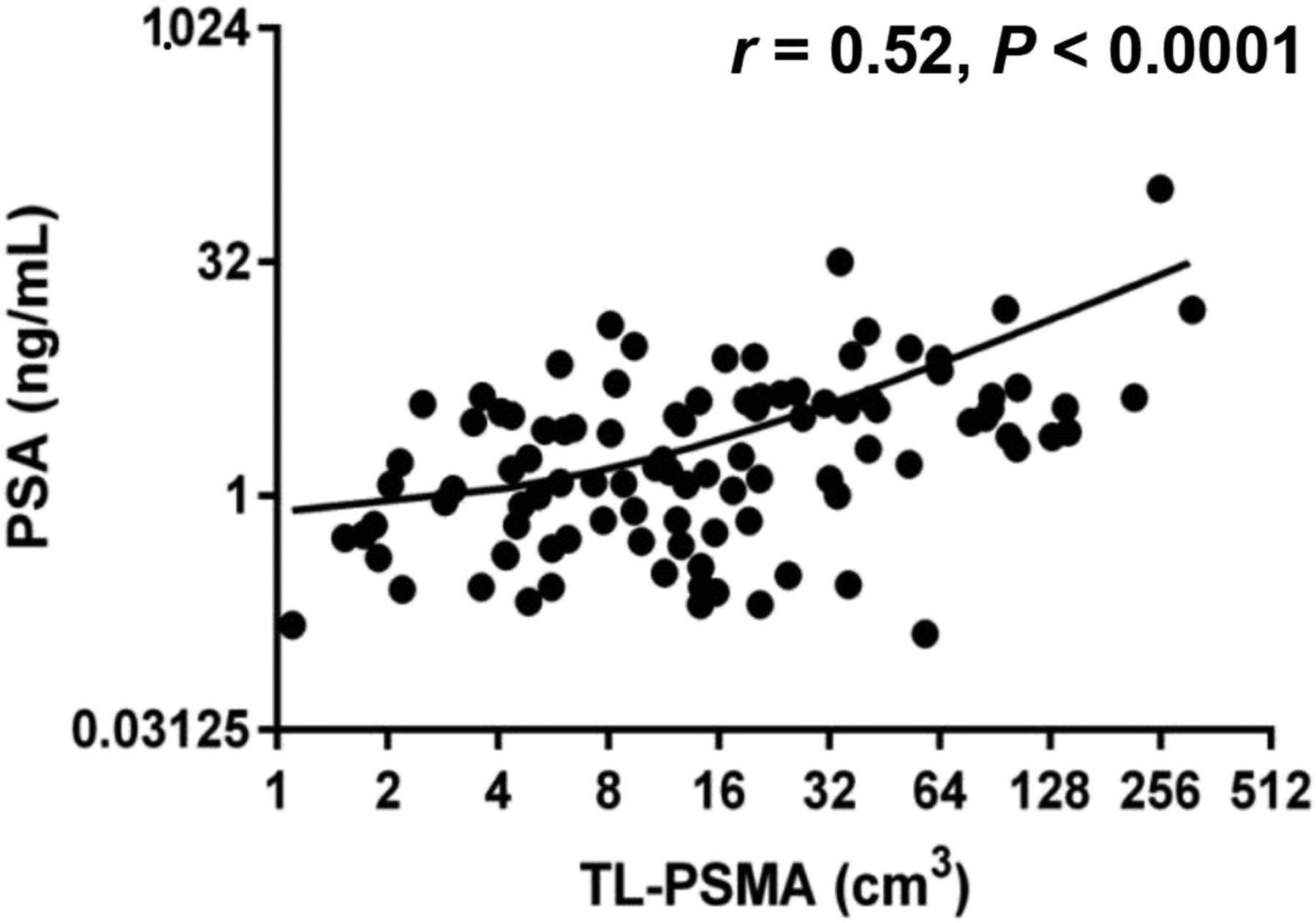
TL-PSMA for volumetric assessment of whole-body tumor burden using 68Ga-PSMA I&T PET. TL-PSMA demonstrates significant correlation with PSA levels (r = 0.52, P < 0.0001).
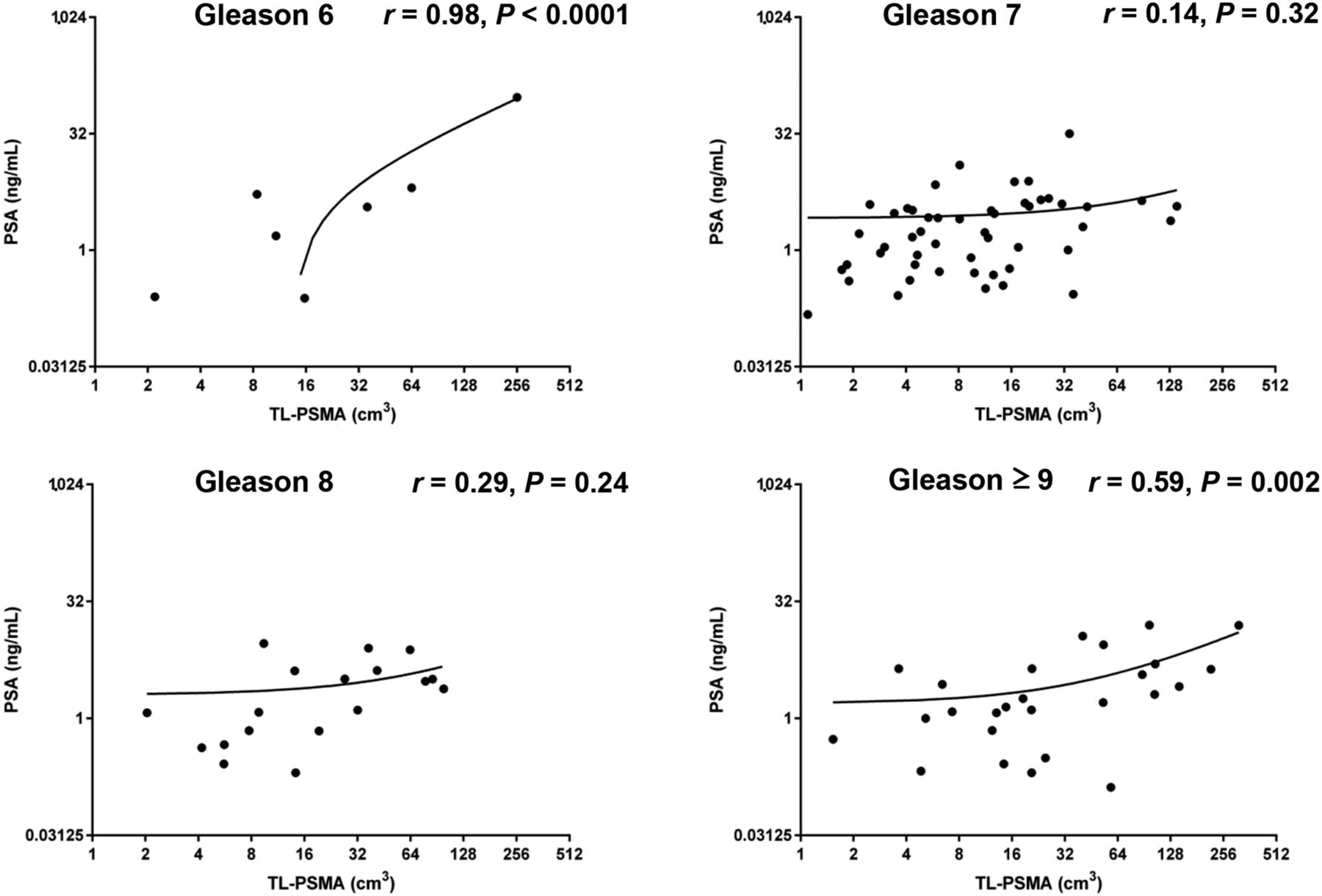
TL-PSMA for volumetric assessment of whole-body tumor burden using 68Ga-PSMA I&T PET. In subgroup analysis, correlation was statistically significant for Gleason 6 and Gleason ≥ 9 tumors, but not for Gleason 7 and 8 tumors.
Serum PSA Levels Are Not Associated with SUVs
Neither SUVmax (r = 0.12, P = 0.22) nor average SUVmean (r = 0.8, P = 0.45) demonstrated a significant correlation with PSA levels.
Preliminary Data of Volumetric Parameters for Treatment Monitoring
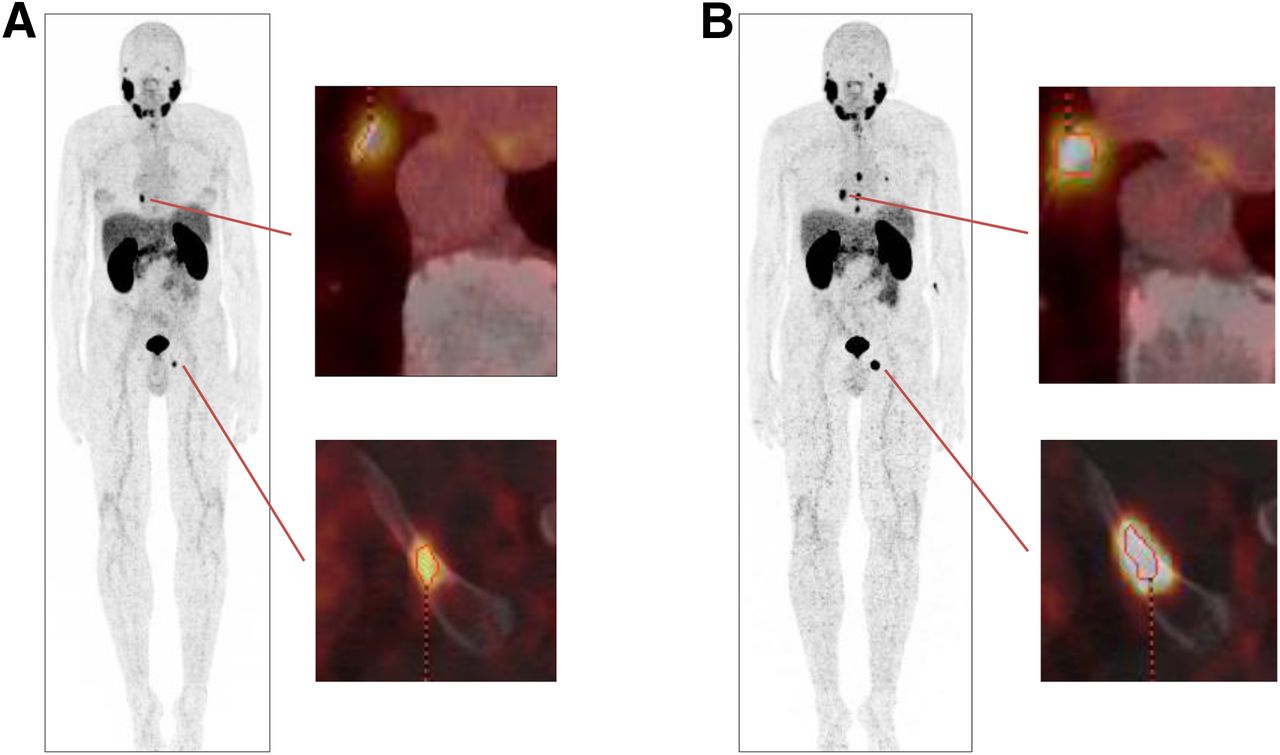
To support the hypothesis that single number volumetric whole-body parameters may be useful for disease monitoring, 10 patients who underwent a baseline and a follow-up 68Ga-PSMA I&T PET/CT scan (6 patients after initiation of androgen-deprivation therapy [ADT], 1 of these with additional 223Ra-dichloride therapy, 2 patients after salvage lymphadenectomy, and 2 patients under “watchful waiting” in the setting of rising PSA) were analyzed (Fig. 6). In 2 patients, PSA levels decreased at follow-up, whereas in 8 patients the PSA levels increased. Both whole-body PSMA-TV (P = 0.02) and whole-body TL-PSMA (P = 0.02) concordantly increased in all patients with increasing PSA levels and declined in all patients with declining PSA levels. Conversely, neither the change in SUVmax (P = 1.0) nor the change in SUVmean (P = 1.0) concordantly paralleled changes in PSA levels, whereby SUVs increased in 1 patient with declining PSA levels and declined in 4 patients with rising PSA levels. Results of the correlation analysis between changes in 68Ga-PSMA I&T PET parameters and changes in PSA levels are shown in Figure 7 and Supplemental Figure 3.

Volumetric assessment of whole-body tumor burden using 68Ga-PSMA I&T PET for therapy monitoring. Baseline PET (A) and follow-up PET (B) 7 mo after initiation of ADT (new lesions are not displayed separately). Serum PSA level increased from 1.22 to 5.01 ng/mL. PSMA-TV concordantly increased from 0.9 to 7.5 cm3, and TL-PSMA increased from 7.29 to 104.46 cm3, respectively.
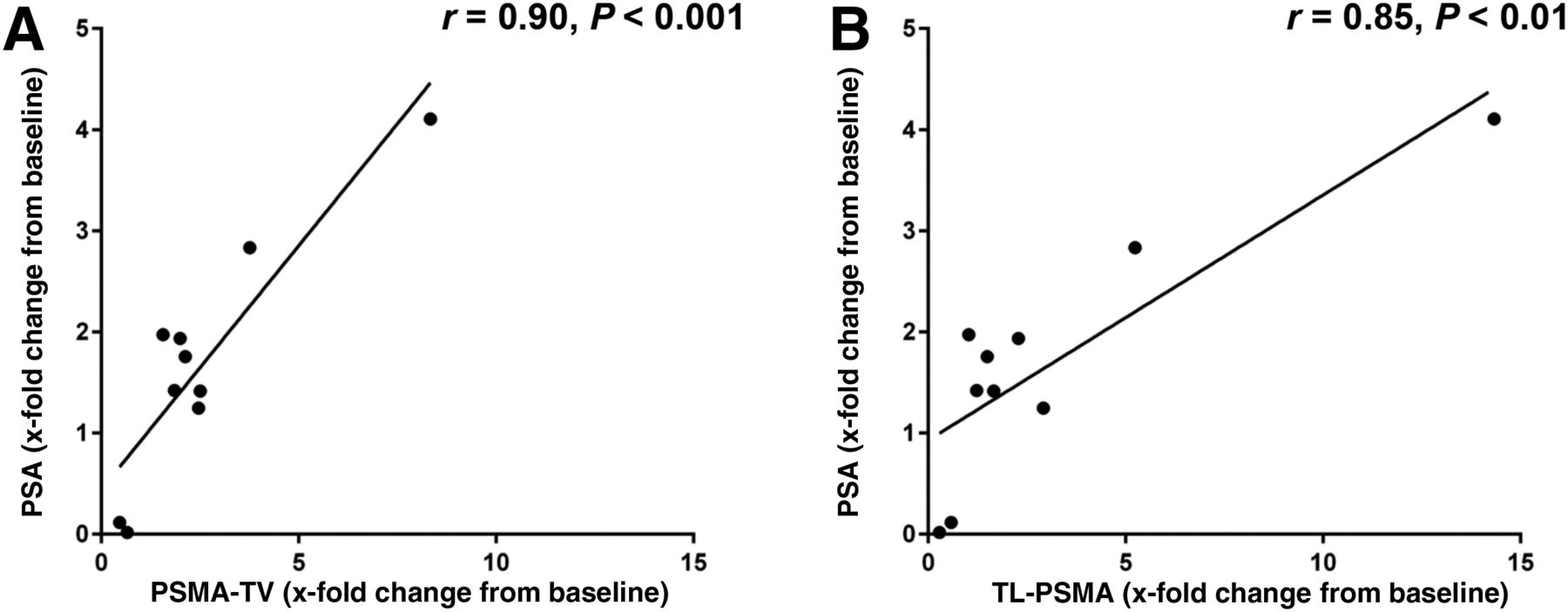
Graphical illustration of results of correlation analysis between changes of 68Ga-PSMA I&T PET parameters and changes in PSA levels. Relative change in PSA level over time is significantly correlated with relative change of both PSMA-TV (A, r = 0.90, P < 0.001) and TL-PSMA (B, r = 0.85, P < 0.01).
DISCUSSION
In the present study, we demonstrated that PSMA-TV and TL-PSMA may be used as quantitative imaging biomarkers in patients with prostate cancer and that these parameters may be applied for therapy monitoring. The use of volumetric parameters in 18F-FDG PET has gained interest to predict treatment response and overall prognosis in oncologic patients. For instance, van Rossum et al. demonstrated that the change in TLG after induction chemotherapy was predictive for a poor pathologic response in patients with esophageal adenocarcinoma (15). In another study, baseline MTV before chemotherapy for diffuse large B cell lymphoma was the only statistically significant predictor of progression-free survival at multivariate analysis (16). In prostate cancer, volumetric parameters have been evaluated in a small number of studies using radiotracers other than PSMA ligands (22,23). Incerti et al. assessed the value of 11C-choline PET/CT in the context of radiation treatment of lymph node recurrence from prostate cancer and reported that MTV was significantly associated with the clinical relapse-free survival and biochemical relapse-free survival (22).
We have applied the concept of whole-body MTV or TLG assessment into the setting of PSMA imaging of prostate cancer. When the relationship between serum PSA levels and volumetric PET parameters was analyzed, a statistically significant correlation was observed with both whole-body PSMA-TV (r = 0.48, P < 0.0001) and whole-body TL-PSMA (r = 0.52, P < 0.0001), demonstrating that the volumetric parameters were consistent with established biomarkers of metastatic tumor load. All patients had undergone radical prostatectomy before PET/CT-based restaging, and special attention was paid to exclude all patients with residual prostate tissue (e.g., after local cryotherapy), which might have influenced the correlation analysis between volumetric parameters and PSA. Previous studies found that high-grade tumors may produce less PSA per gram of tumor (24), and paradoxically low PSA levels in the context of poor differentiation may be observed, limiting the usefulness of PSA measurements (12). Volumetric PET parameters demonstrated a highly significant correlation with PSA (P < 0.0001), which was driven by Gleason 6 tumors (PSMA-TV, r = 0.98, P < 0.0001) and Gleason ≥ 9 tumors (PSMA-TV, r = 0.53, P = 0.006). By contrast, no significant correlation was found between PSA levels and TV in Gleason 7 and Gleason 8 tumors. There is currently no model to fully explain this phenomenon. Other PET-derived parameters such as SUVs are not useful for assessment of tumor burden, because they characterize only the intensity of tracer uptake in individual lesions. Accordingly, neither SUVmax (r = 0.12, P = 0.22) nor SUVmean (r = 0.8, P = 0.45) was associated with PSA levels in this study. Recently, novel biomarkers have been investigated for improved detection of prostate cancer. It would be interesting to explore the correlation of metastatic load on PET/CT and these biomarkers, for example, kallikreins (25).
Whole-body PSMA-TV was not significantly associated with primary Gleason scores (P = 0.32), as was to be expected. The size of metastases depends on other factors such as proliferation rate or previous treatment history. By contrast, whole-body TL-PSMA was independently associated with the initial Gleason score (rpartial = 0.33, P < 0.001). Besides volume, TL-PSMA also considers the degree of PSMA expression. In previous studies, high-level PSMA expression has been found in higher Gleason scores (26), providing an explanation for the correlation between Gleason score and TL-PSMA. However, the major determinant of TL-PSMA is also the patient’s individual course of the disease.
Considering potential applications of volumetric PSMA PET imaging, the prediction of therapy response of internal-emitter therapy may be an interesting option. The metastatic cure probability has been demonstrated to depend on the tumor size and the intratumoral activity concentration in radionuclide therapy influencing the absorbed dose (27). TL-PSMA may be an ideal parameter to account for both lesion size and intralesional PSMA expression when predicting metastatic cure. Moreover, treatment planning based on the extent of tumor burden has recently gained prominence in metastatic prostate cancer therapy (28,29). Several clinical trials have used tumor burden for stratification of patients into low- or high-volume disease. In a recent study that assessed whether ADT plus docetaxel would result in longer overall survival than ADT alone, the median overall survival was 17.0 mo longer in the combination group than in the ADT-alone group (49.2 vs. 32.2 mo) in the subgroup of patients with high-volume disease (28). In the absence of a sensitive imaging–derived biomarker, stratification was performed using suboptimal methods, for example, high volume was defined as the presence of visceral metastases or 4 bone lesions or more with 1 or more beyond the vertebral bodies and pelvis in the aforementioned study (28). In the Southwest Oncology Group trials, minimal disease was defined as disease confined to the spine, pelvic bones, or lymph nodes (29). These definitions can provide only an imprecise estimate of whole-body tumor burden. A more sophisticated approach using PSMA-TV or TL-PSMA may considerably refine stratification of patients, providing real volumetric parameters and a more accurate assessment of the tumor burden.
Assessment of volumetric parameters was time- and labor-intensive in this cohort with metastatic prostate cancer, and we therefore restricted the analysis to patients with 10 or fewer metastases. Although our approach consisting of manual placement of volumes of interest may also be used in patients with more than 10 lesions, other technical approaches may facilitate the assessment of volumetric parameters in patients with extensive disease, for example, fully automated, SUV threshold–based whole-body segmentation techniques that allow for a rapid definition of whole-body tumor burden (14).
Some limitations of the present study should be acknowledged. First, the study was retrospective in nature. Second, we evaluated a single threshold for calculation of PSMA-TV and TL-PSMA. It is important to keep in mind that volumetric data generated by PET represent an estimate of the true volume. Although we experimentally determined that a threshold of 45% provided the best results using our imaging and reconstruction protocol, and have used this threshold in previous studies (9), further refinement using different cutoff values, for example, 46% or 47%, may be beneficial. However, the observed correlations are robust and consistent with the literature. Moreover, the lesions chosen for the threshold assessment were representative of the total study population. The precise threshold used in this study may not be generalized to all types of acquisition protocols or reconstruction techniques but provides a proof of concept for volumetric assessment of prostate cancer lesions. Furthermore, ADT may alter PSMA expression by tumor cells and may potentially influence volumetric assessment based on an SUVmax threshold. Third, it would be desirable to obtain additional histopathologic specimens for assessment of the differentiation of metastatic lesions. After previous treatment, the initial Gleason score may not fully reflect the differentiation of metastases. However, this was not possible for both practical and ethical reasons. Finally, we demonstrated the feasibility of volumetric PSMA ligand PET and explored the relation of PSMA-TV and TL-PSMA with serum PSA levels. Future prospective studies will investigate the prognostic impact of these parameters in prostate cancer.
CONCLUSION
PSMA-derived volumetric parameters provide a quantitative imaging biomarker for whole-body tumor burden, capable of standardizing quantitative changes in PET imaging of patients with metastatic prostate cancer and of facilitating therapy monitoring. Volumetric assessment may allow better stratification of patients into low- and high-volume metastatic disease in clinical trials. Further evaluation will determine the potential prognostic impact of these PET-based parameters in metastatic prostate cancer.
DISCLOSURE
Prof. Dr. Hans-Jürgen Wester is a shareholder of Scintomics. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank James T. Thackeray, PhD, for his thorough revision and language editing of the manuscript.
Footnotes
Published online May 18, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 20, 2017.
- Accepted for publication May 10, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 99mTc-MIP-1404 SPECT/CT Companion Diagnostic for 177Lu-PSMA Therapy in Metastatic Castration-Resistant Prostate Cancer
- Prognostic Performance of RECIP 1.0 Based on [18F]PSMA-1007 PET in Prostate Cancer Patients Treated with [177Lu]Lu-PSMA I&T
- Prognostic Value of Tumor Volume Assessment on PSMA PET After 177Lu-PSMA Radioligand Therapy Evaluated by PSMA PET/CT Consensus Statement and RECIP 1.0
- Using 68Ga-PSMA-11 PET/CT for Therapy Response Assessment in Patients with Metastatic Castration-Resistant Prostate Cancer: Application of EAU/EANM Recommendations in Clinical Practice
- Assessing Response to 177Lu-PSMA Radioligand Therapy Using Modified PSMA PET Progression Criteria
- Intraprostatic Tumor Segmentation on PSMA PET Images in Patients with Primary Prostate Cancer with a Convolutional Neural Network
- Semiautomatically Quantified Tumor Volume Using 68Ga-PSMA-11 PET as a Biomarker for Survival in Patients with Advanced Prostate Cancer
- Disentangling inflammatory from fibrotic disease activity by fibroblast activation protein imaging
- qPSMA: Semiautomatic Software for Whole-Body Tumor Burden Assessment in Prostate Cancer Using 68Ga-PSMA11 PET/CT
- The Future of Nuclear Medicine as an Independent Specialty
- Validation of the Semiautomatic Quantification of 18F-Fluoride PET/CT Whole-Body Skeletal Tumor Burden
- Interobserver Agreement for the Standardized Reporting System PSMA-RADS 1.0 on 18F-DCFPyL PET/CT Imaging
- Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE): Proposed miTNM Classification for the Interpretation of PSMA-Ligand PET/CT