


Abstract
Prostate-specific membrane antigen (PSMA) is an excellent target for radionuclide therapy of metastasized castration-resistant prostate cancer (mCRPC). Besides high affinity and long tumor retention, the DOTA-conjugated ligand PSMA-617 has low kidney uptake, making it an excellent choice for therapeutic application. We retrospectively report our experience with 177Lu-PSMA-617–targeted radionuclide therapy in a case series of mCRPC patients resistant to other treatments. Methods: Patients with PSMA-positive tumor phenotypes were selected by molecular imaging. Thirty patients received 1–3 cycles of 177Lu-PSMA-617. During therapy, pharmacokinetics and radiation dosimetry were evaluated. Blood cell count was checked every 2 wk after the first and every 4 wk after succeeding cycles. Prostate-specific antigen (PSA) was determined every 4 wk. Radiologic restaging was performed after 3 cycles. Results: Twenty-one of 30 patients had a PSA response; in 13 of 30 the PSA decreased more than 50%. After 3 cycles, 8 of 11 patients achieved a sustained PSA response (>50%) for over 24 wk, which also correlated with radiologic response (decreased lesion number and size). Normally, acute hematotoxicity was mild. Diffuse bone marrow involvement was a risk factor for higher grade myelosuppression but could be identified by PSMA imaging in advance. Xerostomia, nausea, and fatigue occurred sporadically (<10%). Clearance of non–tumor-bound tracer was predominantly renal and widely completed by 48 h. Safety dosimetry revealed kidney doses of approximately 0.75 Gy/GBq, red marrow doses of 0.03 Gy/GBq, and salivary gland doses of 1.4 Gy/GBq, irrespective of tumor burden and consistent on subsequent cycles. Mean tumor-absorbed dose ranged from 6 to 22 Gy/GBq during cycle 1. Conclusion: 177Lu-PSMA-617 is a promising new option for therapy of mCRPC and deserves more attention in larger prospective trials.
Despite recent approval of some novel drugs, metastatic castration-resistant prostate cancer (mCRPC) remains a lethal disease and additional treatment options are still needed.
Prostate-specific membrane antigen (PSMA) is a promising target for directing new therapies. It is found in most prostate cancers (1), and its overexpression correlates with traditional adverse prognostic factors (2). Binding of a ligand leads to internalization via clathrin-coated pits (3) and prolonged retention in the cell. PSMA antibody–auristatin conjugates have been considered 1 option (4), but they face the inherent resistance of mCRPC against most (excepting taxanes) conventional chemotherapies. In contrast, prostate cancer is usually radiosensitive. Radiotherapy is a standard treatment for localized prostate cancer, for palliative management of mCRPC, and even radiopharmaceuticals targeting the surrounding bone matrix instead of the tumor itself can improve survival (5). Therefore, it seems more promising that a radioactive PSMA ligand, which is directly internalized into tumor cells, will be effective in delivering high doses for systemic endoradiotherapy. A phase 2 study using the radiolabeled antibody 177Lu-J591 already demonstrated moderate antitumor effects (6), but the slow diffusion of antibodies into solid lesions and hematotoxicity caused by a long circulation time in blood are limitations (7,8). Because of faster kinetics, the PSMA-targeted small-molecule MIP-1095, when labeled with 131I, demonstrated outcomes that were superior to the antibody approach with prostate-specific antigen (PSA) responses in 17 of 28 patients (9). Unfortunately, the coemission of high-energy photons from 131I requires elaborate radiation protection. Unlike 131I, 177Lu is a more pure β-particle emitter and preferable for clinical routine. The DOTA-conjugated PSMA-617 can be labeled with 177Lu-Lu3+ and was further refined in tumor-targeting with low nanomolar affinity in the range of 0.37 nM (NAALADase assay) and 2.34 nM (equilibrium dissociation constant on LNCaP) and highly efficient internalization with approximately 75% of the total cell associated activity internalized after 3 h of incubation on LNCaP (10–12).
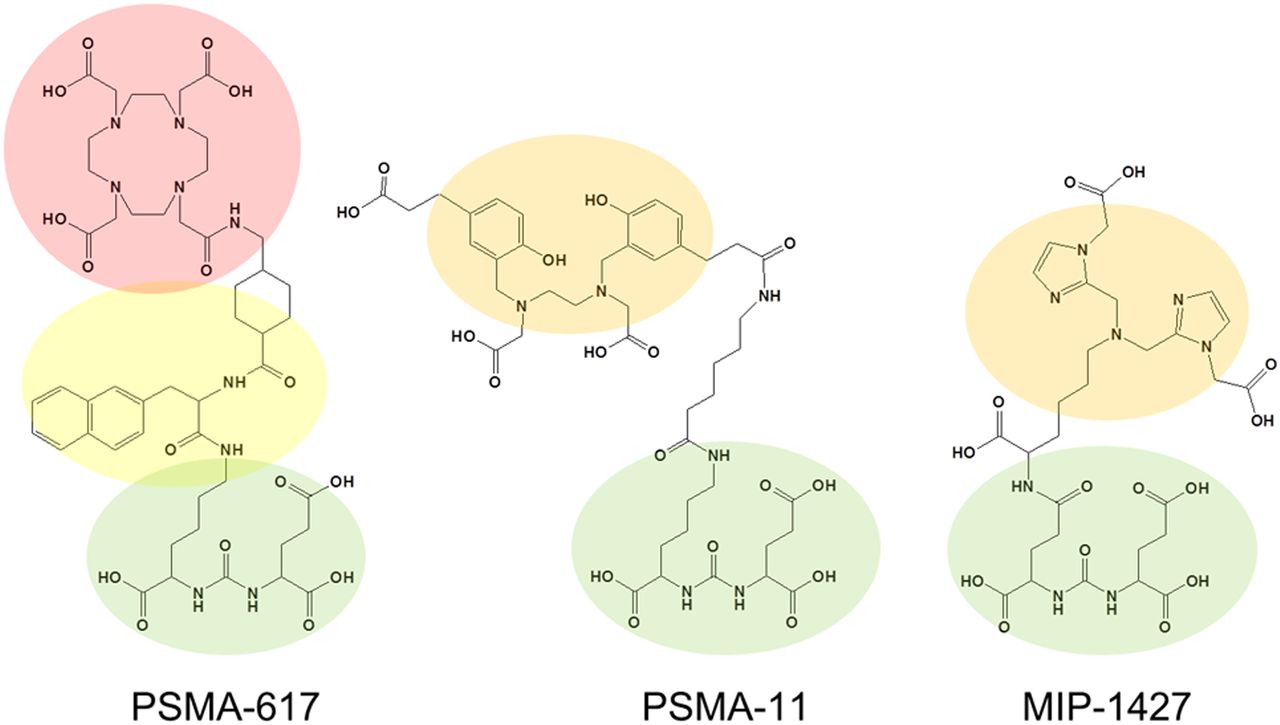
Here, we report our first clinical experience with 177Lu-PSMA-617 in patients with advanced mCRPC resistant to or with contraindications to other conventional therapies and PSMA-positive tumor phenotypes as demonstrated by molecular imaging using structurally related diagnostic analogs (Fig. 1). All used PSMA ligands share the Glu-urea motif for binding to the proteolytic domain and a lipophilic chelate or linker region to interact with the hydrophobic accessory pocket proposed by Bařinka et al. (13).

PSMA equals enzyme glutamate carboxypeptidase II. Its proteolytic domain can be targeted with Glu-urea motif (green). Hydrophobic pocket accessory to proteolytic domain adversely interacts with highly polar chelates such as DOTA (red) but favors more lipophilic chelates (orange) such as CIM (MIP-1427) for labeling with 99mTc or HBED-CC (PSMA-11) for labeling with 68Ga. In PSMA-617, aromatic linker (yellow) exploits lipophilic accessory pocket to keep more universal DOTA-chelate remote to Glu-urea binding site.
MATERIALS AND METHODS
Patients
177Lu-PSMA-617 was offered as surrogate therapy in accordance with the updated Declaration of Helsinki, paragraph-37 “Unproven Interventions in Clinical Practice,” and in accordance with German regulations for “compassionate use,” which includes priority of all approved treatments (without contraindications) and confirmation of the indication by both a nuclear medicine physician and an external expert in urology or oncology. In brief, all 30 patients were refractory to luteinizing hormone-releasing hormone analogs and antiandrogens (Table 1). Twenty-three patients underwent prior treatment with abiraterone or enzalutamide; 11 of them had received both. Fourteen patients were refractory to docetaxel; 4 had subsequently also been treated with cabazitaxel and 4 with estramustine. Six patients were pretreated with 223Ra. In contrast to a formal clinical trial, no systematic patient selection was performed, except all patients had to present with a PSMA-positive tumor phenotype based on PSMA imaging. All patients were informed about the experimental nature of this therapy and gave written informed consent. The institutional review board approved this retrospective study.
Patient Characteristics
Imaging-Based Patient Stratification
PSMA imaging was performed less than 4 wk before the first treatment cycle. Two different kinds of PSMA imaging were used before treatment.
Patients with a public health care provider (only reimbursement for scintigraphy) underwent planar scanning and dual-bed-position SPECT/CT (Infinity; GE Healthcare) covering the thorax/abdomen/pelvis 3 h after intravenous injection of 500–700 MBq of 99mTc-MIP1427 (50 nmol ligand). The precursor was produced in-house as previously described (14) and labeled according to the protocol described with minor modifications; in short the deprotected precursor was radiolabeled with the tricarbonyl method using the CRS Isolink kit (PSI). The intensity of tumor uptake was scored visually.
Patients with a commercial health care provider and reimbursement for PET/CT underwent PSMA PET/CT. This imaging was performed either in our department on a Biograph 6 PET/CT scanner (Siemens) at 1 h after injection of 150 MBq ±20% (2 nmol ligand) of 68Ga-PSMA-11 (15) or at outside PET centers before the patients were scheduled to receive therapy in our department. PSMA PET scans were quantified by measuring SUVmax for the hottest bone, soft-tissue, and lymph node metastasis (as prospectively defined index lesions), respectively.
177Lu Labeling of PSMA-617
The precursor PSMA-617 was synthesized as described previously (10) or was obtained from ABX advanced biochemical compounds and dissolved with dimethyl sulfoxide to obtain a 10 mM solution. Two microliters (20 nmol) of this solution were used per 1 GBq of 177Lu-LuCl3 (NEZ307D [Perkin Elmer], 0.04 M HCl) mixed with 1.25 μL of 20% ascorbic acid and 100 μL of 0.4 M sodium acetate buffer (pH 5; adjusted with acetic acid) and injected directly into the 177Lu-LuCl3 delivery vial. After being heated to 95°C for 10 min, a quality check per reversed-phase high-performance liquid chromatography and instant thin-layer chromatography was performed, and the final product was diluted in 2 mL of 0.9% NaCl.
Pharmacokinetics and Dosimetry
Thorough descriptions of the methods used for evaluation of pharmacokinetics and dosimetry are provided in the supplemental materials (available at http://jnm.snmjournals.org).
Treatment Regime and Follow-up
According to German radiation protection laws, the patients were treated as in-patients on the nuclear medicine ward until 48 h after injection. Clinical examination was performed before and 1 d after therapy. Patients received intravenous hydration (2,000 mL of 0.9% NaCl; flow, 333 mL/h) starting 30 min before therapy. The therapy solution was administered with a slow (30–60 s) freehand injection through a 0.20-μm sterile filter with low protein binding (Filtropur S 0.2; Sarstedt). Our initial treatment regime was based on 3.7–4.0 GBq per cycle repeated every 2 mo, which was derived from data with 131I-MIP1095 (9). Once first ligand-specific dosimetry data became available for 177Lu-PSMA-617, the dose was increased to 6 GBq per cycle. An overview of the administered activities is provided in Table 1. After the first cycle, blood cell count was done every 2 wk, and during the succeeding cycles at least every 4 wk. Serum creatinine, blood-urea-nitrogen, liver enzymes, and PSA were checked every 4 wk. Baseline and follow-up values of laboratory tests were classified into toxicity gradings using the Common Terminology Criteria for Adverse Events 3.0 (16). After 3 cycles, imaging-based restaging was performed with either 68Ga-PSMA11 PET/CT or 99mTc-MIP1427 SPECT/CT as available baseline.
RESULTS
Pharmacokinetics
The initial volume of distribution 1 h after injection was 22 ± 12 L, which approximates extracellular body water (17). Comparison of full-blood samples and serum revealed that there was neither a relevant passive diffusion of PSMA-617 into cellular blood components nor absorption at their surface. Blood clearance could be fitted biexponentially with half-lives of 4 and 95 h (Supplemental Fig. 1A), interpretable as fast clearance from extracellular body water and a slow clearance averaged from organs with specific uptake (including tumor tissue) assuming equilibrium between blood and the particular compartment, respectively. Approximately 50% of the injected activity was eliminated by urine during the first 48 h, then the cumulative clearance curve reached a plateau (Supplemental Fig. 1B). The intestine presented maximum contrast in the 20-h postinjection image, followed by a normal colon passage speed. Approximately 1%–5% of the injected dose was eliminated by fecal excretion.
After 48 h, the direct γ-emission was less than 2 μSv/h at 2 m distance for all patients. Because of the observation that urine clearance of non–tumor-bound PSMA-617 is almost completed 48 h after injection and clearance from the intestine can be stimulated with moderate laxatives administered 24 h after 177Lu-PSMA-617, all patients could be discharged after 48 h in accordance with our currently valid radiation protection regulations (18).
Dosimetry
The dosimetry analyses of 4 patients during their first and second treatment cycles revealed a mean (±SD) kidney dose of 0.75 ± 0.19 Gy/GBq of 177Lu-PSMA-617. The red marrow dose was 0.03 ± 0.01, parotid 1.28 ±0.40, and submandibular gland 1.48 ±0.37 Gy/GBq. There was no relevant difference in dosimetry for the patients with low or high tumor load. In addition, there was no relevant difference in the kidney and red marrow dose between the first and second treatment cycle. Distinct values and additional (not dose-limiting) organs are presented in Table 2. The red marrow dose consists of an approximately 45% self-dose—that is, β-radiation during perfusion and passive diffusion into the interstitial space—and 55% spill-in radiation (5% from the delineable source organs, 50% from the remainder body including tumor lesions).
Dosimetry
Treatment Efficacy
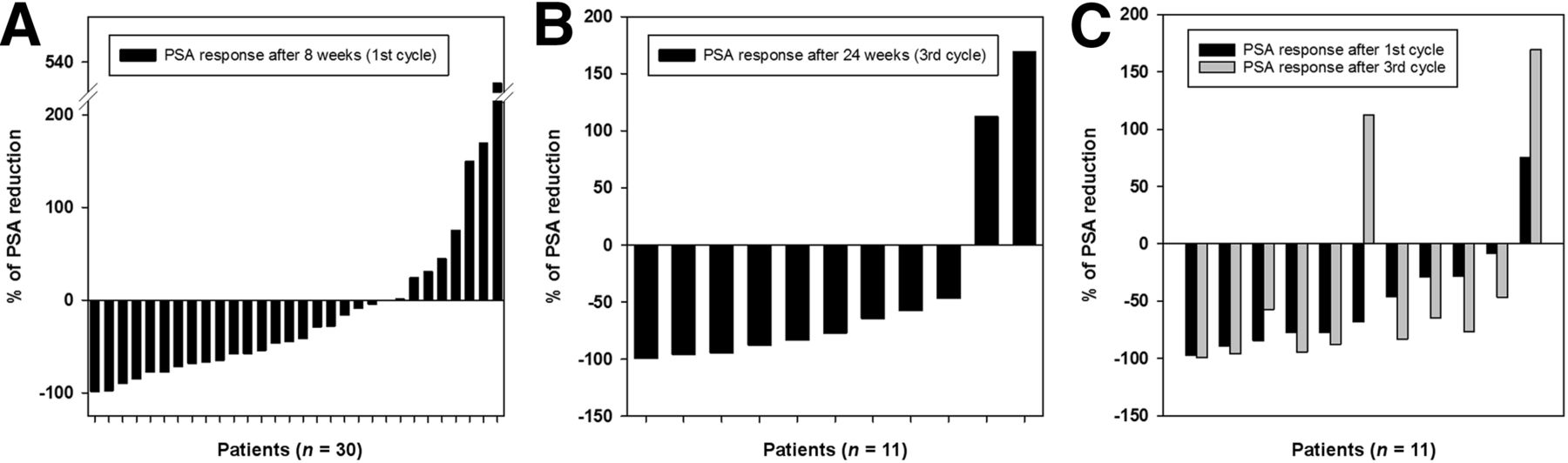
Eight weeks after the first treatment cycle, 21 of 30 patients demonstrated a decrease in PSA; in 18 patients the decrease was more than 25% and in 13 patients more than 50%. However, 8 patients demonstrated a rising PSA and 1 patient remained stable (Fig. 2A). After 24 wk, that is, nearly 6 mo after initial therapy, 9 of 11 patients receiving 3 treatment cycles presented with a sustained decrease in PSA in comparison to the baseline value; the decrease was more than 25% for all of these 9 patients and more than 50% in 8 patients (Fig. 2B). Follow-up between the week-8 and week-24 PSA response (Fig. 2C) revealed that in 8 of 11 patients the PSA levels further decreased from cycle 1 to cycle 3. One patient who already presented with PSA progression after the first cycle continued therapy because of favorable symptomatic response and had further PSA progression after the third cycle. Two patients initially responded to cycle 1 but had PSA relapse by cycle 3; however, in one of these patients the PSA was still less than 50% in comparison to baseline. In these patients, imaging findings also demonstrated partial remission in comparison to baseline staging.

(A) Waterfall graph presenting PSA response after 1 cycle of 177Lu-PSMA-617 therapy. (B) Waterfall graph presenting PSA response after 3 cycles of therapy. (C) Follow-up between PSA response after cycle 1 and cycle 3.
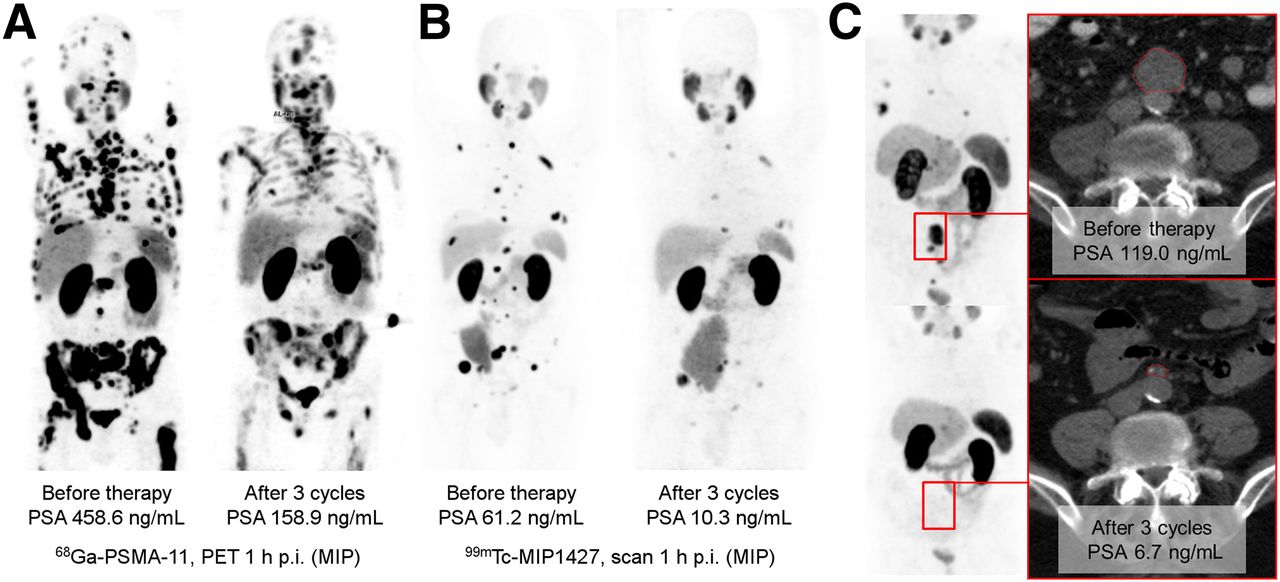
Imaging-based restaging revealed a positive response in 10 of the 11 patients; surprisingly, a positive imaging response was even found in 1 of the 2 patients with rising PSA. Six patients were restaged with PSMA PET/CT, and all presented with a decrease of more than 50% (average of index lesions) in SUVmax (Fig. 3A). Three patients were assessed with 99mTc-PSMA SPECT/CT and presented with visual response (Fig. 3B). In patients with soft-tissue or lymph node metastases (target lesions according to RECIST), response was additionally demonstrated with CT (Fig. 3C). Also, the posttherapeutic emission scans based on the inherent imaging capabilities of 177Lu (coemission of γ-radiation) seem sufficient to monitor treatment response despite a minimal lower resolution and higher noise (Fig. 4). Because of the multitude of lesions, we did not assess the exact lesion number; as long as the total number of delineable metastases decreased by visual estimation, the situation was considered a radiologic response. Thus, similar to the use of bone scans in clinical trials (19), single new lesions were not considered progressive disease.
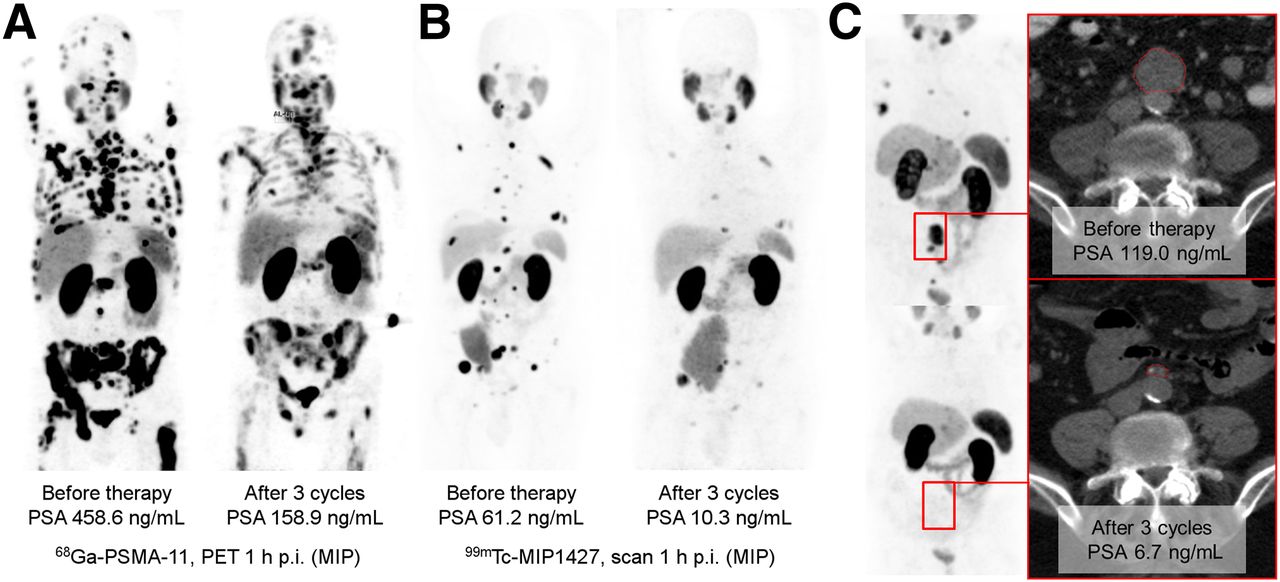
Imaging-based response evaluation. (A) 68Ga-PSMA-11 PET was evaluated semiquantitatively. (B) 99mTc-MIP1427 scintigraphy–enabled visual evaluation. (C) If target lesions were available, CT was evaluated in accordance to RECIST. GM = geometric mean; MIP = maximum-intensity projection; p.i. = after injection.
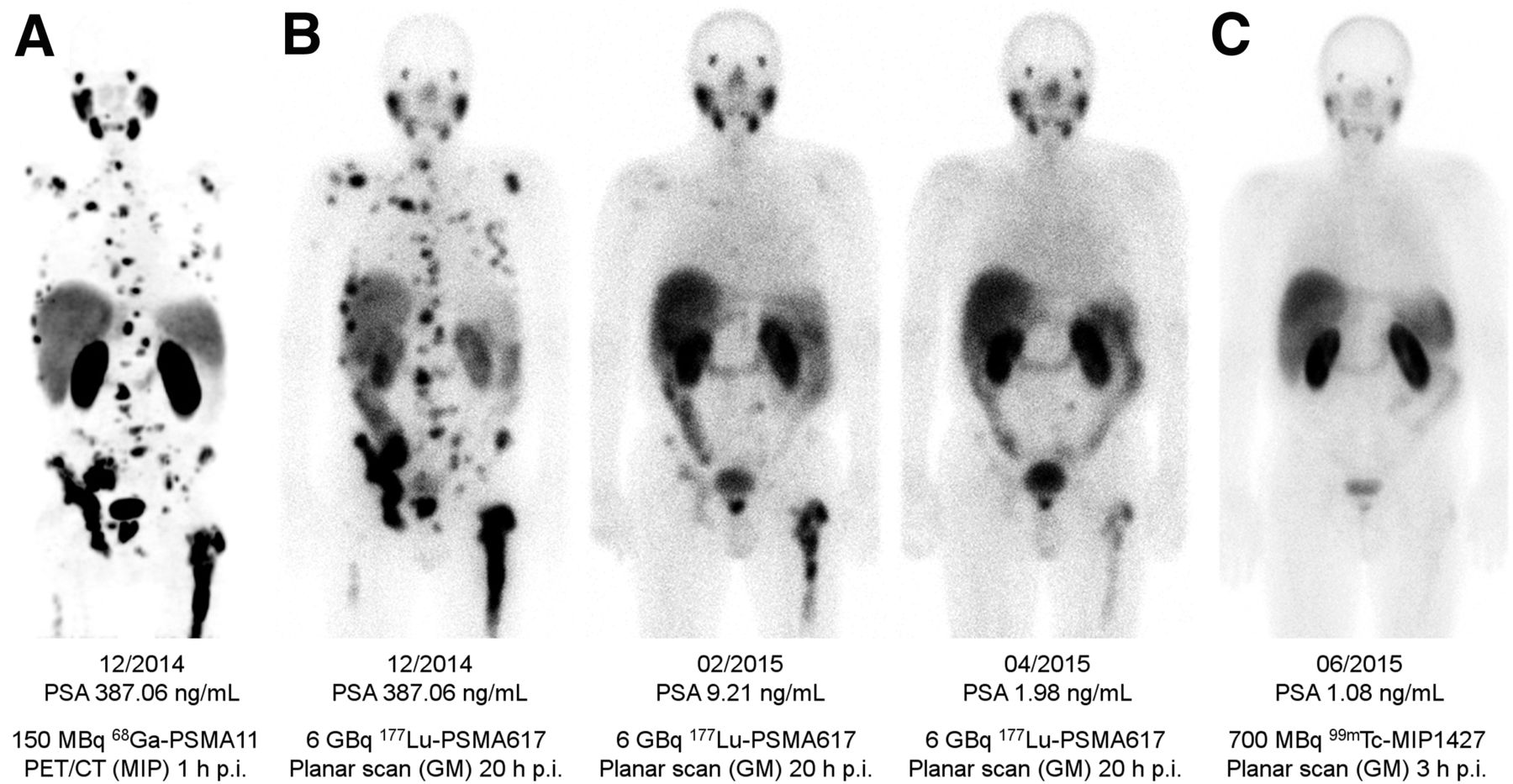
(A) PSMA PET/CT delivers highest resolution. (B) Coemission of γ-rays enables imaging during therapy. (C) 99mTc-PSMA scintigraphy has minimally less noise than posttherapy scanning and can be used for imaging follow-up in out-patient setting. GM = geometric mean; MIP = maximum-intensity projections; p.i. = after injection.
Clinically, the treatment was able to stabilize the patient’s well-being. None of the patients discontinued treatment because of a worsening of their general clinical condition. The body weight remained fairly stable (mean body weight at baseline, 83 kg; at week 24, 81 kg). None of the 24 of 30 patients without opioid analgesics at baseline had to start such a medication during follow-up. The dose of the 6 of 30 patients with opioid analgesics at baseline remained stable.
Treatment Toxicity
Creatinine and urea as well as liver enzymes were not significantly changed during the complete follow-up period, which was 12 wk for the 19 patients receiving 1 treatment cycle and 24 wk for the 11 patients receiving 3 treatment cycles. Thus, follow-up was sufficient to report acute and midterm toxicities but not late effects.
Among 15 patients with normal baseline hemoglobin, 6 patients developed grade I anemia, and 9 had no red cell toxicity. In 10 patients with grade I anemia before therapy, only 3 patients had a decline to grade II, 6 patients remained stable, and 1 patient improved to the reference range (this patient simultaneously presented with striking radiologic improvement of bone metastases). For 3 patients who already had grade II anemia at baseline, 1 worsened to grade III (after only 1 treatment cycle), 1 was stable, and 1 improved to grade I. In comparison to baseline, 18 of 27 patients had no worsening of anemia (66%) and 9 worsened by 1 grade (33%); no patient had a decline of more than 1 grade. The only patient with grade III anemia had diffuse-pattern bone marrow involvement on pretherapeutic imaging. Two patients had already received substitution of erythrocytes less than 6 wk before PSMA therapy and were omitted from evaluation of anemia.
With regard to white blood cell count (Fig. 5A), 22 patients never developed Common Terminology Criteria for Adverse Events toxicity higher than baseline. Grade I leucopenia was observed in 6 patients mainly after the third cycle. Grade II was observed in 2 patients, both with diffuse-pattern bone marrow involvement.
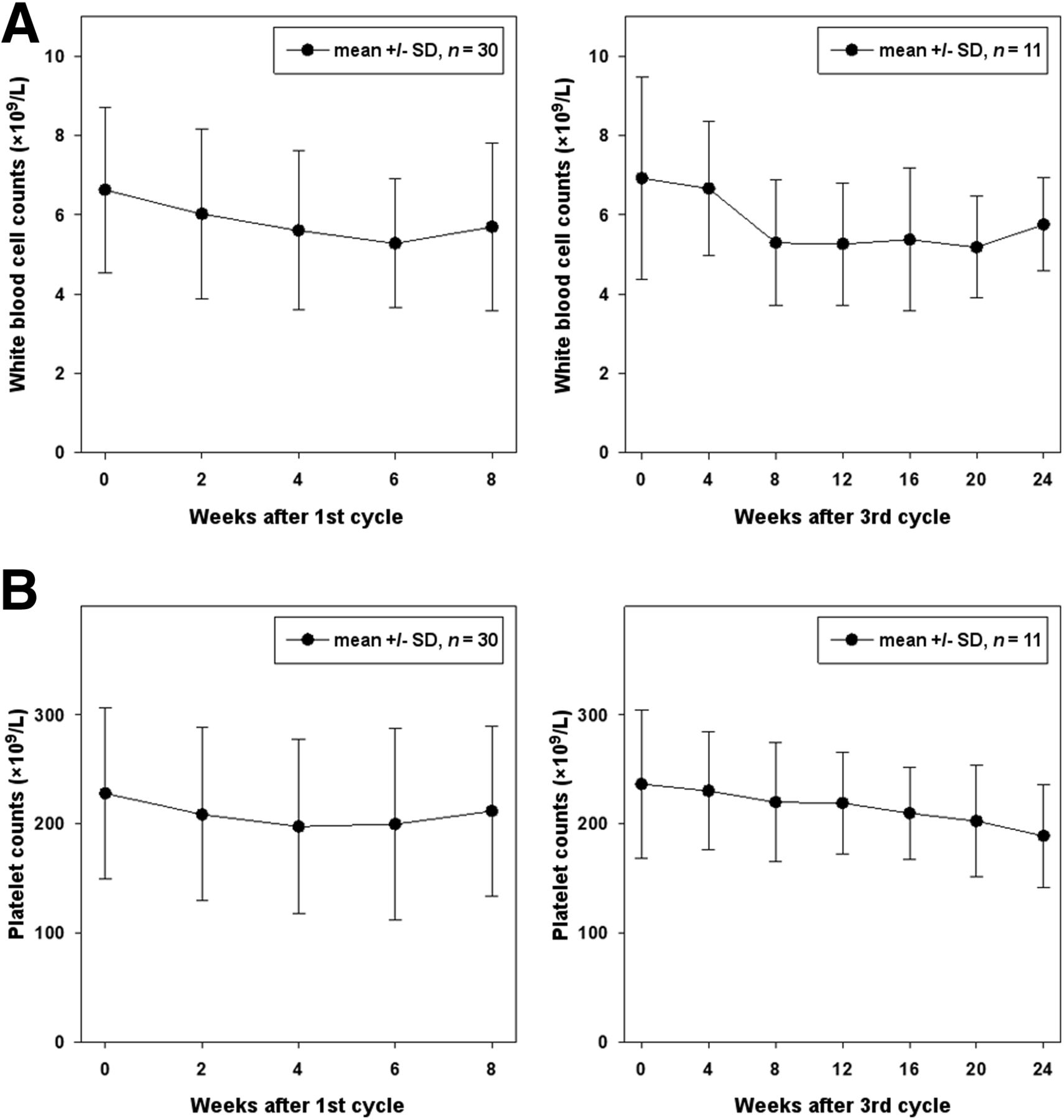
Course of white blood cell count (A) and platelets (B) during 177Lu-PSMA-617 therapy.
Platelet count (Fig. 5B) demonstrated high interindividual variability. However, in 23 patients the absolute platelet count never dropped below the reference range. In 4 patients, grade I thrombocytopenia was observed. One patient developed grade II and 1 patient grade III thrombocytopenia. Both patients had previously presented with diffuse-pattern bone marrow infiltration during imaging and were the same patients who developed the highest white blood cell toxicity. In 1 patient, grade IV thrombocytopenia was already present at baseline. Despite the fact that the absolute platelet count stayed within the reference range (150–300/nL) for 23 of 30 patients, we observed a relative decline in the mean platelet count of −14%, with nadir 4–6 wk after the first therapy that recovered after 8 wk. However, in the 11 patients receiving 3 cycles we found a chronic decrease of platelets (−20%) from baseline to week 24.
Most of the patients reported no relevant dysfunction of salivary glands. Substitution of saliva (spray/gel) was prescribed to 2 of 30 patients; both developed xerostomia after the third cycle. After the first and second treatment cycle only temporal xerostomia without relevant loss in quality of life was occasionally reported. Mild fatigue over baseline was regularly reported, but only 2 times was it attributed to affecting activities of daily living. Nausea and loss of appetite during the first weeks after therapy were reported infrequently.
DISCUSSION
Here, we report our clinical experience with 177Lu-PSMA-617, which revealed antitumor activity in most patients with mild to moderate toxicities.
In contrast to conventional pharmaceuticals, the toxicity and response probability of a radiopharmaceutical predominantly depends on the radiation absorbed dose to healthy and tumor tissue, respectively. There are well-defined radiation tolerance limits for normal organs. Therefore, empiric dose escalation studies can partially be omitted and dosing of radioactive drugs can be based on dosimetry. Our dosimetry data are well in line with 2 other recent investigations (20,21). The highest normal-organ dose was found for the salivary glands. Thus, the sporadic incidence of reversible xerostomia, which was mainly observed after the third cycle, is reasonable, taking into account published radiation tolerance limits (22). However, if mild xerostomia is considered to be an annoying but harmless side effect, kidneys are the only essential dose-limiting organs and their tolerance limits would permit about twice the cumulative dose—that is, 36 GBq of 177Lu-PSMA-617 (23)—which conversely would still stay below the limits to provoke severe and irreversible xerostomia (22). Additionally, recent attempts to reduce kidney uptake of PSMA ligands raise hope to further increase the therapeutic index (24). Selecting the ideal single fraction dose is more challenging because bone marrow reserve can be reduced after previous chemotherapy, and the published tolerance limits are not reliable (25). Also dosimetry can underestimate red marrow dose because the β-radiation arising from bone metastases cannot be sufficiently modeled. The 497-keV β-energy of 177Lu corresponds to a mean and maximum tissue range of only 0.5 and 2 mm (i.e., 10–50 cell diameters), respectively, and it is plausible to neglect this dose contribution if only a limited number of solid bone metastases are present. However, it might be relevant in the case of diffuse bone marrow involvement. Therefore, we initially administered conservative 4-GBq fractions. Once it became clear that only diffuse-type bone marrow involvement, eventually in combination with previous chemotherapy, presented a risk factor for higher hematotoxicity, we escalated to 6 GBq and patients with diffuse-pattern bone marrow involvement were subsequently stratified to receive PSMA-617 labeled with an α-emitter. Targeted α-radiation therapy was already demonstrated to reduce red marrow toxicity in similar situations (26). However, the reliability of this tailored approach has still to be proven. Despite moderate acute hematotoxicity, we observed a chronic decline of platelets during 3 cycles, thus further dose escalations of 177Lu-PSMA-617 should be conducted cautiously. Nevertheless, there is still some room to improve the treatment regime.
The main limitation of this report is that the patients were not systematically selected in a prospective manner with stringent inclusion criteria such as in a typical clinical trial. Therefore, the results of this retrospective evaluation should be considered only explorative. Nevertheless, the findings are noteworthy in view of the high number of prior treatments seen by our patients before receiving 177Lu-PSMA-617. The novel mCRPC agents have been approved with hormone therapy (Cougar-302, PREVAIL) or hormone and docetaxel (Cougar-301, AFFIRM, TROPIC) being the only pretreatments (27). In contrast, if the novel drugs are applied consecutively, the more than 50% PSA response rate is commonly less than 40% (28). Our cohort is high risk, with negative prognostic factors such as high Gleason score and visceral metastases (29), making the high response rate with the absence of severe toxicity all the more remarkable.
It has been reported that tubulin-targeting with taxanes inhibits androgen receptor nuclear translocation (30). Because abiraterone or enzalutamide also interfere with androgen receptor signaling, these drugs are somehow competitive in their mechanism of action and cross resistance may occur, making optimal sequencing of the new drugs challenging (28,30). In contrast, PSMA genes are suppressed by androgens, and androgen independency as well as androgen-deprivation therapy may even increase the expression of PSMA in mCRPC (31,32). Thus, PSMA targeting is rather complementary to the currently approved drugs and can still be effective when targeting the androgen receptor axis fails. This would explain the high rate of radiologic and PSA responses despite excessive pretreatment.
On the other hand, the reported patients include some selection bias. Patients with diffuse bone marrow involvement were excluded, once it became apparent that these patients have a higher probability to develop hematotoxicity. Additionally, a PSMA-positive tumor phenotype based on PET or scintigraphy was a precondition to receive therapy. However, treatment stratification based on prognostic factors is a desired objective in modern oncology, and it is beneficial that PSMA-positive tumors can be easily identified noninvasively with PSMA imaging (33). In addition, a diagnostic study with PSMA PET/CT found PSMA-positive tumor phenotypes in 88% of prostate cancer relapses, suggesting that most mCRPC patients may be potential candidates for PSMA-targeted therapy (34).
CONCLUSION
177Lu-PSMA-617 is a new treatment option for mCRPC that demonstrates substantial antitumor activity with few side effects. 177Lu-PSMA-617, therefore, deserves more attention in larger prospective trials.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This research was supported by the Klaus-Tschira-Stiftung (project no. 00.198.2012). There is a patent pending for PSMA-617 (Martina Benešová, Matthias Eder, Klaus Kopka, and Uwe Haberkorn). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 16, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 16, 2015.
- Accepted for publication February 18, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Best Patient Care Practices for Administering PSMA-Targeted Radiopharmaceutical Therapy
- Dosimetry of [177Lu]Lu-PSMA-Targeted Radiopharmaceutical Therapies in Patients with Prostate Cancer: A Comparative Systematic Review and Metaanalysis
- Deescalated 225Ac-PSMA-617 Versus 177Lu/225Ac-PSMA-617 Cocktail Therapy: A Single-Center Retrospective Analysis of 233 Patients
- Renal and Multiorgan Safety of 177Lu-PSMA-617 in Patients with Metastatic Castration-Resistant Prostate Cancer in the VISION Dosimetry Substudy
- Tandem Isotope Therapy with 225Ac- and 177Lu-PSMA-617 in a Murine Model of Prostate Cancer
- Optimized Methods for the Production of High-Purity 203Pb Using Electroplated Thallium Targets
- Evolution of Models of Prostate Cancer: Their Contribution to Current Therapies
- Novel Framework for Treatment Response Evaluation Using PSMA PET/CT in Patients with Metastatic Castration-Resistant Prostate Cancer (RECIP 1.0): An International Multicenter Study
- Effects of 225Ac-Labeled Prostate-Specific Membrane Antigen Radioligand Therapy in Metastatic Castration-Resistant Prostate Cancer: A Meta-Analysis
- Pretherapeutic Comparative Dosimetry of 177Lu-rhPSMA-7.3 and 177Lu-PSMA I&T in Patients with Metastatic Castration-Resistant Prostate Cancer
- The History of Prostate-Specific Membrane Antigen as a Theranostic Target in Prostate Cancer: The Cornerstone Role of the Prostate Cancer Foundation
- An Improved 211At-Labeled Agent for PSMA-Targeted {alpha}-Therapy
- Radionuclide Therapy in Prostate Cancer: From Standalone to Combination PSMA Theranostics
- Dosimetry in Clinical Radiopharmaceutical Therapy of Cancer: Practicality Versus Perfection in Current Practice
- To Scan or Not to Scan: An Unnecessary Dilemma for PSMA Radioligand Therapy
- Safety of PSMA-Targeted Molecular Radioligand Therapy with 177Lu-PSMA-617: Results from the Prospective Multicenter Phase 2 Trial RESIST-PC (NCT03042312)
- TriTACs, a Novel Class of T-Cell-Engaging Protein Constructs Designed for the Treatment of Solid Tumors
- 177Lu-EB-PSMA Radioligand Therapy with Escalating Doses in Patients with Metastatic Castration-Resistant Prostate Cancer
- Digital Solid-State SPECT/CT Quantitation of Absolute 177Lu Radiotracer Concentration: In Vivo and In Vitro Validation
- 177Lu-NM600 Targeted Radionuclide Therapy Extends Survival in Syngeneic Murine Models of Triple-Negative Breast Cancer
- Radiation Dosimetry in 177Lu-PSMA-617 Therapy Using a Single Posttreatment SPECT/CT Scan: A Novel Methodology to Generate Time- and Tissue-Specific Dose Factors
- JHU-2545 Selectively Shields Salivary Glands and Kidneys during PSMA-Targeted Radiotherapy
- Long-Term Follow-up and Outcomes of Retreatment in an Expanded 50-Patient Single-Center Phase II Prospective Trial of 177Lu-PSMA-617 Theranostics in Metastatic Castration-Resistant Prostate Cancer
- Theranostics: Leveraging Molecular Imaging and Therapy to Impact Patient Management and Secure the Future of Nuclear Medicine
- Hybrid Tracers Based on Cyanine Backbones Targeting Prostate-Specific Membrane Antigen: Tuning Pharmacokinetic Properties and Exploring Dye-Protein Interaction
- Development of Novel PSMA Ligands for Imaging and Therapy with Copper Isotopes
- Imaging Patients with Metastatic Castration-Resistant Prostate Cancer Using 89Zr-DFO-MSTP2109A Anti-STEAP1 Antibody
- Is the Vision of Radioligand Therapy for Prostate Cancer Becoming a Reality? An Overview of the Phase III VISION Trial and Its Importance for the Future of Theranostics
- 177Lu-PSMA-617 Radioligand Therapy in Metastatic Castration-Resistant Prostate Cancer Patients with a Single Functioning Kidney
- Effect of External Cooling on 177Lu-PSMA Uptake by the Parotid Glands
- First Clinicopathologic Evidence of a Non-PSMA-Related Uptake Mechanism for 68Ga-PSMA-11 in Salivary Glands
- Clinical Outcomes of 177Lu-PSMA Radioligand Therapy in Earlier and Later Phases of Metastatic Castration-Resistant Prostate Cancer Grouped by Previous Taxane Chemotherapy
- Dosimetry Estimate and Initial Clinical Experience with 90Y-PSMA-617
- Modeling and Predicting Tumor Response in Radioligand Therapy
- The Relevance of Dosimetry in Precision Medicine
- Detection Threshold and Reproducibility of 68Ga-PSMA11 PET/CT in a Mouse Model of Prostate Cancer
- Predictive Factors of Response and Overall Survival in Patients with Castration-Resistant Metastatic Prostate Cancer Undergoing 177Lu-PSMA Therapy
- The Effect of Total Tumor Volume on the Biologically Effective Dose to Tumor and Kidneys for 177Lu-Labeled PSMA Peptides
- Targeted {alpha}-Therapy of Metastatic Castration-Resistant Prostate Cancer with 225Ac-PSMA-617: Swimmer-Plot Analysis Suggests Efficacy Regarding Duration of Tumor Control
- PSMA-Targeted Radionuclide Therapy and Salivary Gland Toxicity: Why Does It Matter?
- Low-Level Endogenous PSMA Expression in Nonprostatic Tumor Xenografts Is Sufficient for In Vivo Tumor Targeting and Imaging
- Repeated 177Lu-Labeled PSMA-617 Radioligand Therapy Using Treatment Activities of Up to 9.3 GBq
- Why Targeting PSMA Is a Game Changer in the Management of Prostate Cancer
- Establishing 177Lu-PSMA-617 Radioligand Therapy in a Syngeneic Model of Murine Prostate Cancer
- Targeted {alpha}-Therapy of Metastatic Castration-Resistant Prostate Cancer with 225Ac-PSMA-617: Dosimetry Estimate and Empiric Dose Finding
- Dual-Target Binding Ligands with Modulated Pharmacokinetics for Endoradiotherapy of Prostate Cancer
- Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy
- Glu-Ureido-Based Inhibitors of Prostate-Specific Membrane Antigen: Lessons Learned During the Development of a Novel Class of Low-Molecular-Weight Theranostic Radiotracers
- 177Lu-PSMA Radioligand Therapy for Prostate Cancer
- Acceleration of PSMA-Targeted Theranostics to the Clinic: Can Common Sense Prevail?
- Why Targeting of PSMA Is a Valuable Addition to the Management of Castration-Resistant Prostate Cancer: The Urologists Point of View
- Semiquantitative Parameters in PSMA-Targeted PET Imaging with 18F-DCFPyL: Variability in Normal-Organ Uptake
- 68Ga-PSMA-11 PET as a Gatekeeper for the Treatment of Metastatic Prostate Cancer with 223Ra: Proof of Concept
- Preclinical Evaluation of 18F-PSMA-1007, a New Prostate-Specific Membrane Antigen Ligand for Prostate Cancer Imaging
- Radiation Dosimetry for 177Lu-PSMA I&T in Metastatic Castration-Resistant Prostate Cancer: Absorbed Dose in Normal Organs and Tumor Lesions
- Predictors of Response to Radioligand Therapy of Metastatic Castrate-Resistant Prostate Cancer with 177Lu-PSMA-617
- 68Ga-PSMA-11 PET Imaging of Response to Androgen Receptor Inhibition: First Human Experience
- German Multicenter Study Investigating 177Lu-PSMA-617 Radioligand Therapy in Advanced Prostate Cancer Patients
- PSMA-Based Radioligand Therapy for Metastatic Castration-Resistant Prostate Cancer: The Bad Berka Experience Since 2013
- The Rise of PSMA Ligands for Diagnosis and Therapy of Prostate Cancer
- Imaging approaches to optimize molecular therapies