


Abstract
We investigated radiation exposure of patients undergoing whole-body 18F-FDG PET/CT examinations at 4 hospitals equipped with different tomographs. Methods: Patient doses were estimated by using established dose coefficients for 18F-FDG and from thermoluminescent measurements performed on an anthropomorphic whole-body phantom. Results: The most relevant difference between the protocols examined was the incorporation of CT as part of the combined PET/CT examination: Separate low-dose CT scans were acquired at 2 hospitals for attenuation correction of emission data in addition to a contrast-enhanced CT scan for diagnostic evaluation, whereas, at the other sites, contrast-enhanced CT scans were used for both purposes. Nevertheless, the effective dose per PET/CT examination was similar, about 25 mSv. Conclusion: The dosimetric concepts presented in this study provide a valuable tool for the optimization of whole-body 18F-FDG PET/CT protocols. Further reduction of patient exposure can be achieved by modifications to the existing hardware and software of PET/CT systems.
In recent years, PET has gained increasing clinical acceptance as an important functional imaging modality. However, accurate localization and interpretation of tissue structures with increased radiotracer uptake—particularly, in the abdomen or pelvis—are frequently challenged by the limited spatial resolution of PET and the absence of clearly visible anatomic landmarks in the PET images (1).
The development of dual-modality PET/CT systems has addressed these problems (2). These systems allow the quasisimultaneous acquisition of anatomic (CT) and functional (PET) information of a patient within a single examination and, thus, provide intrinsically coregistered images of the 2 modalities (3–5). In addition, the “hardware” fusion concept offers the possibility of CT-based attenuation correction of the emission scans instead of using noisy transmission data measured separately by means of an external positron-emitting source (6). The use of CT-based attenuation correction results not only in a marked reduction of the total examination time but also in an improved quality of the corrected PET scans (5,7,8).
On the other hand, whole-body PET/CT examinations incur an increased patient exposure compared with an individual CT or PET examination (8). Thus, patient referral for PET/CT studies must be justified in each case to avoid repeated exposure or overexposure of patients (9). Besides justification, optimization is the second general principle in radiologic protection (10). It was, therefore, the aim of the present study (a) to evaluate radiation exposure of patients undergoing whole-body PET/CT examinations after administration of 18F-FDG, (b) to derive a practical dosimetric concept for dose estimation in whole-body CT, and (c) to discuss strategies for dose reduction to decrease radiation risks to patients.
MATERIALS AND METHODS
We reviewed whole-body PET/CT acquisition protocols used between September 2003 and May 2004 in 4 German university hospitals. Table 1 summarizes the main technical details of the 4 different PET/CT models installed in these hospitals. 18F-FDG PET scans were characterized by the administered activity and the scan time; CT scans were characterized by the tube potential U, electrical current-time product Qel, volume CT dose index CTDIvol, scan length L, slice collimation hcol, and pitch factor p.
Characterization of 4 PET/CT Tomographs Considered in This Study
Internal Exposure
Absorbed doses DT to a tissue or organ T resulting from intravenous administration of an activity A of 18F-FDG were computed by means of dose coefficients ΓTFDG provided by the International Commission on Radiological Protection (ICRP) in its Publication 80 (11) for a variety of organs and tissues of the adult hermaphrodite MIRD phantom—that is, DT = A·ΓTFDG. Effective doses were estimated by:
 Eq. 1 where ΓEFDG = 19 μSv/MBq is the dose coefficient for the effective dose and wT are the tissue weighting factors (∑T wT = 1) given in ICRP Publication 60 (12).
Eq. 1 where ΓEFDG = 19 μSv/MBq is the dose coefficient for the effective dose and wT are the tissue weighting factors (∑T wT = 1) given in ICRP Publication 60 (12).
External Exposure
To estimate radiation exposure of patients resulting from the acquisition of topograms and scans in CT, dose measurements were performed on an anthropomorphic whole-body Alderson RANDO phantom (Alderson Research Laboratories Inc.) using thermoluminescent dosimeters (TLDs). The method has been described in detail in a previous article (13). In brief, at least 180 dosimeters (TLD-100; Bicron-Harshaw) were suitably distributed inside and at the surface of the phantom. For smaller organs, absorbed doses were obtained by averaging the TLD values measured within the specified organs, whereas, for extended organs (e.g., skin and bone), they were estimated using specific weighting factors for the various cross sections of the Alderson phantom. The effective dose E was calculated from the absorbed doses DT according to Equation 1.
In analogy to the formalism presented for the case of internal dosimetry, organ doses were described by:
 Eq. 2 where ΓTCT is an organ-specific dose coefficient that relates the volume CT dose index CTDIvol—that is, the average dose for a standardized CT dosimetry phantom—with the organ dose DT. Variations in the organ doses with tube potential are considered by using the CTDIvol value indicated for the specific CT scan on the operators’s console of the scanner. Organ-specific dose coefficients were estimated according to Equation 2, using the organ doses derived from the TLD measurements on the Alderson phantom and the corresponding CTDIvol values.
Eq. 2 where ΓTCT is an organ-specific dose coefficient that relates the volume CT dose index CTDIvol—that is, the average dose for a standardized CT dosimetry phantom—with the organ dose DT. Variations in the organ doses with tube potential are considered by using the CTDIvol value indicated for the specific CT scan on the operators’s console of the scanner. Organ-specific dose coefficients were estimated according to Equation 2, using the organ doses derived from the TLD measurements on the Alderson phantom and the corresponding CTDIvol values.
RESULTS
Table 2 gives an overview of the routine acquisition protocols used for whole-body 18F-FDG PET/CT examinations at the 4 university hospitals (designated H1–H4). For each protocol, the type and sequence of the various scans performed as well as the effective doses per scan and examination are listed. In hospital H3, a high-quality protocol is used in the majority of cases. However, in cases in which a recent diagnostic CT scan exists, the high-quality diagnostic CT scan (D-CT) is replaced by a low-dose scan acquired without intravenous contrast medium (LD-CT). At sites H2 and H4, no high-quality diagnostic CT scan is performed as part of the combined PET/CT examination in such cases. The effective dose values for the 4 high-quality PET/CT protocols (Table 2) were nearly identical. The uterine dose, which is often used to estimate exposure to an embryo in the early stage of pregnancy, was between 20.9 and 23.2 mGy.
Summary of Representative Protocols Used Routinely for Whole-Body 18F-FDG-PET/CT Examinations at 4 German Hospitals Equipped with the Dual-Modality Tomographs Characterized in Table 1
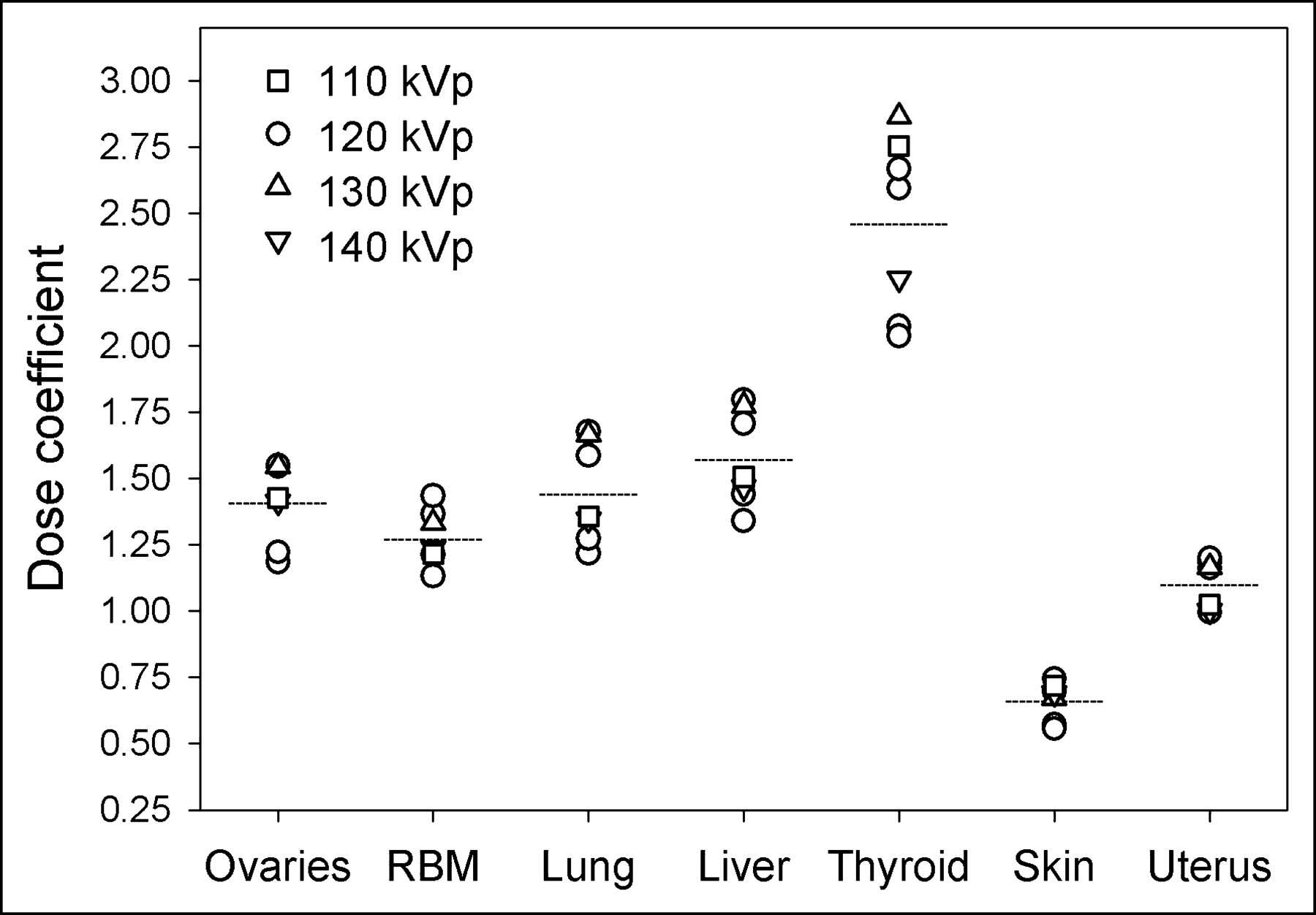
Average 18F-FDG activities of 300 MBq (H2) and of 370 MBq (H1, H3, and H4) were administered, which resulted in estimated effective doses of 5.7 and 7.0 mSv, respectively. The acquisition time for the whole-body 18F-FDG PET scans was <45 min at all sites. The scan parameters used for the different CT scans are specified in Table 3. Because the symphysis was defined as the lower limit of the CT scan range, the testes were not in the imaged body region. Nevertheless, they were exposed by scattered radiation and due to the overranging effect to a varying amount (0.7–7.2 mGy). At the upper side, the thyroid was within the scan region in all cases. For a more detailed assessment of the dose distribution within the human body, dose coefficients for the relevant organs are listed in Table 4 for both 18F-FDG PET and CT examinations. Estimated CT dose coefficients for some representative organs are plotted in Figure 1 along with the corresponding mean values.

CT dose coefficients ΓTCT for some representative organs. Symbols give dose coefficients determined according to Equation 2 for each of the 7 CT scans listed in Table 3, whereas horizontal lines indicate corresponding mean values. RBM = red bone marrow.
Measurement Parameters Used for Low-Dose (LD-CT) and Diagnostic (D-CT) Whole-Body CT Scans Summarized in Table 2
Tissue Weighting Factors and Dose Coefficients for 18F-FDG PET (ΓTFDG) and Whole-Body CT (ΓTCT) Scans
For the 7 CT protocols used (Table 3), the effective dose was calculated on the basis of Equation 2 using the mean dose coefficient of ΓECT = 1.47 ± 0.02 mSv/mGy given in Table 4. The resulting dose values are plotted versus the corresponding values determined from the TLD measurements on the Alderson phantom in Figure 2. Linear regression analysis (SigmaPlot, version 7.101; SPSS Inc.) yielded a slope of 1.03.

Statistical relation between calculated and measured effective doses for 7 CT scans listed in Table 3. Solid line gives result of linear regression analysis through origin with a slope of 1.03 and dashed curves indicate 95% confidence interval. Error bars indicate the uncertainty of dose estimates.
DISCUSSION
The effective dose for patients undergoing high-quality whole-body 18F-FDG PET/CT examinations at the 4 university hospitals participating in this study was about 25 mSv. Despite the similarity of the effective dose values (23.7–26.4 mSv), there were some noticeable differences between the 4 PET/CT acquisition protocols, which are representative of the imaging scenarios reported in the literature. Mainly, the 4 clinical sites (H1–H4) had a different approach to the clinical implications from the CT scan of the combined PET/CT examination.
At 2 hospitals (H2 and H4), separate low-dose CT scans were acquired for attenuation correction of emission data in addition to a contrast-enhanced CT scan. At the other 2 sites (H1 and H3), a single, contrast-enhanced CT scan was used both for a fully diagnostic evaluation and for CT-based attenuation correction. This may imply the question of whether the administration of an intravenous CT contrast agent leads to serious artifacts in the attenuation-corrected PET images, since structures with a strong enhancement in the CT scans may be considered as bone by the attenuation correction algorithm, thus resulting in an overestimation of regional attenuation coefficients (14). However, recent evidence indicates that these artifacts rarely cause a diagnostic challenge in the clinical setting (15) and that these artifacts can be avoided prospectively when using adapted contrast administration protocols (16).
Nevertheless, if a contrast-enhanced diagnostic CT scan has already been performed on a conventional CT system as part of the regular clinical work-up, it is in general acceptable to acquire only a low-dose CT scan as part of the combined PET/CT study (17). The image quality of this scan is certainly adequate for anatomic correlation and attenuation correction (18). In the present study, the effective dose determined for 3 low-dose scans was <5 mSv (Table 2).
The effective doses determined for the 4 high-quality CT scans listed in Table 3 varied between 14.1 and 18.6 mSv. These values are somewhat higher than the dose estimates (mean ± SD) of 14.5 ± 4.9 mSv from a recent survey on whole-body, multislice CT examinations (19), which is mainly due to the inclusion of the thyroid in the whole-body scan range covered in this study.
The dose coefficients listed in Table 4 make it possible to estimate organ doses and—using the corresponding tissue weighting factors—effective doses related to whole-body 18F-FDG PET and CT scans. All data presented are for a standard person with a body weight of about 70 kg and are generic rather than patient specific since the age, sex, and constitution of individual patients are not considered. Nevertheless, they provide a reasonably good indicator of the relative radiation risks to patients (12) resulting from nonuniform exposures related to whole-body PET and CT procedures and, thus, for protocol optimization.
PET/CT users should note that the CTDIvol value displayed on the operator’s console is the principal descriptor to characterize patient exposure in CT on a local dose level. It represents an estimate of the average dose within an irradiated slice of a standardized CT dosimetry phantom and, thus, reflects not only the combined effect of the selected scan parameters but also of scanner-specific factors such as beam filtration, beam-shaping filter, geometry, and overbeaming. A detailed discussion of the various scan parameters and system features determining patient exposure in CT as well as strategies for dose reduction can be found elsewhere (19,20). Besides the CTDIvol, the length of the scan region is the second parameter that determines the effective dose and, thus, the integrated detriment to patients related to a CT examination. Whenever clinically justifiable, the range of whole-body scans should be limited by the symphysis at the lower limit and should exclude the eye lenses from the cranial imaging range.
However, adaptation of the scan length to the individual body size may not be possible at current PET/CT systems because the axial CT range can be set up only in integer multiples of the fixed axial field of view of the PET system. This technical limitation can be overcome in the future, for example, by the implementation of continuous bed motion for PET measurements. In general, noncongruent imaging ranges of PET and CT scans, as well as multiple contiguous spirals with different CT scan parameters, should become available with the clinical PET/CT acquisition software. This flexibility would open the possibility of acquiring a high-quality CT scan for only part of the body and imaging the remaining axial ranges with a low-dose CT, or even without attenuation correction. Moreover, prospective measures that offer the potential for dose reduction in CT without a considerable loss in image quality—such as automatic tube current modulation or adaptive filtering—should be adopted for routine PET/CT.
CONCLUSION
The PET/CT acquisition protocols examined in this study reflect the range of whole-body PET/CT imaging scenarios reported in the literature today. We estimated an average effective patient dose from whole-body 18F-FDG PET/CT examinations of about 25 mSv independent of the acquisition protocol preferred. Considering the increased patient exposure compared with individual CT or PET examinations, a judicious medical justification has to be made with every PET/CT referral. The derived dose coefficients provide a valuable tool for estimating organ and effective doses for a diversity of whole-body CT scans and, in turn, for protocol optimization. Independently, prospective dose reduction measures from state-of-the-art CT practice should be adopted in PET/CT imaging, and modifications to the existing acquisition software should be considered.
Footnotes
Received Aug. 5, 2004; revision accepted Dec. 10, 2004.
For correspondence or reprints contact: Gunnar Brix, PhD, Bundesamt für Strahlenschutz, Abteilung für Medizinische Strahlenhygiene und Dosimetrie, Ingolstädter Landstraβe 1, D-85764 Neuherberg, Germany.
E-mail: gbrix{at}bfs.de
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 68Ga-FAP-2286 PET of Solid Tumors: Biodistribution, Dosimetry, and Comparison with 18F-FDG
- SNMMI Procedure Standard/EANM Practice Guideline for SSTR PET: Imaging Neuroendocrine Tumors
- Reducing Radiation Exposure from PET Patients
- Weight-Based Protocols Offer Significant Reduction in Radiation Dose Without Affecting PET-CT Image Quality
- Establishment of National DRL for CT in Hybrid Imaging Studies (The Second Phase of the National NM CT (PET) Dose Audit for Kuwait Population -2019)
- Is True Whole-Body 18F-FDG PET/CT Required in Pediatric Lymphoma? An IAEA Multicenter Prospective Study
- First Human Imaging Studies with the EXPLORER Total-Body PET Scanner
- Appropriate Use Criteria for Somatostatin Receptor PET Imaging in Neuroendocrine Tumors
- Radiation Dosimetry of Whole-Body Dual-Tracer 18F-FDG and 11C-Acetate PET/CT for Hepatocellular Carcinoma
- Determining the Minimal Required Radioactivity of 18F-FDG for Reliable Semiquantification in PET/CT Imaging: A Phantom Study
- Diagnostic Reference Levels of CT Radiation Dose in Whole-Body PET/CT
- Methods of CT Dose Estimation in Whole-Body 18F-FDG PET/CT
- Using SUV as a Guide to 18F-FDG Dose Reduction
- Late Imaging with [1-11C]Acetate Improves Detection of Tumor Fatty Acid Synthesis with PET
- PET/CT Imaging and Human Papilloma Virus-Positive Oropharyngeal Squamous Cell Cancer: Evolving Clinical Imaging Paradigm
- Regional Cerebral Blood Flow in Children From 3 to 5 Months of Age
- Measured Human Dosimetry of 68Ga-DOTATATE
- Synthesis, Preclinical Validation, Dosimetry, and Toxicity of 68Ga-NOTA-Anti-HER2 Nanobodies for iPET Imaging of HER2 Receptor Expression in Cancer
- Imaging the inflammatory activity of sarcoidosis
- Dose exposure in the ITALUNG trial of lung cancer screening with low-dose CT
- Positron emission tomography imaging approaches for external beam radiation therapies: current status and future developments
- Inadvertent Intraarterial Injection of 18F-FDG: A Case Report and Literature Review of Hot Forearm and Hot Hand Signs
- Implementation of Automated Tube Current Modulation in PET/CT: Prospective Selection of a Noise Index and Retrospective Patient Analysis to Ensure Image Quality
- PET/MRI: Paving the Way for the Next Generation of Clinical Multimodality Imaging Applications
- 18F-FDG PET/CT Identifies Patients at Risk for Future Vascular Events in an Otherwise Asymptomatic Cohort with Neoplastic Disease
- Software Fusion: An Option Never Fully Explored
- Integrated PET/CT in the staging of nonsmall cell lung cancer: technical aspects and clinical integration
- Dual-Modality Imaging: Combining Anatomy and Function
- Estimation of the {beta}+ Dose to the Embryo Resulting from 18F-FDG Administration During Early Pregnancy
- Imaging in staging of malignant lymphoma: a systematic review
- PET/CT in Evaluating Pediatric Malignancies: A Clinician's Perspective
- Impact of [18F]-fluorodeoxyglucose ([18F]-FDG) imaging in sarcoidosis: unsuspected neurosarcoidosis discovered by [18F]-FDG PET and early metabolic response to corticosteroid therapy
- Screening for Cancer with PET and PET/CT: Potential and Limitations
- Can PET/CT Replace Separate Diagnostic CT for Cancer Imaging? Optimizing CT Protocols for Imaging Cancers of the Chest and Abdomen
- Optimized Contrast-Enhanced CT Protocols for Diagnostic Whole-Body 18F-FDG PET/CT: Technical Aspects of Single-Phase Versus Multiphase CT Imaging