


Abstract
Guidelines recommend true whole-body 18F-FDG PET/CT scans from vertex to toes in pediatric lymphoma patients, although this suggestion has not been validated in large clinical trials. The objective of the study was to evaluate the incidence and clinical impact of lesions outside the “eyes to thighs” regular field of view (R-FOV) in 18F-FDG PET/CT staging (sPET) and interim (iPET) scans in pediatric lymphoma patients. Methods: True whole-body sPET and iPET scans were prospectively obtained in pediatric lymphoma patients (11 worldwide centers). Expert panel central review of sPET and iPET scans were evaluated for lymphoma lesions outside the R-FOV and clinical relevance of these findings. Results: A total of 610 scans were obtained in 305 patients. The sPET scans did not show lesions outside the R-FOV in 91.8% of the patients, whereas in 8.2% patients the sPET scans demonstrated lesions also outside the R-FOV (soft tissue, bone, bone marrow, and skin); however, the presence of these lesions did not change the clinical stage of any patient and did not affect treatment decision. Among the 305 iPET scans, there were no new positive 18F-FDG–avid lesions outside the R-FOV, when compared with their paired sPET scans. A single lesion outside the R-FOV on iPET occurred in 1 patient (0.3%), with the primary lesion diagnosed in the femur on sPET that persisted on iPET. Conclusion: The identification of additional lesions outside the R-FOV (eyes to thighs) using 18F-FDG PET/CT has no impact in the definition of the clinical stage of disease and minimal impact in the treatment definition of patients with pediatric lymphoma. As so, R-FOV for both sPET and iPET scans could be performed.
In the last decades, 18F-FDG PET/CT has become the established modality for pediatric staging of all solid tumors (1), Hodgkin lymphoma (HL), non-Hodgkin lymphoma (NHL) (2–4), sarcomas (5,6), and neuroblastomas (7). The literature on pediatric oncologic 18F-FDG PET/CT advocates performance of true whole-body field-of-view (TWB-FOV) examinations, with imaging from vertex to toes (8,9), as tumors in children might have systemic involvement that can include the distal extremities (10–12). In adults, the reduced field-of-view (R-FOV) of 18F-FDG PET/CT (so-called eyes-to-thighs) is limited to the neck, chest, abdomen, pelvis, and upper thighs, which provide significant advantages. Exceptions are made for some sarcomas, melanomas, or cases of primary or suspected extremity involvement (13) in which TWB-FOV PET/CT images are also obtained. Early articles describing the use of 18F-FDG PET/CT in pediatrics were more likely to assume that R-FOVs done in adults may be enough in some cases of pediatric lymphoma (3,9,14).
The R-FOV images provide significant advantages for patients: they decrease radiation exposure and scanning time, potentially improving image quality and reducing anesthesia time.
HL has a relatively predictable progression of metastases, with rare extremity involvement in the absence of disseminated disease or bone marrow involvement within the chest, abdomen, and pelvis (15–19). Indications for 18F-FDG PET/CT have also been established in certain types of NHL (20–23).
There are certain “trues” in science, based mainly in common sense, without solid empiric evidence as TWB for pediatric patients. The purpose of this multicenter international investigation, coordinated by the International Atomic Energy Agency (IAEA), was to evaluate whether there is a clinically significant incidence of lesions outside the R-FOV in PET/CT staging (sPET) and interim (iPET) scans in pediatric lymphoma patients.
MATERIALS AND METHODS
This IAEA project is registered as the Coordinated Research Project E12017. The protocol was developed jointly at 2 investigator’s meetings in 2012 and 2013. The data collection and partial analysis investigator’s meeting was performed in 2015, and the final investigator meeting occurred in 2017.
Research Regulation and Data Protection
Each center obtained research ethics approval for the study protocol and patient information from the appropriate Ethics Review Board. Fully informed consent was an inclusion criterion for recruitment. Signed parental consent was kept by the local investigators. To ensure confidentiality while sharing data internationally, cases and forms were anonymous.
Eligibility Criteria and Treatment Protocol
Pediatric patients (age < 18 y) with newly diagnosed HL or NHL were recruited.
Exclusion criteria were pregnancy, breast-feeding, prior cancer, prior radiation therapy or chemotherapy, concurrent HIV infection or history of tuberculosis, and non-18F-FDG–avid disease on staging PET/CT scans (sPET). Diagnosis was based on biopsy with immunohistochemistry according to the World Health Organization classification criteria (24). Furthermore, because guidelines and 18F-FDG dosing are comparatively broad worldwide, rest period protocols could vary between 50 and 90 min. All imaging data acquired outside the preestablished criteria were excluded.
PET/CT Scheduling, Acquisition, and Reporting
All patients underwent TWB-FOV PET/CT studies, from the top of the skull to the toes. All PET/CT studies were performed for sPET and iPET. Scans were obtained according to the procedure guidelines of the Society of Nuclear Medicine and Molecular Imaging or European Association of Nuclear Medicine (EANM), which are standard for all nuclear medicine practice (13,25).
Clinical data were collected, including for initial staging using the Ann Arbor classification and for NHL using the St. Jude classification. All patients were staged by the local pediatric oncologists.
The iPET scan was recommended after 2 cycles of chemotherapy, at a maximum interval from the preceding treatment (1–5 d before the next chemotherapy cycle). In recognition of technical and scheduling constraints, iPET after 3 cycles was permitted and in no circumstances after 4 cycles.
An expert panel composed of 11 certified nuclear medicine physicians working together on a common platform at the final collaborator’s meeting reviewed all sPET and iPET scans. Any discrepancy among scans after all reviews were undertaken were resolved by consensus.
The R-FOV and the TWB-FOV were scored separately. Reviewers analyzed the presence of lesions outside the eye to thighs in both scans. Discrepancies were resolved by consensus.
All 18F-FDG uptake above the background and outside the areas of normal biodistribution were considered abnormal. Abnormalities including focal lesions within the bone/bone marrow, focal soft-tissue lesions, or diffuse bone marrow involvement were classified as positive for disease. We also recorded whether these abnormalities changed the stage or disease management in any individual patient.
The above classification was applied for both sPET and iPET scans.
RESULTS
A total of 305 patients underwent paired sPET and iPET examinations, totalling 610 PET/CT scans (Table 1).
Patient Demographics
sPET
All 305 patients underwent sPET examinations. TWB-FOV PET images revealed disease limited to the R-FOV in most of the patients (n = 280; 91.8%), with no lymphoma lesion outside the R-FOV (Fig. 1).

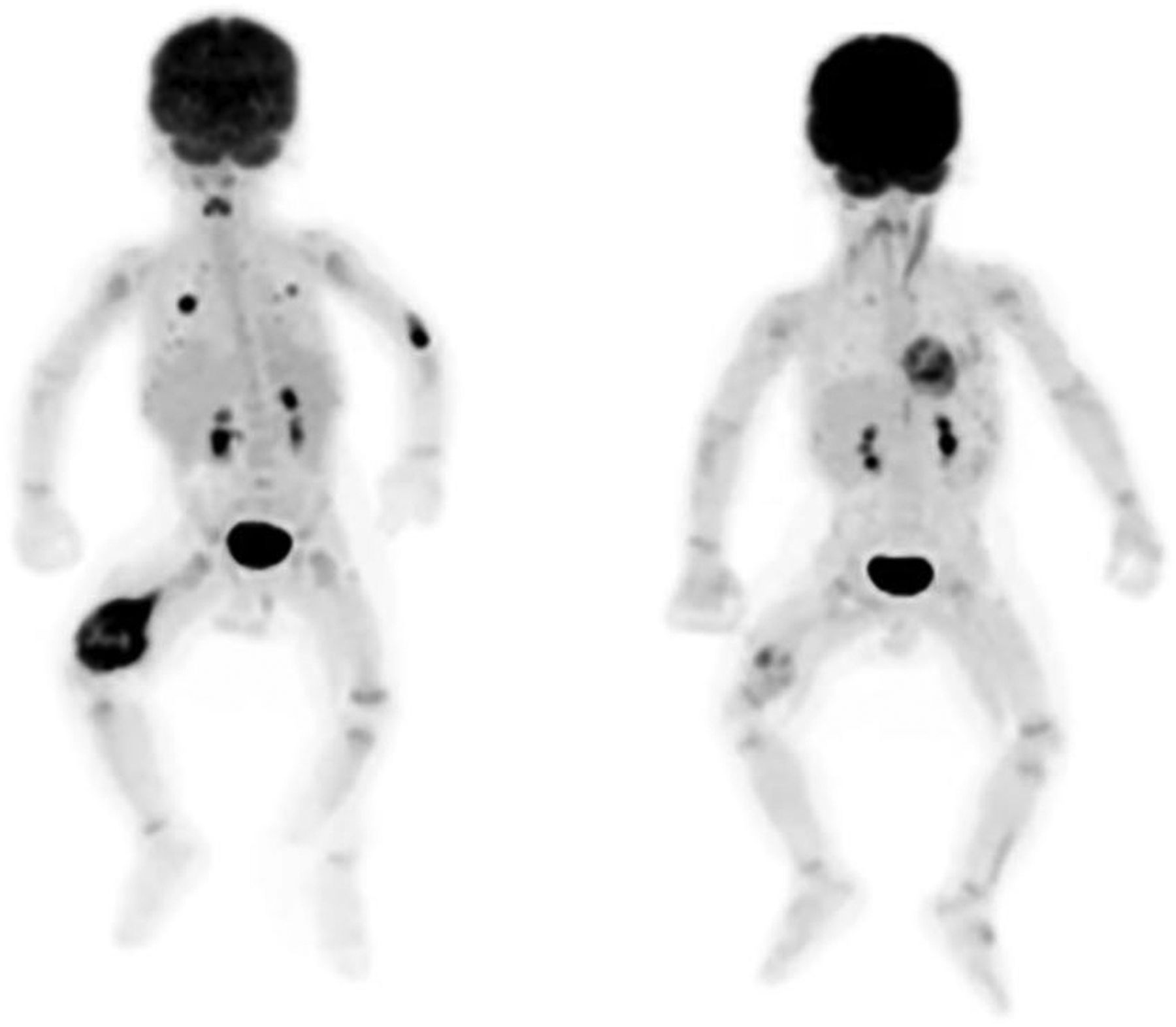
A 12-y-old male patient was diagnosed with clinical stage 2 NHL and underwent sPET and iPET PET/CT studies. sPET (left image) shows no lymphoma lesions outside the R-FOV. iPET (right image), obtained after 2 cycles of chemotherapy, shows a complete metabolic response (Lugano Classification score 1). He was disease free at 12 mo of follow-up.
TWB-FOV sPET images of the remaining 25 (8.2%) patients revealed disease outside the R-FOV. These lesions outside the R-FOV were noted in the soft tissue (1 patient with NHL), bone (2 patients with NHL), bone marrow (23 patients, 9 with HL and 14 NHL), and skin (1 patient with NHL) (Table 2). All patients with lesions outside R-FOV PET presented lesions in the extremities; only 2 patients also presented lesions in the vertex.
Patients with Lesion Outside R-FOV PET/CT Clinical Characteristics
In the 25 patients, age varied from 0.6 to 17 y (median age, 9.31 y), 9 patients with HL (5 nodular sclerosis, 2 lymphocyte-rich classical, and 2 mixed cells) and 16 patients with NHL (9 Burkit, 3 diffuse large B cell lymphoma [DLBCL], 2 T cell, and 2 anaplastic lymphoma).
Twenty-four of these patients (24/25) presented also with lesions in the R-FOV and were already classified as having advanced-stage disease based on the R-FOV sPET images. All patients presented with bone marrow disease (confirmed by bone marrow biopsy in 14 patients, with negative bone marrow biopsy in 11 patients), with more than 1 extranodal site in 15 patients with commitment in lung (6), pleura (3), liver (3), gastrointestinal (3), soft tissue (2), kidney (2), pancreas (1), and skin (1). Therefore, the additional findings of disease outside the R-FOV were not impactful and did not alter the clinical stage or treatment.
Only 1 remaining (1/25) NHL patient (DLBCL) with immunodeficiency presented with a single bone lesion in the right distal femur, exclusively outside the R-FOV. This patient also presented with focal 18F-FDG uptake in the lung, which was related to Pneumocystis carinii pneumonia.
iPET
The same 305 patients who underwent sPET examinations also underwent paired iPET scans. Among the 280 patients in whom sPET revealed disease limited to the R-FOV, no additional disease was noted outside the R-FOV. Therefore, the iPET scans of roughly 92% of patients were also negative for disease outside the R-FOV (Fig. 2).

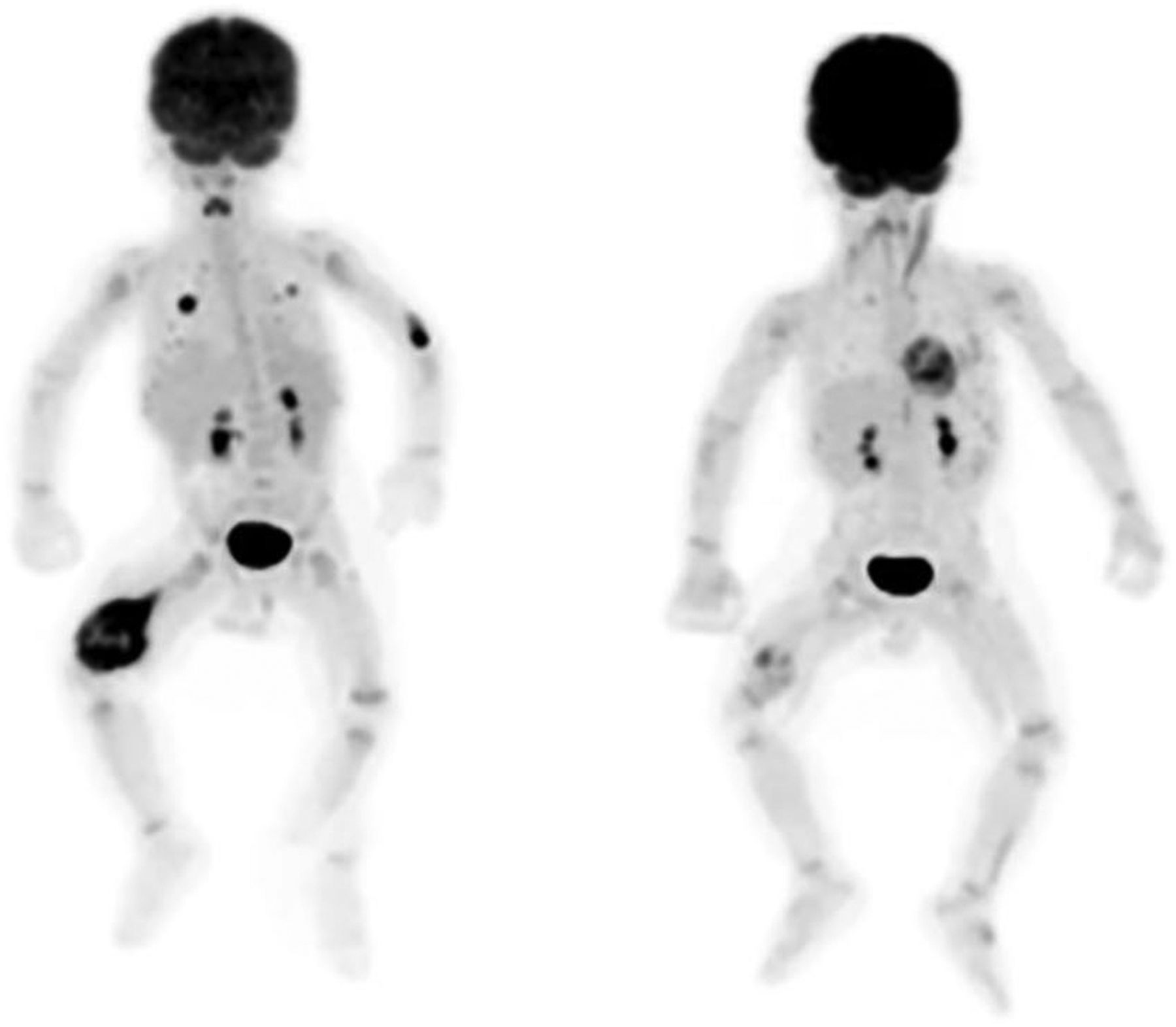
A 15-y-old male patient was diagnosed with clinical stage 4 HL. In addition to the bone marrow lesions identified within the R-FOV, sPET (left image) shows lesions outside the R-FOV, including bone marrow lesions in both humeri, femur and tibiae. iPET (right image), obtained after 2 cycles of chemotherapy, shows a complete metabolic response (Lugano Classification score 1). The patient is still disease-free at 33 mo of follow-up.
Among the 25 patients in whom the TWB-FOV sPET images revealed disease outside the R-FOV, the paired TWB-FOV iPET images did not identify additional disease outside the R-FOV.
However, the 1 patient (1/25) in whom the sPET images had identified a lymphoma in the right distal femur, the iPET revealed a partial response to therapy with no impact on subsequent patient management as the initial proposed treatment was not modified (Fig. 3). Therefore, in only 1 (0.3%) of the 305 iPET scans was the TWB-FOV important for subsequent patient management (Fig. 4).
A 7-mo-old male patient was diagnosed with clinical stage 4 NHL. sPET (left image) shows 18F-FDG–avid lesions in the lungs and the right distal femur. Further investigation revealed an infectious process due to Pneumocystis carinii in lungs (18F-FDG uptake in left elbow is site of injection). iPET (right image), obtained after 2 cycles of chemotherapy, shows partial response in lymphoma in right distal femur (Lugano Classification score 4). At the end of treatment, there was a complete response and patient was still alive after 38 mo of follow-up.
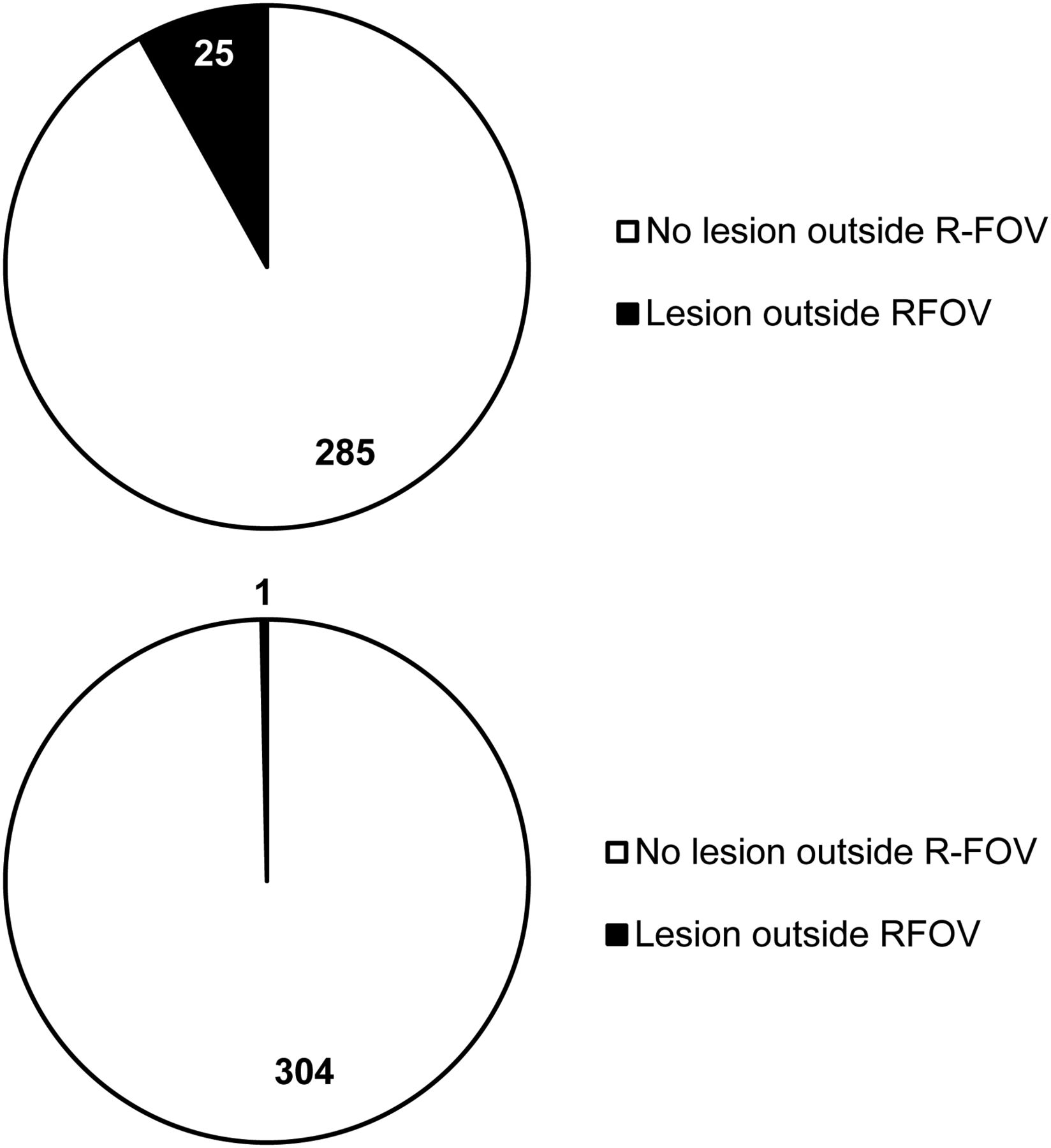
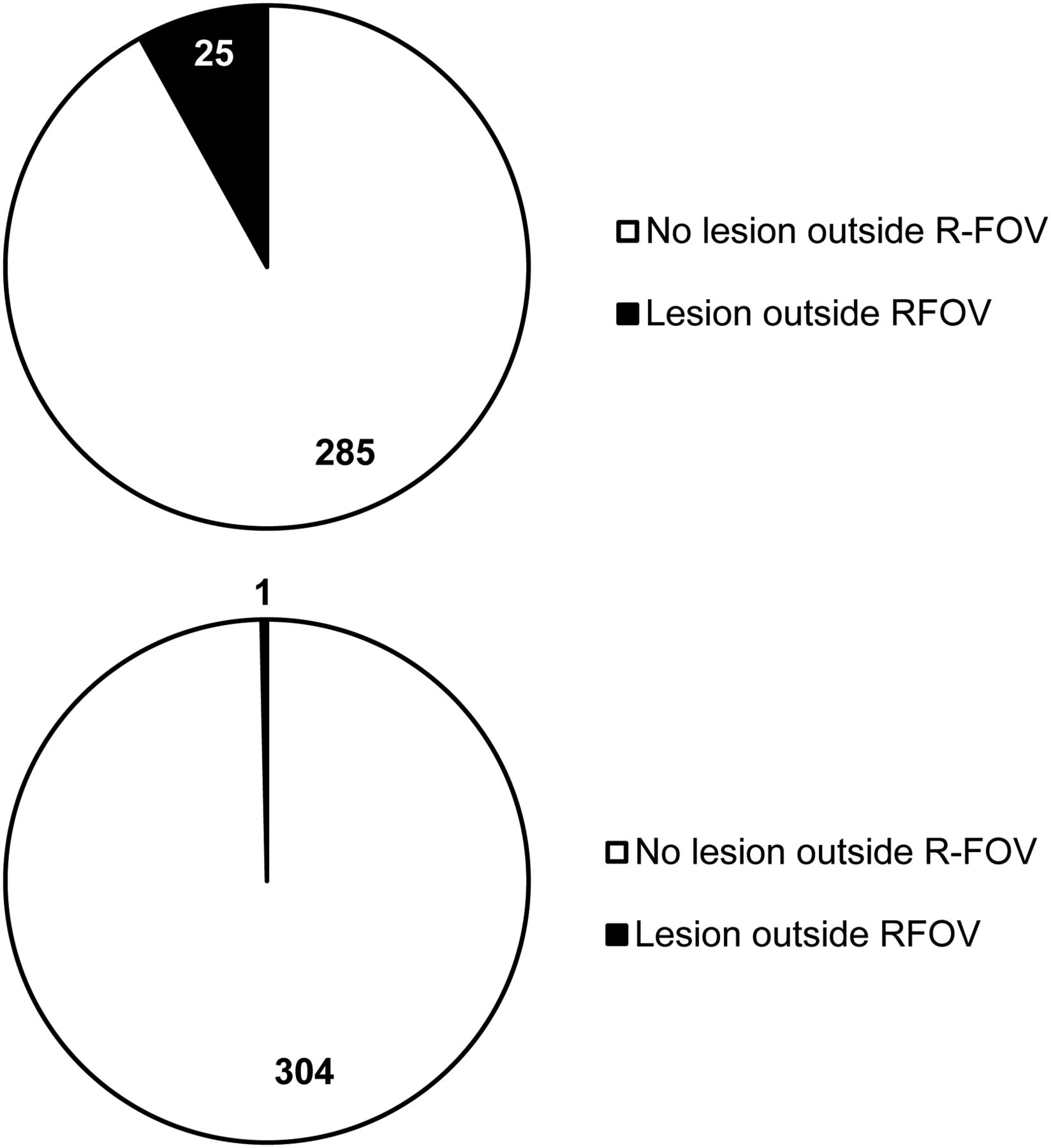
Results of the presence of lesions inside and outside the R-FOV on sPET (A) and iPET (B).
DISCUSSION
In this multicenter international study coordinated by the IAEA, for 610 scans obtained in 305 patients (305 sPET and 305 iPET scans), the sPET scans did not show lesions outside the R-FOV in 92% of the patients. In 8% of the patients, the sPET scans showed lesions outside the R-FOV. These lesions outside the R-FOV were in the soft tissue, bone (2 patients with NHL), bone marrow (23 patients, 9 with HL and 14 NHL), and the skin (1 patient with NHL). There were no changes in the clinical stage of any patient or treatment decision. Although current guidelines for pediatric oncologic 18F-FDG PET/CT empirically suggest use of TWB examinations (8,9), these guidelines and other articles (3,14,26) acknowledge that R-FOV PET/CT is likely to be sufficient for some cases of pediatric lymphoma. Our evidence reinforces that R-FOV PET/CT is sufficient in pediatric lymphoma both at staging and interim assessments.
An R-FOV PET/CT has the advantages of decreased radiation exposure due to a reduction in the area of the body that is irradiated outside of R-FOV. Ionizing radiation has been implicated in conferring a latent increased risk of malignancy (27,28). This is especially important in pediatric patients who, given their age, have longer to manifest these adverse effects (29,30). In pediatric oncology, recent reports have shown a significant cumulative radiation dose in lymphoma patients (31,32). PET/CT applies the “as low as reasonably achievable” principle (ALARA) (33), to both the 18F-FDG dose and the acquisition parameters for the CT scan (34–39). A possibility for decreasing dose is eliminating the CT dose to the extremities and to the brain if an R-FOV PET/CT scan is performed rather than a TWB PET/CT scan. Using published pediatric PET/CT acquisition protocols (40), the R-FOV acquisition imparts a whole-body effective dose of, at most, 5.5 mSv, whereas TWB acquisition imparts 5.7 mSv, resulting in a 5% reduction in whole-body effective dose. In terms of organ-specific doses, compared with the TWB examination, the R-FOV acquisition reduces the CT dose to the brain by 70%, to the skin by 15%, and to the remaining organs (primarily oral mucosa) by 7%.
Another advantage of R-FOV over TWB PET/CT examinations is a shorter scanning time, possibly reducing the risk of movement during the scan (41). Even if the pediatric population represents a reasonably broad spectrum of ages and corresponding sizes, reducing the PET/CT FOV could potentially reduce to half of the scanning time. A shorter imaging time may also increase accessibility of PET/CT examinations in centers at which high demand on facility resources is present. This is a significant consideration in developing countries where there are limited pediatric PET/CT scanners available.
Decreasing imaging time could also result in a similarly decreased length of anesthesia time for those patients requiring sedation. The need for shorter sedation could allow use of a more desirable anesthetic, which would be determined according to pediatric sedation guidelines (42). Depth of sedation may also potentially be reduced, which could result in similar advantages. As we now consider a shift to the use of PET/MRI in children, we will further reduce radiation dose to the child with the CT but there will be a concomitant potential increase in sedation time for the MRI portion of the studies. A Food and Drug Administration drug safety communication stated that there is the probability of increasing neurodevelopmental risks in children younger than 3 y and in women in the third trimester of pregnancy with prolonged and repeated procedural sedation of greater than 3 h (43).
Although our findings challenge conventional clinical practice, for many years consolidated without empiric basis, a similar finding in another study, with a smaller series of cases, supports a reduced FOV practice. Sammer et al. (44) is the only previous paper to have evaluated R-FOV versus TWB-FOV differences in PET/CT studies in 170 lymphoma patients. No disease outside the R-FOV sPET was found on iPET scans in the 150 patients, while 12% of patients had disease outside the R-FOV in staging. In only 1 patient with lymphoblastic NHL was the imaging stage altered with the additional TWB-FOV. They concluded that it was appropriate to perform R-FOV iPET when sPET did not show disease beyond eyes to thighs. Likewise, in our study with a substantially larger cohort, only 8.3% of patients had disease outside the R-FOV in sPET, and also in only 1 case on both sPET and iPET (0.3%) was a clinically relevant bone lesion outside of R-FOV found. It is important to note that this lesion was the primary lesion biopsied in this immunodeficiency related lymphoma patient (DLBCL). The location of his disease would make this case an exception and so this isolated case would have a priori called for a TWB PET scan. This case, although unique, would not be missed because common sense and clinical experience still rule in the clinical decision-making process. Similar to practice in adults, exceptions should probably include cases of primary or suspected extremity involvement (13) for which TWB-FOV PET/CT images are also obtained. Therefore, our results support the use of R-FOV PET/CT not only for iPET but also for sPET.
This paper does not suggest that R-FOV PET/CT should be used in other pediatric tumors. Just as there are certain tumors in the adult population that have more propensities to involve the extremities, tumors such as sarcomas, neuroblastomas, and leukemias are well known to have systemic involvement and TWB PET/CT imaging is still the recommendation in children who may present with these and other tumors, even though there are limited data to support this approach (8,9).
A limitation of our study is our relatively small number of patients with the different subtypes of NHL, even though we obtained 219 PET/CT scans in HL patients and in 86 NHL patients. Whereas HL behaves in a relatively predictable way with well-defined staging methodology, NHL encompasses a relatively heterogeneous group of histologies, many with different morphologies, presentations, and natural histories (45). Consequently, further studies dedicated to NHL or specific types of NHL may be helpful to more precisely define the role of R-FOV PET/CT in these patients. Also, in our study we did not perform dosimetry to determine the percentage reduction in radiation exposure or to determine the exact reduction in scanning time.
Major strengths of this study were that this is the biggest series of cases of pediatric lymphoma patients as far as we know in an international multicenter trial spanning differing socioeconomic layers as defined by the World Bank to include low-middle, upper-middle, and high-income countries.
CONCLUSION
Our results demonstrate that the identification of additional lesions outside the R-FOV (eyes to thighs) 18F-FDG PET/CT has no impact in the definition of the clinical stage of disease and minimal impact in the conduct definition of patients with pediatric lymphoma. As so, R-FOV for both staging and interim 18F-FDG PET/CT scans could be performed. This consideration may be quite impactful in developing countries where there are limited pediatric PET/CT scanners available.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 25, 2019.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 23, 2018.
- Accepted for publication December 19, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.