


Abstract
Our objective was to evaluate the association of arterial 18F-FDG uptake and calcifications in large arteries as detected by 18F-FDG PET/CT with the subsequent occurrence of vascular events in otherwise asymptomatic cancer patients. Methods: Clinical follow-up information was obtained for 932 cancer patients examined with whole-body 18F-FDG PET/CT (median follow-up time, 29 mo). Among this cohort, 279 patients had died from their oncologic disease. In 15 of 932 patients (1.6%), a vascular event, defined as ischemic stroke, myocardial infarction, or revascularization, was registered. The maximal standardized uptake value (SUV) was divided by the blood-pool SUV, yielding a target-to-background ratio (TBR) for each arterial segment. The mean TBR as well as a calcified plaque sum score per patient were calculated in the major vessels: ascending, descending, and abdominal aorta, aortic arch, as well as iliac and carotid arteries. Results: A significant correlation was observed between mean TBR and calcified plaque sum (P < 0.001). Although calcified plaque sum significantly correlated with all conventional risk factors for vascular events, mean TBR correlated only with age, the male sex, and hypertension. The Cox regression hazard model identified a mean TBR ≥ 1.7 and a calcified plaque sum ≥ 15 as independent predictors for the occurrence of a vascular event. Patients with both mean TBR and calcified plaque sum above these thresholds were identified as having the highest risk for a future vascular event. However, a mean TBR ≥ 1.7 had greater prognostic value than did a calcified plaque sum ≥ 15. Conclusion: In a large cohort of cancer patients, increased 18F-FDG uptake in major arteries emerged as the strongest predictor of a subsequent vascular event. Concomitant severe vascular calcifications seemed to impart a particularly high risk. Given the small event rate in the present study, larger, prospective trials of patients without cancer are required to substantiate these promising results.
Complications of cardiovascular disease continue to be the leading cause of death in the Western world, despite significant advances over the past 20 years in treating cardiovascular disease (1). Although the incidence of cardiovascular disease declined somewhat in the interval 1994–2004 (2), there remains an excessively high rate of sudden death due to vascular events in apparently healthy individuals without prior symptoms (3). Vascular events are most frequently caused by sudden rupture of a vulnerable atherosclerotic plaque, resulting in either thrombotic occlusion at the site of rupture or distal embolization (4). In recent years, atherosclerotic disease has come to be recognized as a generalized inflammatory process of the arterial wall (5), thus giving rise to the concept of the “vulnerable cardiovascular patient” (3). Early atherosclerotic lesions are colonized by blood-borne inflammatory and immune cells, which release effector molecules that accelerate and exacerbate progression of the lesions. There then follows a complex cascade of mechanisms finally transforming the stable plaque into a vulnerable, unstable structure, which can rupture and give rise to sudden vascular events (6). It remains a major challenge for preventative medicine to identify asymptomatic high-risk patients who would benefit from intervention before rupture of the nascent plaques.
Historically, atherosclerosis-imaging modalities have been used to assess the cross-sectional diameter of the arterial lumen. Although the extent of luminal stenosis is certainly an indicator of plaque burden, the likelihood of plaque rupture is more especially related to the extent of inflammatory activity within the plaque and consequent changes in the plaque morphology (4). Therefore, knowledge of plaque composition and morphology seems crucial to determine the vulnerability of a particular plaque.
A reliable and well-established method to image and quantify plaque inflammation is provided by whole-body 18F-FDG PET (7). 18F-FDG is entrapped within plaque macrophages more avidly than within other plaque elements and may thus be used as a biologic marker of vessel wall inflammation (8–11). The advent of combined 18F-FDG PET and CT in a single instrument enables the exact anatomic assignment of focally increased 18F-FDG uptake to specific arterial vessel segments (12) and furthermore allows the detection and quantification of vascular calcifications, which are revealed by the CT modality alone. Although it is well documented that calcified coronary atherosclerotic plaque burden is an independent risk factor for future vascular events (13), a recent publication has also described an association between aortal calcifications and vascular events (14).
The purpose of this study was to evaluate the association of both arterial 18F-FDG uptake and atherosclerotic calcified plaque burden in large arteries as detected by 18F-FDG PET/CT dual-mode imaging with the occurrence of future cardio- and cerebrovascular events. Given the low incidence of vascular events in an asymptomatic population, it would scarcely be possible to conduct a prospective study of the sensitivity of metabolically active intravascular plaques as a predictor of subsequent events. However, 18F-FDG PET/CT is now routinely performed in the course of clinical investigations for neoplastic disease; we have access to a series of more than 1,000 such patients. In the present study, we investigated this population, in whom the occurrence of vascular events was known during several years of follow-up after the PET/CT examination. We used this population as a surrogate for an—in practical terms—unattainable large population of healthy subjects without a history of cardiovascular disease. We contend that vascular imaging in our patient population should provide the basis for establishing methods to identify and treat asymptomatic patients with a particular risk for future vascular events. Furthermore, we hope to establish the utility of vascular examination in the course of oncologic investigations as a clinically important incidental finding, worthy of routine attention by nuclear medicine physicians and radiologists.
MATERIALS AND METHODS
Patient Selection and Follow-up
Patients were referred to our institution for a PET/CT scan between August 2004 and August 2007. Patients with prior or ongoing steroid medication, inflammation of unknown origin, sepsis, or vasculitis, as well as patients known to have coronary artery disease or patients with prior cardio- or cerebrovascular events, were excluded from our study. For the remaining patients, cardiovascular risk factors and relevant medications were recorded during their first PET/CT scan in our institution. The study protocol was approved by the local clinical institutional review board and complied with the declaration of Helsinki.
We assumed that an otherwise asymptomatic cohort of oncology patients without known coronary artery disease should likely experience cardiovascular events at a rate of about 1% per year, based on observations of the population at large. Therefore, inclusion of 1,000 patients was considered to be sufficient for statistical outcome analyses.
Clinical follow-up information, including the occurrence of a cardio- or cerebrovascular event after the PET/CT scan or the occurrence of noncardiac death related to oncologic disease, was obtained during regular follow-up visits or by telephone interviews for 932 patients or their relatives (68 could not be reached by telephone). When an event was registered during follow-up, the type of event was double-checked by consultation with the patient's referring physician. Of the 932 patients, 282 died from their oncologic disease during follow-up. Fifteen of the 932 patients (1.6%) did not succumb to their oncologic disease but did experience nonfatal cardio- or cerebrovascular events during the interval of follow-up after the PET/CT scan (“event group”). We defined these vascular events as including ischemic stroke, myocardial infarction, or cardiac revascularization after acute coronary syndrome. For the remaining 638 surviving patients (“control group”), we performed a sample-size calculation, which justified the random selection of every second PET/CT subject (i.e., 319 patients) for further evaluation of plaque and calcium load in the PET/CT scans.
Imaging Technique
All patients underwent 18F-FDG PET/CT on a Gemini PET/CT scanner (Philips), consisting of a germanium oxyorthosilicate full-ring PET scanner and a 2-detector-row CT scanner. Before being scanned, the patients fasted for at least 6 h to ensure a serum glucose level below 130 mg/mL. The patients received 20 mg of furosemide and 20 mg of butylscopolamine bromide at the same time as intravenous injection of 200–480 MBq of 18F-FDG (5 MBq/kg of body weight; mean dose, 230 MBq). The patients rested for 45 min in a comfortable sitting position and then were brought to the scanning suite. At 60 min after 18F-FDG administration, transmission data were acquired by means of a low-dose CT scan (20 mA·s, 140 kV, a 512 × 512 matrix, a 6-mm slice thickness, an increment of 5 mm/s, a rotation time of 0.5 s, and a pitch index of 1.5) extending from the base of the skull to the proximal thighs. When clinically indicated, a contrast agent was applied for diagnostic CT. PET emission scans were acquired afterward in a caudocephalad direction in 3-dimensional mode with a 144 × 144 matrix. After scatter and decay correction, PET data were reconstructed iteratively with and without attenuation correction and then reoriented in axial, sagittal, and coronal slices. A fully 3-dimensional reconstruction algorithm based on the row-action maximum-likelihood algorithm was applied with PET-View software (Philips).
Image Analysis
PET/CT scans were read by an experienced reviewer, who was unaware of any subject information or clinical information. Maximal standardized uptake values (SUVs) for 18F-FDG were measured in the following arterial segments: both common carotid arteries, ascending aorta, aortic arch, descending aorta, abdominal aorta, and both iliac arteries. On axial, coronal, or sagittal coregistered PET/CT slices, simple circular regions of interest (ROIs) were placed so as to cover the carotid and iliac arterial walls and lumen. For those vessels of greater diameter, 1-cm-diameter ROIs were placed along the arterial walls and were slid along the arterial segments to locate the highest maximal SUV within the tubular arterial segment.
For blood-pool SUV measurements, three 1-cm-diameter ROIs were placed in the mid lumen of the inferior vena cava and superior vena cava, and the mean of the 6 measurements was taken as a representation of blood-pool activity. Within each ROI, the maximal SUV was divided by the blood-pool SUV, yielding a target-to-background ratio (TBR) for each arterial segment (Fig. 1B). For further statistical analyses, we used the mean of all TBRs for each patient, as previously recommended (7,15); the mean TBR was calculated as the mean value of TBRs from the right and left common carotid arteries, ascending aorta, aortic arch, descending aorta, abdominal aorta, and both iliac arteries.

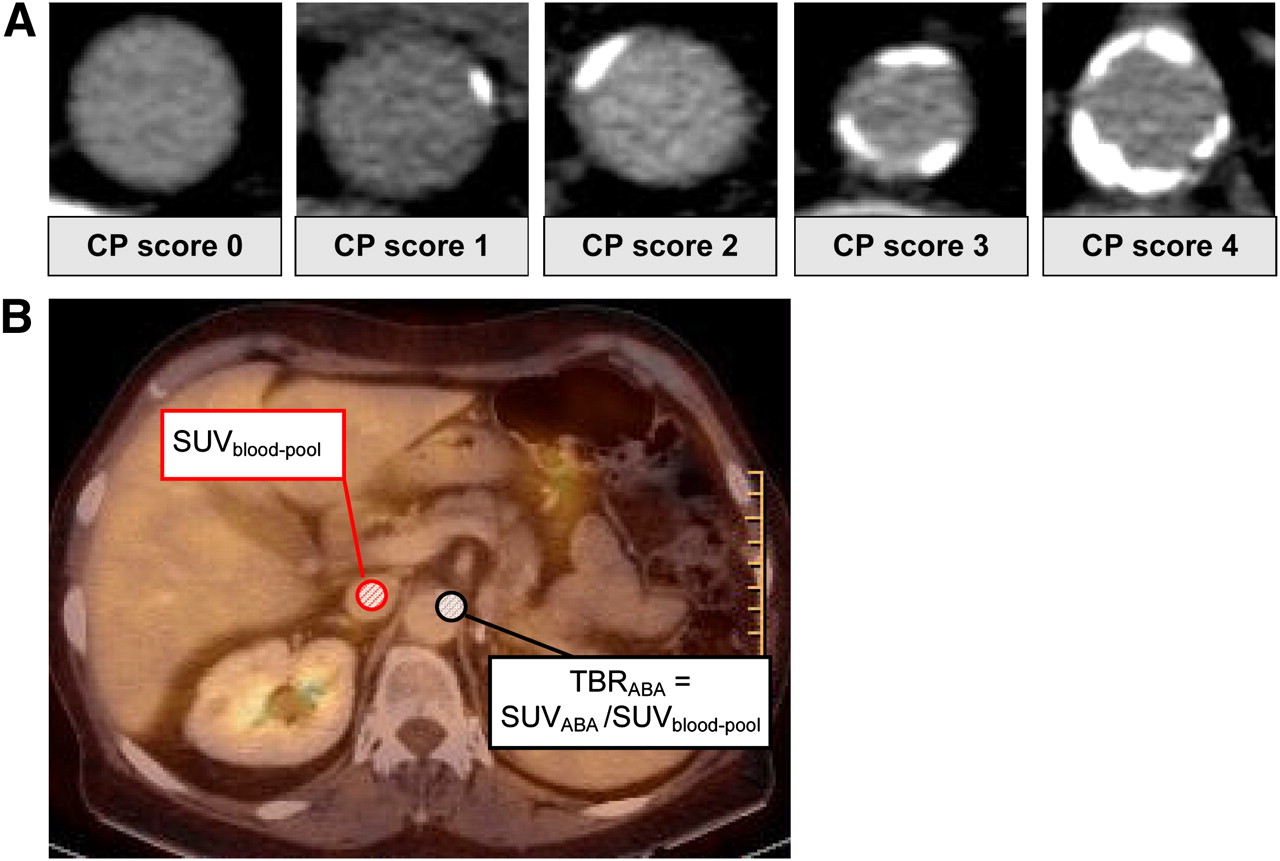
PET/CT image analysis. (A) Example of modified calcified plaque scoring system (16). Images from left to right show scores of 0 (no calcified plaque), 1 (calcified plaque involving <10% of vessel circumference), 2 (calcified plaque involving 10%−25%), 3 (calcified plaque involving 25%−50%), and 4 (calcified plaque involving >50%). (B) Example of TBR calculation method. ROIs were drawn in center of vena cava inferior (red) and in arterial wall of abdominal aorta (black). ABA = abdominal aorta; CP = calcified plaque.
The CT scans were examined for the presence of calcified plaque in the walls of the same arterial segments investigated by 18F-FDG PET. The amount of calcification was semiquantitatively ranked according to a scale modified from a previous report (16): a score of 0 was assigned when calcified plaque was absent; 1, when a small calcified plaque covering less than 10% of the vessel circumference was found; 2, when the calcified plaque involved 10%−25% of the vessel circumference; 3, when 25%−50% of the circumference was involved; and 4, when more than 50% of the vessel circumference was involved. The calcified plaque scores were summed for the 8 areas, that is, both common carotid arteries, ascending aorta, aortic arch, descending aorta, abdominal aorta, and both iliac arteries (Fig. 1A).
Eighty arterial sites of 10 individual, randomly selected subjects were reevaluated 8 wk after the initial review by the same reviewer and by a second reviewer to assess intra- and interreader reproducibility.
Patterns of Inflammation and Calcification
A TBR ≥ 1.7 and a calcified plaque score ≥ 3 were the thresholds used to identify arterial segments with increased 18F-FDG uptake or heavy calcifications. Segmental patterns showing both values consistently below or above these thresholds were defined as proportional, whereas high TBRs with low calcified plaque values or vice versa were defined as disproportional.
Statistical Analysis
Categoric variables are presented with absolute and relative frequencies, whereas continuous variables are presented with mean and SD (except age and follow-up time, which are presented as median [Q1, Q3], where Q1 is the median of the first quartile and Q3 is the median of the third quartile). For between-group comparisons, unpaired Student t tests were used for parametric data, and Mann–Whitney U rank sum tests were used for nonparametric data. The Pearson χ2 or Fisher exact test was performed, where appropriate, to determine the significance of differences in proportions. For each individual, the date of the PET/CT scan was defined as entry into follow-up (“baseline”). The end of follow-up was defined as either the date of a cardio- or cerebrovascular event or the date of the telephone interview.
The sample size for the control group was calculated with the assumptions that the difference in mean TBR between the event group and the control group was 0.3, the SD was 0.4, and the statistical power was 0.80, leading to a group size of 293. To prevent any overestimation of hazard ratios due to a reduction of the control group but not the event group, we used a weighting factor of 2 in the Cox model. The multivariate Cox proportional hazard model was used to obtain hazard ratio estimates and 95% confidence intervals for mean TBR, calcified plaque sum, and presence of established risk factors. Based on multiple threshold estimations, the following values were selected: mean TBR, <1.7 and ≥1.7; calcified plaque sum, <15 and ≥15. For univariate analysis of time-to-event data, Kaplan–Meier survival curves were constructed including log-rank tests.
The SAS statistical package (version 9.1 for PC; SAS Institute Inc.) was used to conduct the analyses. P values below 0.05 were considered to be significant.
Intraclass correlation coefficients (ICCs) with 95% confidence intervals were calculated to test the intra- and interreader agreement for the mean TBR and the calcified plaque sum. An ICC value of unity indicates perfect agreement, with random or systematic differences between the 2 measurements decreasing the value of the ICC. Generally, ICC values greater than 0.8 are accepted as a measure of excellent reproducibility (17).
RESULTS
Patient Population
Relevant baseline characteristics of the patients are reported in Table 1. Patients who had a vascular event during follow-up were older, included a higher proportion of men, and had a higher prevalence of hypertension than did the control group. The prevalence of active smokers was higher in the vascular event group than in the control group, although this difference did not reach statistical significance (P = 0.054).
Baseline Characteristics of Study Population
The frequency of statin medication use and the other cardiovascular risk factors did not significantly differ between the 2 groups.
PET/CT
In the entire group of 334 patients (15 vascular events and 319 controls), a total of 2,672 arterial segments were evaluated and statistically analyzed. Of the 334 patients, 319 underwent CT with an intravenous contrast agent. In the remaining 15 patients, low-dose CT was performed for attenuation correction. When the SUVs from the blood-pool ROIs were compared, no significant difference was found between the group that had CT with a contrast agent and the group that had CT without (mean SUV, 1.15 ± 0.27 vs. 1.18 ± 0.20). Furthermore, when mean TBRs were compared, there was no difference between patients who had low-dose CT and patients who had diagnostic CT.
Twenty-eight of 334 patients (8.4%) showed a mean TBR ≥ 1.7, and 28 patients (8.4%) showed a calcified plaque sum ≥ 15. Seven patients had both a mean TBR ≥ 1.7 and a calcified plaque sum ≥ 15. The highest TBRs were documented in the descending and abdominal aorta as well as the aortic arch (1.51 ± 0.44 [0.43, 3.67], 1.57 ± 0.35 [1.00, 6.33], and 1.50 ± 0.44 [0.47, 3.67], respectively), whereas lowest TBRs were seen in the iliac arteries (1.21 ± 0.31 [0.67, 5.00]) and common carotid arteries (1.23 ± 0.27 [0.57, 2.33]). Calcified plaque scores were highest in the abdominal aorta (1.6 ± 1.6) and the iliac arteries (0.9 ± 1.4), and the lowest values were found in the ascending aorta (0.1 ± 0.5). Calcified plaque and TBRs showed a highly significant correlation in the aortic arch (r = 0.127, P < 0.05), in the descending and abdominal aorta (r = 0.144, P < 0.01, and r = 0.112, P < 0.05), and in the common carotid arteries (r = 0.153, P < 0.01) (Fig. 2A). No significant correlation was found between calcified plaque and TBR in the iliac arteries.

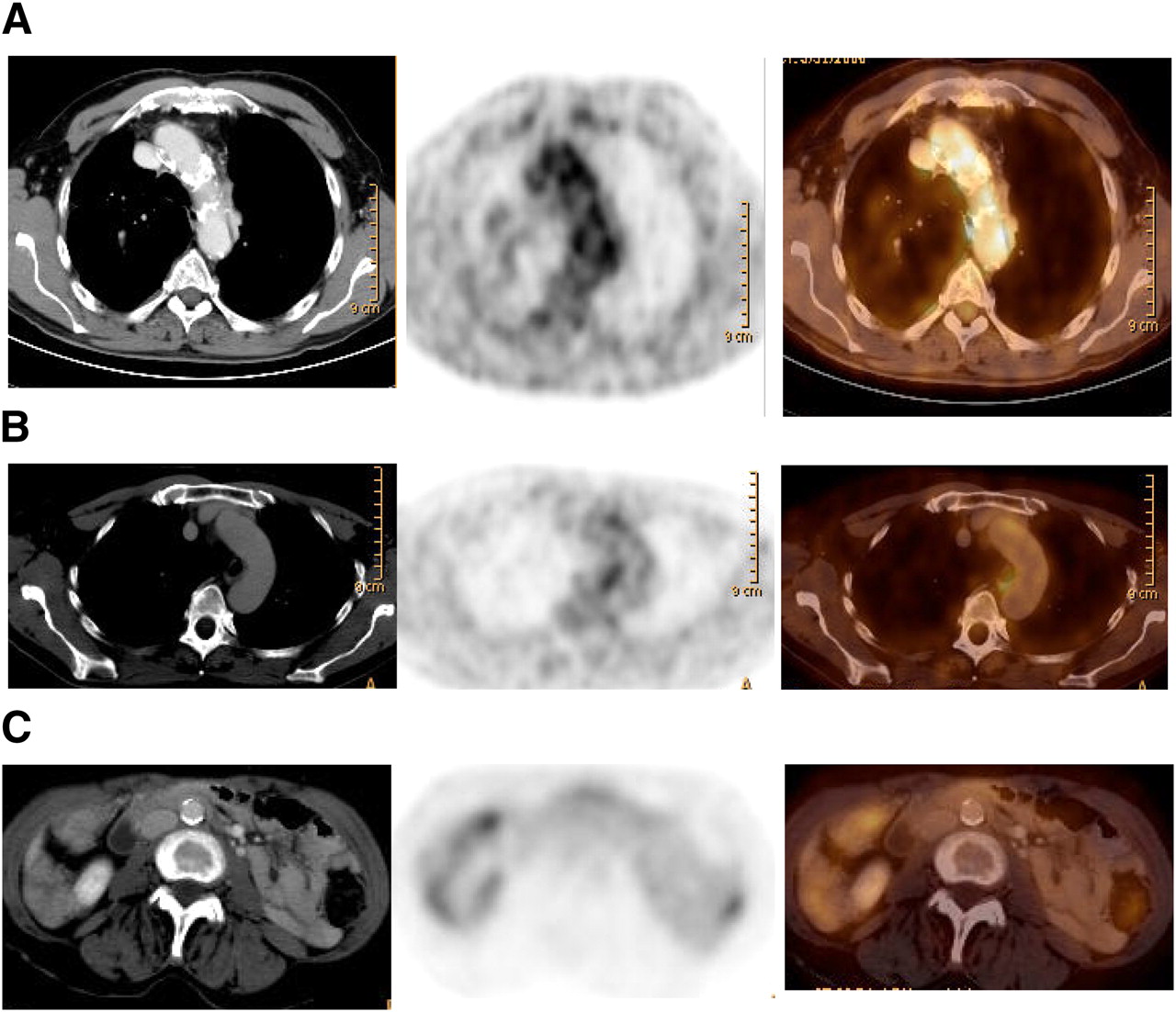
Arterial 18F-FDG uptake and calcifications in relation to patient outcome. From left to right are representative transaxial CT, 18F-FDG PET, and fused PET/CT images. (A) 81-y-old man with significantly increased uptake in region of aortic arch (TBR, 1.78; mean TBR, 1.62). Calcified plaque in aortic arch was 3, and calcified plaque sum was 21. Patient experienced myocardial infarction 14 mo later. (B) 45-y-old man with calcified plaque score of 0 in aortic arch (calcified plaque sum, 2) but aortic arch TBR of 1.90 (mean TBR, 1.74), who experienced vascular event 14 mo after PET/CT. (C) 64-y-old woman with calcified plaque score of 4 in abdominal aorta (calcified plaque sum, 14) and TBR of 1.49 in abdominal aorta (mean TBR, 1.56), who experienced no vascular event during follow-up.
Intrareader reproducibility was 0.84 (95% confidence interval, 0.48–0.96) for ICC and 0.80 (0.38–0.95) for TBR, whereas interreader reproducibility was 0.99 (0.96–0.99) for ICC and 0.98 (0.94–0.99) for calcified plaque.
Correlation of Baseline Parameters
Within the 334 subjects, a significant correlation was observed between calcified plaque sum and mean TBR (r = 0.187, P < 0.001). Although calcified plaque sum correlated significantly with age, the male sex, and all conventional cardiovascular risk factors except hypercholesterolemia, mean TBR correlated significantly with the male sex, age, and hypertension. Both mean TBR and calcified plaque sum correlated significantly with the occurrence of vascular events during follow-up (Table 2).
Correlation of Baseline Characteristics with Mean TBR and Calcified Plaque Sum
Five patients had a stroke during follow-up. TBRs in the carotid arteries were higher in these patients than in controls without events during follow-up (stroke patients vs. controls: 1.60 ± 0.32 vs. 1.18 ± 0.25 for the right common carotid artery and 1.64 ± 0.17 vs. 1.21 ± 0.25 for the left), indicating a trend toward higher TBRs before stroke.
Outcome Events and Survival Analysis
During a median follow-up of 29.0 (21.0, 33.0) months, 15 patients with a vascular event were registered (5 ischemic strokes, 7 coronary stent implantations after acute coronary syndrome, and 3 myocardial infarctions). The mean postscanning time to the event was 12.5 ± 8.8 (1, 29) months.
For the following calculations, the 15 vascular event patients and the 319 control subjects were considered as a single population of 334 patients with respect to mean TBR and calcified plaque sum as predictive factors. Nine of 28 patients (32%) with a mean TBR ≥ 1.7, and 6 of the 306 patients (2%) with a mean TBR < 1.7, had a vascular event during follow-up. Kaplan–Meier curves for mean TBR (cutoff, 1.7) showed a significantly inferior outcome for patients with a mean TBR ≥ 1.7 (P < 0.001; Fig. 3A). Figure 3B shows corresponding Kaplan–Meier curves for patients with calcified plaque sums ≥ 15 and < 15, where patients with a calcified plaque sum ≥ 15 also showed significantly decreased cumulative event-free survival (P < 0.001). Six of the 28 patients (21%) with a calcified plaque sum ≥ 15, but only 9 of the 306 patients with a calcified plaque sum < 15 (3%), had a cardiovascular event during follow-up. The combination of a calcified plaque sum ≥ 15 and a mean TBR ≥ 1.7 identified patients at highest risk for a future vascular event (P < 0.001; Fig. 3C).

Kaplan–Meier cumulative event-free survival curves: mean TBR using mean TBR cutoff of ≥1.7 (A), calcified plaque sum using calcified plaque sum cutoff of ≥15 (B), and combined subgroups of mean TBR and calcified plaque sum (C). *P < 0.01. **P < 0.001.
Cox regression hazard models identified mean TBR (hazard ratio, 14.144; P < 0.001) and calcified plaque sum (hazard ratio, 3.560; P = 0.025) as independent predictors for the occurrence of cardio- or cerebrovascular events (Table 3). Additionally, the presence of cardiovascular risk factors was a significant factor in the multivariate model (hazard ratio, 8.711; P = 0.038). In addition to the PET/CT findings listed above, univariate analysis identified the male sex (hazard ratio, 3.355; P = 0.027) as a predictor for vascular events, whereas patient age did not reach significance (hazard ratio, 2.181; P = 0.132).
Cox Proportional Hazards Model
Incremental Prognostic Value of Mean TBR
Six of 28 patients with a calcified plaque sum ≥ 15 had a vascular event during follow-up. These patients showed significantly higher TBRs (1.78) than did patients with a calcified plaque sum ≥ 15 without events during follow-up (mean TBR, 1.43; P = 0.014). Furthermore, 9 of 28 patients with a mean TBR ≥ 1.7 had a cardio- or cerebrovascular event during follow-up. These patients showed no significant difference in calcified plaque sum scores, albeit with a trend toward higher values (a mean calcified plaque sum of 10.7 in patients with events, vs. 5.7 in patients without events; Figs. 2B and 2C).
Interestingly, 5 of 21 patients (24%) with a calcified plaque sum < 15 had a vascular event during follow-up when the mean TBR was ≥ 1.7. On the other hand, only 2 of 21 patients (9.5%) with a calcified plaque sum ≥ 15 showed a vascular event during follow-up when mean TBR was < 1.7, whereas 4 of 7 patients (57.1%) with a calcified plaque sum ≥ 15 and a mean TBR ≥ 1.7 had a vascular event. Patients with a mean TBR ≥ 1.7 showed significantly increased event rates, compared with patients with a mean TBR < 1.7, independent of the calcified plaque sum scores (Fig. 3C).
Discrimination of High-Risk Patients
When the TBRs of a high-risk population, defined as 3 or more cardiovascular risk factors at baseline, were compared between those with and those without a cardiovascular event during follow-up, there was still a significant difference for both groups (mean TBR, 1.86 ± 0.56 vs. 1.40 ± 0.26; P < 0.05). Interestingly, no significant difference in calcified plaque sum was found between high-risk patients with and without cardiovascular events during follow-up (calcified plaque sum, 11.1 ± 7.0 vs. 9 ± 1.9).
Patterns of Inflammation and Calcification
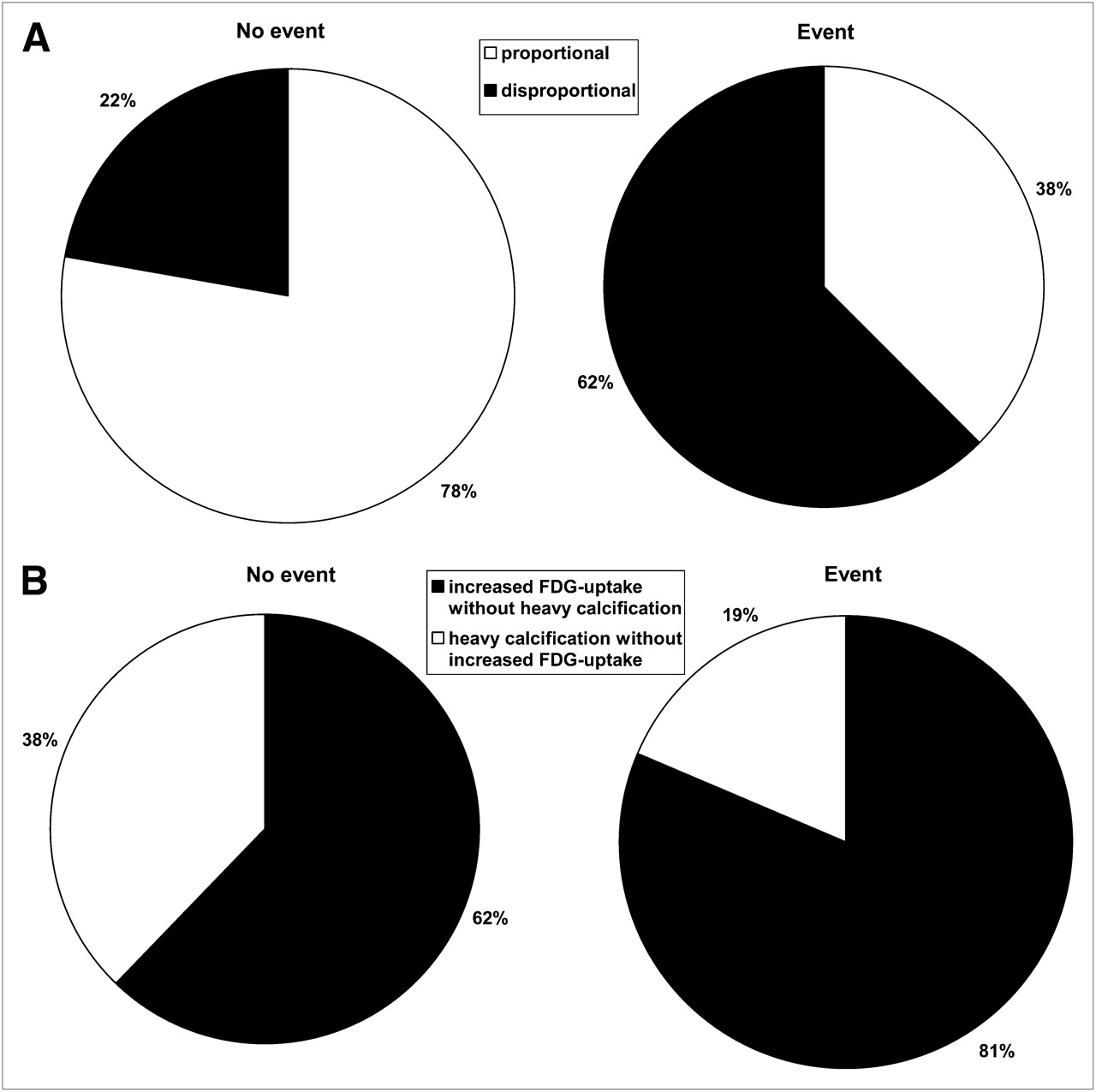
As indicated in Figure 4A, there was a clearly higher rate of disproportional distribution patterns for 18F-FDG uptake and calcified plaque scores in the small group of patients who had a vascular event during follow-up than in those without events (62% vs. 22%). Additionally, focusing on segments with disproportional distribution patterns, we found that patients with a vascular event during follow-up showed a higher rate of increased TBR and low calcified plaque values than did the control group (81% vs. 62%).
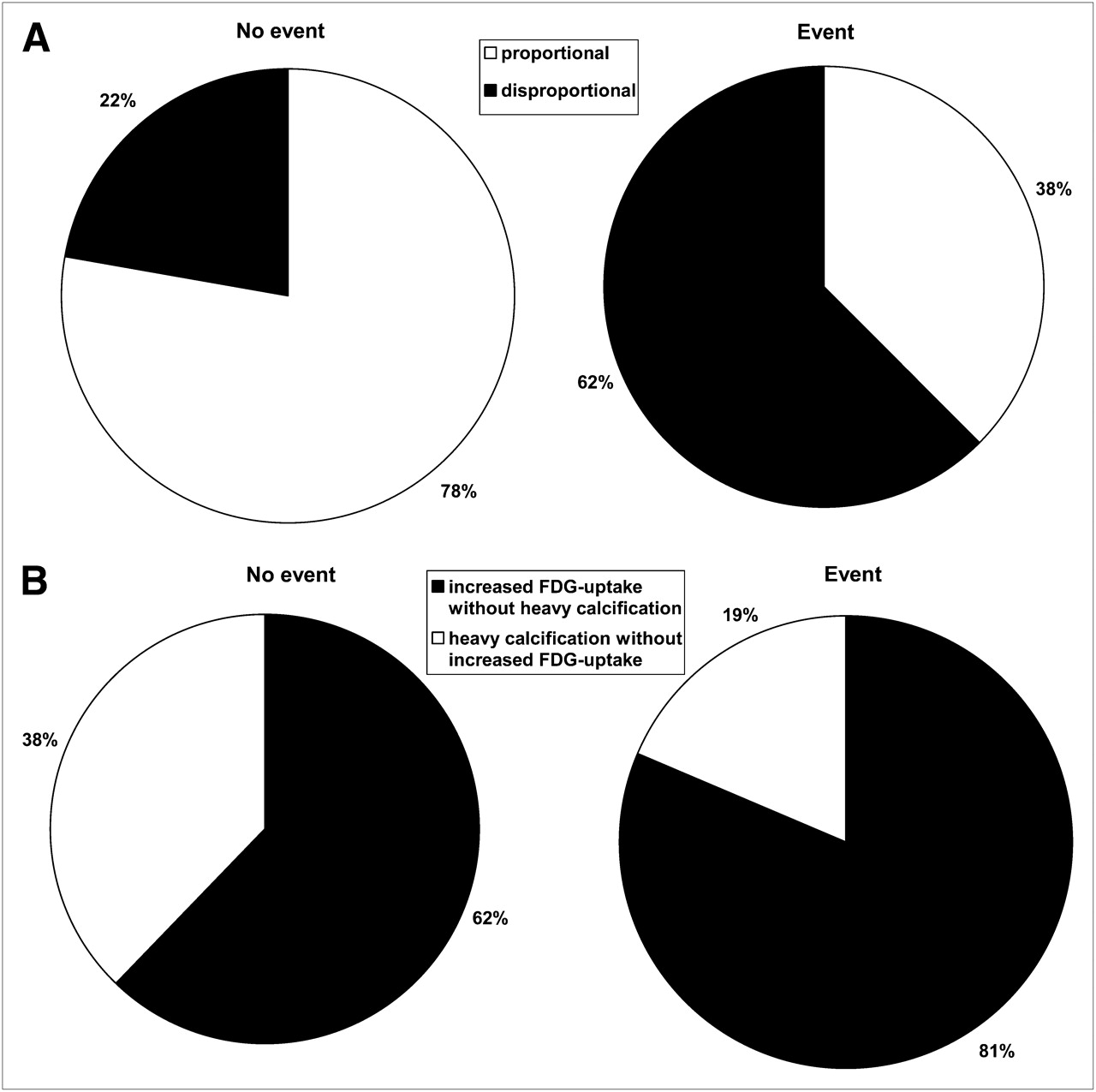
Distribution of arterial segments with different patterns of 18F-FDG uptake and calcifications in patients with and without vascular event during follow-up: proportional and disproportional distribution patterns in event group vs. control group (A); arterial segments with high TBR and low calcified plaque values vs. segments with low TBR and high calcified plaque values (B).
DISCUSSION
The need to establish a rational screening procedure for detecting preclinical atherosclerosis has become a topic of intense discussion in the medical imaging community. More than half of all first acute myocardial infarctions, and more than half of sudden cardiac deaths, occur in previously asymptomatic individuals (18). It seems likely that many of these events are preceded by undetected vascular changes, such as calcification or inflammatory infiltration of the large vessels. Verification of this claim in an asymptomatic cohort would require a PET/CT study in a large population, which would entail certain ethical and financial considerations. Therefore, we used cancer patients without a history of cardiovascular disease as a surrogate for the ideal, but practicably unattainable, nondiseased group. Multimodal vascular examination of PET/CT results in our large cohort, which was unselected for vascular event risk profile, enabled the evaluation of vascular changes in hundreds of subjects during several years of follow-up, such that risk factors for vascular events might be identified prospectively.
The results of this longitudinal multimodal imaging study suggest that increased 18F-FDG uptake in the walls of major arteries and increased calcium burden of the same vessels were both independent predictors for the subsequent occurrence of cardio- and cerebrovascular events in cancer patients. Insofar as these findings can be generalized to a healthy, asymptomatic population, the utility of 18F-FDG PET/CT for identifying asymptomatic patients with an increased risk for future vascular events is substantiated.
PET/CT
18F-FDG PET/CT has rapidly emerged as a noninvasive imaging technique that is eminently suited for staging and therapy monitoring of tumor patients (19), diagnosing inflammatory vascular disease (20), and performing cardiac imaging (21). 18F-FDG PET in conjunction with CT enables the combined functional and anatomic examination of the entire body; this approach has shown distinct advantages over either imaging modality alone in the diagnosis of many diseases. In particular, 18F-FDG PET/CT is of proven reliability for detecting inflamed plaques in the walls of large arteries while also providing the means for counting calcified plaques. These combined methods show excellent intra- and interreader reproducibility (7), as was confirmed by the present study.
Correlation of Baseline Parameters
Several previous studies reported significant correlations between focally increased 18F-FDG uptake in the walls of large arteries and the presence of conventional cardiovascular risk factors (22–26), as if risk factors predispose to inflammatory changes resulting in formation of plaques at risk for rupture. In all these studies, increased vascular wall 18F-FDG uptake was most strongly correlated with patient age. In addition, Ben Haim et al. also found significant correlations with the male sex and hypertension (22), which were confirmed in the present study. Interestingly, we found no significant correlation between hypercholesterolemia and the arterial 18F-FDG uptake score. It may be that those patients with hypercholesterolemia have already benefited from optimized antiinflammatory therapy, resulting in stabilization of their atherosclerotic plaques (27,28), especially given that all these variables were strongly covariant with increased number of arterial calcifications. The correlation between calcified plaque sum and increased cholesterol level indeed was not significant, but there was a trend toward higher calcified plaque scores in those patients (P = 0.12). In addition, the magnitude of calcified plaque sum correlated with all other vascular event risk factors, underlining its inherent association with the presence of atherosclerosis. Indeed, such an association has already been documented in several studies regarding coronary (29,30) and peripheral vascular calcifications (14).
Outcome Events and Survival Analysis
To our knowledge, only a single study to date has systematically investigated the covariance of increased 18F-FDG uptake and calcifications of the arterial wall with the occurrence of vascular events (24). In that study, on a series of 101 stable cancer patients, most of the registered vascular events occurred before the PET/CT scan. The study demonstrated that those patients with a recent history of vascular events, occurring within the 6 mo preceding the 18F-FDG PET/CT scans, showed significantly higher arterial wall 18F-FDG uptake scores than did patients without previous vascular events. In contrast, those patients whose vascular event had occurred more than 6 mo before PET/CT did not show significantly increased 18F-FDG uptake (24). In that study, vascular events were broadly defined to include cases of ischemic stroke, symptomatic chronic peripheral artery disease, acute peripheral ischemia, chronic coronary artery disease, acute coronary syndrome, any revascularization procedure, and aortic or peripheral aneurysm.
In our prospective study, increased 18F-FDG uptake and distinct arterial calcium burden were both highly associated with the occurrence of a vascular event during follow-up. Cox regression analysis, however, showed a 4-fold-higher hazard ratio for subsequent events with the mean TBR than with the calcified plaque sum score, and an incremental prognostic value over the calcified plaque sum score alone. Indeed, those patients in whom both mean TBR and calcified plaque sum score were increased were identified as being at highest risk for a vascular event during follow-up.
In accordance with findings published previously by other groups (14,15,23), we found that the highest scores for both calcified plaque and TBR were detected in the aortal region. Additionally, a significant correlation was found between calcified plaque sum and mean TBR within individual patients (r = 0.187, P < 0.01). Just as reported in the recent study by Paulmier et al. (24), those tumor patients with the greatest increase in arterial wall inflammatory activity, as revealed by 18F-FDG PET, also tended to have the largest number of calcified plaques. However, also as reported by several groups (15,22,31–33), zones of elevated vascular metabolic activity and vascular calcification were rarely found to overlap with such precision that they could be assignable to the same arterial lesion.
In general, 18F-FDG–avid vascular lesions are the product of a dynamic process such as transient inflammation (11,34), such that reduction of inflammation by medical therapy can frequently be visualized using 18F-FDG PET (27,28). On the other hand, the occurrence of arterial calcifications may indicate a stable and potentially late stage of atherosclerosis (35), unresponsive to medical treatment. Indeed, calcified plaques are rarely associated with an acute vascular event (36), even though the abundance of coronary artery calcifications is inherently related to the extent of coronary atherosclerosis (37). This seeming paradox is resolved if one considers that both TBR and calcified plaque represent different stages in the progression of atheroma, figuratively representing 2 sides of the same coin: TBR is a biomarker for unstable, vulnerable plaques likely to give rise to a vascular event, whereas calcified plaque is a surrogate marker for the presence of atherosclerosis, irrespective or independent of the plaque vulnerability. Further to the observations in the present study pertaining to the segmental distribution of lesions, we found that those patients who had a vascular event during follow-up showed a higher incidence of disproportionate patterns. These patients typically presented with foci of high 18F-FDG uptake in association with low calcifications, whereas the patients without severe events during follow-up tended to have more concordant findings.
Interestingly, both mean TBR and calcified plaque sum scores correlated with vascular events during follow-up independently of the conventional cardiovascular risk factors, such as family history of cardiovascular disease, hypercholesterolemia, diabetes, hypertension, and smoking. This observation is perhaps not surprising, as increased coronary and aortal calcium burden (14,38) has already been shown to have incremental value compared with conventional risk factors in the prediction of mortality from all causes. Our results have important implications for the comprehensive treatment of patients scheduled for diagnosis or staging of their cancer, who may not be regularly assessed for conventional atherogenic risk stratification; more widespread exploitation of the vascular 18F-FDG PET/CT results, although incidental with respect to the main oncologic findings, seems justified by the greater prognostic value imparted by conventional atherogenic risk factors for vascular events.
Limitations
The present study had several limitations. Obviously, PET/CT was performed on cancer patients, in whom cancer type and chemotherapies may have been a confounding factor in the expression of vascular pathology. Be that as it may, there emerged no significant relationship between the main tumor types (breast, ovarian, lung, and colorectal) and either the vascular findings or concurrent vascular event risk factors (results not presented in detail). Furthermore, the overall rate of vascular events was similar to the rate expected for an asymptomatic screening population, suggesting that treatment with antineoplastic agents or radiotherapy did not itself precipitate vascular changes leading to vascular events in our population. Cases of frank vasculitis were excluded from our study and in any event would scarcely have been identified as presenting focal intravascular 18F-FDG anomalies. The stringent national guidelines for recruitment of healthy control subjects (related to the radiation exposure of about 8 mSv per PET/CT examination using low-dose CT (39)) necessitated the present use of an ill cohort. Nonetheless, the present findings constitute a compelling rationale for conducting prospective PET/CT vascular examinations on patients without cancer and at risk for vascular events, with the aim of defining robust thresholds for mean TBR and calcified plaque sum as prognostic indicators.
Unfortunately, blood sampling for obtaining serum cholesterol levels was not routinely obtained in the present cohort, such that Framingham or similar risk scores could not be calculated. Instead, cardiovascular risk factors were systematically noted during the patients' first PET/CT visit at our institution. To obtain an optimally sensitive marker for the prediction of future cardiovascular events, we defined the presence of one or more cardiovascular risk factors as the threshold and implemented it as a variable in our multivariate Cox model.
The small number of vascular events registered during follow-up must be considered another limitation of this study. Although our observed percentage (1.6%) fell within the range expected for an asymptomatic screening population of this age composition, the much higher mortality due to oncologic disease (29%) in our cohort would have tended to reduce the number of vascular event cases. Because of the small number of vascular events, no more than 5 variables in the multivariate Cox model could be included. Consequently, we used a combined variable with a sensitive threshold with the existence of at least one risk factor.
Acquisition of the PET/CT images began approximately 60 min after 18F-FDG injection, as required for optimal detection of neoplastic tumors. However, somewhat longer 18F-FDG circulation times were recommended by Rudd et al. (7) for the detection of inflammatory plaques. Nonetheless, our use of the 60-min protocol seemed adequate for the purpose of the present study, although one might speculate that our findings would have been even stronger had we used a more specific PET protocol.
Acknowledgments
A substantial part of this work originated from the doctoral thesis of Sarah Wolpers. We thank Prof. Paul Cumming for critical revisions of the manuscript.
Footnotes
-
↵* Contributed equally to this work.
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication April 14, 2009.
- Accepted for publication June 30, 2009.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Continuous positive airway pressure but not Liraglutide-mediated weight loss improves early cardiovascular disease in obstructive sleep apnea: Data from a randomized proof-of-concept study
- Vascular Inflammation in Subclinical Atherosclerosis Detected by Hybrid PET/MRI
- Unraveling Vascular Inflammation: From Immunology to Imaging
- Association Between Osteogenesis and Inflammation During the Progression of Calcified Plaque Evaluated by 18F-Fluoride and 18F-FDG
- Head-to-Head Comparison of Inflammation and Neovascularization in Human Carotid Plaques: Implications for the Imaging of Vulnerable Plaques
- Arterial and Cellular Inflammation in Patients with CKD
- Positron Emission Tomography Assessment of Left Main Coronary Arterial Inflammation With Coronary Computed Tomographic Angiography Validation Before and After Statin Therapy: More Promise for Fluorodeoxyglucose Vascular Uptake?
- Coronary Plaque Morphology and the Anti-Inflammatory Impact of Atorvastatin: A Multicenter 18F-Fluorodeoxyglucose Positron Emission Tomographic/Computed Tomographic Study
- GlycA Is a Novel Biomarker of Inflammation and Subclinical Cardiovascular Disease in Psoriasis
- Evaluation of 68Ga-Glutamate Carboxypeptidase II Ligand Positron Emission Tomography for Clinical Molecular Imaging of Atherosclerotic Plaque Neovascularization
- Thresholds for Arterial Wall Inflammation Quantified by 18F-FDG PET Imaging: Implications for Vascular Interventional Studies
- GM-CSF Enhances Macrophage Glycolytic Activity In Vitro and Improves Detection of Inflammation In Vivo
- Arterial Stiffness Is Positively Associated With 18F-fluorodeoxyglucose Positron Emission Tomography-Assessed Subclinical Vascular Inflammation in People With Early Type 2 Diabetes
- Relationship Between Measures of Adiposity, Arterial Inflammation, and Subsequent Cardiovascular Events
- Radiotracer Imaging of Peripheral Vascular Disease
- Systemic Atherosclerotic Inflammation Following Acute Myocardial Infarction: Myocardial Infarction Begets Myocardial Infarction
- Carotid FDG Uptake Improves Prediction of Future Cardiovascular Events in Asymptomatic Individuals
- Nonpharmacological Lipoprotein Apheresis Reduces Arterial Inflammation in Familial Hypercholesterolemia
- A Randomized Trial on the Optimization of 18F-FDG Myocardial Uptake Suppression: Implications for Vulnerable Coronary Plaque Imaging
- Oxidized Low-Density Lipoprotein Stimulates Macrophage 18F-FDG Uptake via Hypoxia-Inducible Factor-1{alpha} Activation Through Nox2-Dependent Reactive Oxygen Species Generation
- Molecular imaging of atherosclerosis: clinical state-of-the-art
- Is Carotid Intima-Media Thickness as Predictive as Other Noninvasive Techniques for the Detection of Coronary Artery Disease?
- Imaging and Nanomedicine in Inflammatory Atherosclerosis
- Measurement of Arterial Activity on Routine FDG PET/CT Images Improves Prediction of Risk of Future CV Events
- 18F-FDG Imaging of Carotid Arteries for Identifying the Vulnerable Patient: Are We at the Beginning of the End?
- Radiotracer Imaging of Peripheral Vascular Disease
- Imaging of Arterial Inflammation: Keeping Our Cool on a Hot Topic
- Relation of Carotid Artery 18F-FDG Uptake to C-Reactive Protein and Framingham Risk Score in a Large Cohort of Asymptomatic Adults
- Bioenergetic Profiles Diverge During Macrophage Polarization: Implications for the Interpretation of 18F-FDG PET Imaging of Atherosclerosis
- Focal Arterial Inflammation Precedes Subsequent Calcification in the Same Location: A Longitudinal FDG-PET/CT Study
- Subclinical Vasculitis as a Potential Mechanism to Explain the Heightened Cardiovascular Risk in Rheumatoid Arthritis
- Impact of Noninsulin-Dependent Type 2 Diabetes on Carotid Wall 18F-Fluorodeoxyglucose Positron Emission Tomography Uptake
- Feasibility of 11C-Acetate PET/CT for Imaging of Fatty Acid Synthesis in the Atherosclerotic Vessel Wall
- Prevalence and Risk Factors of Carotid Vessel Wall Inflammation in Coronary Artery Disease Patients: FDG-PET and CT Imaging Study
- Imaging Inflammatory Changes in Atherosclerosis: Multimodal Imaging Hitting Stride
- Incidental Diagnosis of Thrombus Within an Aneurysm on 18F-FDG PET/CT: Frequency in 926 Patients
- Imaging Atherosclerosis With F18-Fluorodeoxyglucose Positron Emission Tomography: What Are We Actually Seeing?
- Correlation of Inflammation Assessed by 18F-FDG PET, Active Mineral Deposition Assessed by 18F-Fluoride PET, and Vascular Calcification in Atherosclerotic Plaque: A Dual-Tracer PET/CT Study
- Vessel Wall Inflammation in Spontaneous Cervical Artery Dissection: A Prospective, Observational Positron Emission Tomography, Computed Tomography, and Magnetic Resonance Imaging Study
- Imaging the Vulnerable Plaque
- Association of Adiponectin, Resistin, and Vascular Inflammation: Analysis With 18F-Fluorodeoxyglucose Positron Emission Tomography
- In Vivo Imaging of Mineral Deposition in Carotid Plaque Using 18F-Sodium Fluoride PET/CT: Correlation with Atherogenic Risk Factors
- The Year in Molecular Imaging
- Imaging Atherosclerotic Plaque Inflammation by Fluorodeoxyglucose With Positron Emission Tomography: Ready for Prime Time?
- The Role of 18F-FDG PET in Aortic Dissection
- In Vivo Imaging of Macrophage Activity in the Coronary Arteries Using 68Ga-DOTATATE PET/CT: Correlation with Coronary Calcium Burden and Risk Factors