


Abstract
The purpose of this study was to compare various PET/CT examination protocols that use contrast-enhanced single-phase or contrast-enhanced multiphase CT scans under different breathing conditions. Methods: Sixty patients with different malignant tumors were randomized into 4 different PET/CT protocols. Single-phase protocols included an intravenous contrast–enhanced (Ultravist 370; iodine at 370 mg/mL) single-phase whole-body CT scan (90 mL at 1.8 mL/min; delay, 90 s) during shallow breathing (protocol A) or during normal expiration (NormExp; protocol B). Multiphase protocols included 2 separate CT scans in the arterial contrast enhancement phase (90 mL at 2.5–2.8 mL/min; bolus tracking; scan range, base of the skull to the kidneys) and the portal-venous contrast enhancement phase (delay, 90 s; scan range, base of the lungs to the proximal thighs) during shallow breathing (protocol C) or during NormExp (protocol D) followed by a low-dose CT scan during shallow breathing for attenuation correction and whole-body PET. Feasibility was assessed by comparing the misalignment of the upper abdominal organs quantitatively by means of the craniocaudal, lateral, and anterior–posterior differences on coregistered PET/CT images. For image quality, the occurrence of CT artifacts and mismatching of rigid body points were evaluated qualitatively. Results: Misalignment was significantly lower for protocol B in almost all organs and represented the best coregistration quality. Surprisingly, protocol A showed significantly better alignment than the multiphase CT scans during NormExp. Misalignment values between the multiphase protocols were not significantly different, with a trend toward lower values for protocol D. The best CT image quality, with a significantly lower occurrence of artifacts, was found for protocols B and D (NormExp). The levels of mismatching of rigid body points because of patient movement in between the transmission and emission scans were similar for all protocols. Conclusion: Multiphase CT protocols presented a technical disadvantage represented by suboptimal image coregistration compared with single-phase protocols. Nevertheless, multiphase protocols are technically feasible and should be considered for patients who will benefit from a contrast-enhanced multiphase CT examination for diagnosis.
Diagnostic image quality plays a key role in the detection of diseases. Since the introduction of hybrid scanners delivering different types of diagnostic information, such as PET and CT (1,2), excellent performance and optimization of diagnostic methods are of utmost interest.
Complementary information for anatomic structures and metabolism leads to a benefit in diagnostic imaging not only because of simple coregistration of separate methods but also because of the high reproducibility of the simultaneous use of 2 innovative methods. The latest generation of PET/CT scanners, with multidetector CT in combination with high-resolution PET, allow faster and more exact image acquisition. The adaptation of imaging protocols for ultrafast imaging has been performed on stand-alone PET and CT scanners but should improve the value of combined imaging as well; therefore, imaging protocols have become an important consideration (3–5).
A variety of imaging protocols have been reported in the literature (3–8). These reports have elucidated the diagnostic necessity of CT contrast medium or the combination of contrast-enhanced attenuation correction CT scans and PET. Furthermore, breathing protocols have been designed for the prevention of motion artifacts, especially in the upper abdominal organs (4,9–12). Until now, CT expiration protocols have been preferred despite the facts that the emission scan is performed during shallow free breathing and there will be a decrease in diagnostic CT quality, especially in lung tissue.
The question arises as to whether it is possible to perform a full diagnostic CT scan with different contrast phases in combination with a whole-body PET emission scan. Finding a dedicated breathing protocol should permit a diagnostically powerful coregistration of PET and multiphase CT scans. Such a method would require an ultrafast multislice CT scanner that is equipped with a 4-row or 16-row multidetector system and that can scan without increasing examination time.
To study this concept, we used 4 different contrast-enhanced CT image protocols with single-phase and multiphase CT scans. The alignments of PET and CT protocols were analyzed during different breathing states. The diagnostic performance of CT scans should have approximated standard diagnostic image quality. We evaluated the misalignment of upper abdominal organs together with CT image quality as parameters of technical feasibility.
We hypothesize that the integration of multiphase CT protocols into a PET/CT examination is a technically feasible approach for the replacement of separate CT scans. However, with these protocols, a decrease in image fusion quality and an increase in scanning time have to be considered.
MATERIALS AND METHODS
Sixty patients were included in this study. The patients (age [mean ± SD], 58.2 ± 14.2 y; 38 men, 22 women) mainly had malignant diseases and were referred for a whole-body PET/CT scan with 18F-FDG. All patients gave written informed consent, and the studies were performed according to hospital guidelines for diagnostic procedures.
Patients fasted at least 6 h before the examination. Before the examination, patients received an intravenous injection of approximately 400 MBq (mean ± SD, 413.6 ± 42.5 MBq) of 18F-FDG. During the uptake phase of approximately 60 min (mean ± SD, 73.2 ± 13.8 min), patients were asked to drink 1 L of a water-equivalent oral contrast dispersion without known adverse effects on the accumulation of 18F-FDG (13).
Patients were preselected for multiphase or single-phase protocols depending on diagnostic CT procedures performed in the previous 3 mo to prevent superfluous radiation exposure. Patients were included in the study only if they had not undergone a diagnostic contrast-enhanced CT examination 4 wk before PET/CT. However, if patients had undergone a diagnostic contrast-enhanced multiphase CT examination between 1 and 3 mo before PET/CT, they were preselected into a single-phase protocol. The breathing protocols were randomized by the examination date to prevent systematic bias caused by age, sex, or disease. PET/CT was performed with one of the various protocols for 15 patients per group (Tables 1 and 2).
Anthropometric and Examination Data for Various Protocols
Pathologic Entities for Study Population and Distribution Within Protocols
PET/CT was performed with a dual-modality PET/CT tomograph (Biograph 16; Siemens Medical Solutions) consisting of an ultrafast CT scanner with a 16-row multislice detector system and a minimal rotation time of 0.5 ms. The intravenous contrast agent Ultravist 370 (Schering AG) was used; it has an iodine concentration of 370 mg/mL.
The PET scanner had a full-ring lutetium oxyorthosilicate system with a crystal size of 4 × 4 mm2. Three-dimensional PET was performed from feet to head; scanning of the lower body parts was performed first. For the emission scan, the bed time was 3 min, resulting in a total PET scan time of approximately 20–25 min (7 or 8 bed positions) (Table 1; Fig. 1).
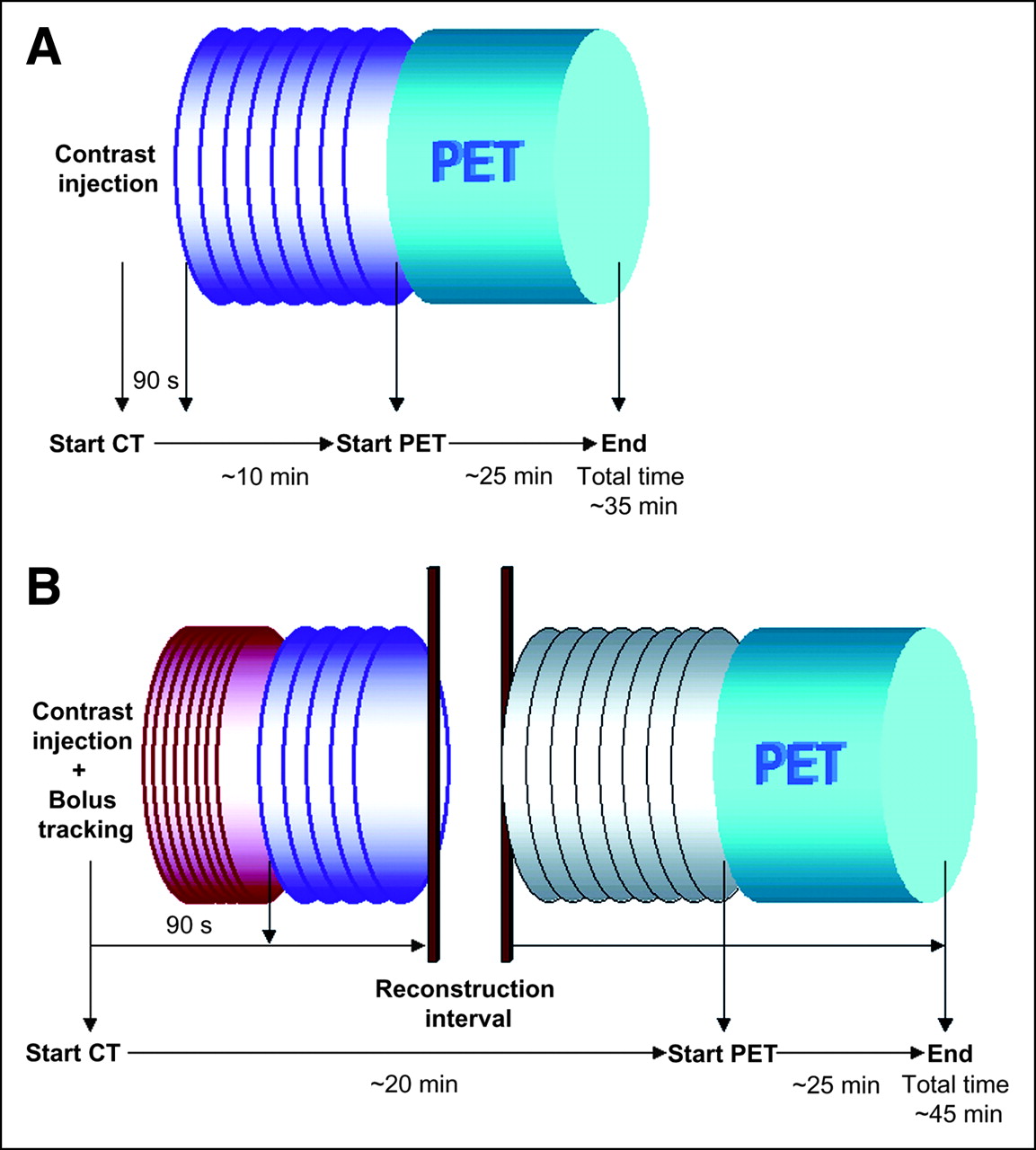
PET/CT protocols for single-phase (A) and multiphase (B) examinations. For protocol A, purple spiral represents whole body in portal-venous contrast enhancement. Scan range included base of skull to proximal thigh, as in PET (blue cylinder). For protocol B, 2 examination protocols had to be implemented because of technical standards of scanner. After injection and bolus tracking of contrast medium, first CT scan covered base of skull to lower borders of kidneys (red spiral). At 90 s after injection, CT ranging from base of lungs to proximal thighs was performed in portal-venous contrast enhancement phase (purple spiral). After short reconstruction interval, attenuation LD-CT (gray spiral) and PET were performed. Thickness of spiral lines indicates dose (thick line: 160 mAs; thin line: 30 mAs); width of spirals indicates collimation (narrow: 0.75; wide: 1.5).
CT data were used for attenuation correction as previously described by others (14). After attenuation and scatter correction of the PET data, images were reconstructed by use of an attenuation-weighted ordered-subsets maximization expectation approach (15) with 4 iterations and 8 subsets on a 128 × 128 matrix and with gaussian postfiltering of 5 mm.
Imaging Protocols
Single-Phase Protocols.
In accordance with general scanning procedures, CT was performed in the spiral mode. After acquisition of a topogram and definition of the scan range, continuous acquisition was performed in protocols A and B at 120 keV, 160 mAs, a collimation of 1.5, and a table feed of 24 mm. Images were reconstructed with a slice thickness of 5 mm.
Single-phase protocols included a contrast-enhanced whole-body scan covering the base of the skull to the upper thighs. This CT transmission scan also was used for attenuation correction in the reconstruction of PET data. The patients were positioned head first supine on the examination table with arms raised and with standard support for comfortable overhead positioning. Before the scan, 90 mL of contrast medium at a flow rate of 1.8 mL/s were administered, and a portal-venous phase (delay, 90 s) was used to prevent subclavian vein artifacts caused by a high concentration of contrast medium (Fig. 1A).
Patients were randomized to either protocol A, which included shallow breathing during the CT and PET scans, or protocol B, which included a CT examination in which patients were asked to hold their breath during normal expiration (NormExp) (11) and then a PET scan during shallow free breathing. In between the transmission and emission scans, there was a short break for image reconstruction. The patients then were moved into the PET gantry. Examination time ranged from 30 to 40 min.
Multiphase Protocols.
In contrast to protocols A and B, the multiphase protocols included multiple CT scans adapted for standard CT image quality before the PET scan.
After the administration of an intravenous contrast agent (90 mL; flow rate, 2.5–2.8 mL/s), bolus tracking was performed with the region of interest positioned on the descending aorta to cover the late pulmonary–arterial phase and the abdominal arterial phase. The arterial scan was performed at 120 keV, 160 mAs, a collimation of 0.75, and a table feed of 12 mm. This first scan covered the neck, the thorax, and the upper abdominal organs extending to the lower borders of the kidneys.
The second scan began at the base of the lungs and continued to the proximal thighs, including all abdominal and pelvic structures, in the portal-venous phase (delay, 90 s after injection). The portal-venous scan was performed with the same parameters as those described above for protocols A and B.
In a second examination protocol, which directly followed the CT scan after image reconstruction, a low-dose CT attenuation scan was performed (120 keV, 30 mAs, collimation of 1.5, table feed of 24 mm) before the PET emission scan. During the examination, patients were required to keep their arms elevated (Fig. 1B).
As for protocols A and B, patients were randomized to different breathing protocols for the contrast-enhanced CT scans, which included shallow breathing (protocol C) or a NormExp state (protocol D).
For all multiphase examinations, the low-dose CT attenuation scan and the PET emission scan were performed without a dedicated protocol during shallow breathing. For both breathing protocols, examination time was between 40 and 50 min (Fig. 1B).
Image Processing and Data Analysis
Image analysis was performed with a commercially available Syngo workstation (version VD 20K; Siemens Medical Solutions). For the assessment of alignment quality, CT and PET images underwent semiautomatic image fusion by use of a 3-dimensional tool kit with a linear mutual coregistration algorithm as described in previous publications (16,17). In cases of low-quality image fusion, manual coregistration was performed in the axial, sagittal, and coronal planes with reference to comparatively rigid body points (e.g., pelvis, promontorium, spine, and upper and lower extremities).
As an indicator of misalignment, the borders of the liver were identified on identical image planes on the PET and CT images. The distance between the organ border on the PET image and the equivalent organ border on the CT image was measured by methods described for the detection of organ misalignment (10,18,19). Measurements were obtained in the axial, sagittal, and coronal planes for representative midorgan sites. For the identification of organ borders on PET images, a fixed contrast scale was used according to a standardized uptake value ranging from 0 to 8. For better visualization, organs were enlarged on the monitor for single measurements.
Misalignment for each organ was given as the absolute length of the vector calculated from the 3 orthogonal distances as follows (10,20): √x2 + y2 + z2; in this equation, x, y, and z describe the distances between organ borders in the lateral, anterior–posterior, and caudocranial directions, respectively.
Additionally, CT image quality was assessed qualitatively for blurring artifacts caused by breathing or movements. Furthermore, noncompliance of patients in between the 2 examinations resulting in mismatching of rigid body points (e.g., pelvis, promontorium, spine, and upper and lower extremities) was assessed qualitatively (yes/no).
Statistical Evaluation
For data evaluation, an unpaired 2-tailed Student t test was used to detect differences in mean values for organ misalignment when protocols A, B, C, and D were compared. For the evaluation of multiphase CT scans within the same group, a paired Student t test was applied. A P value of <0.05 was considered significant; a P value of <0.005 was considered highly significant. Values are given as mean ± SD.
For differences in image quality based on the occurrence of artifacts on CT images or mismatching of rigid body points on coregistered PET/CT images, χ2 values were calculated. A P value of <0.05 was considered significant. Statistics and graphs were generated by use of SigmaPlot 2000 (SPSS Science).
RESULTS
Single-Phase CT
For protocol A (shallow breathing, portal-venous enhancement), we found a mismatch for the liver of less than 10 mm (mean value, 9.4 mm; range, 5.7–12.1 mm) (Fig. 2). There were CT artifacts in 10 of 15 cases (66.7%) as a result of breathing and mismatching of rigid body points (upper extremities) in 1 case (6.7%) (Fig. 3). For protocol B (NormExp, portal-venous enhancement), the mean value for mismatching was 6.2 mm (range, 3.2–9.4 mm) (Fig. 2). No CT artifacts and no mismatching of rigid body points were noted for this protocol, which produced good image quality. Unfortunately, 2 cases in this group were not included because of technical problems in the archiving system (Table 1; Figs. 2 and 3).
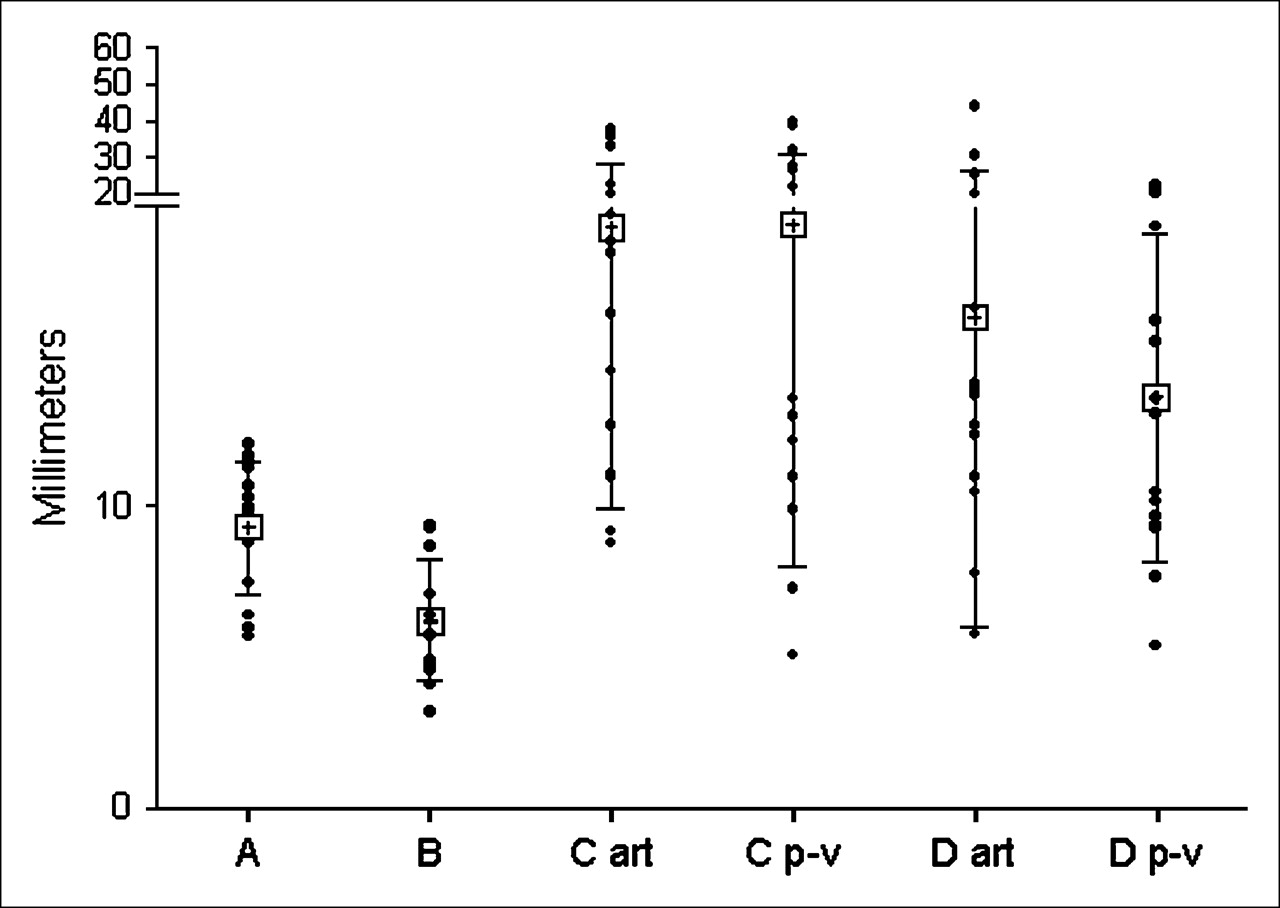
Comparison of misalignment of contrast-enhanced CT examinations for protocols A, B, C, and D. Protocol B (NormExp; single phase) had significantly lowest values for all abdominal organs. Significant differences between multiphase protocols (C and D) could not be assessed. art = arterial; p-v = portal-venous. • = individual values; + = mean values. Error bars indicate SDs.

Occurrence of image artifacts caused by breathing and severe mismatching caused by movements of patient in between CT and PET scans. Mismatching was distributed equally among protocols, whereas image quality correlated strongly with breathing protocols. NormExp protocols (B and D) had significantly lower occurrences of artifacts and, therefore, superior image quality. art = arterial; p-v = portal-venous.
Multiphase CT
Arterial Contrast Enhancement.
For protocol C (shallow breathing), the mean value for misalignment was 19.3 mm (range, 8.8–37.4 mm) (Fig. 2). CT artifacts were found in 11 of 15 cases (73.3%). Mismatching of rigid body points occurred in 2 of 15 cases (13.3%) (Fig. 3). For protocol D (NormExp), the mean value for misalignment was 16.3 mm (range, 5.8–44.0 mm). In 1 of 15 cases (6.7%), we found CT artifacts, and 2 of 15 cases (13.3%) showed mismatching of rigid body points (Figs. 2 and 3).
Portal-Venous Contrast Enhancement.
For protocol C (shallow breathing), the ranges of the mean values were similar to those of the arterial-phase CT scans. The mean value for the liver was assessed to be 19.4 mm (range, 5.1–39.5 mm) (Fig. 2). CT artifacts were found in 14 of 15 cases (93.3%). Mismatching of rigid body points did not occur in any cases (Fig. 3). The mean value for the liver in protocol D (NormExp) tended to be lower (mean value, 13.6 mm; range, 5.4–22.6 mm). CT artifacts were found in 3 of 15 cases (20%), and mismatching of rigid body points was found in 2 of 15 cases (13.3%) (Figs. 2 and 3).
Comparison of Alignment and Image Quality
When we compared the mean values of the contrast-enhanced CT examinations, we found a significantly lower value for protocol B (NormExp, single phase) than for all other protocols. Differences in mean values were highly significant (P < 0.005) for the liver (Fig. 2). We found significantly lower values for protocol A (shallow breathing, single phase) than for protocols C and D, accounting for both contrast-enhanced phases. When we compared the multiphase protocols, we found only a trend toward lower values for protocol D (NormExp); misalignment values were not significantly different in these protocols.
The occurrence of CT artifacts differed significantly according to the breathing protocols. As expected, we found a significantly higher occurrence of CT artifacts for protocols A and C than for protocols B and D. However, there were no differences between the NormExp protocols (B and D) and the shallow-breathing protocols (A and C) (Fig. 3).
Mismatching of rigid body points did not correlate with breathing protocols and was distributed equally among all protocols (Fig. 3).
Comparison of Attenuation Correction CT Scans in Multiphase Protocols
Surprisingly, as described above, we found lower misalignment values for the single-phase protocol during shallow breathing (protocol A) than for the multiphase protocol during NormExp (protocol D). To determine whether this finding was attributable to the fusion process implemented by the software system or was caused by patient noncompliance, we compared the diagnostically nonrelevant low-dose CT (LD-CT) scan, which was used for attenuation correction, and the arterial and portal-venous CT scans with protocols C and D. In both protocols C and D, the LD-CT was applied during shallow breathing.
For protocol C (shallow breathing), we found significantly lower values for the liver in the LD-CT than in the arterial and portal-venous phases (Fig. 4A). For protocol D (NormExp), there was a significantly lower value for the LD-CT than for the arterial phase (P = 0.04). We did not find a significant difference between the LD-CT and the portal-venous phase (Fig. 4B). Therefore, contrast-enhanced CT scans with protocol D failed to show superiority over attenuation scans applied during shallow breathing.

Multiphase PET/CT. Comparison of misalignment in protocol C (A) and protocol D (B). LD-CT attenuation scans were performed during shallow breathing. However, with regard to misalignment in liver, values for LD-CT were significantly lower. For protocol D, contrast-enhanced CT scan during NormExp did not show superiority over LD-CT scan during shallow breathing. Instead, values for LD-CT were significantly lower than those for arterial phase for liver. LD = low dose; ART = arterial; P-V = portal-venous. • = individual values; + = mean values. Error bars indicate SDs.
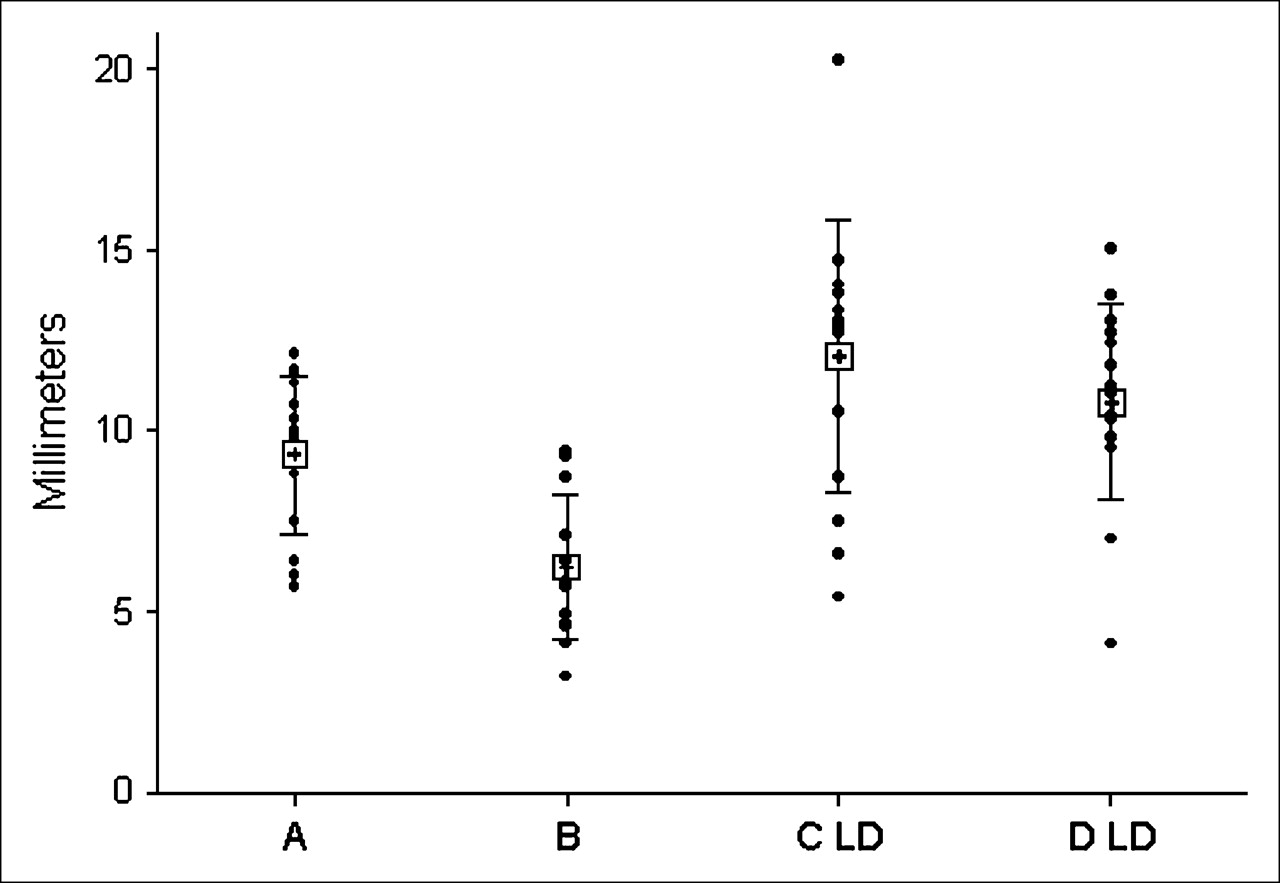
As expected, when the same breathing protocols were used, misalignment values in the LD-CT with both protocols were similar to those obtained with protocol A (Fig. 5). CT artifacts were not assessed because the LD-CT was used only for attenuation correction.

Comparison of CT attenuation scans. Protocol B showed lowest values for misalignment in all organs. Attenuation scans with protocol C (C LD) and protocol D (D LD) showed values similar to those with protocol A, as expected. • = individual values; + = mean values. Error bars indicate SDs.
DISCUSSION
In the present study, we compared intravenous contrast–enhanced single-phase CT with intravenous contrast–enhanced multiphase CT combined with whole-body PET by use of a high-performance dual-modality PET/CT system. Additionally, we defined breathing protocols to achieve optimal preconditions for good alignment and therefore good image quality in both PET and CT.
It was shown that a single-phase contrast-enhanced whole-body CT scan during NormExp results in significant superiority over 3 other protocols on the basis of the alignment of the liver in PET and CT. This type of protocol has technical advantages with regard to examination time and therefore the patient's comfort. For patients undergoing repeated diagnostic CT scans in a comparatively short time period or even in younger patients, radiation exposure should be considered in the choice of a protocol. Brix et al. (21) described an effective dose of approximately 25 mSv for a PET scan combined with a single-phase contrast-enhanced whole-body CT scan, which contributed approximately 18 mSv to the total exposure. In comparison, the radiation dose from CT alone with multiphase protocols would be significantly higher and would range from 25 to 30 mSv (22,23).
At present, there are many PET/CT protocols that follow the principles of a complete whole-body scan while modifying contrast injection into mono- or biphasic protocols inducing more-or-less relevant artifacts on corrected PET images caused by high concentrations of CT contrast medium (3–8). However, from a diagnostic point of view, such protocols would be only a compromise compared with a state-of-the-art multislice CT scan performed, for example, in the staging of cancer patients. The necessity of multiphase CT as performed with our study protocols may be subject to debate on principle (3); nevertheless, such a technique would be necessary for detecting lesions in some patients if neither 18F-FDG PET nor single-phase CT led to a clear diagnosis.
For technical feasibility, we used the parameter of misalignment of the liver, which has been described by other authors (10,18–20). Because of the character of the distribution of 18F-FDG, organ borders are identified best for the liver, whereas the kidneys and the spleen cannot always be distinguished clearly from their abdominal surroundings, leading to high misalignment values for these organs. The latter situation, in turn, decreases the reliability of fusion quality to a rather low level. Furthermore, the differences in organ borders along the z-axis contribute the most to the misalignment value (data not shown) and can be considered the most relevant (18,19) and highly predictive.
Surprisingly, the multiphase protocols showed significantly inferior quality of alignment even when compared with the single-phase whole-body scan (protocol A) during shallow breathing. One reason may be the reproducibility of the NormExp state, which varies during repeat CT scans. Other factors are the compliance of the patient and the frequency of as many as 3 CT scans before PET. Therefore, examination time increases by as much as about 10–15 min and may contribute to major discomfort for some patients.
Another reason for the comparatively low alignment quality may be the different fields of view of the whole-body PET scan and the multiphase CT scans, which only cover either the thorax and the upper abdomen or the abdomen and the pelvis. This property leads to a minor number of rigid body points that may be located on the PET scan but that are not seen on the CT scan; for example, upper parts of the spine or upper extremities are not seen on an abdomen–pelvis scan. Therefore, there is a discrepancy in comparisons of the results of single and multiphase protocols with regard to the mismatching of rigid body points, which did not vary among the protocols.
Overall, the differences in alignment were almost the same as the differences reported for separate-modality scanners (19); from a technical point of view, this finding is a clear disadvantage.
On the basis of image quality, examinations with the breath-hold technique as performed in protocols B and D clearly are superior to shallow free-breathing protocols and, furthermore, show better alignment than equivalent CT scans (Fig. 2). However, the NormExp state is not able to reveal small nodules in the lungs because of the small expansion of lung tissue. The result is a lack of sensitivity in the detection of such lesions because of the failure of the PET system to add information on such pathologies because its resolution is lower than that of multidetector CT. This situation would require an additional CT scan of the thorax because the presented protocols do not cover breathing states in full inspiration, which would be necessary for detecting small lung lesions. This option easily can be included in the examination protocol, for example, before the injection of contrast medium or even after the PET scan, with an acceptable moderate increase in the radiation dose and the examination time.
CONCLUSION
We assessed the technical feasibility of 4 different contrast-enhanced whole-body PET/CT examination protocols. We showed that multiphase CT with standard diagnostic quality reached by state-of-the-art examinations with a stand-alone scanner can be integrated into a standard PET/CT protocol and that coregistration is technically possible. However, the quality of alignment is significantly inferior compared with that of single-phase contrast-enhanced CT, which also is used for attenuation correction of the PET data.
The diagnostic accuracy of image interpretation was not evaluated in this study, but we attributed the lack of diagnosis to the use of single-phase contrast-enhanced or attenuation correction low-dose CT. This situation was especially true for patients with hypervascularized metastases or tumors. In such cases or even in patients without prediagnostic examinations, multiphase CT will be necessary for correct diagnosis and image interpretation. The technical standards needed to achieve good coregistration quality include a breath-hold technique for CT scans during NormExp, and quality should be improved by the use of fixation devices.
The effect of contrast enhancement in attenuation scans was not evaluated in this study but may be considered a minor factor in the diagnostic relevance and quality of the images, especially when late contrast enhancement phases with low-density peaks are used. Therefore, we strongly support and recommend the use of these protocols in clinical cases that will benefit from a multiphase contrast-enhanced CT examination.
Acknowledgments
We acknowledge our technical staff members, Henriette Heners and Sylvia Stotz, for excellent assistance during the studies and for the extra hours they worked. We also thank Stefan Kaepplinger from Siemens Medical Solutions and Fritz Schick from the Department of Diagnostic Radiology for giving useful advice and intellectual support.
References
- Received for publication July 23, 2005.
- Accepted for publication November 23, 2005.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- MRI-Based Attenuation Correction for Whole-Body PET/MRI: Quantitative Evaluation of Segmentation- and Atlas-Based Methods
- Dual-Modality Imaging: Combining Anatomy and Function
- Limitations of CT During PET/CT
- Value of contrast-enhanced multiphase CT in combined PET/CT protocols for oncological imaging
- Evaluation of Image Registration in PET/CT of the Liver and Recommendations for Optimized Imaging
- Adequate Evaluation of Image Registration in Hybrid PET/CT
- Reply: Adequate Evaluation of Image Registration in Hybrid PET/CT.