


Abstract
Although 18F-FDG examinations are widely used, data are lacking on the dose to human embryo tissues in cases of exposure in early pregnancy. Although the photon component can easily be estimated from available data on the pharmacokinetics of 18F-FDG in female organs and from phantom measurements (considering the uterus as the target organ), the intensity of embryo tissue uptake, which is essential for deriving the β+ dose, is not known. We report the case of a patient who underwent 18F-FDG PET/CT for tumor surveillance and who was later found to have been pregnant at the time of the examination (embryo age, 8 wk). Methods: The patient received 320 MBq of 18F-FDG. Imaging started with an unenhanced CT scan 1 h after the injection, followed by PET acquisition. PET images were used to compute the total number of β+ emissions in embryo tissues per unit of injected activity, from standardized uptake value (SUV) measurements corrected for partial-volume effects. A Monte Carlo track structure code was then used to derive the β+ self-dose and the β+ cross-dose from amniotic fluid. The photon and CT doses were added to obtain the final dose received by the embryo. Results: The mean SUV in embryo tissues was 2.7, after correction for the partial-volume effect. The mean corrected SUV of amniotic fluid was 1.1. Monte Carlo simulation showed that the β+ dose to the embryo (self-dose plus cross-dose from amniotic fluid) was 1.8E−2 mGy per MBq of injected 18F-FDG. Based on MIRD data for the photon dose to the uterus, the estimated photon dose to the embryo was 1.5E−2 mGy/MBq. Thus, the specific 18F-FDG dose to the embryo was 3.3E−2 mGy/MBq (10.6 mGy in this patient). The CT scan added a further 8.3 mGy. Conclusion: The dose to the embryo is 3.3E−2 mGy/MBq of 18F-FDG. The β+ dose contributes 55% of the total dose. This value is higher than previous estimates in late nonhuman-primate pregnancies.
Radiopharmaceuticals are occasionally administered to pregnant patients, either out of clinical necessity (for suspected pulmonary embolism, for example) or by accident (1,2).
In recent years, PET has become an essential component of cancer management. Several million 18F-FDG PET examinations are performed yearly worldwide. Reports of 18F-FDG PET examinations accidentally performed during pregnancy are exceedingly rare (3). Estimates of the dose received by the embryo or fetus are thus essentially theoretic.
Although the photon component can easily be estimated from available data on the pharmacokinetics of 18F-FDG in female organs and from phantom measurements (considering the uterus as the target organ in early pregnancy, and using specific anthropomorphic phantoms later on), precise data on the intensity of embryo tissue uptake, which are essential for deriving the β+ dose, are lacking.
We report the case of a woman who underwent 18F-FDG PET/CT in our institution and who was later found to be 8 wk pregnant (10 wk of amenorrhea) at the time of the scan.
Image-based embryo dosimetry was performed by summing the different components of the dose. The positron dose was estimated with a Monte Carlo simulation based on corrected standardized uptake values (SUVs). The photon dose was adapted from the MIRD schema. The CT component of the dose was then added.
MATERIALS AND METHODS
The patient, a 27-y-old woman weighing 60 kg, was referred to our department for follow-up of Hodgkin's lymphoma. The lymphoma had been diagnosed 2 y previously and treated with chemotherapy and radiotherapy. Because a residual mediastinal mass persisted on CT, the patient was considered to be in complete remission, unconfirmed. She had been pregnant the previous year and was referred for verification of the residual mass a few months after delivery.
Imaging was done with a Gemini PET/CT device (Philips) and started 1 h after injection of 320 MBq of 18F-FDG. Patients are asked to urinate just before imaging begins.
The Gemini PET/CT system consists of an Allegro 3-dimensional PET scanner in line with an Mx8000 EXP dual-slice CT system. The latter is programmed to acquire a low-dose CT scan (120 kV, 40 mAs/slice). No contrast medium was injected. PET image reconstruction used a 3-dimensional RAMLA algorithm. PET images were corrected for attenuation, scattered coincidences, and random coincidences.
On review of the images, and from information collected later, the patient was found to be pregnant. Ultrasound examination indicated that the embryo had been 55 d old (±3 d) at the time of the PET/CT examination.
For the dosimetry assessment, we focused on the 3 components of the embryo dose (β+ dose, photon dose, and CT dose).
Positron Dose
The SUV measured in the embryo and in the amniotic fluid was corrected for the partial-volume effect using the method developed by Frouin et al. (4). Then, from the corrected SUVs, we calculated the total number of disintegrations per unit of injected activity (assuming instantaneous tracer uptake and no removal). Monte Carlo calculation was then used to derive the β+ self-dose and the β+ cross-dose from amniotic fluid. Although the embryo self-absorbed positron dose could have readily been estimated using existing data in the literature—for example, using the OLINDA/EXM sphere self-dose model (5)—we chose a Monte Carlo simulation to also include the contribution from the surrounding amniotic fluid.
Geometric Model.
We considered that the embryo, at the date of the 18F-FDG study, had the average dimensions of a normal 8-wk embryo (6,7). The embryo was thus represented by a cylinder capped with hemispheres, with a total length of 3 cm and a diameter of 1.58 cm (volume, 4.84 cm3) (8). The embryo mass value we chose was also fairly consistent with the values reported in the ICRP 89 publication (9). The embryo was surrounded by a sphere 3.8 cm in diameter containing the amniotic fluid, as deduced from PET images.
Monte Carlo Simulation.
We used a code that has been described elsewhere and validated for dosimetric purposes (10,11). It was recently updated for positrons in liquid water (12), using recently published positron theoretic cross-sections (13). All positrons and secondary electrons are followed down to a cutoff energy of 12.6 eV. Photons are not considered in this Monte Carlo code. However, the fraction of photon energy that is retained in such a small structure (i.e., the photon self-dose of the embryo) is in the range of 2.3%–2.6% (14).
Photon Dose
The uterus is generally used as a surrogate of the embryo photon dose in early pregnancy (15), when it is assumed that the abdominal organs have not yet been displaced or changed in shape (16).
The photon dose to the uterus was obtained by summing the contributions from the surrounding organs.
Because the image acquisition was not dynamic but static (1 h after tracer injection), we had no information on the pharmacokinetics of the tracer in maternal tissue. We thus used published data on the pharmacokinetics of 18F-FDG in nonpregnant women (17,18) and calculated an average photon dose by using the dose equation of the MIRD committee (19), that is, S values for 18F in the nonpregnant female phantom were those published by the Radiation Dose Assessment Resource group (20).
S values for 18F in the nonpregnant female phantom were those published by the Radiation Dose Assessment Resource group (20).
CT Dose
When the uterus is included in the field of view of the CT scanner, the embryo doses are close to the volumetric CT dose index (CTDIvol) values (21). The CTDIvol, the main descriptor used to characterize patient exposure at a local dose level, represents an estimate of the average dose within an irradiated slice and thus reflects not only the combined effect of the selected scan parameters but also the effect of scanner-specific factors such as beam filtration, beam-shaping filter, geometry, and overbeaming (15).
In our patient, the CTDIvol value was corrected by the organ-specific dose coefficient (Γct-t, 1.11) suggested by Brix et al. (15), to obtain the final CT dose, as follows: D = Γct-t × CTDIvol.
RESULTS
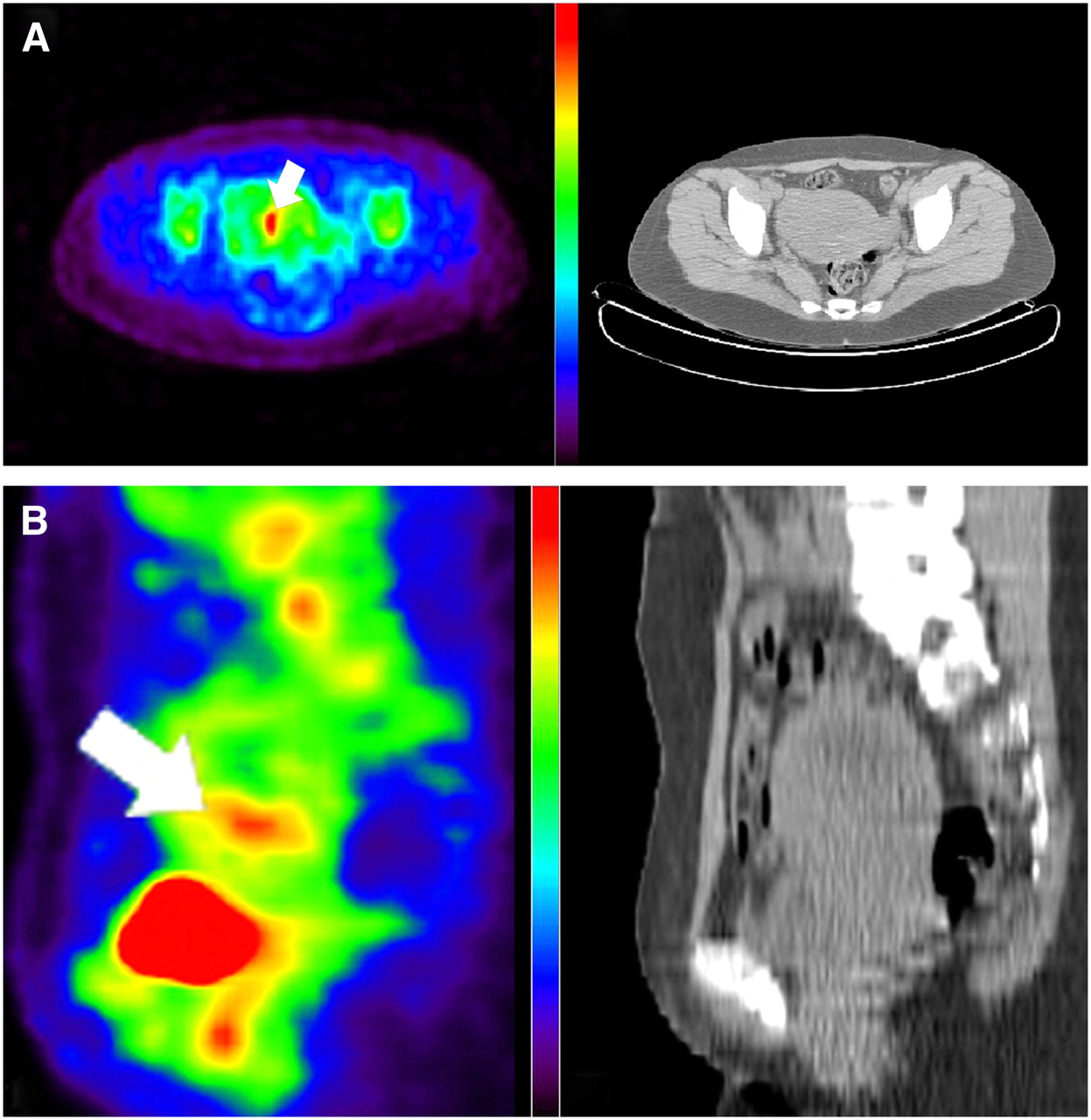
Figures 1A and 1B show a transaxial and a sagittal slice, respectively, through the uterus. The embryo is indicated by an arrow.

Transaxial (A) and sagittal (B) 18F-FDG PET (left) and CT (right) slices through uterus. Embryo is indicated by arrow.
The mean SUV in the embryo was 2.2. The maximum SUV was 2.7. This maximum SUV of 2.7 was found in 2 successive slices. After correction for the partial-volume effect (4), the corrected mean SUV was also 2.7, matching the maximum SUV of the uncorrected images. We thus used the SUV of 2.7 to derive the total number of disintegrations occurring in the embryo. The mean corrected SUV for intrauterine amniotic fluid was 1.1.
18F-FDG Dose
Positron Dose.
The total number of disintegrations occurring in the embryo was 2,070,000/MBq injected to the mother. The total number of disintegrations occurring in amniotic fluid was 4,158,000/MBq. Monte Carlo track structure simulation showed that, from a total positron energy of 5.15E11 eV released in embryo tissues (per MBq injected), 5.05E11 eV stays within the embryo. Amniotic fluid contributed a further 3.66E10 eV to the embryo. Summing the 2 contributions yielded a β+ dose to the embryo of 1.8E−2 mGy/MBq.
Photon Dose.
The photon cross-dose to the embryo, coming from maternal tissues, was calculated at 1.5E−2 mGy/MBq.
In total, the average dose to the embryo per unit of 18F-FDG activity administered to the mother was estimated at 3.3E−2 mGy/MBq (10.6 mGy in this patient, who received 320 MBq).
CT Dose.
The CT dose to the embryo, taking into account the relevant CTDIvol and the Gemini Mx8000 EXP dual-slice CT dose coefficient (Γct-t) for the uterus (15), was 8.3 mGy.
DISCUSSION
The absorbed dose from internal emitters is a major preoccupation (22), especially in the case of developing organs and tissues, which show increased radiosensitivity (2). Estimation of the specific absorbed doses to the embryo and fetus from radionuclide exposure of the mother is a challenging task. In the case of 18F-FDG administration to a pregnant woman, the dose to the fetus is given by the sum of photon emissions (principally deriving from maternal tissues) and the β+ dose (mainly absorbed as the self-dose).
Although the photon dose can be realistically approximated by using phantoms and mathematic models, fetal self-irradiation is more difficult to estimate. Data on radionuclide uptake by the embryo or fetus are rare, as they can be obtained only after accidental exposure or by extrapolating the results of animal experiments (1,23).
Our results suggest that the dose received by an 8-wk embryo is about 3.3E−2 mGy/MBq. This is higher than the dose estimated by Stabin (24), who reported a value of 2.2E−2 mGy/MBq up to the third month of pregnancy (and 1.7E−2 mGy/MBq in later pregnancy). This difference results from a higher estimate of the β+ contribution. We found that the β+ self-dose (1.8E−2 mGy/MBq) represented a major component of the total 18F-FDG dose in embryos (55% here).
Stabin made the assumption that the average concentration of 18F-FDG was the same in fetal tissues as in the mother (24). This assumption was based on a report by Benveniste et al. of similar 18F-FDG uptake in primates, as measured by mother–fetus SUV ratios (23). However, our data suggest that, at least in early pregnancy, uptake of 18F-FDG by human embryo tissues is higher.
Besides differences between nonhuman-primate and human physiology, this discrepancy may be explained by the following 3 considerations: First, the nonhuman-primate fetuses in the study by Benveniste et al. were at a later stage of development than was the human embryo described here (the youngest nonhuman-primate fetus was in the early second trimester). The embryonic phase is the main period of organogenesis, characterized by a rapid mass increase (7). Generally, higher cell proliferation is associated with more glucose consumption. Second, glucose is the principal energy substrate for the embryo and fetus. Its uptake is regulated by the expression of glucose transporters on the plasma membrane of embryonic cells (25). Third, the nonhuman primates in the study by Benveniste et al. were anesthetized with high doses of propofol (200–300 μg/kg/min), which is known to cross the placenta (26) and may possibly influence 18F-FDG uptake by the fetus.
For our estimation, we assumed that the SUV recorded 1 h after the injection was representative of the average concentration in the embryo over time. This was a necessary approximation, as we do not know the kinetics of 18F-FDG in embryo tissues.
We may have underestimated the real dose to the embryo from positrons: At this stage of pregnancy, the embryo is constantly moving in amniotic liquid, potentially leading to an underestimation of SUVs on PET images.
Moreover, the tracer distribution within the embryo is probably heterogeneous, even if, given the spatial resolution of the PET scanner used here, SUVs on the images appeared homogeneous. Thus, our study does not address the possibility of heterogeneous distribution of the dose at a microscopic level. Our work gives an estimate of the dose to the embryo per megabecquerel of 18F-FDG if this examination is performed out of necessity during early pregnancy or in cases of accidental exposure.
Our patient received 320 MBq of 18F-FDG, and the resulting radionuclide dose to the embryo was 10.6 mGy. After adding the dose of the unenhanced CT scan (8.3 mGy), we estimated that the total dose was 18.9 mGy. This dose remains well within the range of “safe” levels (27). Steenvoorde et al. reported that, at this stage of pregnancy, the risk to the embryo of malformation is about 0.05%/mGy, with a suggested threshold of 100 mGy. Growth retardation occurs after a threshold of 50–250 mGy (27). It remains, however, that combined PET/CT examinations result in a relatively high dose. The CT component of the dose depends on the characteristics of the scanner and increases if high-quality, contrast-enhanced CT is used (15). For example, CT doses to the uterus can vary by a factor of 5, depending on the scanner and protocol (28).
In a patient with a history of cancer, the relative risks from radiologic studies are to be considered along with those from other, more immediately hazardous exposures such as chemotherapy (29). Our patient had been pregnant on a prior occasion about 1 y after the completion of therapy for lymphoma, and the outcome of that pregnancy was normal. When a new pregnancy was discovered after the PET study, the patient was counseled that radiation risk was below the safety threshold; no specific recommendation was made. The patient delivered at term a healthy baby.
CONCLUSION
Uptake of 18F-FDG by embryo tissues in early pregnancy may be higher than previously postulated. Our data suggest that the embryo dose in early pregnancy is at least 3.3E−2 mGy/MBq administered to the mother. About 55% of this dose comes from positrons.
Because our data involve only 1 subject, they do not necessarily suggest a change in currently reported standard values (24). As other data become available in the future, the average from these studies may be used to establish a new recommended dose value.
Acknowledgments
The authors thank Dr. Yolande Petegnief and Dr. Michael G. Stabin for helpful discussions and David Young for editorial assistance.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 8, 2007.
- Accepted for publication December 19, 2007.





{kind=link}
Jump to section
Related Articles
Cited By...
- Fetal Dose from PET and CT in Pregnant Patients
- 18F-FDG Fetal Dosimetry Calculated with PET/MRI
- New Fetal Dose Estimates from 18F-FDG Administered During Pregnancy: Standardization of Dose Calculations and Estimations with Voxel-Based Anthropomorphic Phantoms
- Fetal Radiation Dose from 18F-FDG in Pregnant Patients Imaged with PET, PET/CT, and PET/MR
- 18F-FDG PET in Pregnancy and Fetal Radiation Dose Estimates
- Absorbed 18F-FDG Dose to the Fetus During Early Pregnancy