


Abstract
The fetal radiation dose from 18F-FDG was estimated in a series of pregnant women who underwent a PET scan during a clinical workup for malignancies. Methods: Six pregnant patients were injected with 18F-FDG (activity range, 296–385 MBq). Three patients were scanned during the first trimester (1 with PET and 2 with PET/CT), 2 were scanned during the second trimester (with PET/MR imaging), and 1 was scanned during the third trimester (with PET). The time-integrated activity coefficients were derived from the fetal radioactivity concentrations measured on the images for all but 1 patient (in early pregnancy [5 wk]), in whom the activity in the uterus was used as a proxy. The coefficients of the mother’s organs were derived from standard values (from the International Commission on Radiological Protection). Results: Fetal doses ranged from 6.29E–03 to 2.46E–02 mGy/MBq. An earlier bladder voiding reduced these doses by 25%–45%. The 2 patients who underwent PET/MR imaging—in whom fetal contours could be accurately delineated—displayed the lowest fetal absorbed dose, likely because of more accurate region drawing, with the inclusion of areas of both low and high fetal uptake. Moreover, PET/MR imaging did not necessitate additional radiation for attenuation correction. The placenta, delineated on a PET/MR imaging scan, concentrated 0.27% of the injected activity. Conclusion: Fetal radiation doses are higher in early pregnancy than in late pregnancy, and there can be considerable intersubject variability. However, the total absorbed dose is always well below the threshold for noncancer health effects throughout pregnancy. PET/MR imaging is the optimal PET procedure for imaging pregnant women because it is not associated with radiation for attenuation correction and allows more accurate dosimetric calculations.
Cancer staging with 18F-FDG is the main reason for the widespread use of PET technology in clinical practice. Between 2001 and 2010, the annual number of PET scans performed in the United States increased nearly 7-fold (from ∼250,000 to >1.7 million) (1), and 18F-FDG is used for most PET examinations. As a consequence, an ever-increasing number of pregnant women are injected with radiopharmaceuticals (2). Fetal radiation exposure may be accidental if the pregnancy is unknown at the time of the PET scan (3–6) or may be the consequence of a diagnostic workup for cancer in the mother (7–9). In both cases, knowing the fetal absorbed dose is important for correctly assessing the risk to the fetus and for putting this risk in perspective against the clinical benefit for the mother.
18F-FDG crosses the placental barrier and accumulates in fetal tissues (3,4,7,10). Therefore, the resulting fetal self-dose can be determined only from actual in vivo data. The first in vivo data were published in 2003 by Benveniste et al., who studied placental crossover and 18F-FDG uptake in nonhuman primates at a late stage of pregnancy (11). These data constitute the basis of the currently adopted standard dosimetry values for 18F-FDG fetal exposure, which are 2.2E–02 mGy/MBq for the first trimester of pregnancy and 1.7E–02 mGy/MBq after the first trimester (12).
Dosimetry from several cases of women at different stages of pregnancy subsequently became available (3,4,7,8,13), but the results were sometimes contradictory. Two cases in early pregnancy suggested that the absorbed dose might be higher than standard values (3,4). In contrast, a recent series of 5 different pregnant women showed that the dose might actually be lower than standard values in all trimesters, especially in later pregnancy (13).
In this study, we aimed to significantly expand the available dosimetric data by performing dose calculations for a new series of 6 women who were pregnant for 5 wk–7 mo and who were imaged with 3 different modalities (PET only, PET/CT, and PET/MR imaging).
MATERIALS AND METHODS
Patients
The images from 6 pregnant women (23–39 y old) referred to the Nuclear Medicine Department, School of Medicine, Washington University, St. Louis, Missouri, were retrospectively analyzed. The institutional ethics board approved this retrospective study, and the requirement to obtain informed consent was waived.
All patients underwent 18F-FDG scans as part of a diagnostic workup for cancer. The patients gave their consent to the procedure after careful explanation of the possible risks and benefits associated with the use of ionizing radiation. The patients had cancer in the vocal cord (patient 1); in the cervix (patient 2); in the breast, with metastases to the axilla, upper sternum, and pericardium (patient 3); Hodgkin lymphoma in the neck, axilla, and mediastinum (patient 4); Burkitt lymphoma in the head and neck (patient 5); and melanoma of the left lower limb, with inguinal lymph node metastasis (patient 6). The 6 pregnancies were distributed across the 3 trimesters, ranging from a 5-wk (early) pregnancy to a 7-mo (late) pregnancy (Table 1).
Characteristics of Patients, Fetal Fractions, and Time-Integrated Coefficients
Before injection, the patients received intravenous hydration with saline solution. For all 6 patients, a Foley catheter was placed in the bladder to drain radioactive urine and thus reduce the fetal photon exposure. The average injected activity was 328 MBq (range, 296–385 MBq).
Because the patients were imaged over a time span of many years, 3 different scanners were used. Two patients underwent a PET-only scan with a Siemens ECAT EXACT 962 PET scanner. Attenuation correction was performed with a 68Ge source. The images from 1 of these 2 patients were previously used in an online teaching file, but without individual dosimetric estimation (14). Two patients underwent a PET/CT scan with a Siemens Biograph Truepoint lutetium oxyorthosilicate 40-slice PET/CT scanner. The CT acquisition was done with a low-dose radiation exposure (111 mAs effective, 120 keV) and additional modifications in accordance with the vendor’s CARE Dose Beam Modulation (Siemens Medical Solutions). The last 2 patients were scanned with a modern PET/MR imaging camera (Siemens Biograph mMR), and attenuation correction was performed with the 2-point Dixon technique (15).
Dosimetric Calculations
The fetal volume and concentration of radioactivity were calculated for each patient by manually drawing a region of interest around the whole fetus on the PET images. For the 2 patients who underwent PET/MR imaging, the fetal contours were defined on the coregistered MR images. The 5-wk fetus of patient 1, who underwent a PET/CT scan, was not clearly visible on the images of either modality; therefore, as in the approach adopted by Takalkar et al. (13), the dose to the uterus was used as a proxy. The time-integrated activity coefficients for the fetuses (or the uterus for patient 1) were combined with the standard coefficients for the mothers’ organs, taken from ICRP publication 106 (16). The time-integrated activity coefficients were entered into OLINDA/EXM software (17) to obtain the final doses. An anthropomorphic phantom of a pregnant woman in the first trimester was used for patients 2 and 3, a phantom of the second trimester was used for patients 4 and 5, and a phantom of the third trimester was used for patient 6. For the patient in early pregnancy (patient 1), the time integral for the uterus was attributed to the uterus of a phantom for an adult nonpregnant woman.
Because only a static image was acquired for each patient, the physical half-life of 18F-FDG was considered to be equal to the effective half-life of the isotope. For assessment of the impact of bladder voiding on the fetal dose, the OLINDA/EXM dynamic bladder model was used with 2 different voiding times (1 and 3.5 h).
In 1 of the 2 patients who underwent PET/MR imaging (patient 4), the placenta was clearly distinguishable from the uterine wall and the amniotic fluid. This clear visualization allowed accurate manual delineation of its contours and calculation of the percentage of injected activity concentrated by the placenta. The photon dose from the placenta to the fetus is likely to be negligible (10) and was not considered for dose estimation.
RESULTS
The characteristics of the patients, fetal fractions (fraction of injected activity concentrated by the fetus), and time-integrated coefficients are summarized in Table 1.
The fetus was clearly visible on the PET images from all patients except patient 1, for whom the whole uterus was used for dosimetric calculation.
Fetal uptake was generally similar to or slightly higher than the average background activity seen in the mothers’ organs (Fig. 1). In the more mature fetuses (i.e., in the second and third trimesters), areas of prominent uptake were seen in the myocardium and in the abdominal region (most likely the urinary activity in the kidneys and the bladder). No particular uptake was present in the brain of any fetus.
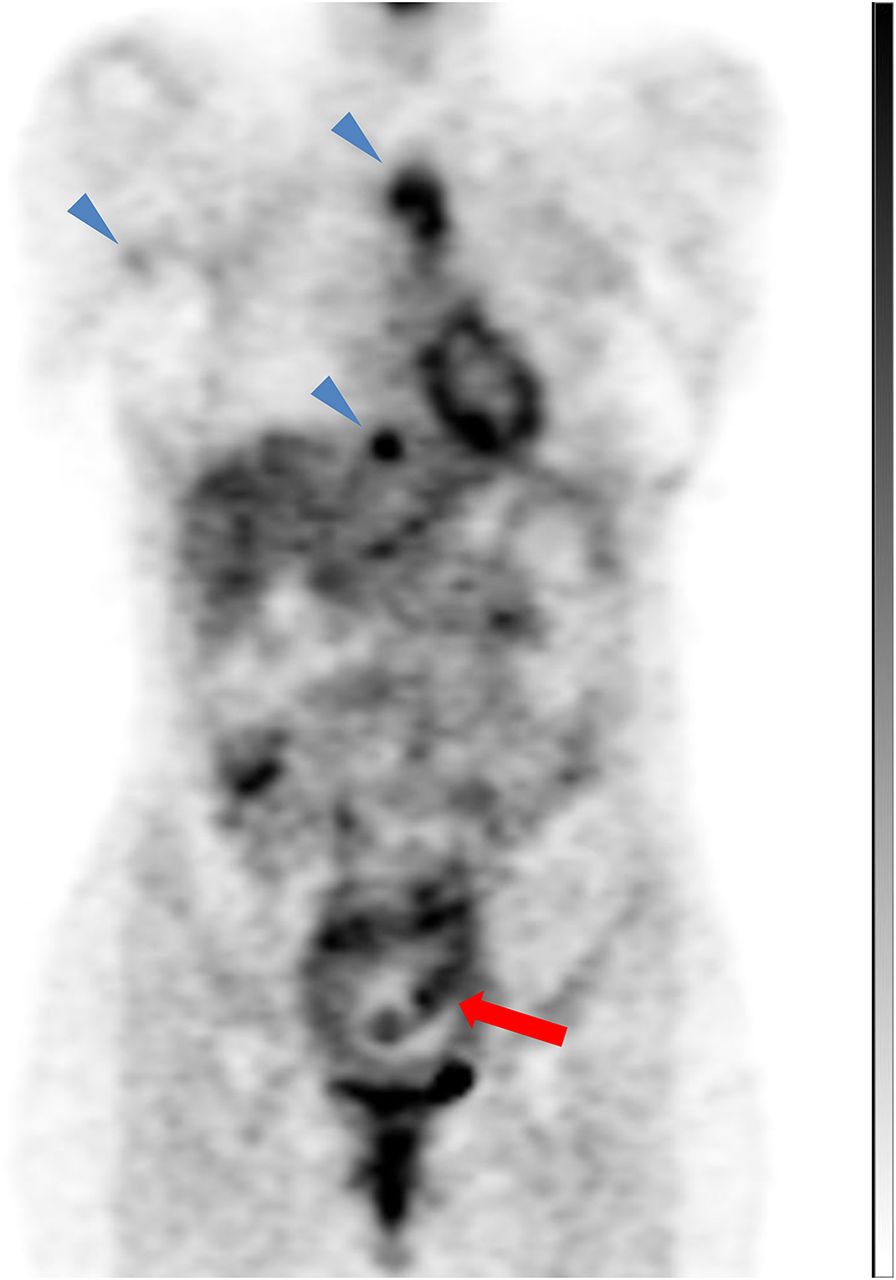
Coronal 18F-FDG PET image of patient (patient 3) monitored for breast cancer, with metastases to sternum, pericardial region, and right axilla (blue arrowheads). Patient had been pregnant for approximately 3 mo, and fetus is clearly visible inside uterine cavity (red arrow).
The 2 fetuses imaged with PET/MR imaging were visible in fine detail on the MR images (Figs. 2 and 3); therefore, fetal contours could be delineated precisely. Interestingly, the MR imaging–derived fetal regions of interest encompassed several areas of low 18F-FDG uptake on PET (Fig. 4).
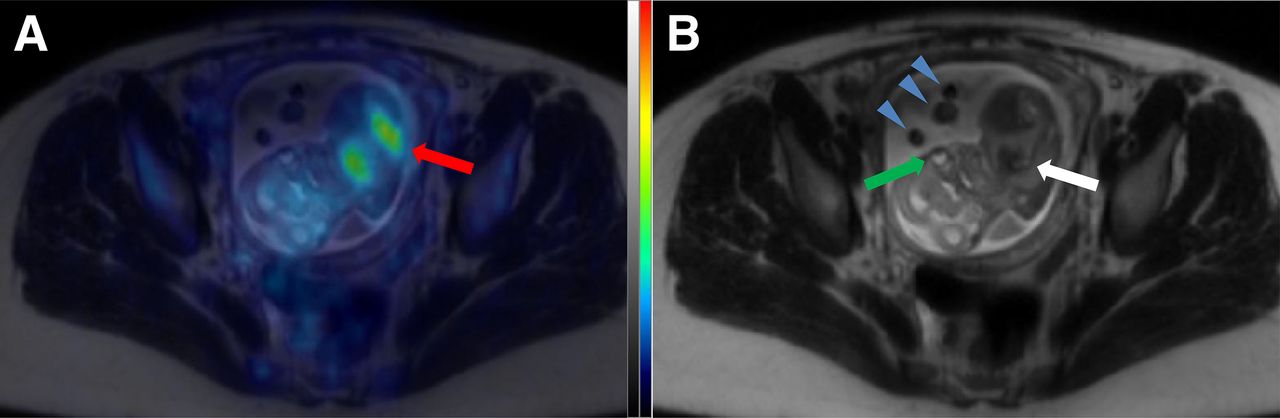
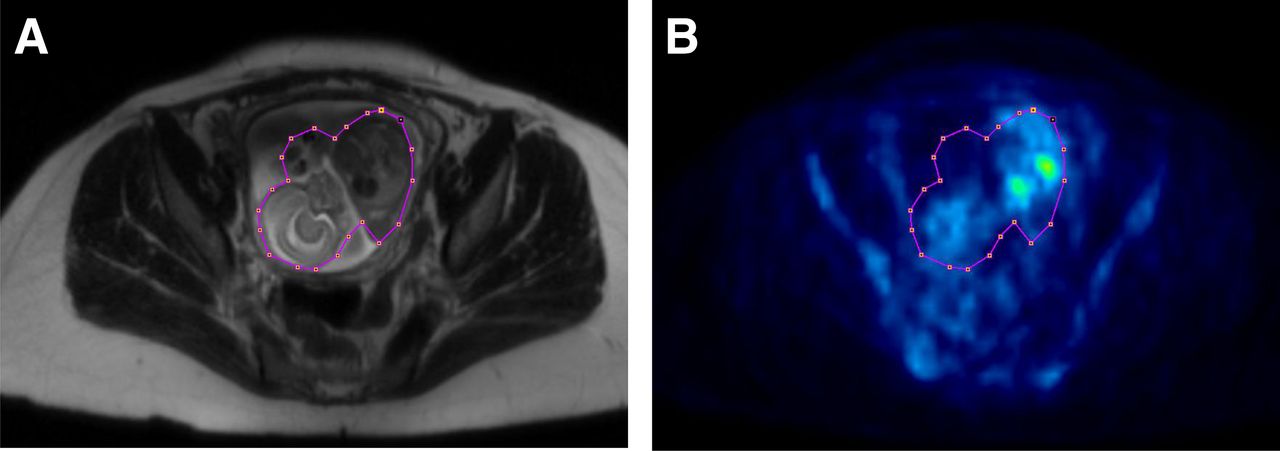
Selected fused (A) and MR imaging–only (B) transaxial slices from 18F-FDG PET/MR imaging study in woman who had been pregnant for 19 wk (patient 4) and was diagnosed with lymphoma that had spread above diaphragm. Fetal details and contours are clearly visible on MR image (B); white arrow indicates heart, and green arrow indicates eye. Structures floating in amniotic fluid just in front of fetus are fetal limbs (blue arrowheads). Fused PET/MR image shows prominent uptake in fetal heart and kidneys (red arrow). Much lower uptake was seen in fetal brain.
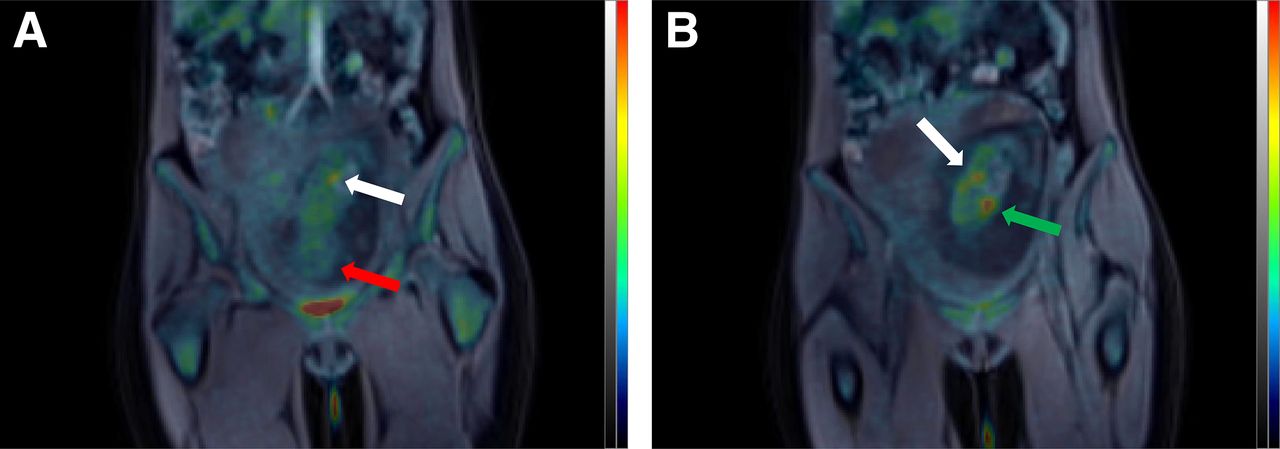
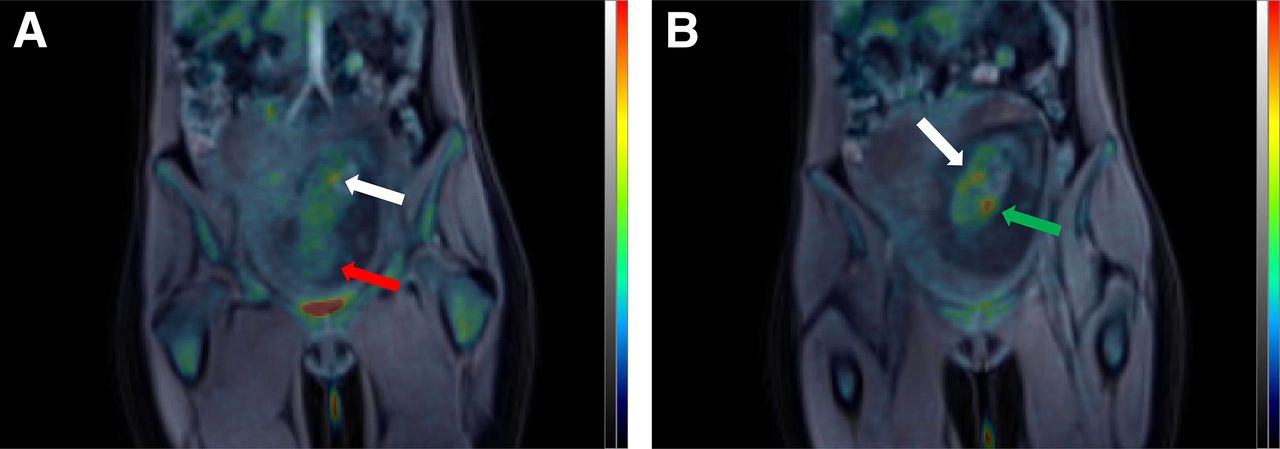
Selected 18F-FDG PET/MR imaging coronal slices in patient who had been pregnant for 19 wk (patient 5) and underwent imaging for Burkitt lymphoma. Areas of increased uptake are clearly visible in fetal bladder (white arrow in A), kidneys (white arrow in B), and myocardium (green arrow in B). No prominent uptake was seen in fetal brain (red arrow in A).

In patients who underwent PET/MR imaging, MR imaging allowed precise delineation of fetal contours (A). Importantly, MR imaging–defined regions of interest encompassed many “cold” areas when superimposed on PET images (B). This finding might have contributed to lower absorbed doses found in 2 patients who underwent PET/MR imaging because cold areas would have reduced average radioactivity value that was used as input for dosimetric calculations.
The absorbed doses were higher in the 3 patients in early pregnancy. When a 1-h voiding was considered, the doses in early pregnancy ranged from 7.25E–03 to 1.73E–02 mGy/MBq (Table 2). These values are consistent with those recently published by Takalkar et al. (13) and are lower than both the standard value of 2.2E–02 mGy/MBq (12) and the estimates we previously published (3,4). In later stages of pregnancy, the absorbed doses were lower than currently adopted standard values (the highest dose was 6.22E–03 mGy/MBq [in patient 6]) (Table 2). In total, for a 1-h voiding time, the fetal absorbed doses from 18F-FDG injection ranged from approximately 1.4 to 5.1 mGy, according to the activity administered, with the highest values generally being found in early pregnancy.
Effect of Bladder Voiding on Fetal Radiation Dose
Bladder voiding had a considerable effect on the radiation dose to the fetus, especially for patients in early pregnancy. The dose reduction for voiding at 1 h compared with voiding at 3.5 h ranged from 25% (for patient 6) to approximately 45% (for patients 2 and 3) (Table 2).
The placenta concentrated 0.27% of the injected activity of 18F-FDG.
DISCUSSION
The present study—to our knowledge, the largest series ever published of pregnant patients imaged with 18F-FDG PET—showed that fetal radiation exposure is generally low, especially in later stages of pregnancy.
The relatively higher absorbed dose found in early pregnancy is likely explained by the smaller volume of the fetus and by the fact that the fetal body at this stage is composed of relatively undifferentiated and rapidly proliferating cells. Cells that proliferate rapidly use more glucose and therefore concentrate 18F-FDG more effectively.
Dose calculations in early pregnancy are particularly challenging. At this stage, fetal contours are not clearly visible on PET images; because the skeleton is not yet formed, the fetus cannot be seen on CT scans. Uncertainties about the estimation of the fetal volume or the average concentration of radioactivity might result in important variations in the final dose estimate. In the existing cases published in the literature, 2 approaches have been used to solve this problem. In the first 2 case reports, the fetal voxel with the highest activity was conservatively considered to be the average concentration in the whole fetus, and the average fetal volume for that stage of pregnancy was used to calculate the dose. This approach yielded doses ranging from 3E–02 to 4E–02 mGy/MBq (3,4). The advantage of this approach is that the dose does not depend on operator variability in drawing the fetal volume. The drawback is that the dose is probably overestimated. Therefore, the dose obtained with this approach should be considered an upper theoretic limit.
Another approach, used for patient 1 in the present study and for patient 1 in the study of Takalkar et al. (13), involved using the dose to the uterus as a proxy. The resulting doses were significantly lower, in the range of 1.5E–02 to 1.7E–02 mGy/MBq, with the most frequent voiding schedule. This approach probably yields a more realistic dose estimate, even if a slight underestimation is possible. Indeed, a higher concentration in the small fetal subvolume would not be properly considered by a region of interest large enough to encompass the whole uterus. Dosimetry results might also vary according to the anthropomorphic phantom used. Using S values derived from the realistic Rensselaer Polytechnic Institute pregnant female phantom and assuming similar uptake values for fetal and maternal tissues, Xie and Zaidi showed that the absorbed dose from 18F-FDG injection in early pregnancy was higher (3.05E–2 mGy/MBq) than reference values (18). However, different methodologic approaches do not fully explain the variability of dose estimates in early pregnancy. A large part of this variability is likely due to actual interindividual differences in glucose metabolism among fetuses. Indeed, the time-integrated activity for the 10-wk fetus in our previous study (4) (0.0035, as measured by Takalkar et al. (13)) was twice as high as that of patient 2 in the present study (0.0016) and considerably higher than that of the 18-wk fetus in the study of Takalkar et al. (0.0023).
In summary, by taking into account the variability due to metabolism and methodologic approaches, published studies, pooled together, suggest that doses in early pregnancy range from 1.5E–02 to 4E–02 mGy/MBq. Thus, the standard value proposed by Stabin (2.2E–02 mGy/MBq) (12) seems to be a reasonable approximation of the average dose.
In later stages of pregnancy, dose estimates are lower, essentially because of the larger mass of the more mature fetus. All published studies of humans (7,8,13,19) and nonhumans primates (11) in late pregnancy have supported the assumption made by Stabin that the average concentrations in maternal and fetal tissues are approximately equal (12). According to the present study and the study of Takalkar et al. (13), doses in late pregnancy approximately range from 0.4E–02 to 1.2E–02 mGy/MBq. These doses are significantly lower than the proposed standard value of 1.7E–02 mGy/MBq (12).
Of importance is the fact that all cases published until now have consisted of simple static images obtained about 1 h after injection. To estimate dosimetry for a fetus, some assumptions have to be made, and such assumptions are usually devised to provide conservatively high values. For instance, the effective half-life of 18F-FDG is assumed to be the physical decay of 18F. Thus, published dose estimates probably still overestimate actual doses. However, given the uncertainties associated with this kind of dosimetric estimation, conservative values are probably justified. For instance, it is unknown whether uptake in fetal tissues peaks at the time of imaging.
In the present study, the fetuses of the 2 patients who underwent PET/MR imaging had the lowest dose per megabecquerel injected. One likely explanation is that the fetal regions of interest delineated by MR imaging included “cold” areas on PET that probably would not have been included had MR imaging not been available (Fig. 4); such circumstances might have reduced the final fraction attributable to the fetus.
If an 18F-FDG PET examination of a pregnant woman with cancer is planned, we suggest that a full dynamic scan be acquired to measure the actual fetal residence time. This procedure would not increase the radiation dose and would directly benefit the patient, as the fetal dose would be calculated with greater accuracy. In addition, the abdominal aorta would be in the field of view during the entire dynamic scan, so that an acceptable surrogate of the arterial input function would be available. Because of the relative large diameter of the aorta, its PET signal should not be polluted by significant partial-volume effects. Moreover, 18F-FDG does not have radiometabolites that might be blocked by the placental barrier. Although full compartmental modeling would not be possible because of the physical limitations of image-derived input functions (20), calculation of the rate of glucose metabolism in different fetal tissues nevertheless would be possible with Patlak graphic analysis (21) and an appropriate kinetic model that takes into account the fetoplacental system. If the examination is scheduled on a PET/MR imaging machine, a T2-weighted sequence could also be acquired to better delineate the fetal and placental structures.
The total fetal radiation dose is the sum of the doses derived from 18F-FDG and from transmission scans acquired for attenuation correction. With PET-only scans, the absorbed dose from radioactive external sources is negligible (22). However, PET-only scanners now have largely been replaced by hybrid PET/CT machines, and these machines may not have the option of operating in PET-only mode. The dose from the CT portion depends on the protocol used during the study but can generally be assumed to add 6–14 mGy to the fetal dose (13). In addition to the advantage of more accurate delineation of fetal tissues, PET/MR imaging does not involve the use of ionizing radiation for attenuation correction. Therefore, PET/MR imaging should be the option of choice for PET imaging of pregnant patients. Notably, the fetus constantly moves inside the amniotic fluid, especially in early pregnancy. Therefore, the delineation of fetal contours with a PET scan coregistered to a previously acquired MR image would not be as accurate as that obtained with hybrid PET/MR imaging.
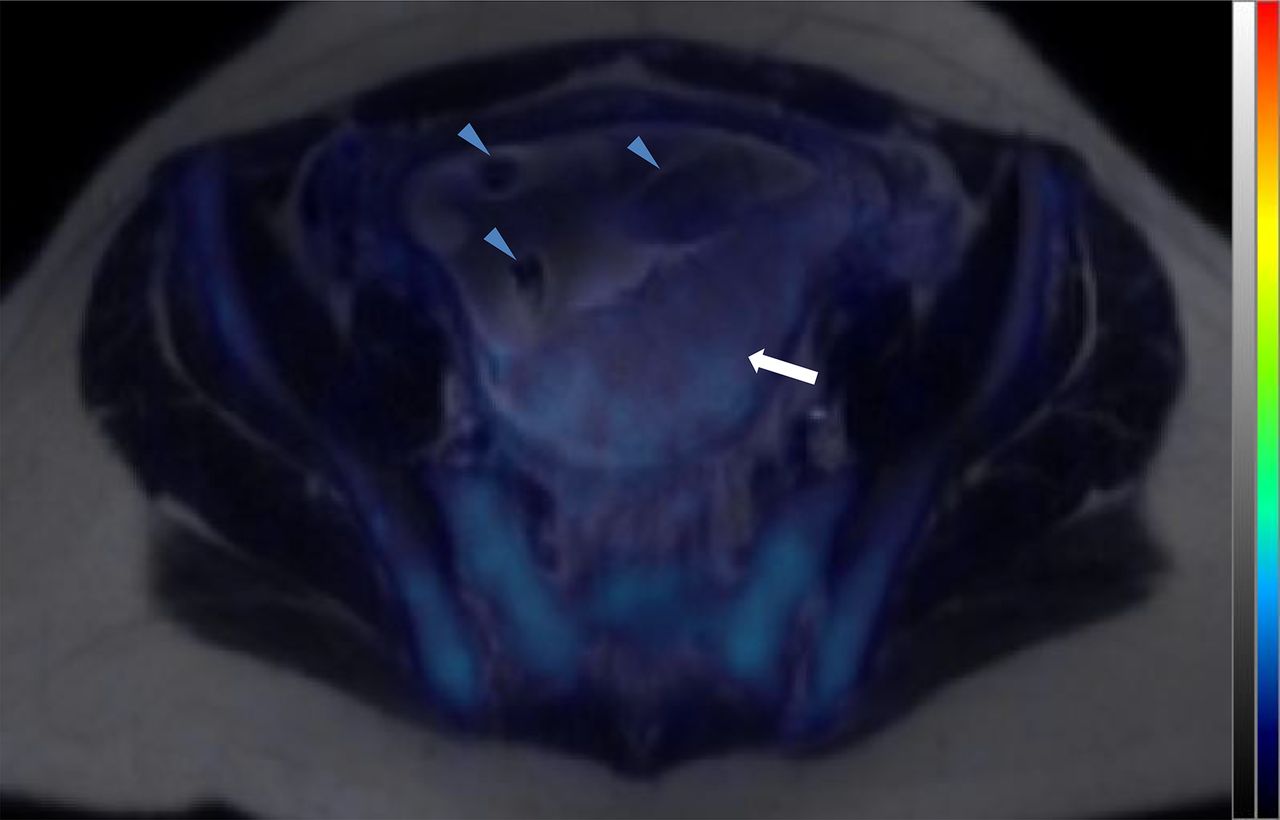
The accumulation of glucose in the placenta is mediated by specific transporters—essentially, GLUT1 and GLUT3 (23)—because glucose is a primary energy source for the fetus. In 2 previous case reports during early pregnancy, the fraction of placental uptake was estimated to be approximately 0.20% (7,10). However, the placental contours were not visible, and an average volume was used as the placental volume. In the present study, PET/MR imaging allowed accurate delineation of the placenta in patient 4 (Fig. 5); placental uptake was estimated to be 0.27% of the injected activity, thus confirming our previous estimates.

18F-FDG PET/MR imaging transaxial slice through placenta (white arrow) of patient 4. Blue arrowheads indicate fetal limbs visible in amniotic fluid.
When a pregnant woman needs to undergo a PET scan, fetal exposure should be reduced as much as possible. In particular, improvements in PET instrumentation may allow the same image quality to be obtained with a smaller amount of injected activity. The highest photon contribution to the fetus comes from the mother’s bladder. Therefore, it is important to facilitate bladder voiding through hydration and, unless contraindicated, the use of a bladder catheter, as in the present study. Frequent bladder voiding is particularly important in reducing the dose in early pregnancy because of the smaller size of the fetus and its closer average proximity to the bladder. Indeed, when a more frequent voiding schedule was used, the doses in the present study were reduced by 25% for patient 6 (in late pregnancy) and by approximately 45% for patients 2 and 3 (in early pregnancy) (Table 2). These rates of dose reduction are similar to those calculated by Takalkar et al. (13).
Notably, in most institutions images are acquired approximately 1 h after injection, and patients are instructed to void just before images are acquired. Therefore, the doses that we found for a voiding time of 1 h are probably more representative of the doses absorbed by the fetuses of patients undergoing clinical PET scans.
Finally, the present study further confirmed that the total radiation exposure of the fetus from PET procedures is significantly lower than the threshold for deterministic effects. Weeks 3 and 4 of gestation are the most sensitive for the induction of embryonic death, which might occur after irradiation with 100 mGy (24). The period between weeks 4 and 15 is the most sensitive for irreversible whole-body growth retardation, microcephaly, and mental retardation, which occur at doses higher than 200 mGy (24). Even with the most conservative assumptions and the use of both PET and CT components, a full PET/CT scan is unlikely to deliver more than 15–20 mGy to the fetus. For PET/MR imaging, the value is more likely 5 mGy or less. Stochastic effects for these doses have never been demonstrated. Even if they do exist, they are small compared with the other risks of pregnancy (25).
CONCLUSION
Fetal radiation doses are higher in early pregnancy, and there can be considerable intersubject variability. However, the total absorbed dose is always well below the threshold for noncancer health effects throughout pregnancy. PET/MR imaging is the optimal procedure for imaging pregnant women because it is not associated with radiation for attenuation correction and allows more accurate dosimetric calculations.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Dr. Michael G. Stabin (Vanderbilt University, Nashville, Tennessee) for useful discussions and suggestions and Anne-Coline Thiburce (CHU Pellegrin, Bordeaux, France) for help in the identification of the fetoplacental structures.
Footnotes
Published online Jun. 18, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication March 3, 2015.
- Accepted for publication May 13, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}