


Abstract
We evaluated the effective dose (ED) of the CT component of whole-body PET/CT using software dedicated to CT dose estimation and from dose–length product (DLP) values to establish practical methods of ED estimation. Methods: Eighty adult patients who underwent 18F-FDG whole-body PET/CT were divided into groups A and B, each consisting of 20 men and 20 women. In group A, ED of the CT component was calculated using CT-Expo for 6 anatomic regions separately, and whole-body ED was obtained by summing the regional EDs (CT-Expo method). DLP was calculated for each of the 6 regions and multiplied by a corresponding conversion factor described in International Commission on Radiological Protection publication 102 to obtain the ED for each region (regional DLP method). Whole-body ED was also calculated as the product of a whole-body DLP value provided by the scanner automatically and a conversion factor (simple DLP method). Moreover, the ED/DLP values were calculated using whole-body ED estimated by the CT-Expo method and the scanner-derived DLP, to optimize the conversion factor. In group B, the optimized conversion factor was applied for the estimation of ED by the simple DLP method. Results: In group A, the regional DLP method allowed an accurate estimation of mean whole-body ED as a result of counterbalance of mild overestimation in men and mild underestimation in women, regarding the CT-Expo method as a standard. The simple DLP method using a conversion factor for the trunk (0.015 mSv/mGy/cm) caused overestimation. On the basis of the ED/DLP values in group A, a modified conversion factor of 0.013 mSv/mGy/cm and sex-specific conversion factors of 0.012 and 0.014 mSv/mGy/cm for men and women, respectively, were determined. In group B, the use of the modified conversion factor improved accuracy, and the use of sex-specific conversion factors eliminated sex-dependent residual errors. Conclusion: ED of the CT component of whole-body PET/CT can be assessed by multiplying the scanner-derived DLP by a conversion factor optimized for whole-body PET/CT.
PET with 18F-FDG has been accepted as a valuable tool in oncology practice. CT images are commonly acquired together with PET images in a single imaging session with an integrated PET/CT scanner (1) and are used for diagnosis on CT images themselves, localization of lesions delineated by PET, and attenuation correction of PET images. The problem of CT acquisition additional to PET is an increase in radiation exposure. The effective dose (ED) derived from the CT component varies widely from 5 to 25 mSv (2–8) and often exceeds the ED from 18F-FDG injection. Although a large amount of radiation exposure is required to acquire high-quality CT images for diagnostic purposes, lesion localization and attenuation correction can be achieved on CT images of lower quality. Dose reduction with preserving clinical utilities should be pursued in each facility considering the purpose of CT and using dose reduction technologies (9,10).
Estimation of ED is a prerequisite for optimization and monitoring of radiation exposure. The volume CT dose index (CTDIvol) and dose–length product (DLP), a product of CTDIvol and scan length, are representative indicators of radiation exposure in CT and are provided on a CT scanner automatically. ED is often estimated as a product of the DLP value and a conversion factor selected according to the imaging region and age (11–13). CTDIvol is calculated on the basis of radiation dose measured in imaging 16- and 32-cm CT dosimetry phantoms for head-mode imaging and body-mode imaging, respectively. When using the same scanner parameters, CTDIvol, and consequently DLP, is larger for a 16-cm phantom than for a 32-cm phantom because of less absorption within a smaller phantom. The conversion factor from DLP to ED depends on the location, size, and radiosensitivity of organs and tissues exposed to radiation and is lower for the head than for the trunk.
In 18F-FDG PET/CT for oncologic applications, CT images are usually acquired from the head to the proximal thigh sequentially, and a single DLP value, representing whole-body radiation exposure, is provided on a scanner. ED of the CT component of whole-body PET/CT may be calculated as a product of the scanner-derived whole-body DLP value and a conversion factor for the trunk (6,8). This method is convenient but neglects regional differences in calculating CTDIvol and in determining the conversion factor from DLP to ED. In this study, we estimated ED of the CT component of whole-body 18F-FDG PET/CT using CT-Expo software (version 2.2; Medizinische Hochschule) (14,15) and from DLP values calculated on region-by-region and whole-body bases. The principal aim of this study was to establish practical methods of approximately estimating ED of the CT component of oncologic 18F-FDG PET/CT.
MATERIALS AND METHODS
Subjects
Eighty adult oncology patients who underwent 18F-FDG PET/CT with their arms raised in October 2013 were studied and divided into groups A and B. Group A consisted of initial 20 consecutive men and 20 consecutive women, and group B consisted of subsequent 20 men and 20 women. The patient characteristics are summarized in Table 1. The institutional review board approved the current retrospective study, and need for informed consent was waived.
Patient Characteristics
Imaging Procedures
A TruePoint Biograph 6 PET/CT scanner (Siemens Medical Solutions), a combination of a PET scanner and a 6-detector-row CT scanner, was used in this study. After fasting for 5 h or longer, patients received an intravenous injection of approximately 185 MBq of 18F-FDG and, 1 h later, underwent whole-body PET/CT imaging, covering the top of the head and the proximal portion of the thigh. CT imaging was performed without the injection of contrast medium during a single breath hold at normal expiration. The scan parameters were as follows: helical mode; slice thickness, 5 mm; slice interval, 2.5 mm; tube voltage, 130 kV; beam pitch, 1.5; beam width, 18 mm; rotation time, 0.6 s; acquisition time, 20–25 s. The autoexposure control was used, and the quality reference mAs, an index to define the image quality, was set at 50 mAs.
Estimation of ED
The scan range was divided into 6 anatomic regions—that is, head, neck, chest, abdomen, pelvis, and proximal thigh (Fig. 1)—and ED was estimated for each anatomic region using the CT-Expo software dedicated to CT dose estimation (CT-Expo method). This method was regarded as a gold standard in the present study. The tube current (mA) value for each slice was extracted from the DICOM header, and mean tube current was calculated for each anatomic region. Imaging parameters including the mean tube current were entered into CT-Expo to estimate ED for each anatomic region, termed regional ED. The head-mode calculation was applied for the head and neck, and body-mode calculation was applied for the chest, abdomen, pelvis, and thigh. Tissue-weighting factors presented in International Commission on Radiological Protection (ICRP) publication 103 were used (16). The whole-body ED was defined as a total of all 6 regional EDs. In helical CT, radiation exposure due to overranging occurs just above and below the scan range (17,18). Because the division of the scan range was imaginary, we excluded exposure due to overranging in the estimation of ED.

Division of scan range into 6 anatomic regions (head, neck, chest, abdomen, pelvis, and proximal thigh) is shown on display of CT-Expo software for male subject.
ED was also estimated from DLP values calculated for the 6 anatomic regions separately (regional DLP method). Mean effective tube current–time product (effective mAs) for each anatomic region was calculated by the equation:
where mA is mean tube current for the respective region. CTDIvol for each anatomic region was obtained as:
The manufacturer provided the constants determined by imaging dosimetry phantoms with the same tube voltage and the same beam width as used in this study. The constant obtained using a 16-cm phantom was used for the head and neck, and that obtained using a 32-cm phantom was used for the chest, abdomen, pelvis, and proximal thigh. CTDIvol was converted to DLP as follows:
Regional ED was determined using the DLP for each region by the equation:
The conversion factor was defined as 0.0021, 0.0059, 0.014, 0.015, and 0.015 mSv/mGy/cm for the head, neck, chest, abdomen, and pelvis, respectively, according to ICRP publication 102 (11). ICRP publication 102 does not indicate a conversion factor for the thigh, and 0.015 mSv/mGy/cm, a value for the trunk, was applied. Whole-body ED was defined as the total of all 6 regional EDs.
In addition, the DLP value provided on the CT scanner automatically, which represented radiation exposure for the entire scan length, was multiplied by a fixed conversion factor to calculate whole-body ED (simple DLP method). The conversion factor used was 0.015 mSv/mGy/cm, a value for the trunk defined in ICRP publication 102 (11).
Theoretically, differences between the regional DLP method and simple DLP method exist in estimating ED for the head, neck, and chest. The contribution of these regions to whole-body ED obtained by the simple DLP method was evaluated. The estimation was similar to the regional DLP method, except for the following modifications. For the head and neck, the mean effective tube current–time product was multiplied by a constant based on a 32-cm phantom to obtain CTDIvol and then multiplied by a conversion factor of 0.015 mSv/mGy/cm to calculate ED. For the chest, 0.015 mSv/mGy/cm was used instead of 0.014 mSv/mGy/cm to convert DLP to ED.
Data Analysis
In group A, EDs for individual anatomic regions and whole body were calculated by the CT-Expo method, regional DLP method, and simple DLP method and compared. Whole-body ED estimated by the CT-Expo method was divided by whole-body DLP provided by the CT scanner, and an ED/DLP value was calculated. Mean ED/DLP calculated in all 40 patients was defined as a modified conversion factor. In addition, mean ED/DLP was calculated in 20 men and 20 women separately to determine sex-specific conversion factors.
In group B, whole-body ED was estimated by the CT-Expo method and simple DLP method using the original conversion factor, 0.015 mSv/mGy/cm. Furthermore, the scanner-derived DLP value was multiplied by the modified conversion factor or sex-specific conversion factor determined in group A, instead of the original conversion factor, to estimate whole-body ED.
Finally, data from groups A and B were pooled together, and mean ED/DLP was calculated for men, women, and all patients. ED/DLP was compared with body height and body weight.
Statistical Analysis
Values were presented as mean ± SD. Correlation was assessed by the Spearman test. A linear regression equation was determined by the least-squares method. A P value of less than 0.05 was deemed statistically significant.
RESULTS
ED and ED/DLP in Group A
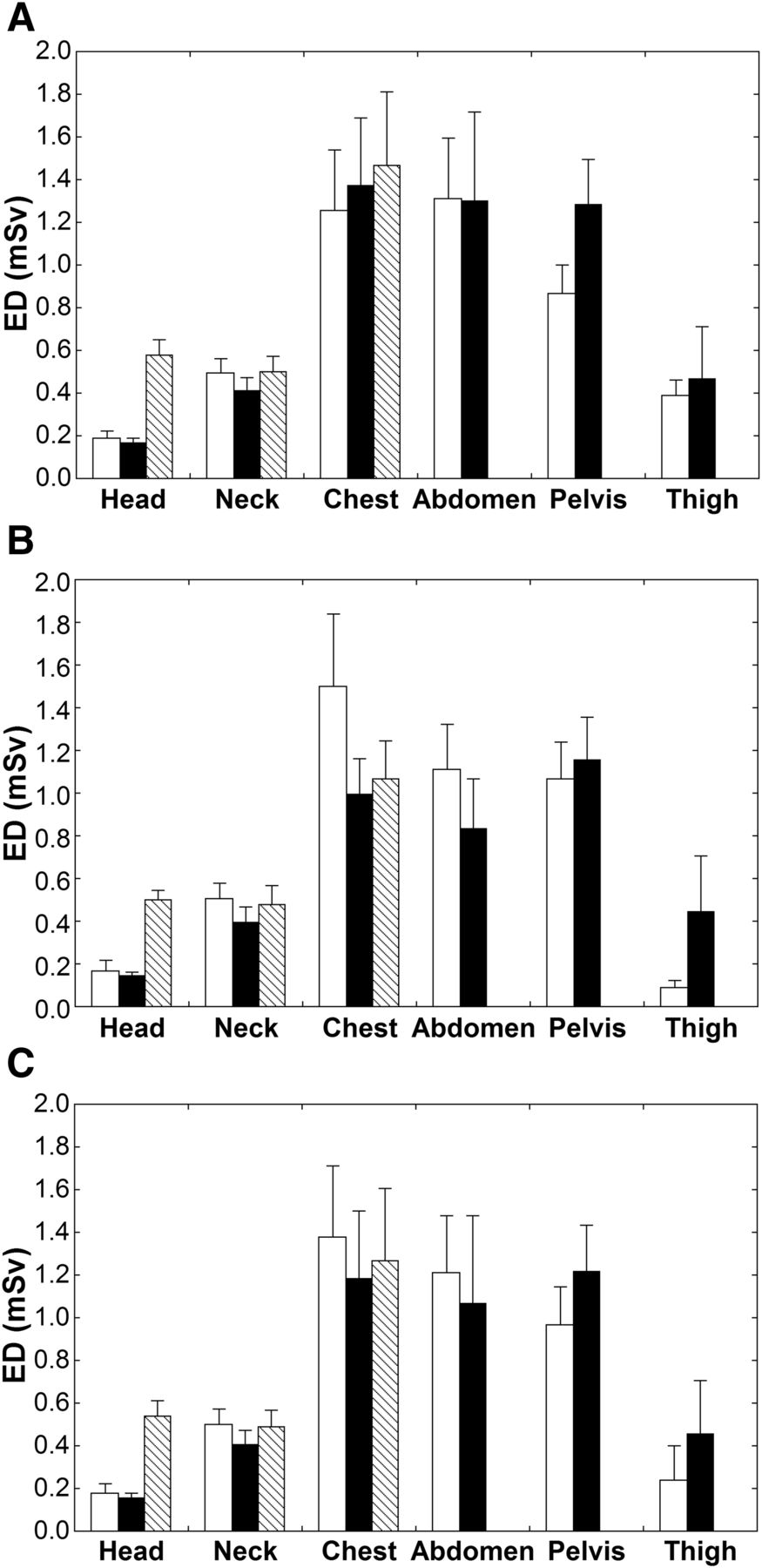
Regional ED values estimated in group A are presented in Figure 2. Regarding the CT-Expo method as a standard, ED for the head was substantially overestimated by the simple DLP method irrespective of sex, and this overestimation was not observed using the regional DLP method. Differences in ED between the estimation methods were relatively small for the neck. For the chest, severe underestimation was observed by the regional DLP method and simple DLP method in women whereas overestimation was shown in men. The regional DLP method caused underestimation for the abdomen in women and overestimation for the pelvis in men. For the proximal thigh, ED was nearly zero by the CT-Expo method in women and was overestimated greatly by the regional DLP method. SDs for the proximal thigh were much larger by the regional DLP method than by the CT-Expo method.

Regional ED values in group A estimated by CT-Expo method (white bars), regional DLP method (black bars), and simple DLP method (shaded bars). Means and SDs in men (A), women (B), and all patients (C) are presented.
Whole-body ED values in group A were summarized in Table 2. The mean ED in all patients was almost identical between the CT-Expo method and regional DLP method. The regional DLP method showed high correlation with the CT-Expo method (Fig. 3), with Spearman correlation coefficients of 0.945 and 0.915 in men and women, respectively; however, mild overestimation in men and mild underestimation in women were observed.
Whole-Body ED Values in Group A

Relationships of EDs estimated by different methods in group A. Estimates of regional DLP method (A) and simple DLP method (B) are plotted against those of CT-Expo method. Line of identity is also shown. ○ = data for men; △ = data for women.
The simple DLP method overestimated whole-body ED in men and provided a 29% larger mean value than the CT-Expo method (Table 2). The difference was small (7%) in women, and overestimation by the simple DLP method was 18% in all patients. EDs estimated by the 2 methods correlated closely, with Spearman correlation coefficients of 0.942 and 0.921 in men and women, respectively (Fig. 3).
The mean ED/DLP in group A was 0.0117, 0.0142, and 0.0129 mSv/mGy/cm in men, women, and all patients, respectively (Table 3). According to these results, the modified conversion factor was defined as 0.013 mSv/mGy/cm. The sex-specific conversion factor was defined as 0.012 and 0.014 mSv/mGy/cm for men and women, respectively.
ED/DLP (mSv/mGy/cm)
Whole-Body ED in Group B
In group B, the simple DLP method with the original conversion factor (0.015 mSv/mGy/cm) overestimated whole-body ED especially in men (Table 4), similarly to group A. When the modified conversion factor was used, mean ED in all patients estimated by the simple DLP method was almost identical to that estimated by the CT-Expo method, as a result of the counterbalance between mild overestimation in men and mild underestimation in women. The use of the sex-specific conversion factors eliminated the errors in both men and women.
Whole-Body ED Values in Group B
ED/DLP in Pooled Subjects
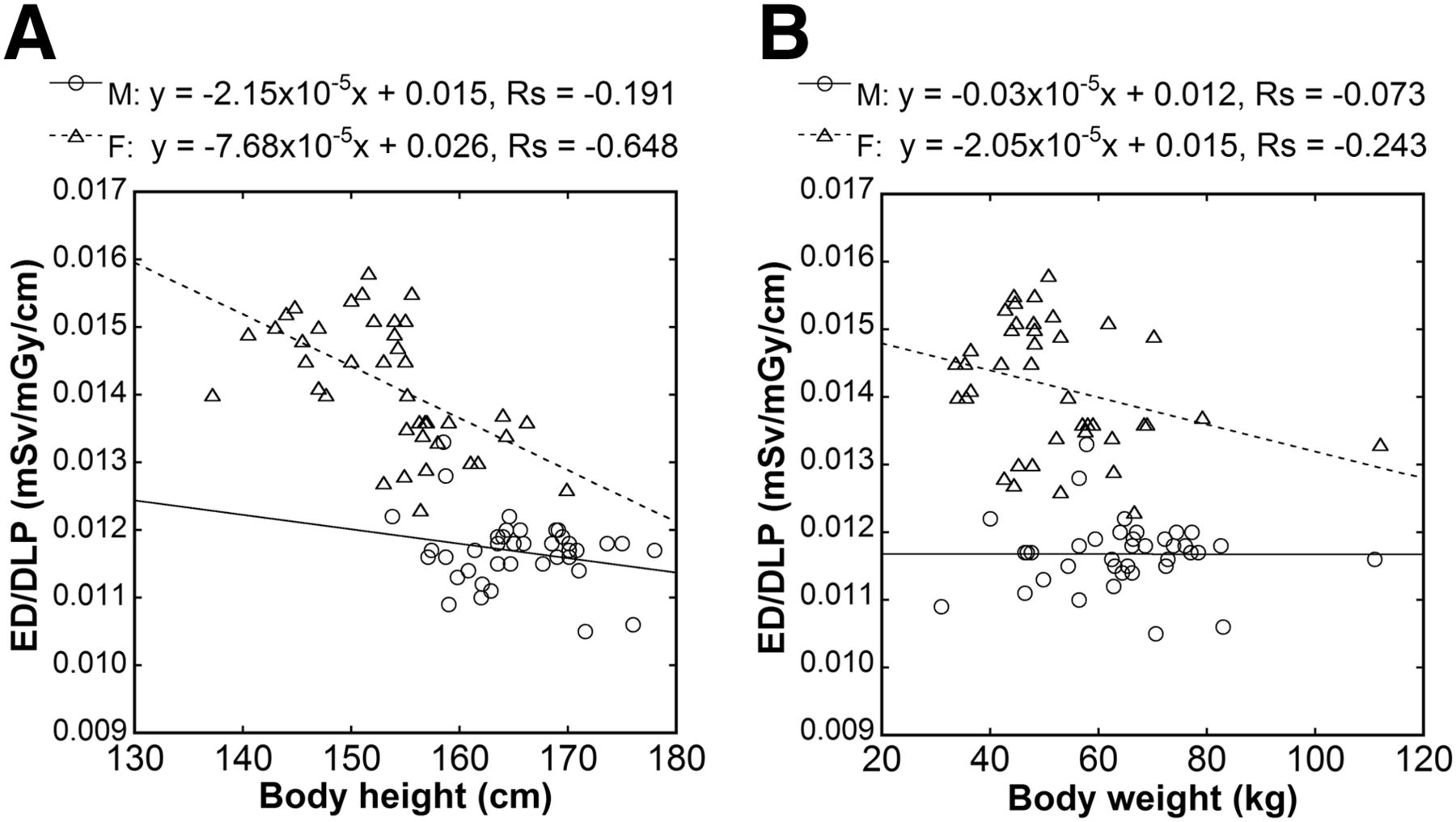
When data from groups A and B were pooled together, mean ED/DLP values were almost identical to those determined in group A alone (Table 3). ED/DLP showed a statistically significant negative correlation with body height in women (Spearman correlation coefficient = −0.648, P < 0.001) (Fig. 4). A significant correlation was not demonstrated between ED/DLP and body height in men. ED/DLP correlated with body weight in neither men nor women. Linear regression analysis between body height and ED/DLP indicated regression equations of y = −2.15 × 10−5x + 0.015 and y = −7.68 × 10−5x + 0.026 for men and women, respectively, where x and y represent body height in cm and ED/DLP in mSv/mGy/cm, respectively. From these equations, ED/DLP is estimated at 0.116 mSv/mGy/cm for a man of 170-cm height and at 0.137 mSv/mGy/cm for a woman of 160-cm height.

Relationships of ED/DLP with body height (A) and body weight (B). Linear regression lines, regression equations, and Spearman correlation coefficients are shown. ○ = data for men; △ = data for women.
DISCUSSION
In this study, we estimated ED of the CT component of whole-body 18F-FDG PET/CT using CT-Expo. We used tissue-weighting factors described in ICRP publication 103 (16), instead of those in ICRP publication 60, and this selection should have influenced the results significantly (19,20). Tube current is a major determinant of radiation dose in CT and is modulated during a single data acquisition by autoexposure control. We divided the entire scan range into 6 anatomic regions, and mean tube current for each region was used for the estimation of ED for each region. When dividing the scan range, the effect of overranging should be considered. In helical CT, additional radiation exposure occurs just above and below the prescribed scan range (17,18). If radiation exposure due to overranging is included in analysis, radiation dose is added at the start and end of each of the 6 anatomic regions. However, radiation exposure due to overranging occurs only just above the top of the head and just below the proximal thigh, which would not cause substantial addition of the stochastic effect of ionizing radiation. Thus, we excluded radiation dose due to overranging.
ED derived from the CT component of whole-body PET/CT varies widely, from 5 to 25 mSv, among PET facilities (2–8). Mean whole-body ED in all 80 patients was 4.61 mSv, indicating relatively low dose, in this study. In our facility, most patients undergo diagnostic CT examinations before 18F-FDG PET/CT, and the roles of the CT component of PET/CT are attenuation correction and lesion localization but not diagnosis on CT images themselves. Therefore, we set imaging parameters to deliver relatively low radiation exposure, which should be the main cause of the low ED. Although a mean body height of 159.5 cm and mean body weight of 58.8 kg in this study are standard in our country, they would be smaller than in most other countries. Autoexposure control increases tube current and consequently radiation dose, with body size. The relatively low ED appears to be partly attributable to the small body size of our patient population. Reconstruction methods using iterative algorithms allow CT images of acceptable quality at reduced radiation dose to be obtained (21,22) but were not available in our facility during the study period. Further reduction in radiation dose should be pursued with the aid of new CT technologies.
ED in CT may be estimated by multiplying DLP calculated on the CT scanner automatically by a conversion factor (11–13). Although this method is convenient, its application to PET/CT covering a wide variety of anatomic regions causes problems in calculating CTDIvol and determining the conversion factor. In the present study, we calculated DLP for each anatomic region and multiplied it by the corresponding conversion factor to obtain ED for each region (regional DLP method). Mean whole-body ED was almost identical between the CT-Expo method and regional DLP method, indicating that the regional DLP method can provide ED of the CT component of whole-body PET/CT without dedicated software. Whole-body ED was overestimated by the simple DLP method using the scanner-derived DLP and the conversion factor for the trunk provided in ICRP publication 102, which was mainly attributable to overestimation of ED for the head. Radiation exposure due to overranging increases the scanner-derived DLP, despite lack of significant stochastic effects, and is considered to be another source of overestimation.
When men and women were analyzed separately, the regional DLP method caused mild overestimation and mild underestimation of whole-body ED in men and women, respectively. Sex-dependence should be considered in CT dose estimation (19), and CT-Expo computes ED considering differences in the location and radiosensitivity of organs between men and women, in contrast to the conversion of DLP to ED. In region-by-region comparisons, underestimation for the female chest was prominent due to high radiosensitivity of the breast. Radiosensitivity for the proximal thigh region is low in women whereas men have the testis as a radiosensitive organ there. Although CT-Expo provided low estimates in the female proximal thigh, the regional DLP method overestimated ED due to neglecting the low radiosensitivity. Intersubject variation in ED estimates for the proximal thigh was greater with the regional DLP method than with the CT-Expo method, which appears to be attributable to variation in the scan range. Extension of the scan range to the distal thigh increases DLP, however, such extension would not affect actual stochastic effects of radiation significantly. It would be better to neglect radiation to the distal thigh and leg when ED is calculated by a DLP-based method.
To improve the estimation of ED by the simple DLP method, we attempted to optimize the conversion factor from DLP to ED. Using ED estimated by the CT-Expo method and scanner-derived DLP in all patients of group A, we determined the modified conversion factor as 0.013 mSv/mGy/cm, which was smaller than the original conversion factor for the trunk (0.015 mSv/mGy/cm). For validation, the modified conversion factor was applied to group B. Although successful estimation was demonstrated in all patients, overestimation in men and underestimation in women were noted. Need for sex-specific conversion factors was emphasized previously (19). We determined sex-specific conversion factors as 0.012 and 0.014 mSv/mGy/cm for men and women, respectively, from group A data, and their application to group B resulted in successful estimation in both men and women. These results indicate that ED of the CT component can be estimated from the scanner-derived DLP using the modified conversion factor and that the estimation is improved by the use of the sex-specific conversion factors. The morphology and radiosensitivity of organs and tissues differ among patients, which is not considered in ED estimation. The role of ED estimation is not to evaluate a risk of cancer induction in an individual patient but to compare radiation dose among radiation sources, among CT imaging protocols, and among facilities. Considering this role, the use of the modified conversion factor may be acceptable. When the proportions of male and female patients deviate from identity, the use of the sex-specific conversion factors may be preferable.
The analysis of the relationship between ED/DLP and body size demonstrated significant negative correlation of ED/DLP with body height in women despite a lack of significant correlation with body weight. In a larger patient, the body thickness is greater and the scan length longer. A thicker body increases tube current due to autoexposure control, resulting in concordant elevation of DLP and ED. A longer scan length increases DLP, a product of CTDIvol and scan length, even when tube current is unchanged. CT-Expo provides ED assuming a man of 170-cm height and 70-kg weight and a woman of 160-cm height and 60-kg weight, and intersubject variation in actual scan length is irrelevant. The difference in the effect of scan length between DLP calculation and ED estimation with CT-Expo appears to explain the dependence of ED/DLP on body height. The patients analyzed in this study were rather small (Table 1). However, when ED/DLP values for a 170-cm man and a 160-cm woman were predicted from regression lines between ED/DLP and body height, they did not differ substantially from mean values in the patients. The small body size of our patient population should not affect the application of the determined conversion factors to different patient populations.
The present study indicated the abilities of the regional DLP method and the simple DLP method combined with the optimized conversion factor to estimate ED of the CT component of whole-body PET/CT. However, this study was performed at a single facility using a single PET/CT scanner, and further validation at different facilities using different scanners is required. In our imaging protocol, the scan range covered from the top of the head to the proximal portion of the thigh. The optimized conversion factor determined in this study may not be applicable when the scan range differs.
CONCLUSION
We evaluated ED derived from the CT component of whole-body 18F-FDG PET/CT for oncologic application using CT-Expo and DLP-based methods. When DLP provided on the CT scanner automatically was multiplied by the conversion factor for the trunk described in ICRP publication 102, whole-body ED was overestimated especially in men. When the scan range was divided into 6 anatomic regions followed by calculation of DLP and conversion to ED for each region, concordance in whole-body ED with CT-Expo improved, except sex-dependent differences. The conversion factor was optimized for whole-body PET/CT. Multiplication of the scanner-derived DLP by the modified conversion factor was indicated to be a practical way of estimating ED with acceptable accuracy, and use of sex-specific conversion factors eliminated sex-dependent residual errors.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Mr. Yoichi Komoto, Siemens Japan, for his cooperation in this study.
Footnotes
Published online Apr. 3, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 30, 2014.
- Accepted for publication February 25, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Feasibility of an Ultra-Low-Dose PET Scan Protocol with CT-Based and LSO-TX-Based Attenuation Correction Using a Long-Axial-Field-of-View PET/CT Scanner
- Establishment of National DRL for CT in Hybrid Imaging Studies (The Second Phase of the National NM CT (PET) Dose Audit for Kuwait Population -2019)