


Abstract
The aim of this evaluation was to identify the first indicators of efficacy for 225Ac-labeled prostate-specific membrane antigen (PSMA)–617 therapy in a retrospectively analyzed group of patients. Methods: Forty patients with metastatic castration-resistant prostate cancer were selected for treatment with three 100 kBq/kg cycles of 225Ac-PSMA-617 at 2-mo intervals. Prostate-specific antigen (PSA) and blood cell count were measured every 4 wk. PSMA PET/CT or PSMA SPECT/CT were used for baseline staging and imaging follow-up at month 6. Follow-up included the duration of PSA response and radiologic progression-free survival at month 6. Patient histories were reviewed for the duration of previous treatment lines, and a swimmer plot was used to intraindividually compare the duration of tumor control by PSMA therapy versus prior treatment modalities. Results: Thirty-one of 40 patients were treated per protocol. Five patients discontinued treatment because of nonresponse, and 4 because of xerostomia. Of the 38 patients surviving at least 8 wk, 24 (63%) had a PSA decline of more than 50%, and 33 (87%) had a PSA response of any degree. The median duration of tumor control under 225Ac-PSMA-617 last-line therapy was 9.0 mo; 5 patients had an enduring response of more than 2 y. Because all patients had advanced disease, this result compares favorably with the tumor control rates associated with earlier-phase disease; the most common preceding first-, second-, third-, and fourth-line therapies were abiraterone (median duration 10.0 mo), docetaxel (6.5 mo), enzalutamide (6.5 mo), and cabazitaxel (6.0 mo), respectively. Conclusion: A positive response for surrogate parameters demonstrates remarkable antitumor activity for 225Ac-PSMA-617. Swimmer-plot analysis indicates a promising duration of tumor control, especially considering the unfavorable prognostic profile of the selected advanced-stage patients. Xerostomia was the main reason patients discontinued therapy or refused additional administrations and was in the same dimension as nonresponse; this finding indicates that further modifications of the treatment regimen with regard to side effects might be necessary to further enhance the therapeutic range.
Prostate-specific membrane antigen (PSMA)–617 is a small molecule targeting PSMA. Because of its conjugation to DOTA, it can be labeled with several radiometals for imaging or radioligand therapy (RLT) of prostate cancer (1).
Several centers worldwide now offer PSMA RLT with the β-emitter 177Lu as a salvage therapy or in early-phase clinical trials for patients with metastatic castration-resistant prostate cancer. These centers confirmatively reported promising antitumor activity with regard to prostate-specific antigen (PSA) serum levels or radiologic response (2–9); however, a considerable number of patients were found to be short responders or nonresponders. Dose escalation was limited by chronic hematologic toxicity (10).
Because of theoretic advantages in the physics and radiation biology of α- versus β-particle emitters and promising preclinical studies, although most of them were done with 213Bi-labeled PSMA ligands (11–15), we introduced PSMA-targeting α-therapy (TAT) for salvage therapy of end-stage metastatic castration-resistant prostate cancer in our hospital. Based on dosimetry estimates (16,17) and preliminary clinical experience with individual patients (17–19), 225Ac was considered the first-choice radionuclide for clinical application, and we defined a 225Ac treatment activity level that became the basis of our first standard operating procedure (19).
Here, we report our clinical findings for the first 40 patients who were treated with the intention of administering this dosing regimen. Because PSMA TAT was always offered as a last-line option, that is, after other options had been exhausted, the duration of tumor control achieved with the approved standard drugs could serve as an intraindividual reference regarding the respective tumor aggressiveness. The swimmer plot, with bars showing the duration of response to the various therapies, is a graphical way of showing the chronology of each patient’s treatment history at a glance.
MATERIALS AND METHODS
Patients
225Ac-PSMA RLT was performed under the conditions of the updated declaration of Helsinki, paragraph 37 (Unproven Interventions in Clinical Practice), and in accordance with the German Pharmaceuticals Law, paragraph 13(2b), as a salvage therapy for patients with metastatic castration-resistant prostate cancer, which had to be progressive and resistant against or ineligible for approved options. This report describes 40 consecutive patients. All had a PSMA-positive tumor phenotype on 68Ga-PSMA-11 PET/CT or on 99mTc-MIP-1427 scanning (planar whole-body, torso SPECT/CT). Because of the short tissue-penetration range of 225Ac-PSMA-617, it has a theoretic advantage regarding hematologic toxicity in patients with diffuse-type bone marrow infiltration; However, some cases of severe xerostomia have been reported after 225Ac-PSMA-617 (17,19). Neither xerostomia nor hematologic toxicity was a relevant issue in the literature about 177Lu-PSMA-617; these side effects were seen only in patients with less advanced disease (4–7). We tailored consecutive patients to receive either 177Lu-PSMA or 225Ac-PSMA according to Figure 1. Patients were informed about the experimental nature of this therapy and gave written informed consent. Our ethical committee approved the retrospective evaluation as an observational study.

Patient selection criteria. (A) Flowchart showing how patients were selected to receive PSMA RLT as unproven intervention in clinical practice. (B) Patients with oligometastatic, hot-spot pattern of tumor spread were preferably stratified to receive 177Lu-PSMA-617. (C) Patients with diffuse pattern of bone marrow infiltration were stratified for 225Ac-PSMA-617. mCRPC = metastatic castration-resistant prostate cancer.
Radiopharmaceuticals and Treatment Regimen
The PSMA-617 precursors were obtained from ABX and labeled with 225Ac as described previously (17). Today, preparation of imaging tracers for PSMA PET/CT or SPECT/CT can be considered clinical routine. The treatment regimen for 225Ac-PSMA-617 was 100 kBq/kg of body weight administered every 2 mo via a 30-s free-hand injection through a low–protein-binding sterile filter (Filtropur S 0.2; Sarstedt). The patients were isolated as inpatients for 48 h, covering urinary clearance of non–tumor-bound radioactivity.
The standard operating procedure for PSMA TAT, including prescribed versus allowed versus obligatory discontinued comedication, is summarized in the Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org).
Follow-up and Response Assessment
PSA, blood cell count, and liver and kidney laboratory values were routinely checked every 4 wk during the first 24 wk and every 8 wk in the long-term follow-up. Other side effects were assessed by anamnesis. Imaging was routinely done at baseline and 6 mo after the first cycle, or earlier if clinically indicated. Other imaging and long-term imaging follow-up was done only if indicated by the responsible urologist or oncologist. Surrogate response markers were interpreted in accordance with the recommendation of the Prostate Cancer Clinical Trials Working Group (PCWG), including best PSA response, PSA response at defined time points, time to PSA progression (TTP), radiologic response at month 6, and clinical duration of tumor control (20–22).
Definition of “Duration of Tumor Control”
Evaluated medical records contained robust information about the chronology of prior treatments. However, the reason for discontinuation of prior treatments could not always be discerned. To address this problem, we defined “Duration of Tumor Control” as the interval from the first administration of a particular drug to the initiation of the next treatment line.
Because PSMA TAT was offered as last-line therapy, the endpoint “switch to next treatment line” was not applicable here. TTP was not considered an equivalent surrogate for evaluation of PSMA RLT response. The methodologic challenge is illustrated in Figure 2: a patient starting with a serum PSA level of 3,000 ng/mL had a PSA nadir of less than 0.1 ng/mL but had already relapsed 4 mo later. However, he was followed during a treatment-free interval of 2 y with a slowly rising PSA until his PSA finally exceeded 100 ng/mL and he was considered for a second course of PSMA TAT, which is currently ongoing. In this case, the TTP would dramatically underestimate the obvious benefit of PSMA TAT. Thus, for patients with an initial response to PSMA TAT, we defined “Duration of Tumor Control” as either “PSA relapse to baseline” or the occurrence of new clinical tumor-related symptoms (considering the criterion that was met first).

TTP vs. duration of clinical benefit. After favorable initial PSA and imaging response to complete remission, patient 14 had TTP of only 1 y (January to December 2015). However, duration of clinical benefit was more than 1 y longer: because of asymptomatic disease and slow growth velocity, treatment-free interval could be prolonged until April 2017. Whether patient will again respond to second series of 225Ac-PSMA-617 is not yet known. (Images courtesy of Prof. Felix Mottaghy, Rheinisch-Westfälische Technische Hochschule Aachen.)
Swimmer-Plot Analysis
Swimmer-plot analysis, as an early option to obtain a longitudinal response parameter, is encouraged by the PCWG3 recommendations (22). In addition to the absolute durations of PSA response and clinical benefits, we also analyzed the relative contribution of 225Ac-PSMA-617 to the entire disease course from reaching the castration-resistant stage to the final switch to palliative care. The rationale is evident from the patient example in Figure 2. The persistent response at more than 27 mo implies a dramatic therapeutic benefit for this patient. However, in comparison to 38-mo tumor control with docetaxel, the relative benefit of this treatment line appears less impressive and might be attributed to an indolent tumor behavior. In contrast, patient 2 presented with a response of only 3 mo to abiraterone, 4 mo to docetaxel, 6 mo to cabazitaxel, and 3 mo to enzalutamide. Considering the documented tumor aggressiveness, the 14-mo response to 225Ac-PSMA-617 (an average outcome for other patients) is remarkable. Thus, to eliminate a random bias by selecting patients with different tumor differentiations, swimmer lanes were normalized to the duration of previous treatment lines.
RESULTS
Clinical Findings
Of 50 patients scheduled to undergo PSMA RLT in our department, 45 were considered PSMA-positive; 10% were rejected after baseline imaging. However, a clear cutoff on what should be considered adequate uptake on PSMA imaging has not been elaborated yet. Thus, the current patient selection and tailoring process is still an individual approach based on visual imaging interpretation and clinical considerations.
The characteristics of the included patients are summarized in the first column of Table 1. The median duration of previous androgen deprivation therapy was 24 mo; the median time from initial diagnosis to the first cycle of PSMA TAT was 49 mo.
Patient Characteristics in Comparison to Experience with 177Lu-PSMA and 223Ra
The delay from the first outpatient consultation to the first administered treatment averaged 4 wk (range, 0–8 wk). During this time, 5 patients died. In contrast, only 2 of 40 patients died within 8 wk after the first RLT cycle. This finding suggests a potential additional indicator of treatment efficacy.
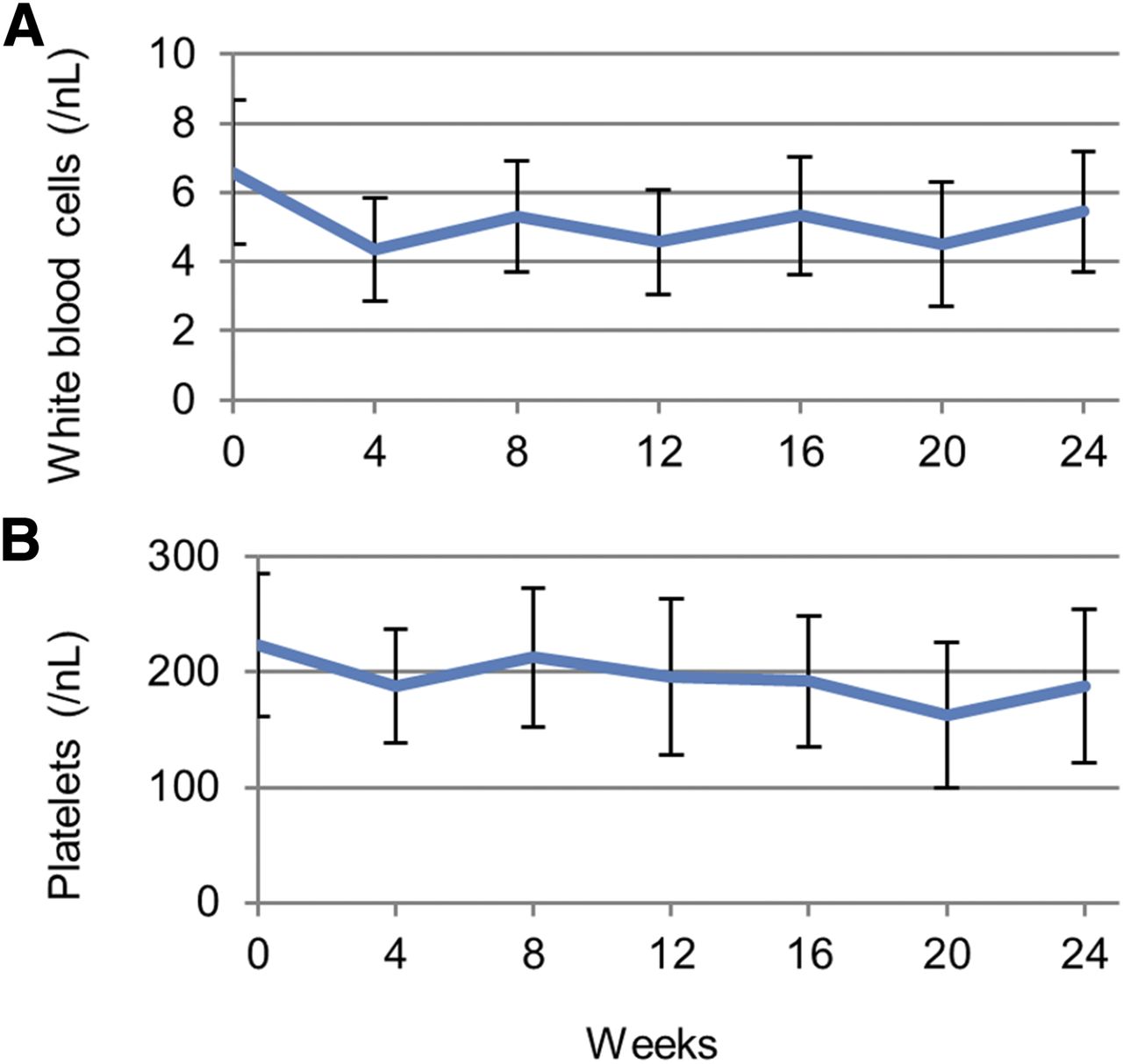
Treatment per protocol was applied to 31 of 40 patients. Eleven of them had further treatment cycles indicated as consolidation therapy or as a second treatment series after relapse. Nine patients discontinued treatment earlier: 5 because of nonresponse or early PSA relapse; 4 because of intolerable xerostomia or loss of taste, despite a promising initial PSA response. Consolidation therapy was offered but, because of the lack of life-threatening situations, was not strongly recommended to 15 of the other per-protocol patients, who had partial remissions and PSMA-positive residual lesions on PSMA imaging at week 24. However, these patients were reluctant to add elective treatment cycles because they reported severe xerostomia and wanted to preserve some remaining salivary gland function. No other clinical side effects led to discontinuation of therapy. The amplitude of hematologic changes was small (Fig. 3).
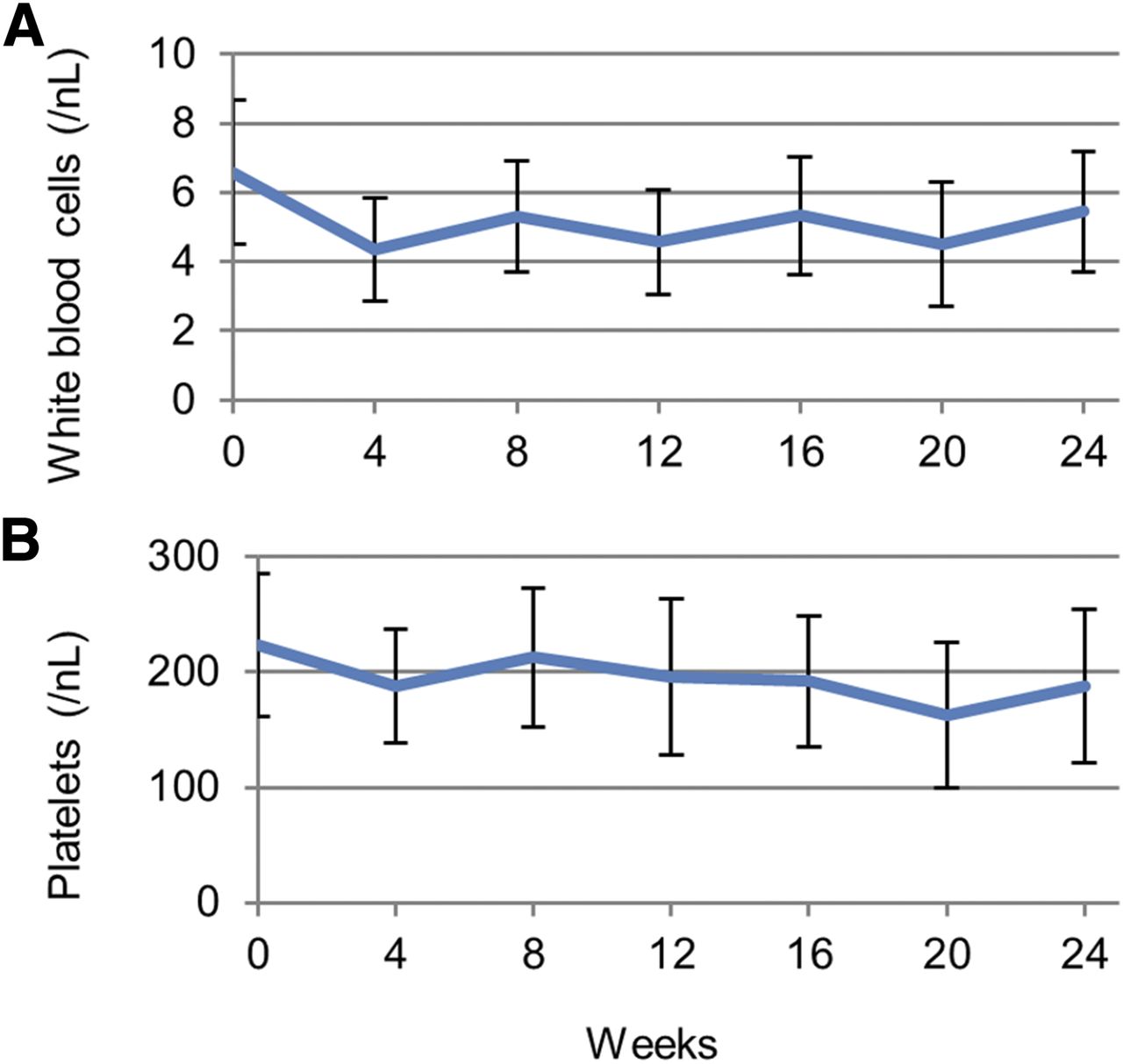
White blood cell count (A) and platelet count (B) during 24 wk.
Exactly 50% of patients showed up for the follow-up examination 1 y after the first treatment; that is, the median overall survival (OS) was more than 12 mo even if the worst case was assumed for all patients lost to follow-up.
Surrogate Markers of Response
Restaging 6 mo after the first treatment revealed a median radiologic progression-free survival of 6 mo. The response in PSMA imaging was closely related to serum PSA levels, and 19 patients showed tumor regression. The second modality regularly confirmed PSMA imaging and serum PSA findings, but often with an additional delay of 3–6 mo (Fig. 4).

(A) Patient with diffuse spine metastases at baseline presented with complete remission regarding serum PSA and PSMA scan at month 6. (B) At month 9, bone scan became confirmative, presenting favorable response; however—most probably because of unspecific bone reactions—some residual lesions did not diminish completely.
Any PSA response was observed in 33 of 38 patients who survived at least 8 wk after the first treatment, and in 24 of them (63%), PSA decreased by more than 50%. Median TTP was 7.0 mo. The best PSA response and the PSA response at defined time points are presented in Figure 5.
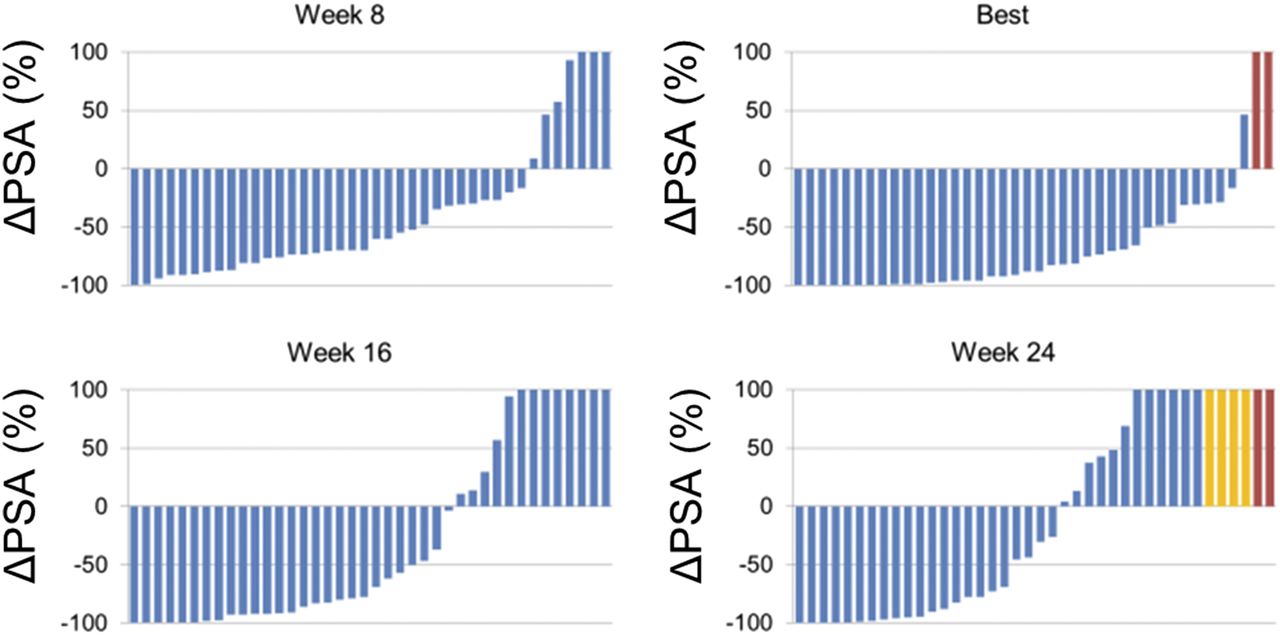
Waterfall graphs of PSA response. Patients who died before week 8 (red) or discontinued because of xerostomia (yellow) were classified as progression.
Swimmer-Plot Analysis
The median duration of any first-, second-, third-, or fourth-line therapy, irrespective of the particular treatment modality (i.e., each treatment line presents a mixture of abiraterone, docetaxel, enzalutamide, and others), was 8.0, 7.0, 6.0, and 4.0 mo, respectively.
The median duration of abiraterone, docetaxel, enzalutamide, cabazitaxel, and 223Ra, irrespective of treatment line (i.e., irrespective of whether the respective drug was administered as first-, second-, third-, or fourth-line treatment), was 10.0, 6.5, 6.5, 6.0, and 4.0 mo, respectively.
The most common first-line therapy was abiraterone, with a median duration of 12.0 mo in this setting; administered as second-, third-, or fourth-line therapy, the median duration of response dropped to 7.0 mo. The second most common first-line therapy was docetaxel, with a median duration of 8.0 mo. Docetaxel was also the most common second-line treatment strategy; however, the median duration dropped to 6.5 mo if docetaxel was administered as third- or fourth-line therapy. Enzalutamide was the most common third-line therapy, with a median duration of 6.0 mo; the duration was 7.0 mo when enzalutamide was given earlier and 5.5 mo when given later.
In contrast, the median duration of tumor control under 225Ac-PSMA-617, always applied as the last-line therapy, was 9.0 mo.
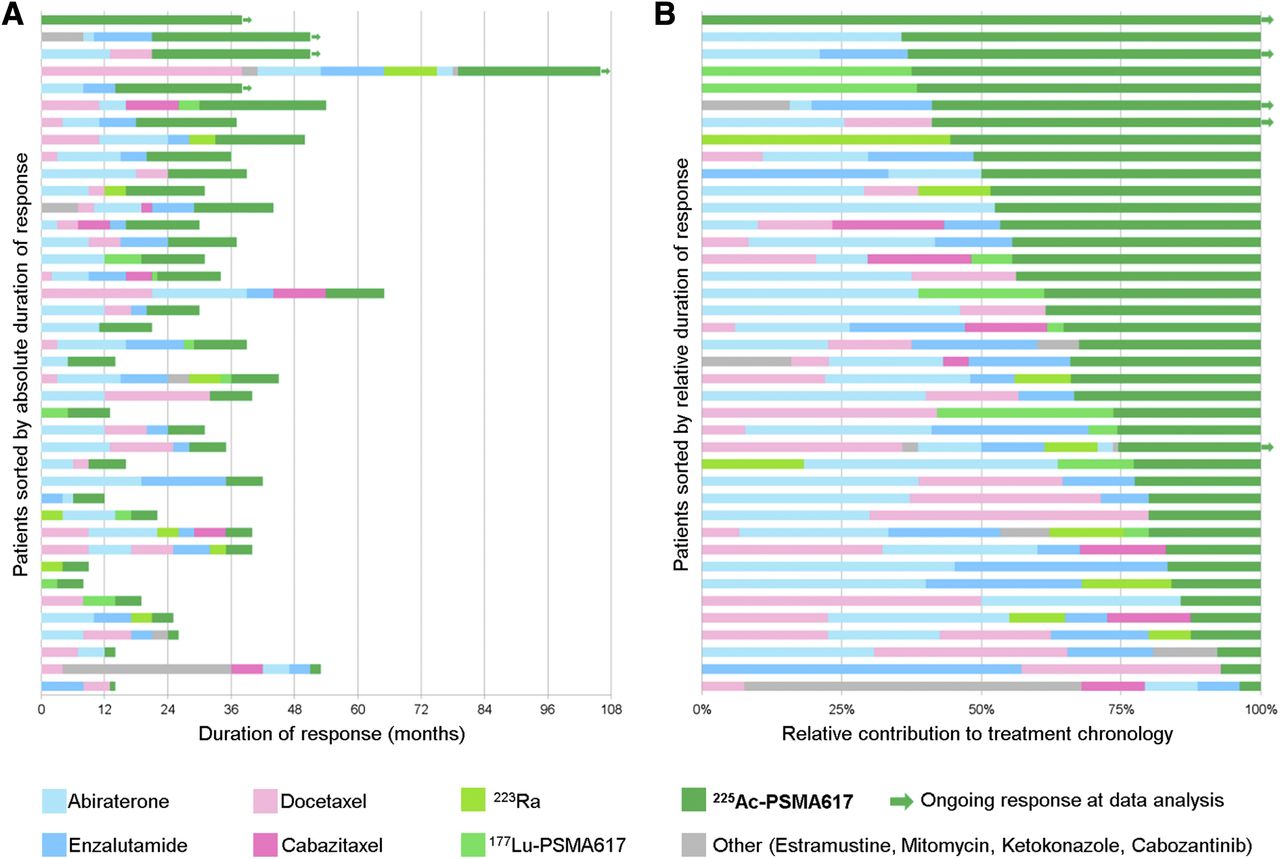
The absolute values of tumor control, in months, are graphically summarized in Figure 6A. The swimmer lanes of 225Ac-PSMA-617, normalized relative to the duration of preceding treatment lines, are provided as Figure 6B.
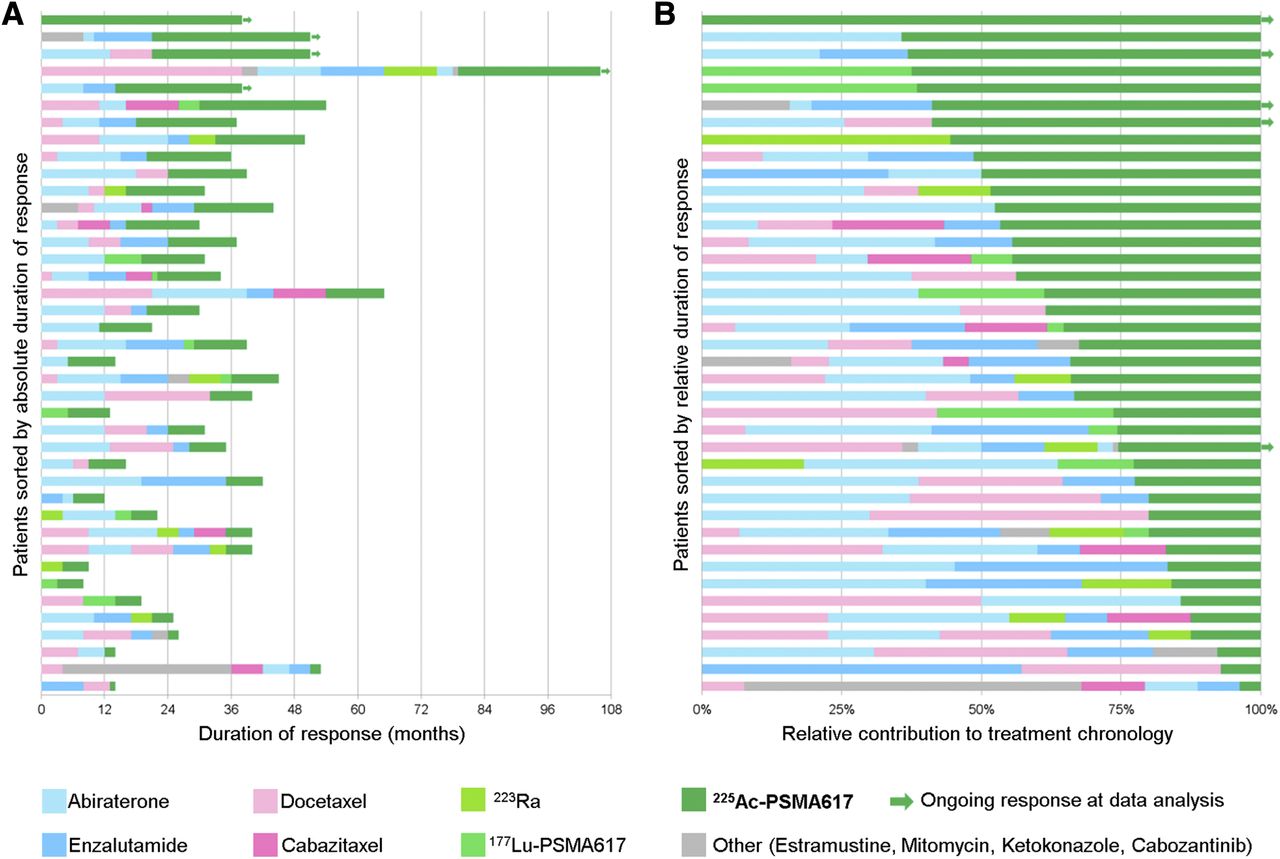
Swimmer plots showing duration of tumor control in months (A) and relative to duration of previous treatment lines (B).
DISCUSSION
Here, we report our clinical findings for 40 patients receiving 225Ac-PSMA-617 as a salvage therapy. Dosimetry estimates and an empiric dose finding—that is, adverse events were used to define the maximum tolerable treatment activity—have already been published previously (17). This evaluation was dedicated to identifying the first indicators to project the clinical efficacy of PSMA TAT.
In contrast to “medical research” (Declaration of Helsinki, paragraphs 1–36), “unproven intervention in clinical practice” (paragraph 37) and our national regulatory adaption thereof does not allow systematic patient selection criteria, randomized controls, or follow-up examinations exceeding the clinical demand, making the obligatory retrospective interpretation of derived findings difficult. Nevertheless, it is explicitly requested that new information be recorded and, when findings are considered such as would affect clinical decision making, made publicly available.
In ALSMYPCA (23), the only recent formal clinical trial that accepted patients who either had received docetaxel or were ineligible to receive it, 43% of the recruited patients had been declared unfit for chemotherapy by their supporting oncologist. The fact that 70% of our patients had prior chemotherapy (despite approval of secondary hormone manipulation in the predocetaxel setting) underlines our attempt to use approved treatment lines on as many patients as possible and for as long as possible before offering an unproven intervention as a salvage option.
Surrogate Markers of Response
To assess the antitumor activity of new drugs in early-phase clinical trials, the criteria of the Prostate Cancer Clinical Trials Working Group 2 (21) recommend PSA response, preferably reported in waterfall graphs, as one of the most established surrogate parameters. At weeks 8 and 16, we observed a PSA decline of more than 50% in 24 (63%) of 38 patients. This rate exceeds the biochemical response rates of 177Lu-PSMA-617, which were reported to range from 30% to 59% (Table 2). In addition, a complete response with regard to PSA and PSMA PET/CT was achieved in 5 (13%) of 38 225Ac-PSMA-617 patients; in contrast, under 177Lu-PSMA RLT, complete remissions are anecdotic (∼1%) even in less advanced disease (9,10). However, PSA is only a surrogate for response, and an improved PSA response is not necessarily predictive of a longer progression-free survival and OS in 225Ac-PSMA patients than in 177Lu-PSMA patients. The drugs cabozantinib and tasquinimod presented significant antitumor activity by biomarker and imaging response in phase 2 trials (24,25) but failed to demonstrate improvement in median OS in succeeding phase 3 trials (26,27). However, the PSA response rates for cabozantinib and tasquinimod have been remarkably lower than those of either 177Lu-PSMA-617 or 225Ac-PSMA-617.
Biochemical Response to First Cycle of PSMA RLT
Comparison to Historical Controls
Another way to cope with the lack of randomized controls would be comparison to historical controls. However, prognostic baseline findings have a significant impact on progression-free survival and OS. For example, abiraterone demonstrated a progression-free survival and OS of 16.5 and 35.3 mo, respectively, in the predocetaxel setting but only 5.6 and 15.8 mo, respectively, in the postdocetaxel setting (28,29). The situation is similar for enzalutamide: OS was 32.4 mo in the predocetaxel setting but only 18.4 mo in the postdocetaxel setting (30,31). In contrast, the absolute improvement of OS for the newly approved drugs, versus placebo, was 3.4 mo (34.7 vs. 30.3) for abiraterone, 2.2 mo (32.4 vs. 30.2) for enzalutamide, 2.4 mo (15.1 vs. 12.7) for cabazitaxel, and 3.6 mo (14.9 vs. 11.3) for 223Ra (23,28–31). Thus, different inclusion criteria had a higher impact on the observed OS than the treatment-related absolute benefit itself had. It is difficult to compare PSMA RLT with these recent phase 3 trials because the stringent inclusion criteria of formal clinical trials translate into artificial patient collectives (e.g., either 0% or 100% previous docetaxel), not ideally reflecting clinical reality (23,28–31). Because the recently approved drugs were developed simultaneously, there are no large numbers of historical controls that already had access to various secondary hormone manipulations.
The baseline characteristics provided in the actual reports about 177Lu-PSMA RLT (Table 1) were closer to those found in today’s clinical practice and more appropriate to serve as comparators. Nevertheless, the reported cohorts present remarkable heterogeneity. An initial read of Table 1 demonstrates that progression-free survival (4.5 vs. 13.7 mo) and OS (8 vs. >28 mo) differ by a factor of 3 among different centers (4,6). However, the prognostic factors have been identified to serve as tools for comparison of studies with different inclusion criteria: Eastern Cooperative Oncology Group performance score, site of visceral metastasis, and high baseline PSA have the highest effect on OS (32–34).
In comparison to Baum et al., who reported the longest progression-free survival and OS of all groups (6), our patient cohort was remarkably more challenging with regard to all relevant prognostic parameters: time from diagnosis to first treatment cycle (7.5 vs. 49 mo), percentage of patients with an Eastern Cooperative Oncology Group performance score of 2 or more (0% vs. 20%), baseline PSA level (43 vs. 169 ng/mL), number of patients with visceral metastases (twice as many), and number of patients who had undergone previous chemotherapy or secondary hormone therapy (more than twice as many) (Table 1). Regarding site of metastasis, baseline PSA level, clinical performance score, and previous therapies, our cohort was somewhat comparable to those of the Münster (4) and Munich (7) groups. In addition, considering that our department offered both 177Lu-PSMA RLT and 225Ac-PSMA TAT and that one of our main stratification criteria was the presence of diffuse-type bone or bone marrow involvement, our patient cohort included a remarkably high percentage (45%) with a superscan pattern (Table 1). This subgroup was not highlighted by most other centers (4–7); however, in the ALSYMPCA trial, such an advanced tumor spread was found in less than only 10% of the patients (23). Despite our even more challenging patient cohort, our median TTP and OS for 225Ac-TAT appeared preferable to those found for 177Lu-PSMA by the Münster (4) and Munich (7) groups (median TTP, 7.0 vs. 4.5 and 5.5 mo; median OS, >12 vs. 8 mo). Nevertheless, a comparison between heterogeneous patient cohorts and historical controls will always be affected by several uncertainties and possible bias effects.
Swimmer-Plot Analysis
In recent years, as several new drugs for metastatic castration-resistant prostate cancer received approval, it became apparent that the respective sequence of treatment modalities is important with regard to potential cross-resistance between drugs with a similar mechanism of action (35,36). Therefore, the updated PCWG3 criteria (22) now recommend reporting the number and sequence of lines of prior systemic treatment rather than continuing to use the nomenclature “predocetaxel vs. postdocetaxel.” The PCWG3 criteria also introduce the “no longer clinically benefiting” concept, which leaves more room for individualized provider–patient decisions, such as on whether to continue therapy even in the face of PSA progression as long as clinical symptoms remain sufficiently controlled. The swimmer plot has been suggested as a preferable way to visualize the sequence and duration of different treatment options (22). For a heterogeneous patient collective without matching controls, such as the group of patients evaluated in this report, this kind of analysis demonstrates some welcome advantages. Using a patient as that patient’s own intraindividual comparator attenuates the random effects normally introduced by the selection bias. Visual presentation also simplifies the interpretation if an observed effect is not only statistically significant but also clinically relevant in comparison to the typical course of disease.
It is well in line with the literature and the theoretic background of cross-resistance and advancing tumor dedifferentiation (35,36) that each of the approved drugs (abiraterone, enzalutamide, docetaxel, cabazitaxel) performed best when used in earlier treatment lines. Tumor control was longer with 225Ac-PSMA-617 therapy than with most of the preceding treatment modalities (with first-line abiraterone being the only exception) even when given in the last-line setting. After the castration-resistant stage was reached, the duration of tumor control achieved with PSMA TAT contributed approximately 30% (mean) to the remaining lifetime (Fig. 3). Whether 225Ac-PSMA-617 can benefit from being given as an earlier treatment line should be elaborated in additional studies.
One critical observation during this evaluation was the high number of patients who, despite a promising PSA response, discontinued therapy because of intolerable xerostomia. However, our treatment regimen was based on dosimetry and empiric dose escalation of the first treatment cycle, with only a limited number of observations available for succeeding cycles (17). It was reported that salivary gland uptake is dependent on tumor load and that the tumor-sink effect may have a protective effect for the first injection (37). Because we often observed that there was already a remarkable PSA response after cycle 1 (Fig. 1), we consider it reasonable to deescalate the treatment activity of the second and third administrations for these patients. The masses of the salivary glands are independent of body weight, and no other organs were found to be dose-limiting; thus, we also presumed that the treatment activity could be simplified to a fixed dose. As a consequence, we adopted our standard operating procedure accordingly (Supplemental Table 1). It is hoped that treatment deescalation will improve tolerability without loss of too much antitumor activity. Furthermore, blocking or displacement strategies should be developed to reduce the dose to critical organs, as was already done in a preclinical study for the kidneys (38).
CONCLUSION
Clinical antitumor activity is highly supported by a positive response by surrogate parameters such as radiologic progression-free survival and PSA. As far as a reliable interpretation can be allowed (considering the differences in baseline patient characteristics), clinical efficacy against tumor seems higher for 225Ac-PSMA TAT than for 177Lu-PSMA RLT, but coradiation to the salivary glands also seems higher. Swimmer-plot analysis provides the first longitudinal indicators of the clinical efficacy of PSMA TAT with regard to the duration of tumor control. It is hoped that minor modifications to the treatment regimen will further refine the therapeutic range of this novel treatment concept.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Jan. 11, 2018.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 16, 2017.
- Accepted for publication December 7, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Deescalated 225Ac-PSMA-617 Versus 177Lu/225Ac-PSMA-617 Cocktail Therapy: A Single-Center Retrospective Analysis of 233 Patients
- Current Status of Prostate-specific Membrane Antigen-targeted Alpha Radioligand Therapy in Prostate Cancer
- An Intrapatient Dosimetry Comparison of 177Lu-rhPSMA-10.1 and 177Lu-PSMA-I&T in Patients with Metastatic Castration-Resistant Prostate Cancer
- Tandem Isotope Therapy with 225Ac- and 177Lu-PSMA-617 in a Murine Model of Prostate Cancer
- Clinical Experience with [225Ac]Ac-PSMA Treatment in Patients with [177Lu]Lu-PSMA-Refractory Metastatic Castration-Resistant Prostate Cancer
- Clinical Translation of Targeted {alpha}-Therapy: An Evolution or a Revolution?
- Clinical Translation of Targeted {alpha}-Therapy: An Evolution or a Revolution?
- 225Ac-MACROPATATE: A Novel {alpha}-Particle Peptide Receptor Radionuclide Therapy for Neuroendocrine Tumors
- Treatment of prostate cancer with CD46 targeted 225Ac alpha particle radioimmunotherapy
- Dosimetry in Radiopharmaceutical Therapy
- mCRPC Patients Receiving 225Ac-PSMA-617 Therapy in the Post-Androgen Deprivation Therapy Setting: Response to Treatment and Survival Analysis
- Effects of 225Ac-Labeled Prostate-Specific Membrane Antigen Radioligand Therapy in Metastatic Castration-Resistant Prostate Cancer: A Meta-Analysis
- [18F]-Labeled PARP-1 PET Imaging of PSMA Targeted Alpha Particle Radiotherapy Response
- The History of Prostate-Specific Membrane Antigen as a Theranostic Target in Prostate Cancer: The Cornerstone Role of the Prostate Cancer Foundation
- Radionuclide Therapy in Prostate Cancer: From Standalone to Combination PSMA Theranostics
- The Impact of Monosodium Glutamate on 68Ga-PSMA-11 Biodistribution in Men with Prostate Cancer: A Prospective Randomized, Controlled Imaging Study
- Comparative Preclinical Biodistribution, Dosimetry, and Endoradiotherapy in Metastatic Castration-Resistant Prostate Cancer Using 19F/177Lu-rhPSMA-7.3 and 177Lu-PSMA I&T
- Mechanisms of Resistance to Prostate-Specific Membrane Antigen-Targeted Radioligand Therapy in a Mouse Model of Prostate Cancer
- The PSMA-targeting Half-life Extended BiTE Therapy AMG 160 has Potent Antitumor Activity in Preclinical Models of Metastatic Castration-resistant Prostate Cancer
- First Clinical Results for PSMA-Targeted {alpha}-Therapy Using 225Ac-PSMA-I&T in Advanced-mCRPC Patients
- The Effects of Monosodium Glutamate on PSMA Radiotracer Uptake in Men with Recurrent Prostate Cancer: A Prospective, Randomized, Double-Blind, Placebo-Controlled Intraindividual Imaging Study
- Genetic signature of prostate cancer mouse models resistant to optimized hK2 targeted {alpha}-particle therapy
- JHU-2545 Selectively Shields Salivary Glands and Kidneys during PSMA-Targeted Radiotherapy
- Patients Resistant Against PSMA-Targeting {alpha}-Radiation Therapy Often Harbor Mutations in DNA Damage-Repair-Associated Genes
- Mathematical Modeling of Preclinical Alpha-Emitter Radiopharmaceutical Therapy
- Predictors of Overall and Disease-Free Survival in Metastatic Castration-Resistant Prostate Cancer Patients Receiving 225Ac-PSMA-617 Radioligand Therapy
- Impact of 18F-PSMA-1007 Uptake in Prostate Cancer Using Different Peptide Concentrations: Preclinical PET/CT Study on Mice
- {alpha}-Particle-Emitter Radiopharmaceutical Therapy: Resistance Is Futile
- Future of Theranostics: An Outlook on Precision Oncology in Nuclear Medicine
- Melanocortin 1 Receptor-Targeted {alpha}-Particle Therapy for Metastatic Uveal Melanoma
- Feasibility of CXCR4-Directed Radioligand Therapy in Advanced Diffuse Large B-Cell Lymphoma
- Monosodium Glutamate Reduces 68Ga-PSMA-11 Uptake in Salivary Glands and Kidneys in a Preclinical Prostate Cancer Model
- Salivary Gland Toxicity of PSMA Radioligand Therapy: Relevance and Preventive Strategies