


Abstract
This was a head-to-head comparison between 68Ga-labeled prostate-specific membrane antigen (PSMA)-11 and 18F-fluciclovine PET/CT in a series of 10 patients with prostate cancer (PCa) recurrence. Methods: In total, 288 patients with PCa recurrence were enrolled in a prospective study of 68Ga-PSMA-11 PET/CT imaging for recurrent disease localization (ClinicalTrials.gov identifier NCT02940262). We retrospectively identified 10 patients who underwent clinically indicated 18F-fluciclovine PET/CT prior to enrollment. Results: The median time between the 2 scans was 2.2 mo (range, 0.2–4.2 mo). The median prostate-specific antigen (PSA) value was 1.0 ng/mL (mean, 4.7 ng/mL; range, 0.13–18.1 ng/mL) and 1.1 ng/mL (mean, 6.2 ng/mL; range, 0.24–31.3 ng/mL) at the time of 18F-fluciclovine and 68Ga-PSMA-11 PET/CT, respectively. Five of 10 patients (50%) were negative with 18F-fluciclovine but positive with 68Ga-PSMA-11 PET/CT. Two of 10 patients (20%) were positive with both 18F-fluciclovine and 68Ga-PSMA-11 PET/CT, but 68Ga-PSMA-11 PET/CT showed additional lymph nodes metastasis. Three of 10 patients (30%) were negative with both 18F-fluciclovine and 68Ga-PSMA-11 PET/CT. Conclusion: This case series suggests improved detection rates for 68Ga-PSMA-11 PET/CT when compared with 18F-fluciclovine PET/CT in patients with recurrent PCa. Prospective trials designed to directly compare the two should be initiated.
See an invited perspective on this article on page 787.
Localizing recurrent prostate cancer (PCa) with PET/CT imaging is clinically relevant because these patients can undergo salvage therapies with curative intent (1). Identifying sites of recurrence with a high accuracy is important to select the best therapeutic approach. Several molecular imaging approaches have been proposed over the last decade. The best results for assessing patients with PCa recurrence were obtained with 18F-fluciclovine and PSMA-targeted PET radiotracers (2–5).
Anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid (18F-fluciclovine [Axumin; Blue Earth Diagnostics]) is a synthetic amino acid and likely a substrate of l-amino acid (L-type amino acid transporter 1 in particular) and the alanine-serine-cysteine transporters (specifically alanine-serine-cysteine transporter 2) (6). The results of the first prospective studies led to Food and Drug Administration approval in 2016 and to reimbursement by the Center for Medicare and Medicaid Service in 2017 for patients with PCa recurrence (7). Thus, 18F-fluciclovine serves as a reference standard for evaluating other PET PCa approaches.
Prostate-specific membrane antigen (PSMA) is a membrane-bound metallopeptidase overexpressed at high levels in 90%–100% of PCa lesions (8). 68Ga-PSMA-11 is a highly specific urea-based inhibitor (Glu-NH-CO-NH-Lys-(Ahx)-[68Ga(HBED-CC)]) that internalizes on ligand binding (8). 68Ga-PSMA-11 PET/CT demonstrates high efficacy in restaging PCa and is thus widely used in clinical trials and routine practice worldwide (2,4,9). These investigations also reported a favorable tumor-to-background ratio for 68Ga-PSMA-11 to detect PCa lesions and a high sensitivity for lesion detection even at low serum levels of prostate-specific antigen (PSA) (<2 ng/mL) (2).
To date, there has been only a single case report of a patient imaged with both 18F-fluciclovine and 18F-radiolabeled PSMA ligand (18F-DCFPyL) PET/CT (10), and to our knowledge, no head-to-head comparison between 68Ga-PSMA-11 and 18F-fluciclovine PET/CT has been published. Here, we report a case series of 10 patients with recurrent PCa who underwent both 68Ga-PSMA-11 PET/CT and 18F-fluciclovine PET/CT. Although we are aware that the present case series can at best provide the impetus for a large prospective trial, we nevertheless felt that these observations were worthwhile reporting.
MATERIALS AND METHODS
Patient Population
From October 2016 to November 2017, 288 patients with PCa recurrence were enrolled in a prospective study of 68Ga-PSMA-11 PET/CT imaging for recurrent disease localization (ClinicalTrials.gov identifier, NCT02940262). The institutional review board approved this study (approval 16-001095), and all subjects gave written informed consent. We retrospectively identified 10 patients who had undergone clinically indicated 18F-fluciclovine PET/CT at other institutions within 4 mo before 68Ga-PSMA-11 PET/CT. We obtained all DICOM files and clinical reports on the 18F-fluciclovine PET/CT scans to perform a head-to-head image analysis. Patient characteristics are listed in Table 1. Four patients had a history of primary surgery and salvage radiation therapy (patients 2, 4, 5, and 10), 2 had primary surgery and adjuvant radiation therapy (patients 6 and 9), 2 had primary surgery only (patients 7 and 8), and 2 had undergone a primary combination therapy of external-beam radiation, brachytherapy, and androgen deprivation (patients 1 and 3). All patients had prior inconclusive or negative imaging results within 3 mo before the 18F-fluciclovine PET/CT study: CT in 6 of 10 patients (patients 1, 2, 3, 8, 9, and 10), multiparametric MRI in 5 of 10 (patients 2, 4, 5, 7, and 8), 18F-fluoride PET/CT in 5 of 10 (patients 1, 3, 5, 9, and 10), and 11C-choline PET/CT in 2 of 10 (patients 2 and 6).
Patient Characteristics and PET/CT Results
PET/CT Imaging Acquisition
68Ga-PSMA-11 PET/CT imaging was performed according to recent guidelines (11) with a 64-detector PET/CT device (Biograph True Point 64 or Biograph mCT; Siemens). 68Ga-PSMA-11 was used as the PSMA ligand (8). The median injected dose was 196 MBq (range, 137–322 MBq). To reduce bladder activity, patients received 20 mg of intravenous furosemide at the time of tracer injection. The median uptake period was 62 min (range, 53–68 min). A diagnostic CT scan (200–240 mAs, 120 kV) was performed after intravenous injection of contrast agent (if not contraindicated) followed by the whole-body PET image acquisition (2–4 min/bed position).
18F-fluciclovine PET/CT was performed at each site according to manufacturer dosing and administration guidelines (6). 18F-fluciclovine was manufactured by automated radiosynthesis (12). Patients were scanned after avoiding significant exercise for at least 24 h to minimize uptake in background muscle, after fasting for at least 4 h to normalize amino acid levels, and immediately after voiding. The median injected dose was 371 MBq (range, 337–396 MBq). The median uptake period was 4 min (range, 2–15 min). A nondiagnostic CT scan was obtained for attenuation correction, followed by PET image acquisition (5 min/bed position in the pelvis, 3 min/bed position in the remainder of the body).
PET/CT Imaging Analysis
18F-fluciclovine and 68Ga-PSMA-11 PET/CT images were coregistered and analyzed by an experienced nuclear medicine physician according to recent recommendations (6,11,13) using OsiriX: any focal uptake above the level of the surrounding background and not associated with physiologic uptake or known pitfalls (14) was considered suggestive of malignancy. On the basis of TNM staging, the following regions were systematically analyzed: prostate bed/seminal vesicle remnants (T), pelvic lymph nodes (LNs) (N) (internal iliac, obturator, external iliac, perirectal, presacral, common iliac), extrapelvic LNs (M1a) (retroperitoneal, inguinal, chest, other), bone (M1b), and other visceral organs (M1c).
RESULTS
PET/CT results and detailed findings are listed in Tables 1 and 2. The median time between the 2 scans was 2.2 mo (range, 0.2–4.2 mo). The median PSA levels were 1.0 ng/mL (mean, 4.7 ng/mL; range, 0.13–18.1 ng/mL) and 1.1 ng/mL (mean, 6.2 ng/mL; range, 0.24–31.3 ng/mL) at the time of 18F-fluciclovine and 68Ga-PSMA-11 PET/CT, respectively. Recurrence sites were localized by 18F-fluciclovine PET/CT in only 2 of 10 patients (20%), whereas 68Ga-PSMA-11 PET/CT detected recurrence sites in 7 of 10 patients (70%). Five of 8 patients (63%) (patients 1, 2, 5, 9, and 10) were negative with 18F-fluciclovine PET/CT but positive with 68Ga-PSMA-11. One patient (patient 3) was positive for local recurrence with both tracers but 68Ga-PSMA-11 revealed additional extrapelvic LN involvement. One patient (patient 7) was positive for a single external iliac LN recurrence with both tracers but 68Ga-PSMA-11 revealed additional obturator LN involvement. Three patients (patients 4, 6, and 8) had concordantly negative scans. No difference was observed between our 18F-fluciclovine PET/CT analysis and the original 18F-fluciclovine PET/CT clinical reports.
Detailed PET/CT Results
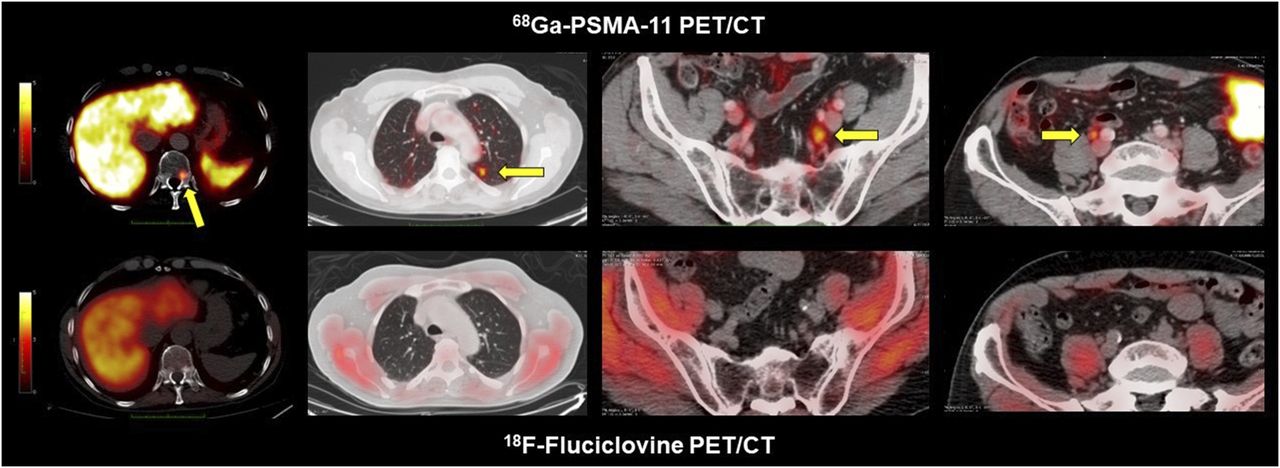
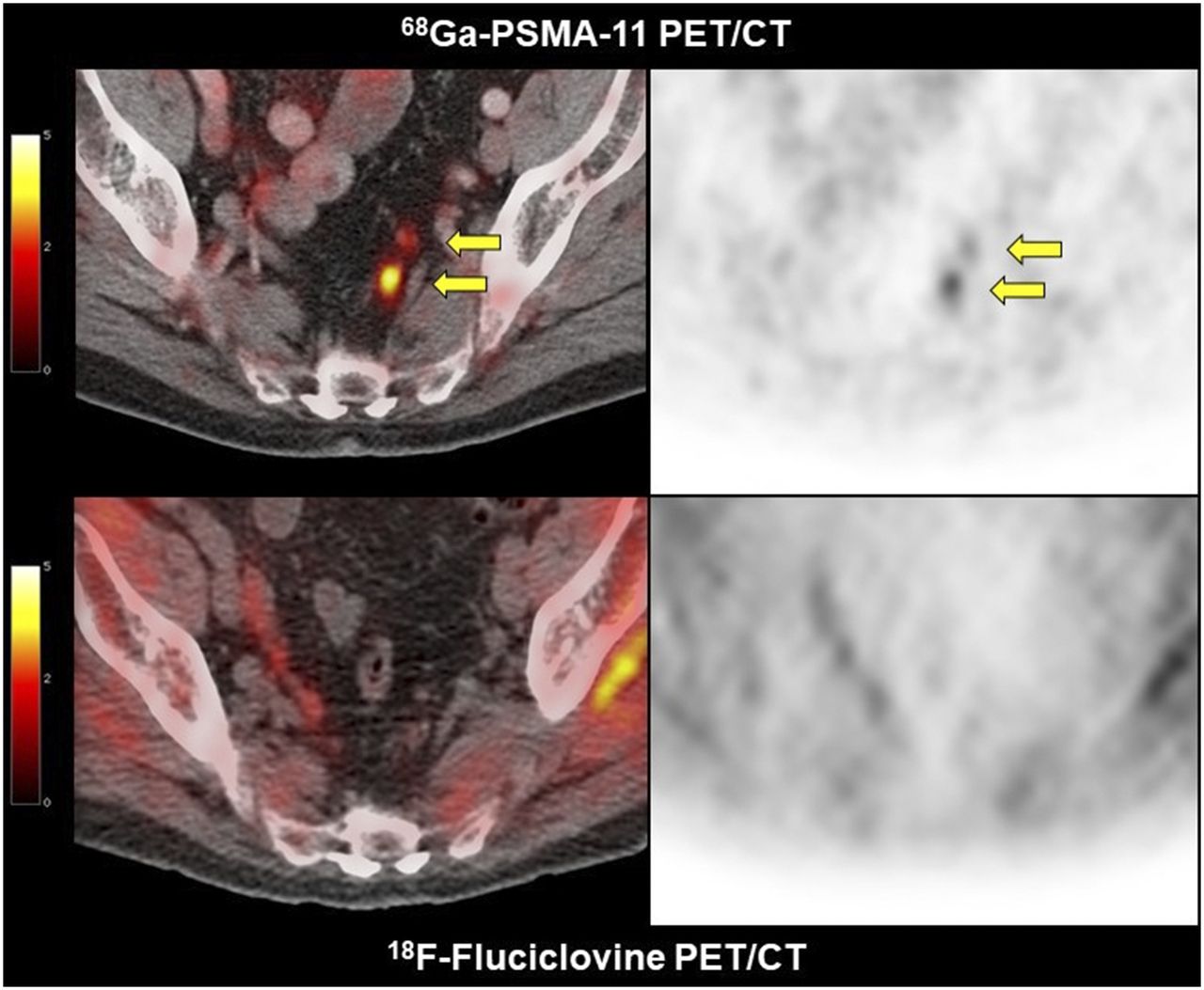
Specifically, the 5 patients who were negative with 18F-fluciclovine but positive with 68Ga-PSMA-11 had the following findings. Patient 1 had multiple 68Ga-PSMA-11–positive lesions involving a small right external iliac LN (5 mm, SUVmax, 7.7), multiple small retroperitoneal LNs (4–5 mm, SUVmax, 17), a right hilar LN (SUVmax, 4), and T8 (Fig. 1). He then received androgen deprivation therapy (ADT). In patient 2, intense 68Ga-PSMA-11 uptake in a solitary osteoblastic T11 lesion (SUVmax, 6) and faint 68Ga-PSMA-11 uptake in multiple bilateral common iliac and presacral LNs (6–8 mm; SUVmax 2.0), as well as multiple bilateral lung nodules (6–10 mm; SUVmax, 2.6), were evident (Fig. 2). He received proton therapy focused on the T11 metastasis and refused any systemic treatment. In patient 5, 4 small perirectal LNs showed mild 68Ga-PSMA-11 uptake (3–4 mm; SUVmax, 2.9) (Fig. 3). His referring physician opted for active surveillance. In patient 9, intense 68Ga-PSMA-11 uptake in multiple left pelvic LNs (4–8 mm; SUVmax, 12.6), retroperitoneal LNs (4–6 mm; SUVmax, 10.3), and supradiaphragmatic LNs (4–8 mm; SUVmax, 16.1) were seen (Fig. 4). The patient received ADT. Finally, patient 10 had a single tiny right upper common iliac LN with intense 68Ga-PSMA-11 uptake (3 mm; SUVmax, 5.3) (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). He received focused ablative RT and ADT initiation was put on hold.

Patient 1 had negative 18F-fluciclovine PET/CT results but positive 68Ga-PSMA-11 PET/CT results. Yellow arrows show intense focus of uptake in T8 lesion, right external iliac LN (5 mm), and tiny retroperitoneal LN (4–5 mm). White arrow indicates urinary excretion of tracer in ureteral dilation. There was no uptake in corresponding structures on 18F-fluciclovine PET/CT.
Patient 2 had negative 18F-fluciclovine PET/CT results and positive 68Ga-PSMA-11 PET/CT results. Arrows show uptake in T11 lesion, lung micronodules, presacral LN, and common iliac LN. There was no uptake in corresponding structures on 18F-fluciclovine PET/CT.
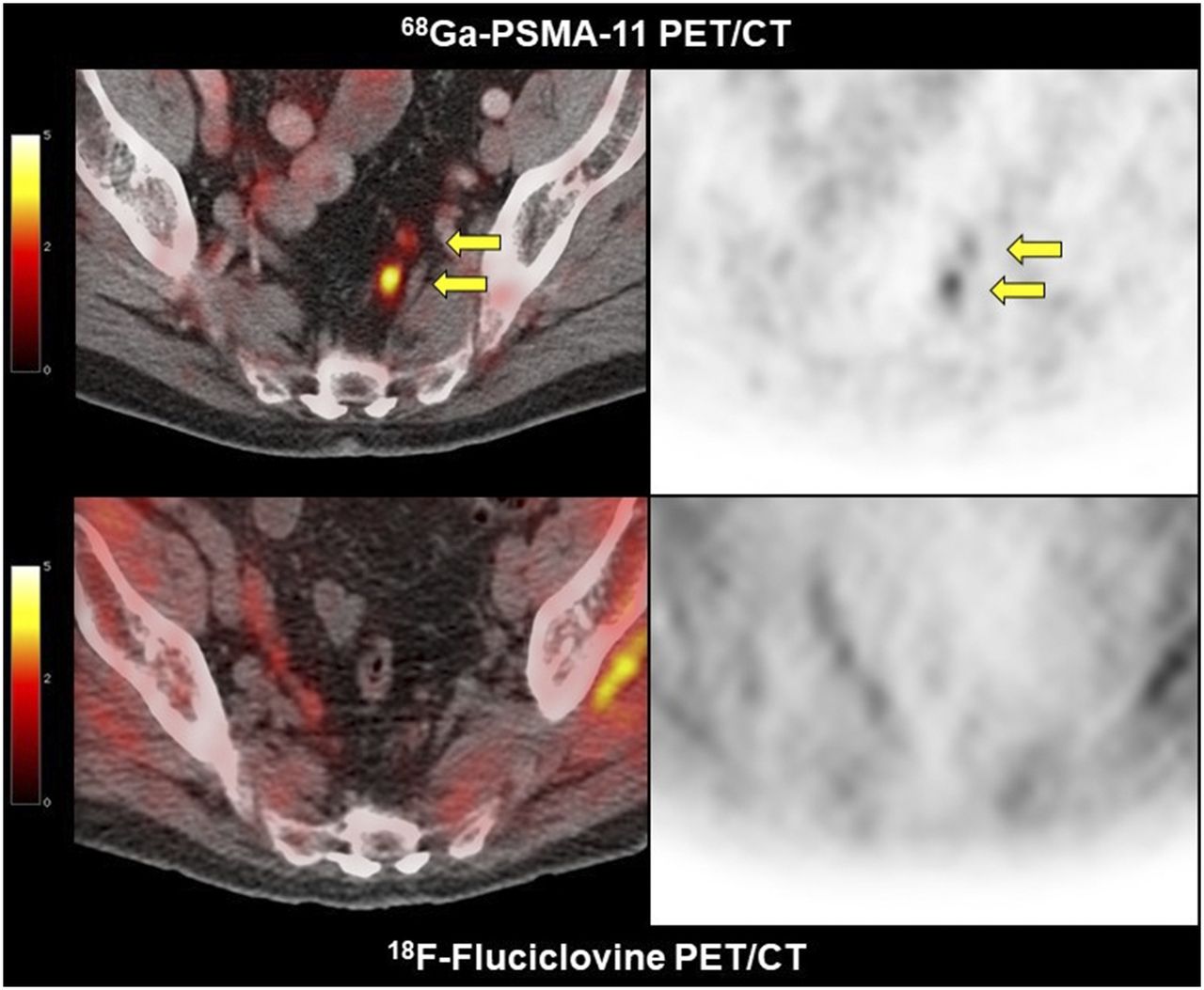
Patient 5 had negative 18F-fluciclovine PET/CT results and positive 68Ga-PSMA-11 PET/CT results. Arrows show uptake in tiny perirectal LN (3–4 mm). Corresponding LN on 18F-fluciclovine PET/CT showed no uptake.
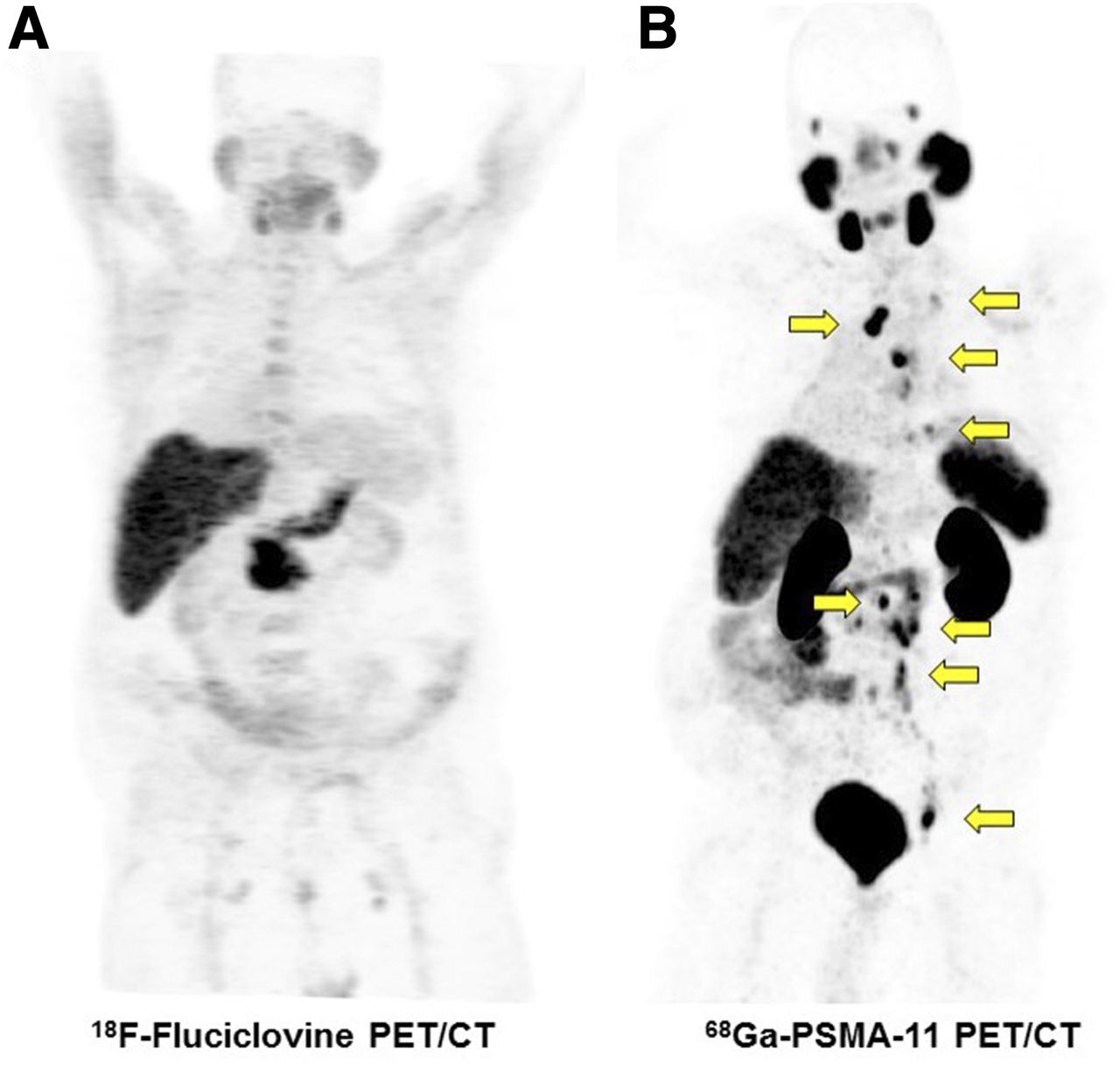
Maximum-intensity-projection 18F-fluciclovine PET (A) and 68Ga-PSMA-11 PET (B) in patient 9. Arrows indicate intense uptake in pelvic, abdominal, thoracic, and supraclavicular LNs. Corresponding LNs on 18F-fluciclovine PET showed no uptake.
The 2 patients who were positive with 18F-fluciclovine had the following findings. Patient 3 had a small 18F-fluciclovine–positive local recurrence (SUVmax, 3.5) whereas 68Ga-PSMA-11 PET/CT showed a much larger local recurrence with intense uptake (SUVmax, 8.9). Moreover, 68Ga-PSMA-11 PET/CT demonstrated additional abnormal retroperitoneal LNs (8–10 mm; SUVmax, 4.7) (Fig. 5; Supplemental Fig. 2). The patient received ADT. Patient 7 had a 18F-fluciclovine–positive right external iliac LN recurrence (7 mm; SUVmax, 4.9). 68Ga-PSMA-11 uptake was much more intense (SUVmax, 8.9). In addition, 68Ga-PSMA-11 PET/CT demonstrated an additional abnormal tiny right obturator LN (4 mm; SUVmax, 3.0) (Supplemental Fig. 3). The patient underwent unilateral right pelvic LN dissection. Three of 8 resected LNs were positive for metastatic adenocarcinoma.

Maximum-intensity-projection 18F-fluciclovine PET (A) and 68Ga-PSMA-11 PET (B) in patient 3. Blue arrow indicates faint and limited uptake in left prostate gland. Yellow arrows indicate diffuse and intense uptake in prostate gland and in extrapelvic LN.
Patients 4, 6, and 8 had concordantly negative findings on 68Ga-PSMA-11 PET/CT and 18F-fluciclovine PET/CT. Patient 4 and 6 were monitored for PSA changes, whereas patient 8 underwent salvage radiation therapy to both prostate bed and pelvic LNs.
DISCUSSION
We are aware that the results of this small case series do not indicate the superiority of 68Ga-PSMA-11 PET/CT over 18F-fluciclovine PET/CT. However, the findings of the 2 tests were so strikingly different that we felt a brief report would be prudent. Issuing a report also seemed justified because no direct comparisons between these 2 tests have been published.
Although 7 of 10 studies (70%) were positive with 68Ga-PSMA-11, 8 of 10 18F-fluciclovine studies were negative (80%), and disease extent was underestimated in both of the patients with a positive 18F-fluciclovine study. Surprisingly, 4 18F-fluciclovine PET/CT studies were negative despite fairly extensive disease on the 68Ga-PSMA-11 PET/CT studies.
Although extensive evidence has been established to support the use of 68Ga-PSMA-11 PET/CT even in patients with biochemical recurrence of PCa at very low serum PSA levels (2,9), much less is known about the performance of 18F-fluciclovine PET/CT.
The main study that led to Food and Drug Administration approval for 18F-fluciclovine was a retrospective analysis of 596 patients (3). The detection rates were 67.7% in the whole population (mean PSA level, 5.43 ng/mL) and 41.4% in the lowest quartile of serum PSA levels (<0.79 ng/mL). Several studies reported a better diagnostic performance for 68Ga-PSMA-11 PET/CT (9). The high accuracy in the detection of PCa metastases at very low serum PSA levels and the high sensitivity for detecting small lesions were considered the strength of PSMA-based imaging (2,4,9).
The high false-negative rate of 18F-fluciclovine scans in the current patients with relatively high serum PSA levels is concerning. Bone marrow and mostly muscle background activity (Fig. 5A) may have interfered with detection of extraprostatic lesions.
There was, of course, a significant selection bias in the current case series. Patients likely had negative 18F-fluciclovine PET/CT results and were therefore referred for 68Ga-PSMA-11 PET/CT. Moreover, the median interval between the 2 scans, 2.2 mo, likely favored lesion detection with 68Ga-PSMA-11 PET/CT. But the median increase in PSA level between the 2 scans was only 0.1 ng/mL (range, 0.03–13.2 ng/mL).
Another important limitation was that histologic confirmation of 68Ga-PSMA-11–positive lesions was available for only one patient (patient 7) who underwent surgery. Histologic verification of lesions in patients with PCa recurrence is not routinely done, and 68Ga-PSMA-11–positive lesions were not biopsied. Two patients (patients 2 and 10) received focal ablative radiation therapy after the scans, whereas the others had nonfocal treatment (ADT or salvage radiation therapy to both prostate bed and pelvic LNs) or active surveillance. Therefore, we cannot exclude that these 68Ga-PSMA-11–positive lesions were in fact false-positive.
CONCLUSION
This case series suggests superior detection rates of 68Ga-PSMA-11 when compared with 18F-fluciclovine PET/CT in patients with recurrent PCa. Although far from being definitive evidence of superiority, the observation strongly supports the initiation of prospective trials to directly compare the performance of 68Ga-PSMA-11 PET/CT with that of 18F-fluciclovine PET/CT.
DISCLOSURE
Jeremie Calais is the recipient of a grant from the Foundation ARC pour la recherche sur le cancer (grant SAE20160604150). Wolfgang Fendler received a scholarship from the German Research Foundation (Deutsche Forschungsgemeinschaft [DFG], grant 807122). Matthias Eiber was supported by the SFB 824 (DFG Sonderforschungsbereich 824, project B11) from the Deutsche Forschungsgemeinschaft, Bonn, Germany. No other potential conflict of interest relevant to this article was reported.
Footnotes
Guest Editor: Michael Graham, University of Iowa
Published online Dec. 14, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 6, 2017.
- Accepted for publication November 26, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-DCFPyL PET Acquisition, Interpretation, and Reporting: Suggestions After Food and Drug Administration Approval
- Disparities in PET Imaging for Prostate Cancer at a Tertiary Academic Medical Center
- Head-to-Head Comparison of 68Ga-PSMA-11 with 18F-PSMA-1007 PET/CT in Staging Prostate Cancer Using Histopathology and Immunohistochemical Analysis as a Reference Standard
- Prospective Evaluation of 18F-DCFPyL PET/CT in Biochemically Recurrent Prostate Cancer in an Academic Center: A Focus on Disease Localization and Changes in Management
- Best Practices for 18F-Fluciclovine PET/CT Imaging of Recurrent Prostate Cancer: A Guide for Technologists
- One-Step 18F-Labeling and Preclinical Evaluation of Prostate-Specific Membrane Antigen Trifluoroborate Probes for Cancer Imaging
- Molecular Imaging of Prostate Cancer: Choosing the Right Agent
- Reply: Comparison of 68Ga-PSMA-11 and 18F-Fluciclovine PET/CT in a Case Series of 10 Patients with Prostate Cancer Recurrence: Prospective Trial Is on Its Way
- Comparison of 68Ga-PSMA-11 and 18F-Fluciclovine PET/CT in a Case Series of 10 Patients with Prostate Cancer Recurrence: Interesting, but Far from Definitive