


Abstract
18F-Galacto-RGD has been developed for PET of αvβ3 integrin expression, a receptor involved in, for example, angiogenesis and metastasis. Our aim was to study the kinetics and biodistribution of 18F-Galacto-RGD in cancer patients. Methods: Nineteen patients with metastases of malignant melanoma (n = 7), sarcomas (n = 10), or osseous metastases (n = 2) were examined. After injection of 133–200 MBq 18F-Galacto-RGD, 3 consecutive emission scans from the pelvis to the thorax or dynamic emission scans of the tumor over 60 min, followed by 1 static emission scan of the body, were acquired. Time–activity curves and standardized uptake values (SUVs) were derived by image region-of-interest analysis with image-based arterial input functions. Compartmental modeling was used to derive the distribution volume for muscle tissue and tumors. Results: 18F-Galacto-RGD showed rapid blood clearance and primarily renal excretion. SUVs in tumors ranged from 1.2 to 9.0. Tumor-to-blood and tumor-to-muscle ratios increased over time, with peak ratios of 3.1 ± 2.0 and 7.7 ± 4.3, respectively, at 72 min. The tumor kinetics were consistent with a 2-tissue compartment model with reversible specific binding. Distribution volume values were, on average, 4 times higher for tumor tissue (1.5 ± 0.8) than those for muscle tissue (0.4 ± 0.1). The data suggest that there was only minimal free and bound (specific or nonspecific) tracer in muscle tissue. Conclusion: 18F-Galacto-RGD demonstrates a highly favorable biodistribution in humans with specific receptor binding. Most important, this study shows that 18F-Galacto-RGD allows visualization of αvβ3 expression in tumors with high contrast. Consequently, this tracer offers a new strategy for noninvasive monitoring of molecular processes and may supply helpful information for planning and controlling of therapeutic approaches targeting the αvβ3 integrin.
Integrins are heterodimeric glycoproteins, which are involved in cell–cell and cell–matrix interactions (1). One member of this class of receptors is the integrin αvβ3, which has been shown to play an essential role in the regulation of tumor growth, local invasiveness, and metastatic potential (2,3). Moreover, αvβ3 is also highly expressed on activated endothelial cells during angiogenesis (4). Inhibition of the αvβ3-mediated cell–matrix interactions has been found to induce apoptosis of activated endothelial cells. However, αvβ3 antagonists can induce apoptosis not only of endothelial cells but also of αvβ3-positive tumor cells, resulting in a direct cytotoxic effect on these cells (5). Thus, the use of αvβ3 antagonists is currently being evaluated as a strategy for anticancer therapy (6). However, currently available morphologic imaging techniques such as CT or MRI are limited in monitoring treatment with this new class of drugs. The response rate and success of an antitumor therapy are generally assessed by evidence of a significant reduction of the tumor size achieved during therapy. Yet, this method may not be applicable for a therapy with αvβ3 antagonists, which is aimed at disease stabilization and prevention of metastases. Therefore, noninvasive determination of αvβ3 expression would be crucial for the assessment of receptor expression during therapy and for the pretherapeutic recognition of those patients most amenable to αvβ3-directed therapies.
Several integrins, including αvβ3, bind to the tripeptide sequence arginine-gylcine-aspartic acid (single-letter code RGD) of different matrix proteins, such as fibronectin and vitronectin (7). On the basis of the αvβ3-selective pentapeptide cyclo(-Arg-Gly-Asp-d-Phe-Val-), a variety of radiolabeled αvβ3 antagonists for SPECT and PET have been developed (8). The glycosylated cyclic pentapeptide 18F-Galacto-RGD resulted from tracer optimization based on the first-generation peptide 125I-3-iodo-d-Tyr4-cyclo(-Arg-Gly-Asp-d-Tyr-Val-) (9). 18F-Galacto-RGD demonstrated high affinity and selectivity for the αvβ3 integrin in vitro, receptor-specific accumulation in a murine αvβ3-positive tumor model, as well as high metabolic stability and predominantly renal elimination (10,11). Moreover, initial data from our patient study indicate that this tracer can be used to noninvasively determine αvβ3 expression in humans (12,13). The present study was performed for detailed characterization of the biodistribution and pharmacokinetics of 18F-Galacto-RGD in cancer patients. Patients with melanomas and musculoskeletal sarcomas have been chosen, because the role of αvβ3 in angiogenesis and metastatic potential has already been described for these tumors (10,14). Moreover, phase I and phase II studies with humanized anti-αvβ3 antibodies have already been performed in patients with soft-tissue sarcomas (15,16).
MATERIALS AND METHODS
Radiopharmaceutical Preparation
Synthesis of the labeling precursor and subsequent 18F labeling were performed as described previously (11). For application in patients, high-performance liquid chromatography eluent was completely removed by evaporation, and 0.5 mL absolute ethanol and 10 mL phosphate-buffered saline (pH 7.4) were added and passed through a Millex GV filter (Millipore GmbH) before injection.
Patients
The study was approved by the ethics committee of the Technische Universität München and informed written consent was obtained from all patients. Nineteen patients included in the study (10 women, 9 men; mean age ± SD, 55.7 ± 16.2 y; range, 26–89 y), had either malignant melanoma with lymph node or organ metastases (n = 7) or malignant lesions of the musculoskeletal system (n = 12; Table 1). Inclusion criteria consisted of known or suspected malignancy, >18 y of age, and the ability to give written and informed consent. Exclusion criteria consisted of pregnancy, lactation period, and impaired renal function (serum creatinine level, >1.2 mg/dL).
Demographics, Pathology, and Scan Protocols of Study Population
PET Procedure
Imaging was performed with either an ECAT EXACT HR+ (n = 8) or an ECAT EXACT (n = 11) PET scanner (CTI/Siemens). Before tracer injection of 18F-Galacto-RGD (133–200 MBq), a transmission scan was acquired for 5 min per bed position (5 bed positions) using 3 rotating 68Ge rod sources (each with ∼90 MBq 68Ge). Two imaging protocols were used to study the whole-body distribution and time course of tumor activity. In 6 patients, dynamic emission scans of 22 frames, during 60 min after bolus injection of the tracer, were acquired covering the region of the tumor to obtain time–activity curves in malignant lesions (10 frames × 30 s, 4 frames × 60 s, 4 frames × 180 s, and 4 frames × 600 s). The dynamic scan was followed by a static emission scan (5 bed positions, 5 min per bed position) covering a field of view from the pelvis to the upper thorax and, when necessary, an additional bed position covering the region of the tumor (when located outside the torso). In the remaining 12 subjects, 3 consecutive static emission scans were acquired in the caudocranial direction, beginning 5 min after injection of 18F-Galacto-RGD, covering a field of view from the pelvis to the thorax (5–7 bed positions, 5 min per bed position). The average starting times of these scans were 6.3 ± 2.7, 35.7 ± 7.9, and 72.0 ± 12.2 min (mean ± SD) after injection.
Image Analysis of Biodistribution Data
Positron emission data were reconstructed using the ordered-subsets expectation maximization (OSEM) algorithm. The OSEM reconstructions were performed with 8 iterations and 4 subsets. The images were attenuation corrected using the transmission data collected over the same region of emission imaging. For image analysis, CAPP software, version 7.1 (CTI/Siemens), was used. Images were calibrated to standardized uptake values (SUVs) or to Bq/mL. The SUV was calculated according to the following formula: (measured activity concentration [Bq/mL] × body weight [g])/injected activity (Bq) (17).
In the static emission scans, circular regions of interest (ROIs) were placed over major organs (lung, left ventricle, liver, spleen, intestine, kidneys, bladder, muscle) and tumor tissue by an experienced operator using the first emission scan acquired shortly after injection. The location of the ROIs was then copied to the second and third emission scans. The diameter of the ROIs was set to 1.5 cm, except for the kidneys and intestine. Here, polygonal ROIs adapted to the contour of the kidney or covering the area of intestine with the maximum activity were drawn. Results are either expressed in SUV or in percentage of the injected dose/volume (%ID/L). The total fraction of injected activity found in the bladder was determined by multiplying the injected dose/volume found in the bladder by the total bladder volume in the last emission scan. The bladder volume was measured by drawing polygonal ROIs around the bladder on each slice with visible bladder activity. For drawing these ROIs, the images were scaled to the maximum SUV in the bladder to avoid an overestimation of the volume due to the high activity concentration in the urine.
Kinetic Modeling
The selection of time–activity curves and subsequent kinetic analyses were performed using the PMOD Medical Imaging Program, version 2.5 (PMOD Group). An ROI approach was applied to the dynamic images to obtain time–activity curves for lesions as well as background tissue (muscle). In the case of tumor tissue, circular ROIs with a diameter of 1.0 cm were drawn over the region with the maximum count density (“tumor maximum”) and in the 2 immediately adjacent slices (18). Additionally, polygonal ROIs were drawn over the whole tumor in all slices with visible tumor uptake. Circular ROIs with a diameter of 15 mm were drawn over muscle tissue in the whole volume of interest. The last frame of the dynamic image series was used to define the ROIs for the tumor, tumor maximum, and muscle. To derive an image-based input function, circular ROIs with a diameter of 5–8 mm were placed over the largest artery in the volume in every slice where the artery could be identified on the frames acquired from 30 to 60 s after injection. All ROIs were then projected onto the complete dynamic dataset and time–activity curves were subsequently derived.
In 2 patients, no correct arterial input function could be derived from the datasets, because the tumors were located below the knee and no adequate artery could be visualized in the scans. Therefore, these scans had to be excluded from the kinetic modeling analysis.
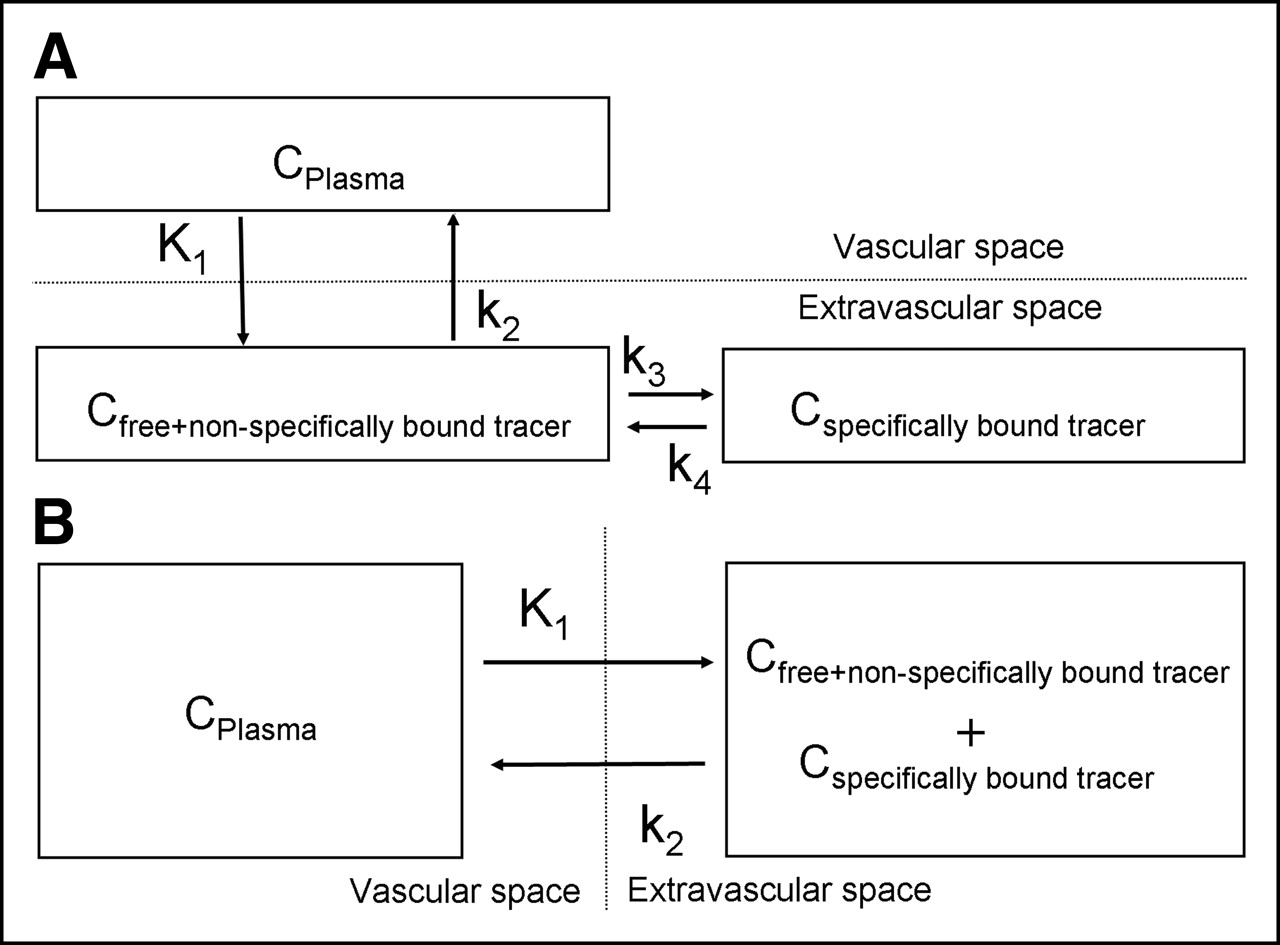
Various compartment models were fitted to the data (Fig. 1) and kinetic constants were estimated by minimizing the sum of squared differences between the tissue time–activity curves and the model-predicted curves. A 2-tissue-compartment (2-TC) model best characterized the tumor and tumor maximum data. In muscle tissue, it was difficult to resolve the second compartment; therefore, a 1-tissue-compartment (1-TC) model was used for further analysis of this tissue. The total distribution volume (DVtot) was calculated for all ROIs based on the directly estimated kinetic rate constants (K1–k4). The peak plasma activity of the tracer might be underestimated by using an image-based arterial input function instead of arterial sampling and, consequently, K1 might be overestimated in our model. Therefore, we also calculated DVtot with K1 set to 0.1 for comparison, which was 3–4 times lower than the calculated K1 values. This value was chosen according to results of kinetic modeling studies using 18F-FDG in solid malignant tumors (19). A more-detailed description of the compartment models and the mathematic definition of DVtot can be found elsewhere (20,21).
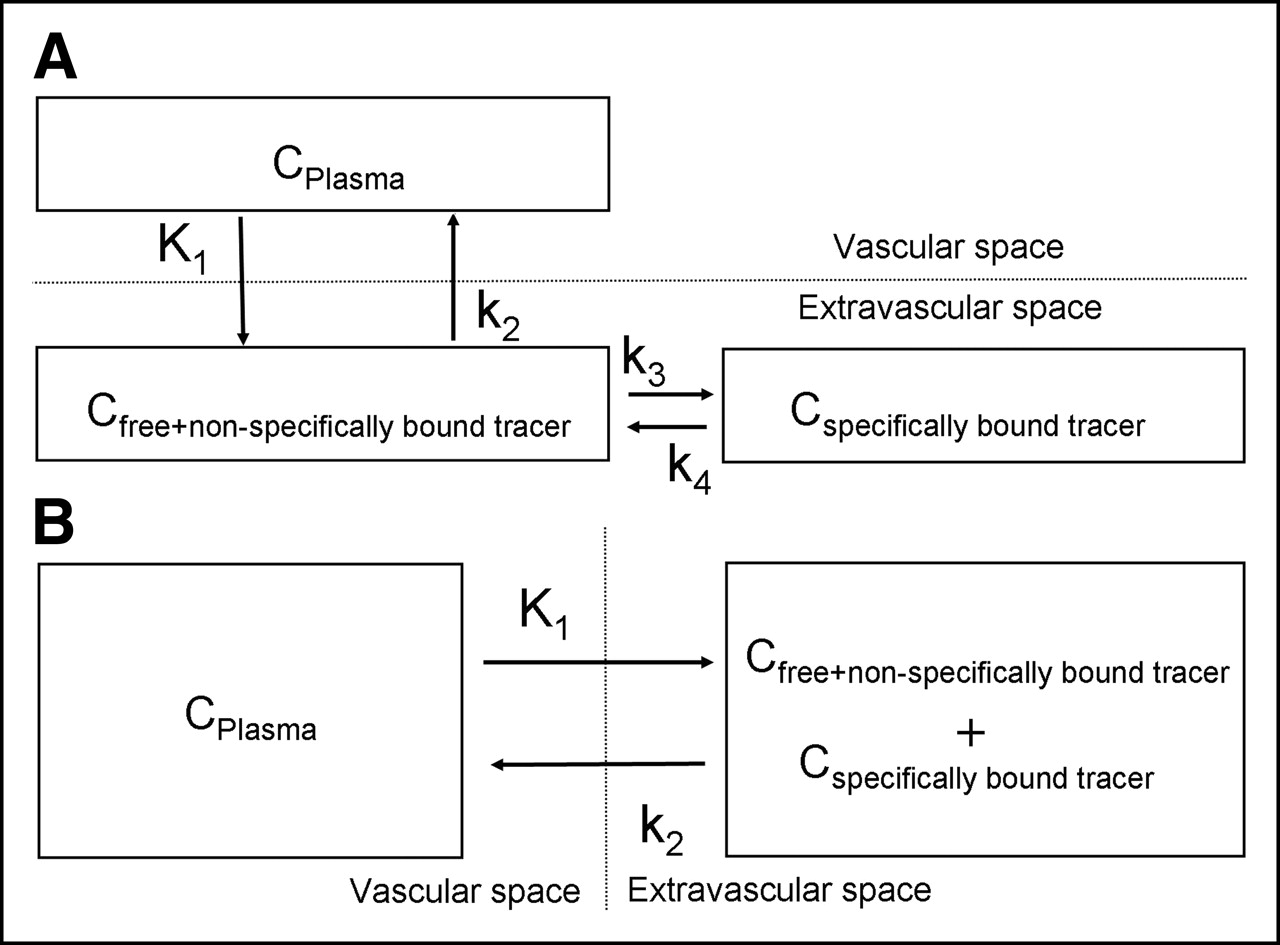
Compartmental models used for 18F-Galacto-RGD kinetics. Vascular compartment represents concentration of unmetabolized tracer in plasma (CPlasma). 2-Tissue-compartment model (A) considers 2 extravascular compartments accounting for free and nonspecifically bound tracer in tissue (Cfree+nonspecifically bound tracer) and 18F-Galacto-RGD specifically bound to αvβ3 receptors (Cspecifically bound tracer). In 1-tissue compartment model (B), all tissue compartments are united to 1 compartment (Cfree+nonspecifically bound tracer + Cspecifically bound tracer). K1–k4 = kinetic rate constants.
The half-time of tracer activity in blood was calculated by fitting a biexponential function to the time points after the peak intensity of the time–activity curve derived from the image-based arterial input function.
RESULTS
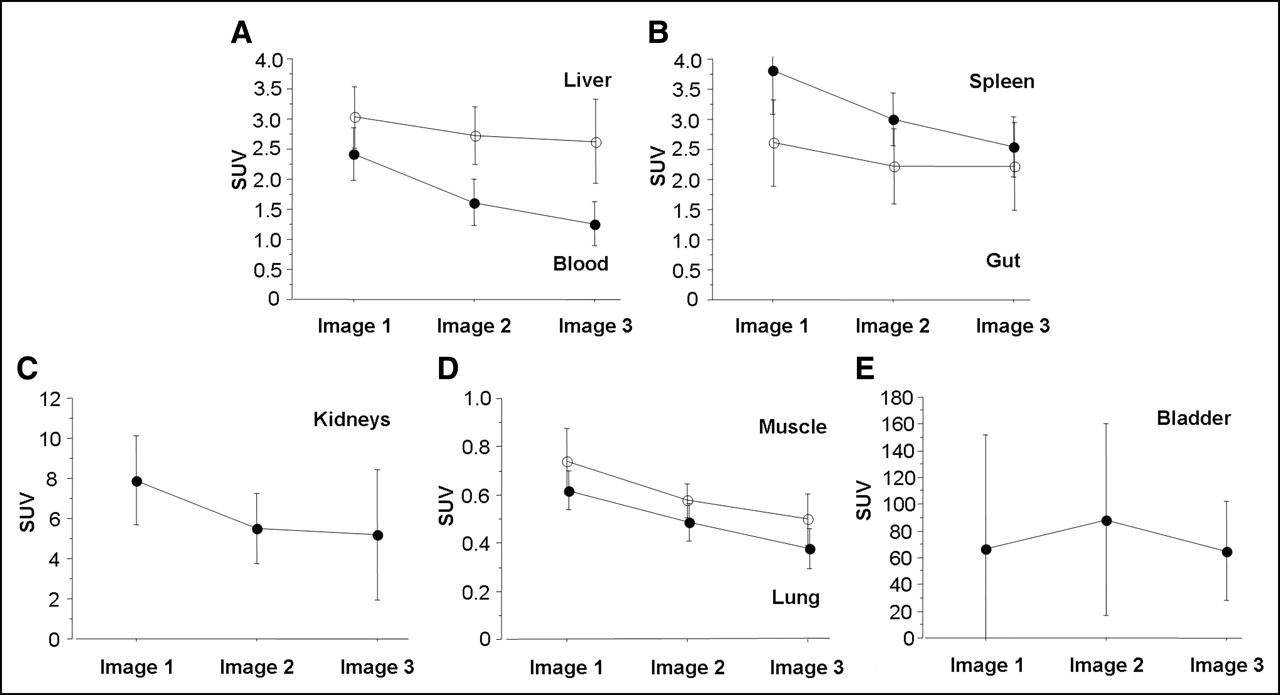
Figure 2 shows the tracer kinetics of 18F-Galacto-RGD in various organs (mean values of the 12 patients who received 3 emissions scans). Table 2 summarizes the results of the last emission scan of all patients, including the 6 patients who had a dynamic emission scan during the first 60 min and a patient with only 1 static emission scan. 18F-Galacto-RGD shows rapid renal excretion and clearance from the blood pool, with 1.8 %ID/L blood-pool activity 72 min after injection (SUV, 1.3 ± 0.4) and 102 %ID/L urinary bladder activity (SUV, 76.5 ± 38.6). The mean fraction of injected activity found in the bladder at 72 min after injection was 49.2% ± 29.1%. The dynamic scans revealed a biexponential clearance of tracer activity from the blood with a rapid first half-time of 0.36 ± 0.28 min and a slower second half-time of 34.13 ± 17.15 min.
Mean SUVs and %ID/L on Basis of Last Emission Scan 72 Minutes After Injection

Mean SUVs ± SDs for major organs and muscle tissue on basis of 3 static emission scans of 12 patients (mean start times of acquisition: bladder, 6, 36, and 72 min after injection; intestine, 13, 43, and 79 min after injection; kidneys, 19, 49, and 85 min after injection; liver/spleen, 21, 51, and 87 min after injection; blood [left ventricle]/muscle, 24, 54, and 90 min after injection; lung [apex], 29, 59, and 95 min after injection).
The highest SUVs in solid organs 72 min after injection were found in the kidneys (SUV, 5.2 ± 3.2), followed by the liver (SUV, 2.7 ± 0.7) and the spleen (SUV, 2.5 ± 0.5). In the liver, there is some retention of activity over time. In contrast, in the spleen, a rapid decrease of activity over time was found, paralleling the decrease in blood-pool activity. There was no significant tracer accumulation in the gut during the examination period. Low activities in the lung and muscle were found with SUVs of 0.4 ± 0.08 and 0.5 ± 0.1, respectively.
Tracer uptake in tumor lesions was very heterogeneous. In 17 of 19 (89.4%) patients, 23 of 29 (79.3%) malignant lesions could be detected. In 2 patients, no regionally increased tracer uptake compared with background activity was found (patients 1 and 19). For 1 patient, the primary tumor as well as an osseous metastasis showed intense tracer uptake, whereas in several pulmonary metastases no tracer uptake was found (patient 8). For another patient, tracer uptake in the primary tumor was moderate, whereas an osseous metastasis showed intense tracer uptake (patient 18). This considerable inter- as well as intraindividual variance in tracer accumulation is reflected in the large SD of the mean SUV for all lesions (Fig. 3). The mean tumor SUV declined only slightly over time to 3.7 ± 2.3 at 72 min after injection, whereas the tumor-to-blood ratio and the tumor-to-muscle ratio increased over time (peak values 3.3 ± 2.2 and 7.7 ± 5.4, respectively).

Mean SUVs ± SD in tumors (A), mean tumor-to-muscle ratios ± SD (B), and mean tumor-to-blood-ratios ± SD (C) for all tumor lesions with visible uptake (12 lesions in 10 patients (mean start times of acquisition: 6, 36, and 72 min after injection; mean start times of acquisition of tumor regions, 17, 47, and 83 min after injection).
In all dynamic scans, tumors showed rapid tracer accumulation during the first 10 min followed by a plateau phase with no, or only minimal, decrease of the activity until 60 min after injection (Fig. 4). The results of the modeling data are summarized in Table 3. The 2-TC model used for tumors and tumor maximum fit well with parameter coefficients of variation (CoV) between 12.3% and 29.3% for tumors and of 24.6%–37.1% for tumor maximum. For muscle, the 1-TC model fits the data best and resulted in parameter CoV values between 15.4% and 16.2%. DVtot values for tumors were always higher than the DVtot for muscle, with a mean ratio of 3.85 for tumors and 9.22 for tumor maximum relative to muscle tissue. Because K1 might be overestimated by using an image-based input function, we also calculated a model fit with a lower K1 value of 0.1 for the datasets. In this scenario, the 1-TC model fit better for 3 of 4 patients for tumors and tumor maximum. However, the resulting DVtot values were similar to the results with a calculated K1 (tumor, 1.41 ± 0.55; tumor maximum, 3.60 ± 2.29; muscle, 0.37 ± 0.12).
Kinetic Modeling Data

Time–activity curves of representative dynamic scan over 60 min (patient 10) for tumor, tumor maximum, and muscle tissue. Circles denote measured data (kBq/mL), whereas lines are results of curve fit of kinetic modeling data, using a 2-TC model for tumor and tumor maximum and a 1-TC model for muscle. Note excellent fit of curves and measured data. The blood curve shows rapid tracer elimination from the blood pool.
Figure 5 shows representative dynamic coronal image sets of normal organs of emission images acquired at 5, 30, and 60 min after tracer injection. Figure 6 shows a representative example of a patient with a large chondrosarcoma of the pelvis and intense heterogeneous tracer uptake of the tumor, which decreased only slightly over time.

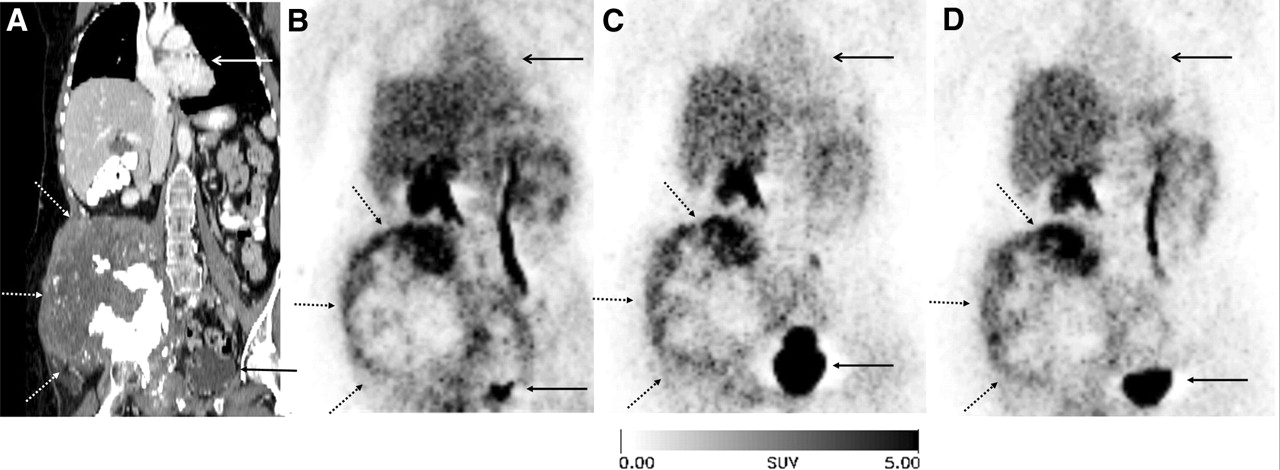
18F-Galacto-RGD scan of 56-y-old patient with multiple metastases to liver and intestine from malignant melanoma (patient 1). Static emission scans at 5, 30, and 60 min after injection (from left to right) with representative coronal views at level of kidneys (A–C) and at level of gallbladder (D–F). No lesions show tracer uptake, indicating lack of, or very low, αvβ3 expression. Liver (arrow with dotted line) shows moderate activity with only slow decrease over time, whereas spleen (open arrow tip) shows higher activity initially, decreasing over time. Gallbladder (closed arrow tip) shows increasing activity over time, indicating hepatobiliary excretion of tracer.

A 26-y-old patient (patient 9) with large chondrosarcoma of right pelvis (arrow with dotted line). Coronal reformation of CT scan (A) and corresponding coronal views of 18F-Galacto-RGD scan (B–D) at 5, 40, and 90 min after injection (from left to right). Note rapid renal tracer excretion into bladder (closed arrow tip) and decrease of activity in blood pool (heart: open arrow tip). Tumor shows heterogeneous tracer uptake with focal maximum at top of tumor. Note there is only minimal decrease of activity over time. Patient had to void after second scan (C) and had to be repositioned for last scan (D); therefore, bladder is smaller in third scan compared with second scan.
DISCUSSION
In this study, we describe the detailed biodistribution and kinetics of the αvβ3-selective tracer 18F-Galacto-RGD in cancer patients. This tracer shows a predominantly renal excretion with rapid blood clearance allowing imaging of tumor lesions with good contrast. The kinetic modeling data indicate specific receptor binding of 18F-Galacto-RGD with low binding in background tissue. These findings suggest that 18F-Galacto-RGD can be effectively used for imaging of αvβ3 expression in humans.
In contrast to the high-activity concentration found in the bladder due to the renal elimination, no increase in activity in the gut was observed, indicating that there is no significant biliary excretion of the tracer into the intestine during the observation period of ∼90 min. The background activity in muscle tissue and blood pool was very low. However, delineation of lesions with moderate tracer uptake might be impaired in the liver and spleen due to the relatively high background activity in these organs. Image quality in the pelvis might also be impaired by artifacts due to the high bladder activity. However, activity concentration in the bladder can be reduced by administration of a diuretic agent (e.g., furosemide, 20 mg intravenously) together with the tracer similar to protocols used for imaging with 18F-FDG.
Nearly 80% of lesions demonstrated uptake of 18F-Galacto-RGD with high tumor-to-blood and tumor-to-muscle ratios. This corroborates previous findings that the integrin αvβ3 plays an essential role in aberrant angiogenesis, which is a hallmark of cancer and an indicator of poor prognosis (22). Tumor-induced angiogenesis is a multistep process involving a variety of different pro- and antiangiogenic factors and is often triggered by the release of growth factors and cytokines from hypoxic tumor cells. Neovascularization is required for adequate nutrition supply and, thus, important for tumor growth. Moreover, it also facilitates the metastatic spread into the blood circulation (23). It requires the interaction of endothelial cells with components of the extracellular matrix during formation of new microvessels, which is mediated by endothelial integrins (24). It has been shown that αvβ3 is expressed on angiogenic blood vessels and on malignant tumors at elevated levels (25) and that a variety of αvβ3 integrin antagonists effectively prevents tumor metastasis, growth, and angiogenesis (26,27). Therefore, it is expected that many tumor lesions can be identified by an αvβ3-selective tracer such as 18F-Galacto-RGD. However, the intensity and pattern of uptake showed large inter- and intraindividual variations: In some patients, metastases and primary tumor demonstrated marked differences in tracer uptake (Fig. 7). In melanoma patients, there were large variations in tracer uptake observed between the patients (Fig. 8). These findings indicate great inter- and intraindividual diversity of αvβ3 expression in cancer patients, which is in accordance with the literature. For example, it is well established for human melanoma that the expression of αvβ3 plays an important role during the transition of cells from the radial growth phase to the vertical growth phase (28,29). However, further changes leading to metastases may be more complex and ultimately not dependent on αvβ3 expression or αvβ3 might be expressed in varying quantities during various stages of metastatic dissemination (30). Moreover, experiments in knockout mice lacking the integrin αvβ3 showed normal developmental angiogenesis and even excessive tumor angiogenesis, which led to a reevaluation of the role of αvβ3 in neovascularization (31). It seems that the absence of αvβ3 may be compensated by other vascular integrins or the vascular endothelial growth factor receptor 2 (VEGF R2), which are downregulated by αvβ3 (32,33). Therefore, it is currently assumed that αvβ3 bears a positive and a negative regulatory role in angiogenesis, depending on the respective biologic context. Therefore, noninvasive methods of determining the αvβ3 receptor status in humans, such as 18F-Galacto-RGD PET, might be used to further elucidate the complex role of this integrin in vivo.
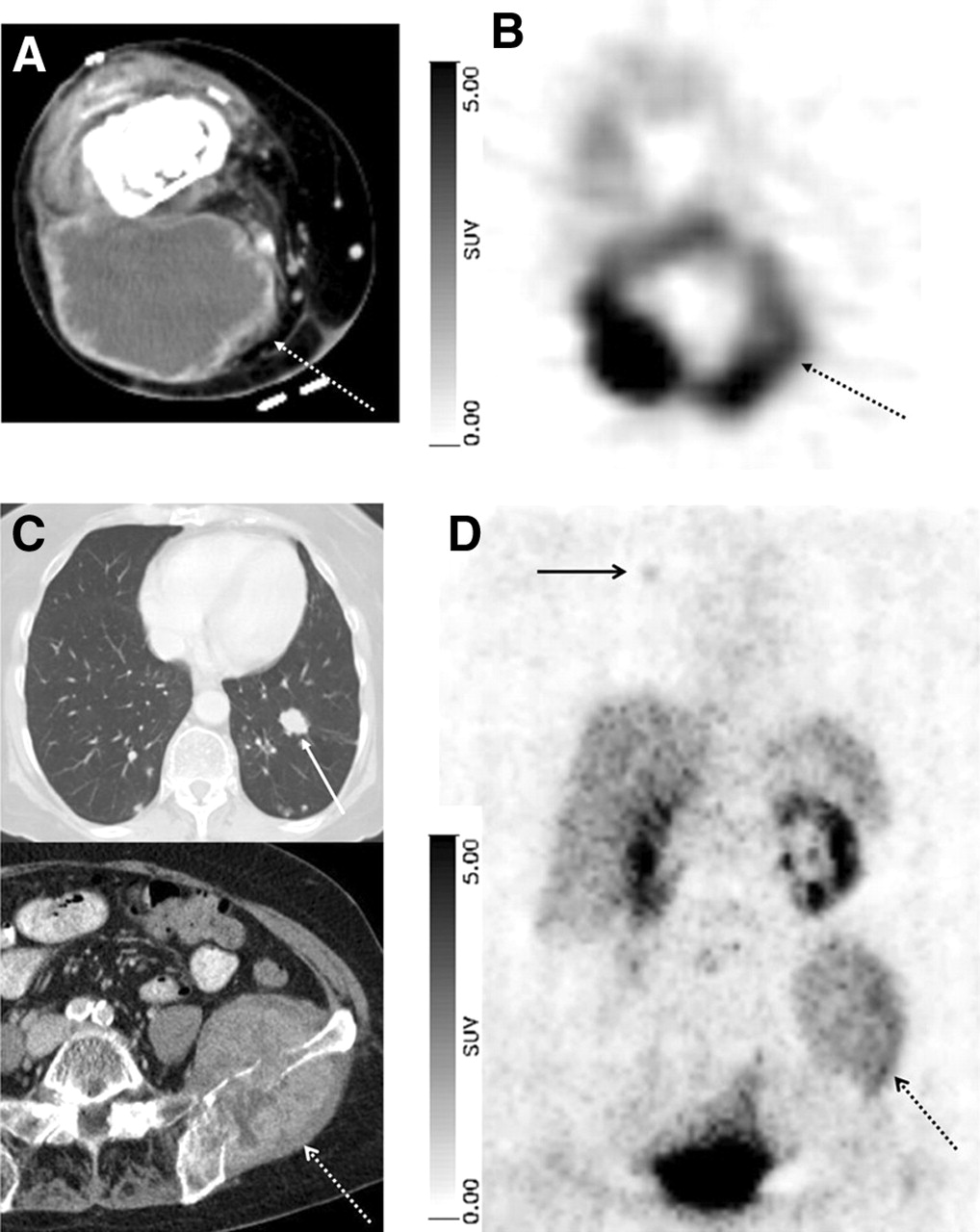
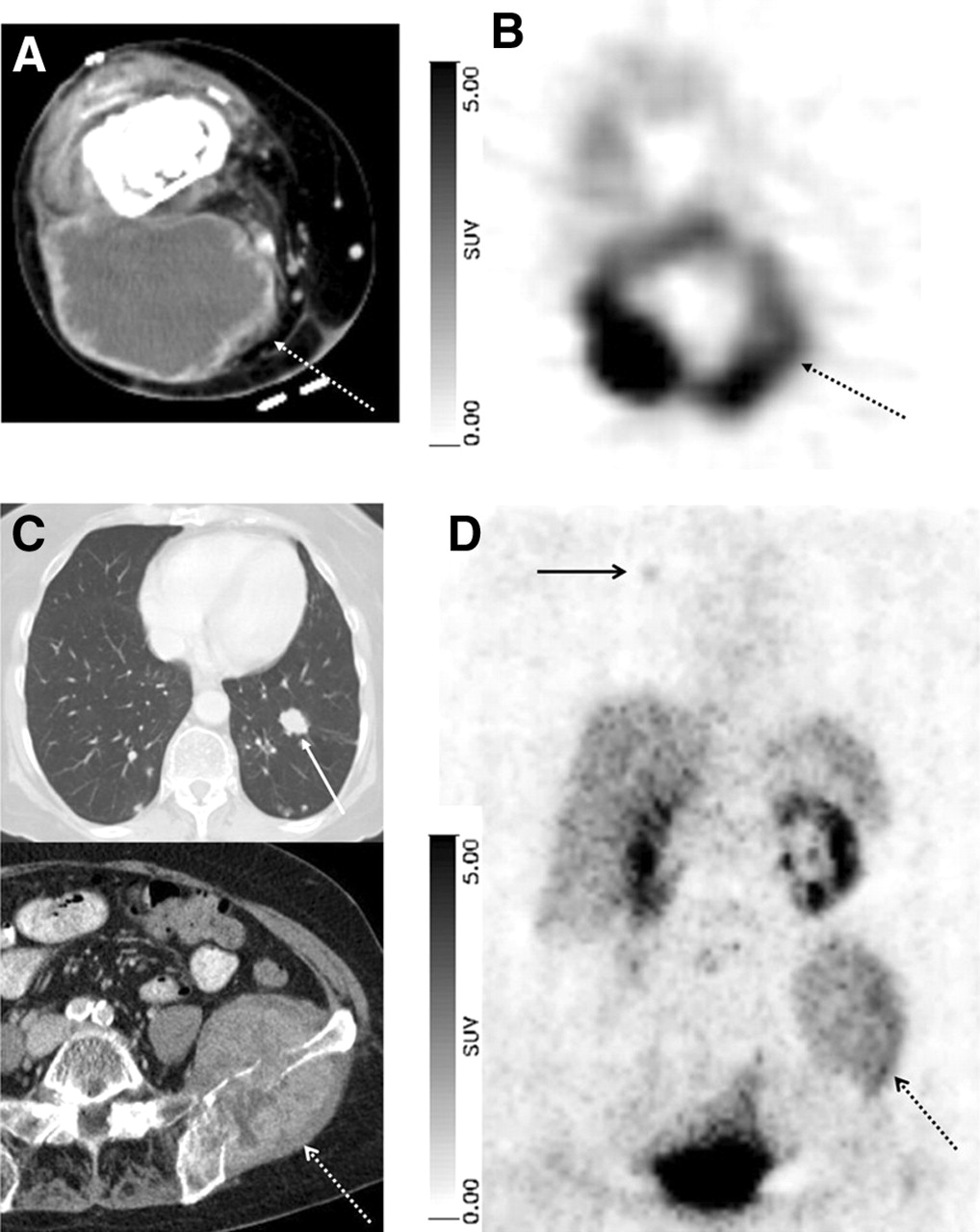
A 75-y-old female patient with soft-tissue sarcoma of distal right upper thigh and multiple metastases to bone and lungs. Primary tumor (arrow with dotted line) shows central necrosis and peripheral contrast enhancement in CT scan (A; transverse plane). 18F-Galacto-RGD scan (B; transverse plane, 120 min after injection) shows intense peripheral tracer uptake (SUV, 10.0). A large osseous metastases in left iliac bone (arrow with open arrow tip and dotted line) shows only moderate tracer uptake (D; 90 min after injection; SUV, 2.7). Metastasis in left lower lobe of lung (arrow with closed arrow tip) shows no tracer uptake, whereas another metastasis in right upper lobe (arrow with open arrow tip) shows faint tracer uptake (SUV, 1.3). Corresponding contrast-enhanced CT scans at level of iliac bone and lower lobes of lungs are shown (C, transverse plane).

18F-Galacto-RGD scans of 2 patients with metastases from malignant melanoma and different tracer uptake. (Upper row images) An 89-y-old female patient with metastasis in subcutaneous fat in gluteal area on left side (arrow with dotted line). Tumor can be clearly delineated in CT scan (A), whereas it shows no significant uptake in 18F-Galacto-RGD PET scan (B; 60 min after injection). (Lower row images) A 36-y-old female patient with lymph node metastasis in right groin (arrow). Again, tumor is clearly visualized in CT scan (C) but also shows intense tracer uptake in 18F-Galacto-RGD PET scan (D; 89 min after injection; SUV, 6.8).
The kinetic modeling approach using the 2-TC model for tumors and the 1-TC model for muscle resulted in good parameter precision (CoV values) and good model fits to the data. Values for DVtot were substantially higher in tumors and tumor maximum than in muscle, indicating increased free and bound tracer in tumor tissues compared with muscle. The good fit of the 2-TC model and the ratios of k3/k4 for tumors are indicative of specific and slowly reversible receptor binding of 18F-Galacto-RGD. These results confirm previously reported data on the properties of 18F-Galacto-RGD and RGD peptides in general and their binding kinetics to the αvβ3 receptor (34). We showed that pretreatment with increasing concentrations of unlabeled αvβ3 antagonists before administration of 18F-Galacto-RGD causes a concentration-dependent decrease of tracer accumulation in αvβ3-positive tumors (10) and found an increasing tracer uptake with increasing αvβ3 expression in a murine tumor model, which strongly supports 18F-Galacto-RGD binding specifically to αvβ3 (12). There are also reports indicating substantial internalization of labeled RGD peptides in vitro (35). However, the ability to estimate k4 with good precision suggests that 18F-Galacto-RGD is not irreversibly trapped inside the cells. However, because of several limitations of our modeling approach, these results have to be interpreted with care: First, only image-based arterial input functions were used; second, the first time frames of the dynamic studies were acquired for 30 s to achieve acceptable counting statistics. These factors probably lead to an underestimation of the peak plasma activity and consequently an overestimation of K1 in our model. However, calculations with a lower estimated K1 of 0.1, based on data obtained in solid tumors (19), resulted in similar DVtot values compared with the K1 derived from our modeling data. Moreover, recent studies on the kinetics of 18F-FDG in tumors using image-based arterial input functions showed good model fits and revealed similar K1 values compared with our results (36,37).
This new tracer offers a variety of possible applications. Recent data on 18F-Galacto-RGD in a murine model of a delayed-type hypersensitivity reaction suggest that it is possible to assess αvβ3 expression in inflammatory processes. The authors conclude that 18F-Galacto-RGD might be used to distinguish between acute and chronic phases of T-cell–mediated immune response and to assess disease activity in autoimmune disorders (38). However, the fact that αvβ3 is also expressed on newly formed blood vessels in inflammatory processes poses some problems in the context of malignant diseases: First, the distinction between malignancies and inflammations might be impaired. Preliminary results in patients with pigmented villonodular synovitis suggest that the uptake of 18F-Galacto-RGD in inflammatory lesions can be intense and similar to the uptake observed in malignancies (12). This might be a shortcoming of 18F-Galacto-RGD, similar to 18F-FDG, which can show high uptake in inflammatory cells (39).
Another potential clinical application would be to document αvβ3 expression of tumors before αvβ3-directed therapies. This is of paramount importance for a correct interpretation of the results of clinical trials with corresponding αvβ3 antagonists, in which a substantial proportion of the patients’ lesions might not be αvβ3 positive at all. No benefit can be expected in αvβ3-negative lesions and the results of a trial concerning the effectiveness of αvβ3 antagonists would be false-negative. This is also illustrated by the results of our study, which showed large inter- and intraindividual variances of 18F-Galacto-RGD accumulation. Furthermore, 18F-Galacto-RGD might be used to assess the inhibition of the αvβ3 integrin, indicating whether the dose of αvβ3 antagonists might be optimized. Finally, αvβ3 expression has been reported to be an important factor in determining the invasiveness and malignant potential of tumors such as breast and colon cancer (40,41). Therefore, noninvasive quantification of αvβ3 expression may provide a unique method of characterizing the biologic aggressiveness of a malignant tumor in an individual patient without the need for collecting tissue samples.
CONCLUSION
18F-Galacto-RGD is a tracer with highly desirable pharmacokinetic properties. The kinetic studies suggest specific binding of the tracer, which allows for noninvasive quantification of αvβ3 expression. Imaging of αvβ3 expression is possible with good contrast in most regions of the body except for the urogenital tract and, to a lesser extent, the spleen and liver. We recommend imaging ∼60 min after injection of the tracer for optimal lesion-to-background contrast. By using furosemide to enhance diuresis, image quality adjacent to the bladder could be further improved.
Acknowledgments
We thank Wolfgang Linke, Janette Carlsen, and the RDS-Cyclotron and PET team—especially Michael Herz, Gitti Dzewas, Coletta Kruschke, and Nicola Henke—for excellent technical assistance and the Münchner Medizinische Wochenschrift and the Sander-Foundation for financial support.
Footnotes
Received Feb. 10, 2005; revision accepted Apr. 19, 2005.
For correspondence contact: Ambros J. Beer, MD, Department of Nuclear Medicine, Technische Universität München, Klinikum rechts der Isar, Ismaninger Strasse 22, 81675 Munich, Germany.
E-mail: beer{at}roe.med.tum.de
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-Alfatide II PET/CT for Identification of Breast Cancer: A Preliminary Clinical Study
- PET Imaging of Very Late Antigen-4 in Melanoma: Comparison of 68Ga- and 64Cu-Labeled NODAGA and CB-TE1A1P-LLP2A Conjugates
- Imaging Integrin {alpha}v{beta}3 on Blood Vessels with 111In-RGD2 in Head and Neck Tumor Xenografts
- PET/CT Imaging of Integrin {alpha}v{beta}3 Expression in Human Carotid Atherosclerosis
- Interrogating Tumor Metabolism and Tumor Microenvironments Using Molecular Positron Emission Tomography Imaging. Theranostic Approaches to Improve Therapeutics
- Iodine quantification with dual-energy CT: phantom study and preliminary experience with VX2 residual tumour in rabbits after radiofrequency ablation
- 99mTc-3PRGD2 for Integrin Receptor Imaging of Lung Cancer: A Multicenter Study
- Radiopeptide Imaging and Therapy in Europe
- Melanin-Targeted Preclinical PET Imaging of Melanoma Metastasis
- 11C-Methionine PET of Acute Myocardial Infarction
- Targeted In vivo Imaging of Integrin {alpha}v{beta}6 with an Improved Radiotracer and Its Relevance in a Pancreatic Tumor Model
- Evaluation of {alpha}v{beta}3 Integrin-Targeted Positron Emission Tomography Tracer 18F-Galacto-RGD for Imaging of Vascular Inflammation in Atherosclerotic Mice
- PET Monitoring of Therapy Response in Head and Neck Squamous Cell Carcinoma
- Derivation of a Compartmental Model for Quantifying 64Cu-DOTA-RGD Kinetics in Tumor-Bearing Mice
- The Biodistribution and Radiation Dosimetry of the Arg-Gly-Asp Peptide 18F-AH111585 in Healthy Volunteers
- Radionuclide Imaging: A Molecular Key to the Atherosclerotic Plaque
- Intratumoral Spatial Distribution of Hypoxia and Angiogenesis Assessed by 18F-FAZA and 125I-Gluco-RGD Autoradiography
- Correlative Imaging of Hypoxia and Angiogenesis in Oncology
- Patterns of {alpha}v{beta}3 Expression in Primary and Metastatic Human Breast Cancer as Shown by 18F-Galacto-RGD PET
- Comparison of Integrin {alpha}v 3 Expression and Glucose Metabolism in Primary and Metastatic Lesions in Cancer Patients: A PET Study Using 18F-Galacto-RGD and 18F-FDG
- [18F]Galacto-RGD Positron Emission Tomography for Imaging of {alpha}v{beta}3 Expression on the Neovasculature in Patients with Squamous Cell Carcinoma of the Head and Neck
- microPET of Tumor Integrin {alpha}v{beta}3 Expression Using 18F-Labeled PEGylated Tetrameric RGD Peptide (18F-FPRGD4)
- 64Cu-Labeled Tetrameric and Octameric RGD Peptides for Small-Animal PET of Tumor {alpha}v{beta}3 Integrin Expression
- Small-Animal PET of Tumor Angiogenesis Using a 76Br-Labeled Human Recombinant Antibody Fragment to the ED-B Domain of Fibronectin
- Nuclear Imaging Probes: from Bench to Bedside
- In vitro and In vivo Characterization of 64Cu-Labeled AbegrinTM, a Humanized Monoclonal Antibody against Integrin {alpha}v{beta}3
- 18F-FDG PET After Radiofrequency Ablation: Is Timing Everything?
- Positron Emission Tomography As an Imaging Biomarker
- Positron Emission Tomography Using [18F]Galacto-RGD Identifies the Level of Integrin {alpha}v{beta}3 Expression in Man.
- A Thiol-Reactive 18F-Labeling Agent, N-[2-(4-18F-Fluorobenzamido)Ethyl]Maleimide, and Synthesis of RGD Peptide-Based Tracer for PET Imaging of {alpha}v{beta}3 Integrin Expression
- PET-Based Human Dosimetry of 18F-Galacto-RGD, a New Radiotracer for Imaging {alpha}v{beta}3 Expression
- Combined Molecular Targeting for Cancer Therapy: A New Paradigm in Need of Molecular Imaging
- Experience of PET for target localisation in radiation oncology