


Abstract
18F-Galacto-RGD is a new tracer for PET imaging of αvβ3, a receptor involved in a variety of pathologic processes including angiogenesis and metastasis. Our aim was to study the dosimetry of 18F-galacto-RGD in humans. Methods: Eighteen patients with various tumors (musculoskeletal tumors [n = 10], melanoma [n = 5], breast cancer [n = 2], or head and neck cancer [n = 1]) were examined. After injection of 133–200 MBq of 18F-galacto-RGD, 3 consecutive emission scans from the thorax to the pelvis were acquired at 6.7 ± 2.9, 35.6 ± 7.6, and 70.4 ± 12.2 min after injection. Blood samples (n = 4) for metabolite analysis were taken 10, 30, and 120 min after injection. The OLINDA 1.0 program was used to estimate the absorbed radiation dose. Results: Reversed-phase high-performance liquid chromatography of serum revealed that more than 95% of tracer was intact up to 120 min after injection. 18F-Galacto-RGD showed rapid clearance from the blood pool and primarily renal excretion. Background activity in lung and muscle tissue was low (percentage injected dose per liter at 71 min after injection, 0.56 ± 0.15 and 0.69 ± 0.25, respectively). The calculated effective dose was 18.7 ± 2.4 μSv/MBq, and the highest absorbed radiation dose was in the bladder wall (0.22 ± 0.03 mGy/MBq). Conclusion: 18F-Galacto-RGD demonstrates high metabolic stability, a favorable biodistribution, and a low radiation dose. Consequently, this tracer can safely be used for noninvasive imaging of molecular processes involving the αvβ3 integrin and for the planning and monitoring of therapeutic approaches targeting αvβ3.
The integrin αvβ3 is an important receptor affecting tumor growth, local invasiveness, and metastatic potential (1,2). Integrins are dimeric transmembrane glycoproteins mediating adhesion and migration of cells on a variety of extracellular matrix proteins. Specifically, αvβ3 is highly expressed on activated endothelial cells during angiogenesis (3). The use of αvβ3 antagonists is currently being evaluated as a strategy for anticancer therapies (4). Therefore, noninvasive determination of αvβ3 expression would be of great importance for pretherapeutic recognition of those patients most amenable to αvβ3-directed therapies and for the assessment of receptor expression during therapy.
Because many integrins, including αvβ3, bind to the tripeptide sequence arginine-glycine-aspartic acid (single letter code RGD) of different matrix proteins (5), several radiolabeled RGD peptides have been developed for SPECT and PET (6–8). The glycosylated cyclic pentapeptide 18F-galacto-RGD resulted from tracer optimization based on the first-generation peptide [125I]-3-iodo-dTyr4-cyclo(-Arg-Gly-Asp-dTyr-Val) (9). A murine αvβ3-positive tumor model has already shown that 18F-galacto-RGD has receptor-specific accumulation, high metabolic stability, predominantly renal elimination, and a high affinity and selectivity for the αvβ3 integrin in vitro (10). Radiation dose estimates from dynamic PET studies on New Zealand White rabbits suggested that the effective dose should be in the range of an 18F-FDG PET scan (11). The present study was performed to estimate the associated radiation dose and to characterize the biodistribution and metabolic stability of 18F-galacto-RGD in humans.
MATERIALS AND METHODS
Radiopharmaceutical Preparation
Synthesis of the labeling precursor and subsequent 18F labeling were performed as described elsewhere (10,11).
Analysis of Metabolites in Blood Samples
Blood samples were collected 10, 30, and 120 min after tracer injection. Samples were centrifuged at 2,000 rotations per minute, and the supernatant was passed through a Sep-Pak C-18 cartridge (Waters). The cartridge was washed with 1 mL of phosphate-buffered saline and was eluted with 1 mL of acetonitrile that included 0.1% trifluoroacetic acid. The solvent was removed in vacuo, and 0.5 mL of phosphate-buffered saline was added before analysis using reversed-phase high-performance liquid chromatography (10%−50% acetonitrile and 0.1% trifluoroacetic acid; 20 min at a flow rate of 3 mL/min).
Patients
The study was approved by the ethics committee of the Technische Universität München and the local radiation protection authorities. Informed written consent was obtained from all patients. Eighteen patients (11 women and 7 men; mean age ± SD, 50.8 ± 17.8 y; range, 31–89 y), with diseases of the musculoskeletal system (n = 10), melanoma (n = 5), breast cancer (n = 2), or head and neck cancer (n = 1), were included in the study from September 2003 until April 2005 (Table 1). Diagnosis was confirmed by histopathology in 17 cases. In 1 case of metastasized melanoma, the diagnosis was based on clinical and imaging findings (contrast-enhanced CT of the thorax, abdomen, and pelvis and 18F-FDG PET). In all patients with lesions of the musculoskeletal system, MRI of the tumor region was performed. For patients with melanoma, 18F-FDG PET was performed in 4 cases and contrast-enhanced CT in 3 cases. All patients with breast cancer underwent mammography and breast ultrasound, and 1 patient underwent MRI mammography as well. In the patient with head and neck cancer, MRI and contrast-enhanced CT of the head and neck were performed. Inclusion criteria consisted of known or suspected malignancy, age over 18 y, and the ability to give written and informed consent. Exclusion criteria consisted of pregnancy, lactation, and impaired renal function (serum creatinine level > 1.2 mg/dL).
Patient Data
PET Procedure
Imaging was performed with an ECAT EXACT PET scanner (CTI/Siemens). The patients urinated before the examination and did not urinate between scans. Before injection of 18F-galacto-RGD (133–200 MBq), a segmented transmission scan was acquired for 5 min per bed position (5 bed positions) using 3 rotating 68Ge rod sources (each with approximately 90 MBq of 68Ge) followed by 3 consecutive static emission scans in 2-dimensional mode beginning 5 min after tracer injection and covering the thorax to the pelvis (5−7 bed positions, 5 min per bed position). The field of view was 15.5 cm with overlapping acquisitions, resulting in a length of 13.6 cm for each bed position. The mean starting times for these emissions scans were 6.7 ± 2.9, 35.6 ± 7.6, and 70.4 ± 12.2 min after injection. Scanning was performed in the caudocranial direction.
Image Analysis and Dosimetry
Positron emission data were reconstructed using the ordered-subsets expectation maximization algorithm. Reconstructions were performed with 8 iterations and 4 subsets. The images were corrected for attenuation using the transmission data collected over the same region as for emission imaging. For image analysis, CAPP software, version 7.1 (CTI/Siemens), was used. Images were calibrated to Bq/mL for radiation dosimetry estimates.
An experienced operator placed regions of interest (ROIs) over major organs (lung, left ventricle, liver, spleen, intestine, kidneys, bladder, muscle, and breast) on 3 adjacent slices of the static emission scans. Because no substantial tracer accumulation was noted in the red bone marrow, no ROI could be drawn. The diameter of the ROIs was set to 2.5 cm, except for the kidney and intestine ROIs. There, polygonal ROIs adapted to the contour of the kidney or covering the area of maximum intestinal activity were drawn. For liver, spleen, and kidneys, we deliberately did not draw ROIs adapted to organ contours; doing so might have underestimated organ activity because of partial-volume effects. These effects can be avoided by placing an ROI of sufficient diameter in the center of the organ. Because of the limited number of time points at which measurements were obtained, a monoexponential fit was used for calculation of organ residence times (12,13).
For dosimetry calculations, the OLINDA 1.0 software (Vanderbilt University (14)) was used. Activity in the source organs was determined by multiplying the measured concentration (Bq/mL) by the organ masses of the OLINDA adult phantom. This activity was expressed as percentage injected dose and plotted against time. Thus, the dose factors given here are dose factors for the reference man or woman, allowing easy comparison of our results with those of other dosimetric studies using this approach (15–17). Moreover, only about 5% of body weight is amenable to volumetry by using, for example, CT or PET datasets (liver, spleen, kidneys). For the patient with the highest body weight (patient 13), we compared dosimetry results obtained using, on the one hand, organ weights from the OLINDA adult phantom with those obtained using, on the other hand, organ weights from individual volumetry based on CT datasets (liver, spleen, kidneys). The effective dose was determined to be 16.8 μSv/MBq using the individual organ masses and 17.0 μSv/MBq using the organ masses from the adult phantom—a difference of only 1.2%. However, this example is just illustrative and the results cannot be generalized.
Bladder activity was determined as follows. Activity concentration was determined from 3 adjacent ROIs at least 2.5 cm in diameter drawn inside the bladder. Subsequently, the bladder volume was measured by drawing freehand ROIs around the bladder contour, with the images scaled to the maximum activity in the bladder. The volume was then calculated by the CAPP software. The mean bladder volume for the last emission scan at 70.4 min after injection was 491 ± 286 mL. Averaged data were fitted to an exponential rise to maximum, from which the total fraction of activity entering the bladder was derived. The total percentage of activity entering the bladder based on these results was estimated to be 71.2% (±31.5%). The biologic half-life was determined from whole-body effective half-life using various voiding intervals (120, 60, and 30 min). Both values were entered in the dynamic bladder model of the OLINDA 1.0 program to determine the bladder-content residence time.
The gastrointestinal tract model of the OLINDA software was used to estimate hepatobiliary tracer elimination. The fraction of activity entering the intestine was determined by multiplying the measured small-intestine activity concentration by the standard mass of the small intestine. For calculation of total-body half-life, the total-body activity of each emission scan was determined by using the open-source software AMIDE 0.8, and the bladder activity was subtracted (18). A monoexponential fit was then applied to calculate the residence time for the total body. The residence time for the remainder of the body was calculated by subtracting organ and bladder residence times from the whole-body residence time.
RESULTS
Analysis of metabolites in blood samples (n = 4) using reversed-phase high-performance liquid chromatography showed that more than 95% of the tracer was intact at 120 min after injection.
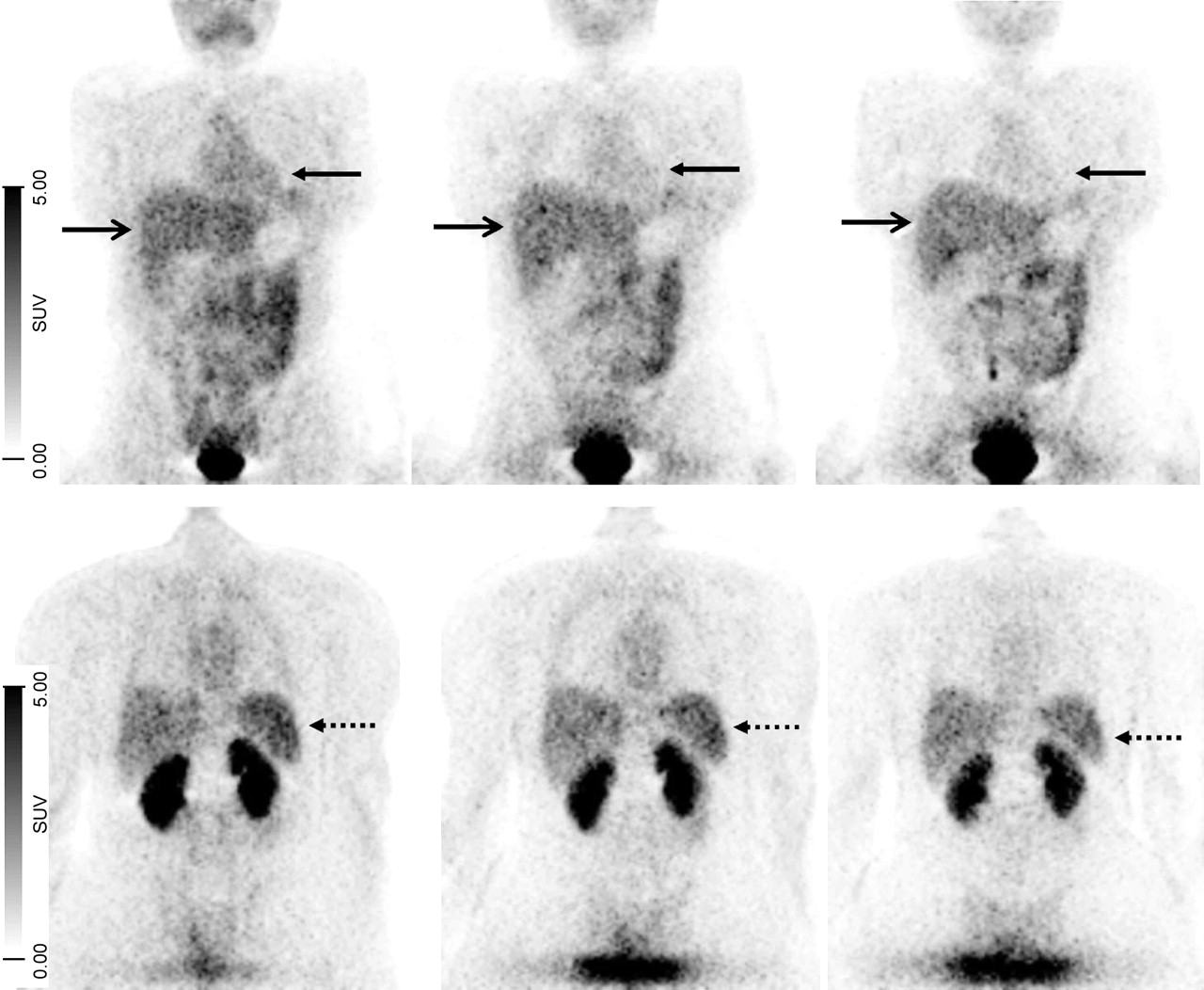
Table 2 lists the average absorbed radiation dose for all organs using the individual organ residence times. Average residence times are listed in Table 3. The maximum residence time for 18F is 2.64 h, and the sum of the mean residence times is 1.15 h. The difference accounts for activity excreted via the kidneys during a voiding interval of 2 h. The effective total-body half-life was 46 ± 12 min. For the 2-h voiding interval, the effective absorbed radiation dose was 18.7 ± 2.4 μSv/MBq (17.1 ± 0.7 μSv/MBq for men and 20.2 ± 2.5 μSv/MBq for women), with the highest absorbed dose—0.22 ± 0.03 mGy/MBq—being in the bladder wall. Other organs with relatively high doses were the kidneys, liver, small intestine, and lungs. We also calculated the average absorbed radiation dose for a 1-h voiding interval and a 30-min voiding interval. For these intervals, the effective radiation doses were 12.7 ± 2.2 and 9.5 ± 1.7 μSv/MBq, respectively. Again, the highest absorbed doses were in the bladder wall (0.11 ± 0.02 and 0.06 ± 0.01 mGy/MBq, respectively). Figure 1 shows representative dynamic coronal images acquired at 5, 33, and 62 min after tracer injection.
Radiation Dose Estimates for Intravenous Administration of 18F-Galacto-RGD
Mean Organ Residence Times of All Patients
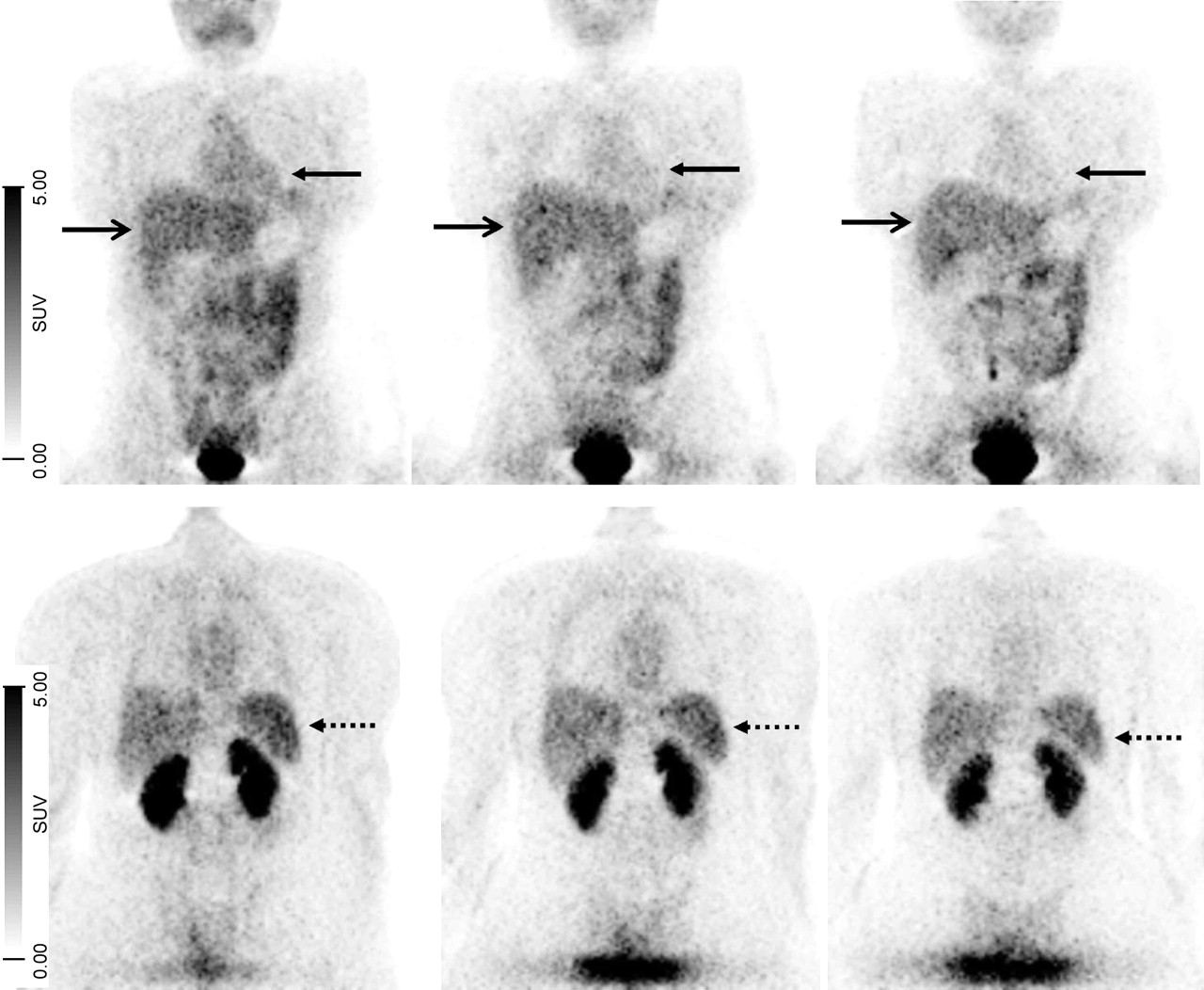
Static 18F-galacto-RGD emission scans of 37-y-old woman at (from left to right) 5, 33, and 62 min after injection, with representative coronal views at level of heart and liver (top) and at level of kidneys (bottom). Blood pool (heart, upper solid arrow) shows rapid elimination of tracer, liver (lower solid arrow) shows moderate activity slowly decreasing over time, and spleen (dashed arrow) shows initially high activity decreasing over time.
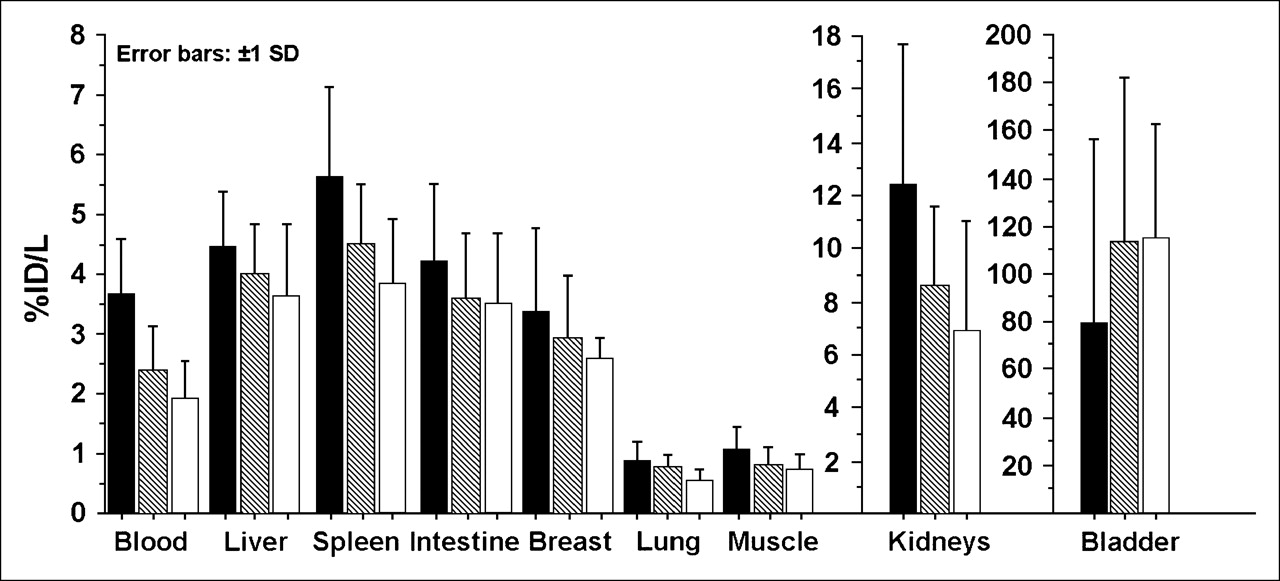
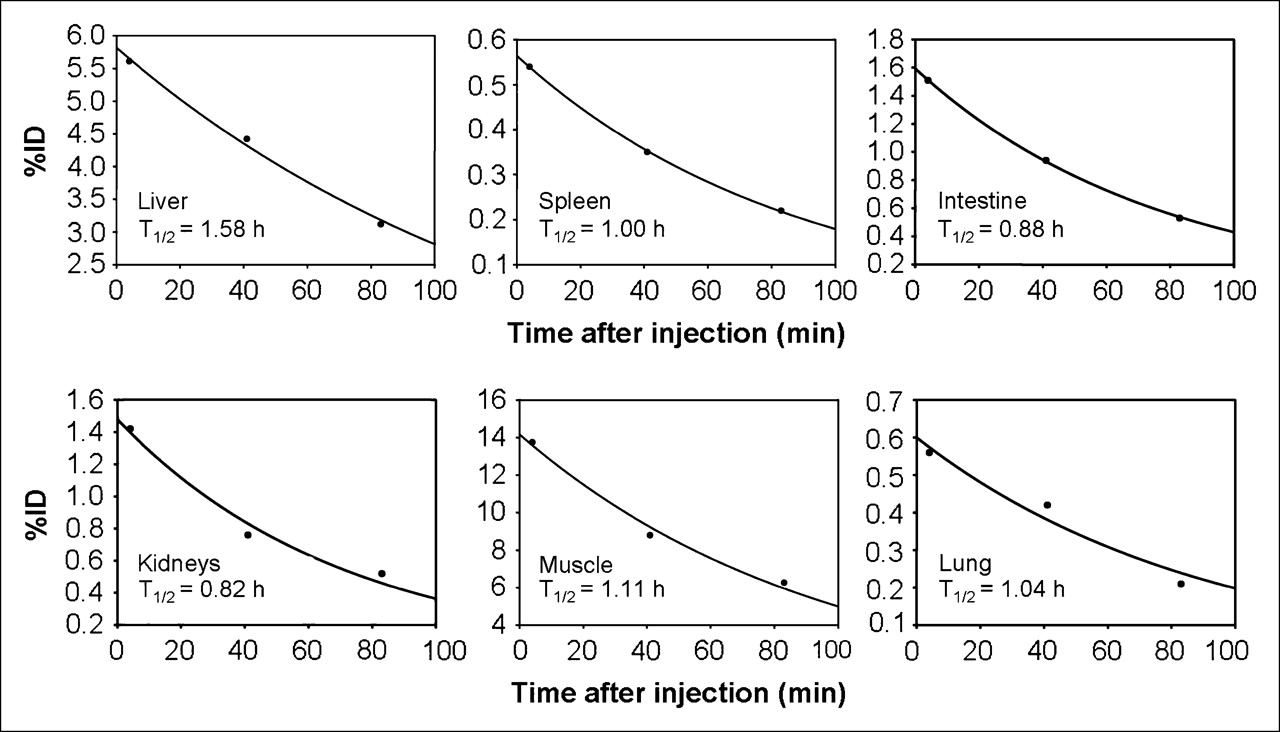
Figure 2 summarizes the percentage injected dose per liter for the various organs measured in the emission scans and averaged over all patients. The organ time–activity curves of a representative patient are shown in Figure 3. In general, the areas of highest activity were the urogenital tract (kidneys, ureter, and bladder), followed by the liver, spleen, and gut. Blood-pool activity was only moderate and declined over time. Background activity in the muscles and lungs was low. We observed no significant tracer accumulation in the gut during the examination period, and the fraction of activity entering the gastrointestinal tract was calculated to be 3.0% ± 1.7%. This finding confirms that the tracer was predominantly excreted via the renal pathway.
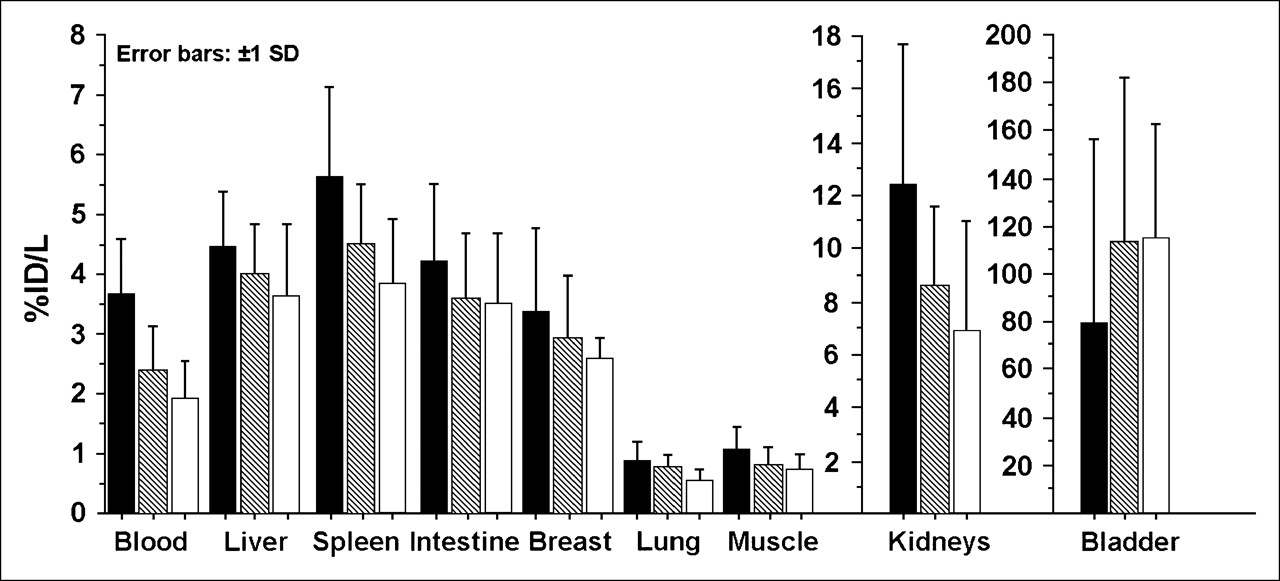
Mean percentage injected dose per liter, and SD, for major organs and muscle tissue determined on the basis of 3 static emission scans corrected for decay. Solid bar = 6 min after injection; hatched bar = 36 min after injection; open bar = 71 min after injection.
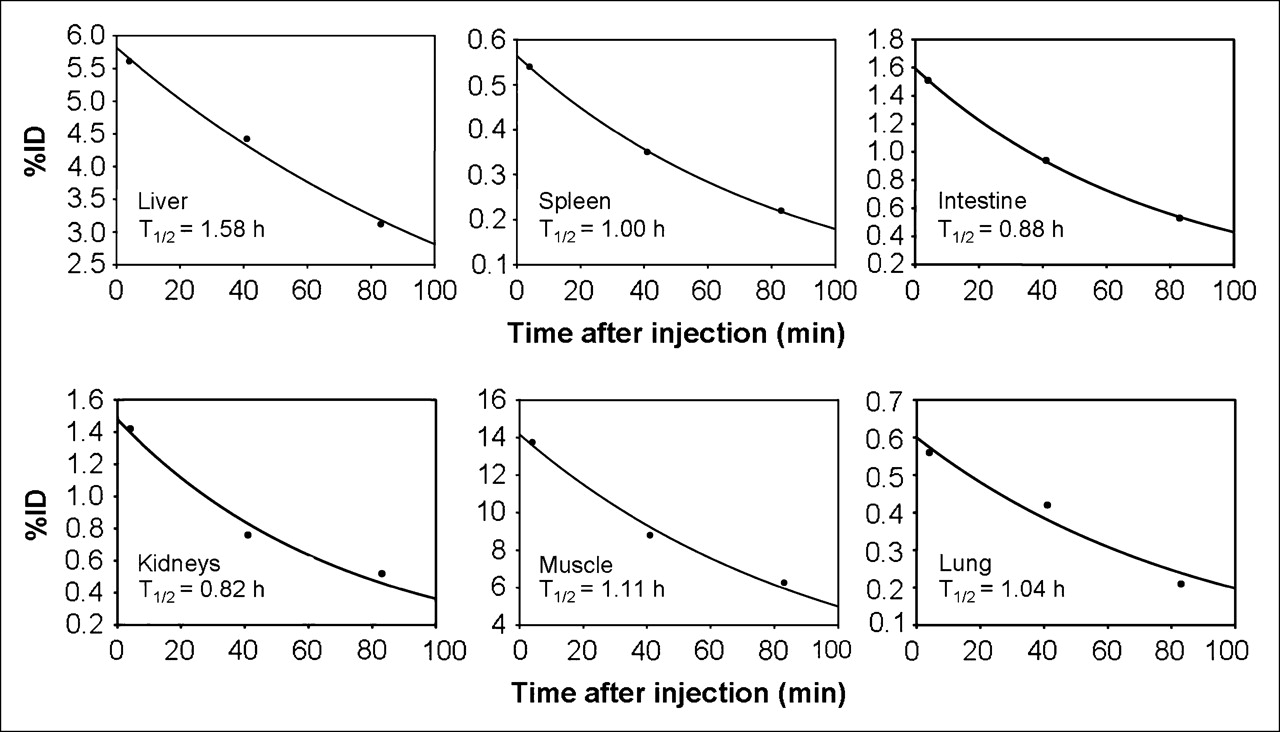
Organ time–activity curves and corresponding effective half-times for 18F-galacto-RGD in patient 3. Graphs indicate percentage of total injected activity in each organ vs. time after injection of 18F-galacto-RGD.
DISCUSSION
In this paper, we have described the dosimetry of the αvβ3-selective tracer 18F-galacto-RGD in humans. The radiation dose is similar to that of 18F-FDG. The tracer shows predominantly renal elimination and low background activity in most organs. These findings suggest that 18F-galacto-RGD can safely and effectively be used for imaging αvβ3 expression in humans.
The dosimetry calculations revealed the effective dose to be 18.7 μSv/MBq and the bladder to be the critical organ, receiving the highest absorbed radiation dose (218 μGy/MBq). Other organs receiving relatively high doses were the kidneys, spleen, liver, and small and large intestines. However, the dose to the intestine did not seem to be caused by hepatobiliary excretion, because the activity did not increase over time. Therefore, we suggest that there might be a specific uptake in the bowel wall, perhaps due to αvβ3 expression on intestinal smooth muscle cells (19). However, the absorbed dose for all these organs is considerably lower than that to the bladder wall (12–30 μGy/MBq). The radiation dose estimates from our study correspond well with the estimates from our animal study on New Zealand White rabbits and mice (11). The animal study also showed that renal elimination of the tracer was fast, that tracer was not retained in any investigated organs, and that activity was highest in the bladder, at 60 min after injection. The radiation dose estimated for an adult female patient from the results of the animal study with New Zealand White rabbits was 0.22 μSv/MBq and therefore similar to the results of our current study (0.20 μSv/MBq). In both the animal study and the human study, the bladder proved to be the critical organ. However, the estimated dose to the large intestine in the mouse model and, to a lesser extent, in the rabbit model was substantially higher than that found using our current data (mouse data, 0.082 mGy/MBq; rabbit data, 0.028 mGy/MBq; human data, 0.019 mGy/MBq). On the other hand, the estimated dose to the liver using mouse data and rabbit data was lower than that found using human data (mouse data, 0.010 mGy/MBq; rabbit data, 0.016 mGy/MBq; human data, 0.027 mGy/MBq). This result probably reflects slower excretion kinetics and higher tracer retention in the liver in larger animals and humans than in small animals.
The dose factors we calculated were those for the reference man or woman—a routine approach in dosimetric studies of new PET tracers (15–17). It was not our intention to calculate doses using the individual organ or body masses of our patients, because these values cannot be directly compared with published dose estimates for other compounds. Moreover, only about 5% of body weight is amenable to volumetry by using, for example, CT or PET datasets (liver, spleen, kidneys). However, if RGD peptides were to be used for radionuclide therapy, individual dosimetry based on the volumetry of individual organ masses would of course be essential. The total effective dose of 18F-galacto-RGD according to our results is in the range of commonly applied oncologic radiotracers, such as 18F-FDG (approximately 19.0 μSv/MBq) (20,21). Even with the maximum amount of tracer (200 MBq of 18F-galacto-RGD) injected in our study, a patient would be exposed to an effective dose of not more than 3.7 mSv. Using a higher—400-MBq—activity, similar to 18F-FDG PET, to improve image quality would result in an effective dose of 7.4 mSv, which still corresponds to risk category IIb as defined by the International Commission on Radiological Protection (minor to intermediate level of risk, appropriate for intermediate to moderate societal benefit) (22). Moreover, the absorbed dose could be reduced further by lowering the rather long voiding interval in our scenario from 2 to 1 h, assuming that for routine applications of 18F-galacto-RGD, only 1 static emission scan at 60 min after injection would be necessary. For this scenario, we calculated a lower effective dose of 12.7 μSv/MBq. Use of a diuretic agent such as furosemide could further decrease the absorbed dose of the bladder wall and probably would reduce the voiding interval to 30 min, resulting again in a markedly reduced effective dose compared with the 2-h voiding interval (effective dose, 9.5 μSv/MBq). Image quality in the pelvis adjacent to the bladder would probably also improve, because the concentration of tracer in the bladder should be markedly reduced. This protocol (application of furosemide, 1 static emission scan at 60 min after injection) would be similar to the protocol used for 18F-FDG PET in our institution, which is well tolerated by most of our patients. Moreover, bladder catheterization with continuous drainage could further reduce the radiation burden to the urinary tract.
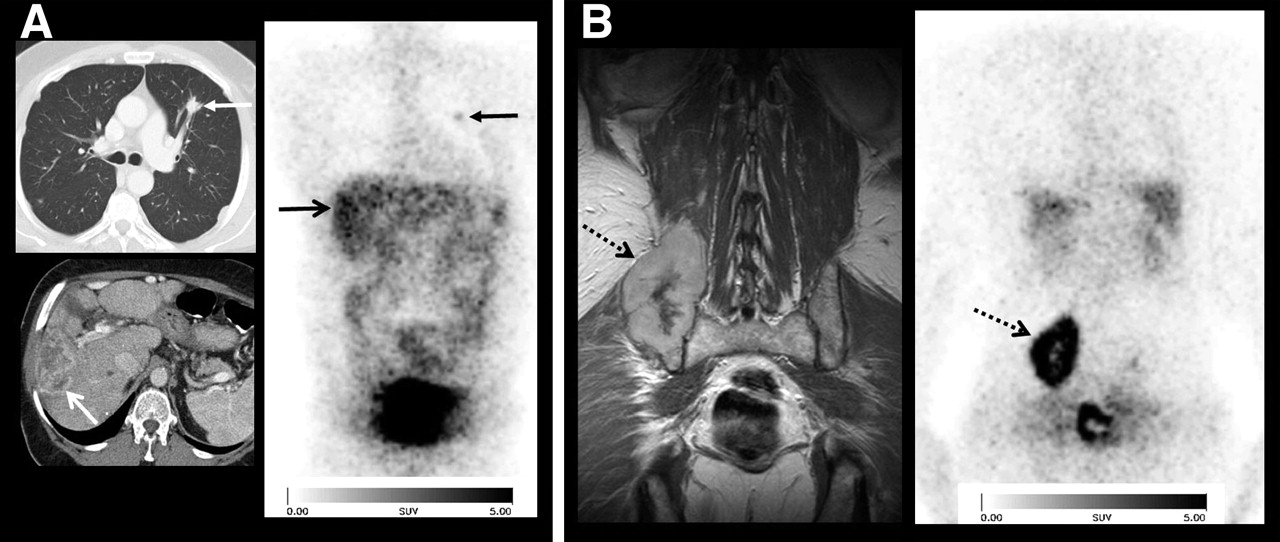
The biodistribution data for 18F-galacto-RGD showed that the primary route of clearance is renal, with high tracer accumulation in the kidneys and especially in the bladder. Because of the high activity in the urine, image quality adjacent to the urinary tract and bladder was slightly impaired. The background activity in muscle tissue and the blood pool was low and decreased further over time. On the basis of these biodistribution patterns, imaging of αvβ3 expression with 18F-galacto-RGD is possible in the thorax, abdomen, and extremities, except for the urogenital tract. In the liver, spleen, and intestine, detection of lesions with only moderate tracer uptake might be impaired because of the higher background activity in these organs. Image quality in the pelvis might also be impaired by artifacts due to the high bladder activity (Fig. 4).

65-y-old man with hepatocellular carcinoma metastatic to lung and iliac bone. (A) Images of primary tumor (upper arrows) and of lung metastasis (lower arrows) include 18F-galacto-RGD scan obtained 76 min after injection (right) and CT scans at levels of lungs (top left) and liver (bottom left). (B) Images of large osseous metastasis (arrows) in right iliac bone include 18F-galacto-RGD scan obtained 76 min after injection (right) and T1-weighted coronal MRI scan obtained with intravenous gadolinium-diethylenetriaminepentaacetic acid (left). Hepatocellular carcinoma is barely visible because of low lesion-to-background contrast in liver, whereas lesions in lung and bone are well demarcated. Hepatocellular carcinoma shows only intermediate tracer uptake (standardized uptake value, 2.9), compared with osseous lesion (standardized uptake value, 6.2), indicating lower αvβ3 expression in primary tumor than in metastasis.
The integrin αvβ3 plays a critical role in regulating tumor growth and angiogenesis and is significantly upregulated in sprouting tumor vessels and the cells of various tumors (23,24). Therefore, the noninvasive visualization and quantification of αvβ3-integrin levels in patients would allow a variety of possible applications. One potential application would be to document the αvβ3 expression of tumors before therapy with αvβ3 antagonists. Initial results from our patient study showed large inter- and intraindividual variances of 18F-galacto-RGD accumulation in cancer patients (25,26). Patients with low or lack of αvβ3 expression may not benefit from αvβ3 antagonists and could receive an alternative therapeutic regimen. In patients with αvβ3-positive lesions, 18F-galacto-RGD might be used to assess inhibition of the αvβ3 integrin to optimize the dose of αvβ3 antagonists. αvβ3 expression has also been reported to be an important prognostic factor in tumors such as breast and colon cancer (27,28). Therefore, 18F-galacto-RGD might be used to noninvasively characterize the biologic aggressiveness of a malignant tumor in an individual patient. Moreover, the noninvasive determination of αvβ3 expression might be used as a surrogate parameter of angiogenesis in tumors that express this integrin only on endothelial cells and not on tumor cells. Recent data also suggest that it is possible to assess αvβ3 expression in inflammatory processes using 18F-galacto-RGD (29).
There are potential limitations to our study. Because our study, like many other dosimetric studies of new tracers, investigated patients rather than healthy volunteers, data from only 3 time points were used for calculation of residence times. More than 90 min without voiding would not have been tolerated by most of our patients unless the bladder had been catheterized. Also, no dynamic scans were obtained in this study, because we favored static emission scans of diagnostic quality with longer scans at each time point, consequently reducing the temporal resolution. Moreover, we cannot exclude the possibility that some tracer elimination to the bowel might have become notable because of the longer measurement periods. However, the advantage of a patient study is that the population under investigation is more representative of the future patient collective that would be investigated with 18F-galacto-RGD.
CONCLUSION
18F-Galacto-RGD demonstrates a radiation dose comparable to that of 18F-FDG and therefore can safely be used for imaging αvβ3 expression. Because of the predominantly renal excretion of 18F-galacto-RGD, the effective dose could be further reduced by applying diuretic agents and by reducing the voiding interval.
Acknowledgments
We thank Wolfgang Linke, Janette Carlsen, and the RDS-Cyclotron and PET team, especially Michael Herz, Petra Watzlowick, Gitti Dzewas, Coletta Kruschke, and Nikola Henke. The Münchner Medizinische Wochenzeitschrift and the Sander Foundation (grant 96.017.3) are acknowledged for financial support.
References
- Received for publication December 19, 2005.
- Accepted for publication January 24, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-Alfatide II PET/CT for Identification of Breast Cancer: A Preliminary Clinical Study
- PET-Based Human Dosimetry of the Dimeric {alpha}v{beta}3 Integrin Ligand 68Ga-DOTA-E-[c(RGDfK)]2, a Potential Tracer for Imaging Tumor Angiogenesis
- 68Ga-NOTA-PRGD2 PET/CT for Integrin Imaging in Patients with Lung Cancer
- Role of Positron Emission Tomography for the Monitoring of Response to Therapy in Breast Cancer
- Biodistribution and Radiation Dosimetry of the Integrin Marker 18F-RGD-K5 Determined from Whole-Body PET/CT in Monkeys and Humans
- 18F-ML-10, a PET Tracer for Apoptosis: First Human Study
- Monitoring Tumor Response to Antiangiogenic Sunitinib Therapy with 18F-Fluciclatide, an 18F-Labeled αV{beta}3-Integrin and αV{beta}5-Integrin Imaging Agent
- 2-18F-Fluoropropionic Acid as a PET Imaging Agent for Prostate Cancer
- Radiopharmaceuticals in Preclinical and Clinical Development for Monitoring of Therapy with PET
- PET-Based Biodistribution and Radiation Dosimetry of Epidermal Growth Factor Receptor-Selective Tracer 11C-PD153035 in Humans
- Gene expression profiling-based identification of cell-surface targets for developing multimeric ligands in pancreatic cancer
- Phase I Trial of the Positron-Emitting Arg-Gly-Asp (RGD) Peptide Radioligand 18F-AH111585 in Breast Cancer Patients
- Advances in Anatomic, Functional, and Molecular Imaging of Angiogenesis
- Patterns of {alpha}v{beta}3 Expression in Primary and Metastatic Human Breast Cancer as Shown by 18F-Galacto-RGD PET
- Application of PET/CT in the Development of Novel Anticancer Drugs
- Comparison of Integrin {alpha}v 3 Expression and Glucose Metabolism in Primary and Metastatic Lesions in Cancer Patients: A PET Study Using 18F-Galacto-RGD and 18F-FDG
- [18F]Galacto-RGD Positron Emission Tomography for Imaging of {alpha}v{beta}3 Expression on the Neovasculature in Patients with Squamous Cell Carcinoma of the Head and Neck
- microPET of Tumor Integrin {alpha}v{beta}3 Expression Using 18F-Labeled PEGylated Tetrameric RGD Peptide (18F-FPRGD4)
- Nuclear Imaging Probes: from Bench to Bedside
- Future Issues in Highly Conformal Radiotherapy for Head and Neck Cancer