


Abstract
2-((2S,5R,8S,11S)-5-benzyl-8-(4-((2S,3R,4R,5R,6S)-6-((2-(4-(3-18F-fluoropropyl)-1H-1,2,3-triazol-1-yl)acetamido)methyl)-3,4,5-trihydroxytetrahydro-2H-pyran-2-carboxamido)butyl)-11-(3-guanidinopropyl)-3,6,9,12,15-pentaoxo-1,4,7,10,13-pentaazacyclopentadecan-2-yl)acetic acid (18F-RGD-K5) has been developed as an αvβ3 integrin marker for PET. The purpose of this study was to determine the biodistribution and estimate the radiation dose from 18F-RGD-K5 using whole-body PET/CT scans in monkeys and humans. Methods: Successive whole-body PET/CT scans were obtained after intravenous injection of 18F-RGD-K5 in 3 rhesus monkeys (167 ± 19 MBq) and 4 healthy humans (583 ± 78 MBq). In humans, blood samples were collected between the PET/CT scans, and stability of 18F-RGD-K5 was assessed. Urine was also collected between the scans, to determine the total activity excreted in urine. The PET scans were analyzed to determine the radiotracer uptake in different organs. OLINDA/EXM software was used to calculate human radiation doses based on human and monkey biodistributions. Results: 18F-RGD-K5 was metabolically stable in human blood up to 90 min after injection, and it cleared rapidly from the blood pool, with a 12-min half-time. For both monkeys and humans, increased 18F-RGD-K5 uptake was observed in the kidneys, bladder, liver, and gallbladder, with mean standardized uptake values at 1 h after injection for humans being approximately 20, 50, 4, and 10, respectively. For human biodistribution data, the calculated effective dose was 31 ± 1 μSv/MBq, and the urinary bladder wall had the highest absorbed dose at 376 ± 19 μGy/MBq using the 4.8-h bladder-voiding model. With the 1-h voiding model, these doses reduced to 15 ± 1 μSv/MBq for the effective dose and 103 ± 4 μGy/MBq for the absorbed dose in the urinary bladder wall. For a typical injected activity of 555 MBq, the effective dose would be 17.2 ± 0.6 mSv for the 4.8-h model, reducing to 8.3 ± 0.4 mSv for the 1-h model. For monkey biodistribution data, the effective dose to humans would be 22.2 ± 2.4 mSv for the 4.8-h model and 12.8 ± 0.2 mSv for the 1-h model. Conclusion: The biodistribution profile of 18F-RGD-K5 in monkeys and humans was similar, with increased uptake in the bladder, liver, and kidneys. There was rapid clearance of 18F-RGD-K5 through the renal system. The urinary bladder wall received the highest radiation dose and was deemed the critical organ. Both whole-body effective dose and bladder dose can be reduced by more frequent voiding. 18F-RGD-K5 can be used safely for imaging αvβ3 integrin expression in humans.
Tumor-induced angiogenesis undoubtedly influences tumor progression. Great efforts are being made to develop antiangiogenic therapeutic strategies that interrupt the angiogenic process to deprive the tumor of necessary nourishment (1). Vital components of the angiogenic process are the αvβ3 integrins, which mediate endothelial cell migration and survival during angiogenesis (2). They are expressed on the endothelial cells, forming potential vasculature structures that aid in supplying nutrients to tumor cells, particularly melanomas. In normal tissues, expression of integrin αvβ3 is highly restricted, making the αvβ3 subtype an attractive target for cancer imaging probes. The imaging of integrin αvβ3 as it relates to angiogenesis could provide early information related to changes in a tumor's response to the antiangiogenesis therapy preceding changes in tumor sizes, which are typically visualized using standard imaging methods such as CT or MRI. With this early biochemical information, nonresponders might avoid the continuation of the ineffective antiangiogenesis therapy, unwanted side effects, and cost associated with the treatment. In addition, αvβ3 expression may be an important prognostic factor in characterizing the invasiveness and malignant potential of tumors, including breast and colon cancer (3,4). Noninvasive quantification of αvβ3 expression may have the additional potential of characterizing a malignant tumor's aggressiveness, without the need for invasive collection of tissue samples (i.e., tissue biopsy).
Several integrin αvβ3 receptor binding agents have been developed for use in PET. Several of these imaging agents incorporate a cyclic peptide consisting of an Arg-Gly-Asp (RGD) sequence, which is a well-studied integrin-binding pharmacophore. 18F-galacto-RGD is the most investigated PET tracer for detecting aberrant αvβ3 expression in tumors, showing a favorable biodistribution in humans, with specific receptor binding and visualization of αvβ3 expression in tumors with high contrast (5). However, the radiosynthetic preparation of 18F-galacto-RGD remains complex, involving multiple synthetic steps that complicate routine production (6). In addition, reducing the liver uptake of these RGD-based imaging agents would help widen the imaging area in patients. 2-((2S,5R,8S,11S)-5-benzyl-8-(4-((2S,3R,4R,5R,6S)-6-((2-(4-(3-18F-fluoropropyl)-1H-1,2,3-triazol-1-yl)acetamido)methyl)-3,4,5-trihydroxytetrahydro-2H-pyran-2-carboxamido)butyl)-11-(3-guanidinopropyl)-3,6,9,12,15-pentaoxo-1,4,7,10,13-pentaazacyclopentadecan-2-yl)acetic acid (18F-RGD-K5) is also an RGD-based PET integrin radiotracer (Fig. 1) but additionally contains a metabolically stable, yet highly polar, 1,2,3-antitriazole moiety that increases the tracer's excretion via the kidneys into the bladder, thus circumventing unwanted liver uptake. This tracer binds selectively to integrin αvβ3 (dissociation constant = 7.9 nM) over other related integrins. The tracer has preferential tumor uptake in U87MG xenografts, with a tumor-to-muscle ratio of more than 5:1 after 2 h, making 18F-RGD-K5 a promising tracer for imaging integrin αvβ3 expression in vivo in tumors undergoing aberrant angiogenesis (7). In comparison to 18F-galacto-RGD, the preparation of 18F-RGD-K5 is simple and straightforward using click chemistry, consisting of a single reaction that can be readily automated (7).
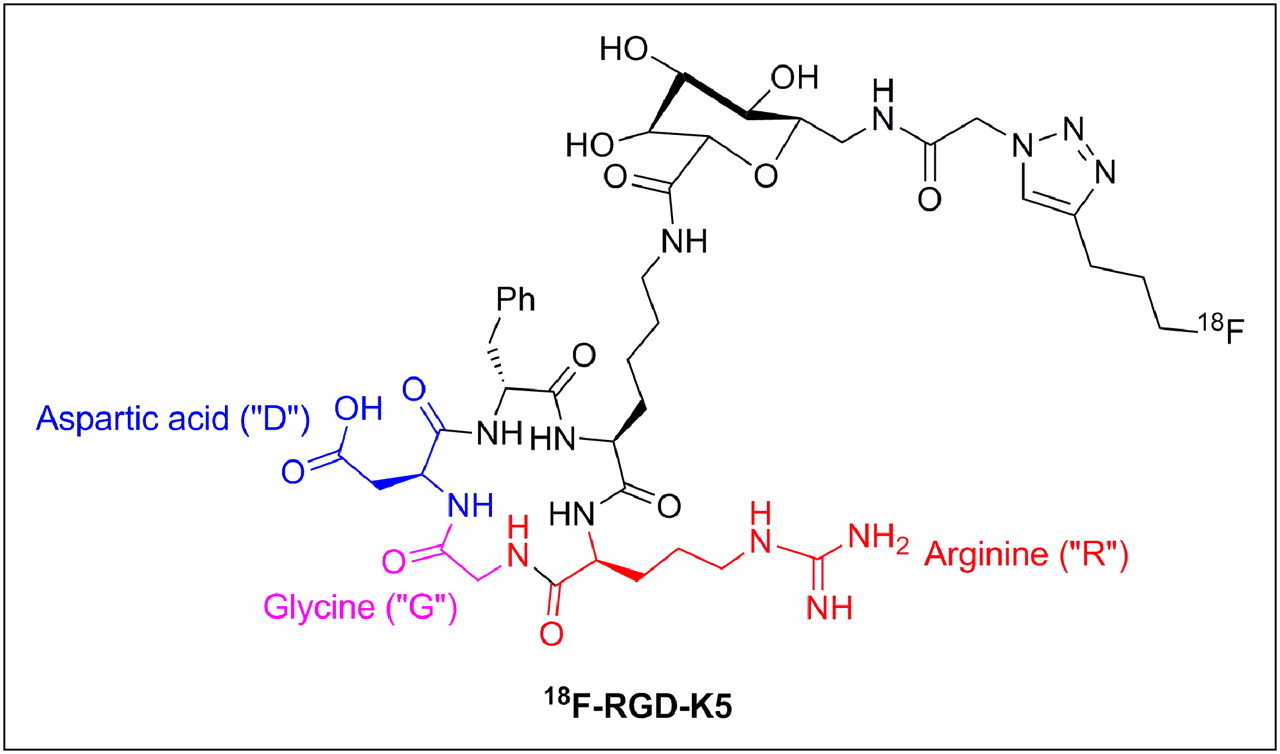
Chemical structure of 18F-RGD-K5.
The main goal of this study was to measure the biodistribution and dosimetry of 18F-RGD-K5 in humans. A secondary goal was to determine whether biodistribution of 18F-RGD-K5 in monkeys can adequately predict the biodistribution and dosimetry in humans.
MATERIALS AND METHODS
Radiopharmaceutical Preparation
18F-RGD-K5 is a triazole-containing RGD peptide useful for detecting αvβ3 integrin expression in vivo.
Production of 18F-RGD-K5 suitable for human injection was accomplished in 2 steps on an automated synthesis module. First, pentyne tosylate was reacted with K18F in the presence of Kryptofix 222 (Sigma Aldrich), K2CO3, and acetonitrile (MeCN) at 110°C for 10 min. After fluorination, the 18F-pentyne was distilled into a vial containing RGD-K5-N3, CuSO4, sodium ascorbate, and a copper ligand tris[(1-benzyl-1H-1,2,3-triazol-4-yl)methyl]amine in the presence of alcohol (EtOH) and water (Fig. 2). After reacting for 10 min, the crude reaction mixture was purified by reversed-phase high-performance liquid chromatography (HPLC) (MeCN:water with 0.05% trifluoroacetic acid), and the collected fraction was reconstituted as an injectable solution of 10% EtOH:water via C18 trap and release. The final solution was passed through a sterile filter (Pall Corp.). This process produced 18F-RGD-K5 that was free of Kryptofix 222, pyrogens, and residual solvents (MeCN ≤ 0.04%); was sterile; and possessed an acceptable pH profile (pH 5–7.5).
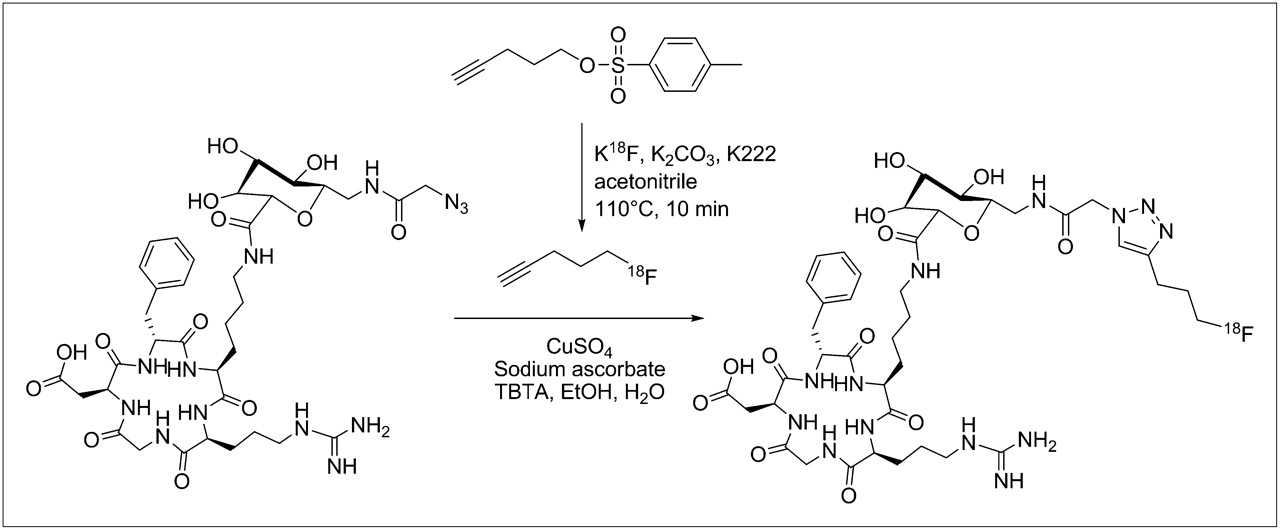
Synthesis of 18F-RGD-K5 from precursor.
The production of 18F-RGD-K5 investigational product was conducted according to our Investigational New Drug application (no. 102,075), submitted to the U.S. Food and Drug Administration. Individual doses of 18F-RGD-K5 contained a maximum of 740 MBq. Each manufactured batch of 18F-RGD-K5 was formulated to yield a minimum specific activity of more than 14.8 GBq/μmol. Therefore, a typical individual patient dose contained, by weight, a microdose ranging up to a maximum of 50 μg of RGD-K5 per dose.
Human Subjects
The study was approved by the Research Review Committee, Institutional Review Board, and Radiation Safety Committee of Fox Chase Cancer Center. Four healthy female volunteers (mean age ± SD, 53 ± 18 y; age range, 32–75 y) were included in the study. Written informed consent was obtained from each subject. The subjects’ weights were 64 ± 5 kg (range, 57–68 kg). All subjects were healthy based on history, physical examination, electrocardiogram, urinalysis, and standard blood tests.
Human PET/CT Acquisition and Image Analysis
After the intravenous injection of 18F-RGD-K5 (583 ± 78 MBq; range, 474–659 MBq) to the volunteers, 5 successive whole-body (WB) PET/CT scans were obtained on a Discovery LS (GE Healthcare) PET/CT scanner. The lowest possible milliampere setting on the scanner was used to acquire the CT scans for attenuation correction. The helical CT scan acquisition parameters were 140 kVp, 10 mA, 0.8-s rotation, 5-mm slice thickness, and 4.25-mm interval.
The WB PET scans were acquired in 2-dimensional mode and ranged from the top of the head to mid thigh. The 5 WB scans were acquired at approximately 15, 60, 90, 120, and 140 min after injection. The scan time was 1.5 min per bed position, and each scan covered 7 bed positions, with single-slice overlap between the bed positions. In addition, after the first WB scan, a PET/CT scan of mid thigh to toes was obtained. Blood pressure, body temperature, pulse, and electrocardiogram were monitored before the administration of 18F-RGD-K5, after the first and second PET/CT scans, and at 24 h after dose administration.
Blood and urine were collected before the drug injection and in the breaks between the PET scans. Urine was also collected at the end of the last PET scan. Samples of urine were assayed in a well counter to estimate the excreted activity in urine. HPLC was performed to determine the amounts of intact 18F-RGD-K5 and its radioactive metabolites in the plasma. Briefly, the radioactivity of the whole-blood samples was measured in a well counter in counts per minute. The whole blood was centrifuged at 3,500 rpm for 5 min to separate plasma from whole cells. The plasma fraction was removed and placed in a separate, empty, preweighed tube to record the weight of plasma. An aliquot of plasma (400 μL) was removed, followed by spiking of the aliquot with nonradioactive RGD-K5 standard (80 μL of 2.5 mg/mL) and acetonitrile (400 μL). After the sample was stirred in a vortex mixer for 30 s and centrifuged at 13,000 rpm for 8 min to separate proteins from plasma, the plasma supernatant was removed and weighed and the counts per minute of pellet and extract were measured. An aliquot (50–100 μL) of the processed plasma sample was injected onto the radio-HPLC column. The radio-HPLC conditions were B = 0.1% trifluoroacetic acid in water; D = 0.1% trifluoroacetic acid in MeCN; t = 0 min 95% B, 5% D; t = 19 min 70%B, 30%D; t = 21 min 5%B, 95% D; flow, 2 mL/min; and wavelength, 206 nm. The radio-HPLC eluent was collected in 1-min fractions and individually counted. No attempts were made to identify the radioactive metabolites in the plasma or urine.
The PET scans were reconstructed to a 50-cm display field of view using an ordered-subsets expectation maximization algorithm with 28 subsets and 2 iterations. The reconstruction included corrections for random coincidences and scatter. Attenuation correction was applied on the basis of the low-dose CT. The accuracy of the activity in the PET images was verified by summing the activity in the first WB PET scan and the PET scan from mid thigh to toes and comparing it with the decayed injected activity.
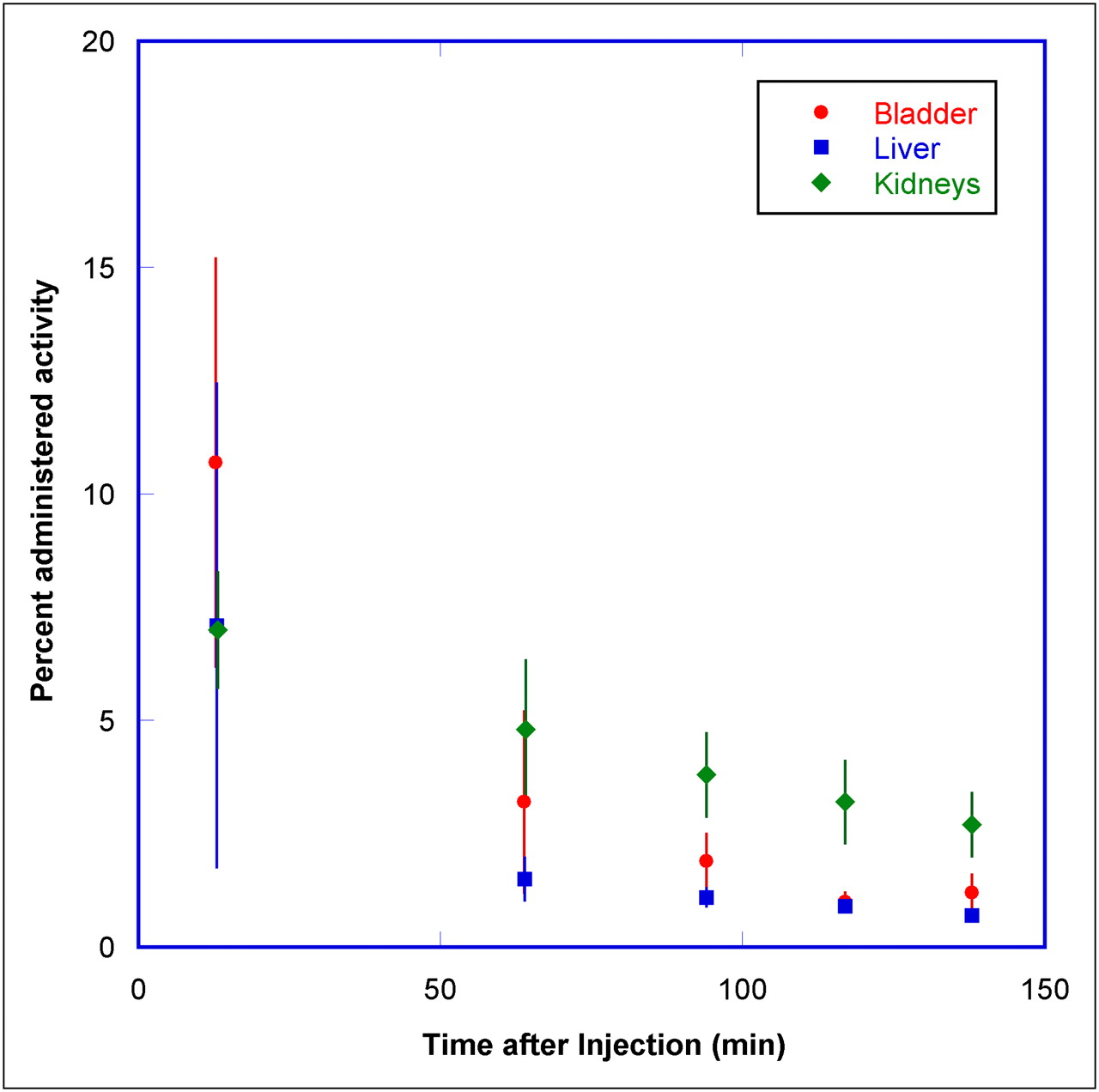
The PET images for the middle time point for each patient were displayed on an imaging workstation. For each organ—including the brain, kidneys, bladder, liver, gallbladder, and large intestine (upper and lower)—volume regions of interest (ROIs) were drawn. For the small intestine, which was not visualized above background, a volume ROI was determined by marking the boundaries of visualized adjacent organs. The PET images for other time points were displayed and registered with this PET scan to transfer the volume ROI and determine the total activity in the organs. Adjustments to the individual ROIs were made to ensure the inclusion of visualized organs (e.g., bladder, gallbladder). The percentage injected activity was determined for the organs for each of the time points. The decay-corrected percentage administered activity for the top 3 organs are shown in Figure 3.

Mean percentage administered activity and SD for top 3 organs determined on basis of four 18F-RGD-K5 PET emission scans in human volunteers, as function of time after injection. Rapid clearance of activity was observed in organs.
Normalized Number of Disintegrations
The percentage administered activity for each organ for each time point was fitted to an exponential or sum-of-exponentials function in OLINDA/EXM software (8) to determine the total number of disintegrations per unit administered activity, hereafter referred to as normalized number of disintegrations. Activity in the remainder of the body was calculated for each time point as the injected activity minus the activity in all the source organs and in collected urine. The half-times for biologic excretion were computed by exponential fitting of injected activity minus accumulated urine activity as a function of time. The 1- and 4.8-h bladder-voiding models in OLINDA/EXM were used to determine the normalized number of disintegrations in the bladder. Absorbed doses in the various organs were calculated by entering the normalized number of disintegrations of all source organs for each subject into OLINDA/EXM, using the standardized adult male and female models.
Animal Subjects
The rhesus monkey studies were approved by the West Point Institutional Animal Care and Use Committee at Merck Research Laboratories. Three male rhesus monkeys (ages, 7, 9, and 11 y) were initially anesthetized with ketamine (10 mg/kg intramuscularly), then induced with propofol (5 mg/kg intravenously), intubated, and ventilated with medical-grade air. Anesthesia was maintained with propofol (0.4 mg/kg/min) for the duration of the study, and the vital signs (electrocardiogram, expired tidal CO2, SPO2, and temperature) were monitored and maintained in the reference range for the duration of the study. Animals were administered an intravenous bolus of 167 ± 19 MBq of 18F-RGD-K5 in a 3 mL-volume injected with a 10- to 15-s bolus duration.
PET/CT Acquisition
After the injection of 167 ± 19 MBq of 18F-RGD-K5 to the monkeys, low-dose unenhanced CT (120 kVp, 60 mA, 0.5-s rotation, and 3.75-mm slice thickness) was performed, followed by dynamic whole-body PET on a Discovery ST (GE Healthcare) PET/CT scanner. Twenty-four WB PET images were acquired in 2-dimensional mode for 5 bed positions covering 72.9 cm axially for a total duration of 200 min (time per bed range, 15 s to 4 min).
After the completion of WB PET, contrast-enhanced CT (200 mA, 120 kVp, 0.5-s rotation, and 3.75-mm slice thickness) using iohexol (Omnipaque 300; GE Healthcare) (2.5 mL/kg) was performed to assist with organ identification.
Data Analysis
The PET scans were reconstructed using an ordered-subsets expectation maximization algorithm with 30 subsets and 2 iterations and a gaussian postprocessing filter of 3 mm in full width at half maximum. The reconstruction included corrections for scatter and random coincidences. Attenuation correction was applied on the basis of the low-dose CT.
For each study, ROIs were delineated using both the enhanced CT and the summed PET. ROIs included the brain (CT), heart content (first PET), liver (summed PET), spleen (CT), kidneys (CT), testes (CT), and urinary bladder (last PET). The gut ROI was drawn around the abdomen, excluding all other delineated organs. As such, the gut ROI included the gallbladder. ROIs were projected onto the PET images at each time point. Time–activity curves were obtained by calculating the total activity in the ROIs and expressing them as percentage of the total injected activity.
Absorbed Dose Calculations
The percentage administered activity in each source organ was iteratively fitted to a biexponential function using a nonlinear least-squares regression algorithm (SAAM II, version 1.2, software) (9) to obtain the normalized number of disintegrations for important source organs.
Rhesus monkeys accumulated radioactivity in the urinary bladder over the duration of the study. The percentage administered activity in the bladder, obtained from the monkey images, was used as input, and the number of disintegrations from the urinary bladder's contents was calculated using the dynamic bladder model of Cloutier et al. (10). Bladder-voiding intervals of 1 and 4.8 h were used.
In this analysis, the gut ROI comprised the gallbladder, small bowel, upper large intestine, and lower large intestine. The value for fecal excretion fraction (fgut) was taken as the value at the last image time (≅200 min). The gut residence times were calculated using the model for gastrointestinal tract kinetics from the International Commission on Radiation Protection publication 30 (11), assuming the radioactivity entered via the small bowel.
To obtain an estimate of the corrected total-body time–activity curve (which excluded the activity in the gut and bladder), the total-body time–activity curve was first constructed as decay-corrected injected activity minus the urinary excreted activity and was fit to a biexponential function. Second, to correct the total-body time–activity curve for fecal excretion, the total-body curve was also multiplied by a factor of 1 – fgut, where fgut is the fecal excretion fraction. The corrected total-body number of disintegrations was calculated by integrating the corrected total-body time–activity curve fit. The remainder of the body number of disintegrations was calculated as the corrected total-body number of disintegrations minus all other disintegrations, except the bladder and gut.
Human radiation doses were calculated from these rhesus monkey normalized number of disintegrations using OLINDA/EXM for the adult male and female phantoms. No scaling of the rhesus biodistribution data was done to estimate human absorbed radiation doses. Thus, it was assumed that the biodistribution in these monkeys was the same as in humans.
RESULTS
Human Studies
The injection of 583 ± 78 MBq of 18F-RGD-K5 in 3 subjects produced no clinically significant effects on vital signs (blood pressure, temperature, pulse, and electrocardiogram) and blood tests during the 2.5-h observation period after administration and in the follow-up visit at 24 h.
The analysis of plasma samples of 2 subjects showed that the level of unmetabolized 18F-RGD-K5 in the plasma remained constant (>95% intact) over 90 min after injection, consistent with human metabolism data reported for this class of compounds (5). 18F-RGD-K5 exhibited a plasma clearance half-time of approximately 12 min.
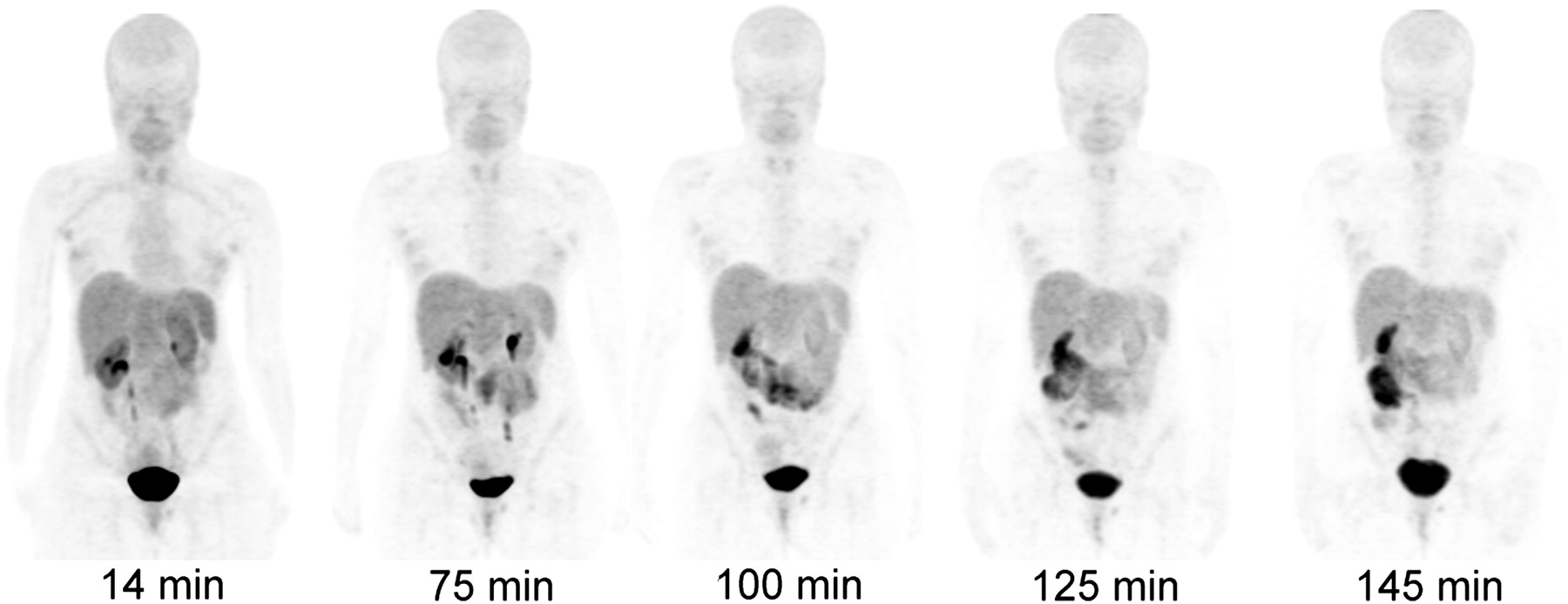
Figure 4 displays PET maximum-intensity-projection images for 1 of the subjects from the PET scans. In the first scan, the predominant uptake was seen in the urinary bladder, with moderate uptake in the liver and kidneys. The gallbladder and small intestine displayed 18F-RGD-K5 uptake in later scans. All other organs had a near-background level of activity. Mean standardized uptake values at about 1 h after injection were approximately 50 in bladder, 20 in kidneys, 10 in gallbladder, and 4 in liver. The rest of the body had low standardized uptake values. The percentage administered activity for the top 3 organs is shown in Figure 5. There was large intersubject variation in the bladder uptake (6.4%–12.4%) and kidney uptake (3%–14%), as indicated by the large error bars. The renal system (kidneys and bladder together) had more consistent uptake, ranging from 18.4% to 20.4%. The liver had the next highest uptake, ranging from 6.2% to 8.7%. The study drug was excreted primarily via the renal system. By the end of the study (∼2.5 h), approximately 44% of the injected activity of 18F-RGD-K5 had been excreted in the urine, as determined by assaying urine samples in a well counter.

Decay-corrected anterior maximum-intensity projections of PET at 14, 75, 100, 125, and 145 min after injection of 18F-RGD-K5 in female volunteer. There was rapid clearance of activity in kidneys, liver, and bladder. Gallbladder activity peaked at 75 min and then decreased with time.

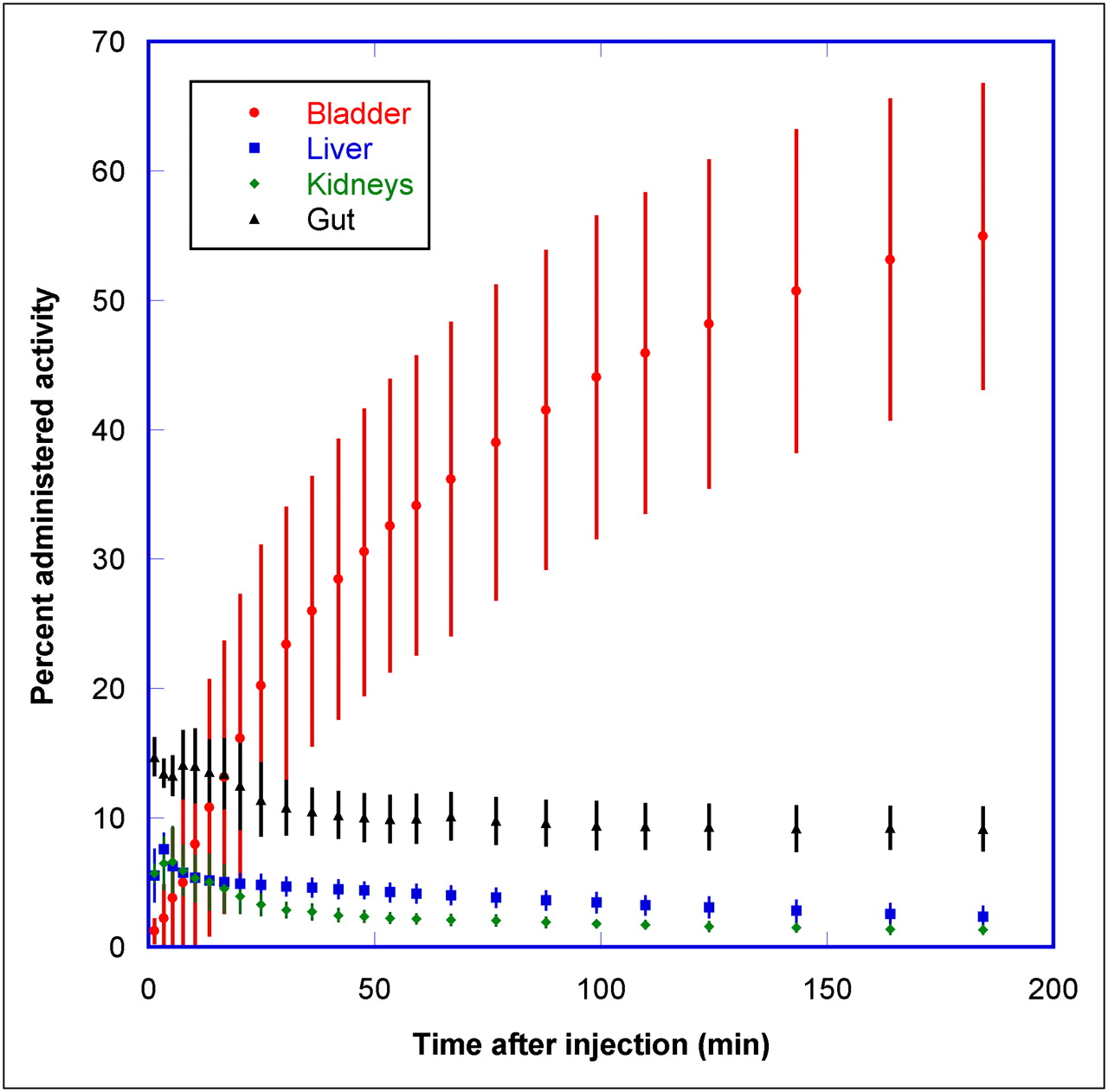
Mean percentage administered activity and SD for top 4 organs determined on basis of 3 rhesus monkey 18F-RGD-K5 PET emission scans, as function of time after injection. Liver and kidney activities decreased rapidly with time, and bladder activity increased with time (there was no voiding because monkeys were anesthetized).
The normalized number of disintegrations for the organs is listed in Table 1. The mean organ doses are given in Table 2. The mean effective dose of 18F-RGD-K5 for the human adult male phantom was 15 ± 1 and 31 ± 1 μSv/MBq for the 1- and 4.8-h bladder-voiding models, respectively. For a typical 555-MBq injected dose of 18F-RGD-K5, the WB effective dose for the 2 models would be 8.3 ± 0.6 and 17.2 ± 0.6 mSv, respectively. The adult female phantom doses were typically approximately 25% higher. The 3 organs with the highest radiation absorbed doses were urinary bladder wall, gallbladder wall, and kidneys.
Normalized Number of Disintegrations of Source Organs for Human Subjects Injected with 18F-RGD-K5
Radiation Dosimetry Estimates per Unit Administered Activity for 18F-RGD-K5 for Human Adult Male Phantom in 1- and 4.8-Hour Bladder-Voiding Models, Based on Human Biodistribution Data
Monkey Studies
The injection of 167 ± 19 MBq of 18F-RGD-K5 in 3 male monkeys produced no clinically significant effects on vital signs (blood pressure, pulse, and electrocardiogram) and blood tests during the 3-h observation period after administration. In the rhesus monkey, the liver was best visualized at approximately 37 min after injection, whereas the bladder content became visible at approximately 10 min after injection.
The PET maximum-intensity-projection images at 1, 13, 42.6, 111.5, and 190 min after injection are shown in Figure 6. At 3 min, rapid uptake of 18F-RGD-K5 was observed in the heart, kidneys, and liver. The bladder's activity accumulated over time, because the rhesus monkeys were under anesthesia and did not void. Gallbladder uptake was observed at later time points. Rapid clearance of activity in the kidneys and liver was observed in the images at subsequent time points. The urinary bladder had the highest uptake, with 55% ± 12% of injected activity at the end of the 3-h PET/CT acquisition. The peak values of percentage administered activity in the liver, kidneys, and brain were 7.6% ± 1.2%, 6.6% ± 2.7%, and 0.42% ± 0.1%, respectively, at 3–4 min after injection. At the end of the study, 9.1% ± 1.6% of injected activity was found in the gut, which included the gallbladder, small intestine, and upper and lower portions of the large intestine.

Decay-corrected anterior maximum-intensity projections of PET at 1, 13, 42.6, 111.5, and 190 min after injection of 18F-RGD-K5 in rhesus monkey. Liver and kidney activities decreased rapidly with time, and bladder and rectum accumulated activity with time (there was no voiding of bladder because monkey was anesthetized).
The normalized number of disintegrations for the organs is listed in Table 3. The mean organ doses for the male human phantom estimated using primate 18F-RGD-K5 biodistribution are given in Table 4. The 4 organs with the highest radiation-absorbed doses were the urinary bladder wall, upper large intestine wall, small intestine, and testes. The mean effective dose of 18F-RGD-K5 was 23 ± 0.3 for the 1-h and 40 ± 4.4 μSv/MBq for the 4.8-h bladder-voiding models. The estimated doses for the female human phantom were higher by approximately 25%.
Normalized Number of Disintegrations of Source Organs for Rhesus Monkeys Injected with 18F-RGD-K5
Radiation Dosimetry Estimates per Unit Administered Activity for 18F-RGD-K5 for Human Adult Male Phantom in 1- and 4.8-Hour Bladder-Voiding Models, Based on Primate Biodistribution Data
DISCUSSION
18F-RGD-K5, developed as an integrin marker, was investigated in this dosimetry study in both humans and monkeys. The findings from this investigation show substantial promise of 18F-RGD-K5 as a PET agent, with a reasonable biodistribution and safety profile in human subjects. This study provides information on the background uptake levels in normal organs. The data also assess the potential radiation exposure in humans through WB PET in humans and monkeys.
In humans, 18F-RGD-K5 revealed a biodistribution dominated by activity in the bladder, kidneys, and liver and steady renal clearance, with 44% of injected activity excreted within the 2.5-h duration of the study. In the intermediate and late scans, gallbladder and small intestine activity was observed. The relatively wide range of activities seen in the various organs implies a wide range of absorbed radiation doses. The urinary bladder, liver, kidneys, gallbladder, and small intestine had radioactivity levels greater than background radioactivity.
Among all the organs observed, the urinary bladder received the highest dose in the 4.8-h bladder-voiding model. The mean urinary bladder wall dose was 103 ± 4 and 376 ± 19 μGy/MBq for the 1- and 4.8-h bladder-voiding models, respectively. The gallbladder and kidneys had the next highest doses: 104 ± 52 for the 1-h model and 45 ± 10 μGy/MBq for the 4.8-h model. The remaining organs had lower doses, in the range of 5–32 μGy/MBq. The average values of effective dose for 18F-RGD-K5 were 15 ± 1 and 31 ± 1 μSv/MBq, respectively, for the 2 models. For a typical 555-MBq injected dose of 18F-RGD-K5, the effective dose for the 4.8-h model is 17.2 ± 0.6 mSv. The effective dose was lower than the 30-mSv WB dose limit specified by the Food and Drug Administration for research subjects (12). The doses can be reduced by more frequent bladder voiding. For the 1-h bladder-voiding model, the WB effective dose reduces to 8.3 ± 0.6 mSv.
18F-RGD-K5 was found to be intact in human plasma up to 90 min after injection. This result is consistent with the metabolic profile of other RGD-containing PET tracers in human plasma (5). One possible explanation for the stability of this tracer in vivo is the rapid clearance of the tracer through the renal system, with relatively little exposure time within the liver.
In monkeys, 18F-RGD-K5 showed a biodistribution dominated by activity in the kidney and bladder and steady renal clearance, with 17% ± 2% of injected activity excreted in the 3 h of the study. In the intermediate scans, rapid clearance of activity was observed in all the organs, and intestinal elimination as indicated by gut activity was also observed. The liver, kidneys, and heart contained above-background activities in the early stages after injection, with the gallbladder and gut activity accumulating at later time points. Mean standardized uptake values 1 h after injection were approximately 2 in liver and approximately 6 in the kidneys and gallbladder.
For the human adult male model, only the urinary bladder wall was estimated to receive radiation doses larger than 100 μGy/MBq. The mean bladder wall dose was 110 and 400 μGy/MBq for 1- and 4.8-h bladder-voiding intervals, respectively. Upper large intestine wall and small intestines received the next highest doses. The mean values of the effective dose for the human adult male model were 23 ± 0.3 μSv/MBq (1-h voiding interval) and 40 ± 4.4 μSv/MBq (4.8-h voiding interval).
The monkey data included fast-sampling or dynamic PET scans (15 s per bed position) during the first few minutes, followed by longer PET scans (4 min per bed position). The human data did not include the fast sampling but consisted of sequential WB PET scans at 6 min per bed position. A comparison of dosimetry for another 18F-based imaging agent using similar datasets has shown that consistent dosimetry results were obtained without the fast sampling (13). Hence, the comparison of results between monkey and human data may be justified despite differences in the acquisition parameters.
There were many similarities between the monkey and human biodistribution and dosimetry data. In both human and monkey datasets, the organs with the highest normalized number of disintegrations of 18F-RGD-K5 were the urinary bladder, liver, and kidneys. In addition, in both cases the bladder wall received the highest dose. In both datasets, the various organs of the digestive tract had similar dose levels. For humans, the doses ranged from 6 to 64 μGy/MBq, whereas for monkeys, the doses ranged from 9 to 75 μGy/MBq. The effective dose was 40 ± 4.4 μSv/MBq for monkey-derived estimates and 31 ± 1 μSv/MBq for human-based estimates in the 4.8-h bladder-voiding model. For the 1-h bladder-voiding model, the effective doses were 23 ± 0.3 μSv/MBq for monkey-derived estimates and 15 ± 1 μSv/MBq for human-based estimates.
Table 5 compares the doses to individual organs for 18F-RGD-K5, 18F-FDG (14), 18F-HX4 (15), and 18F-fluromisonidazole (4-h bladder-voiding model) (16,17). The absorbed doses in the heart, brain, and breasts were much lower for 18F-RGD-K5 than for 18F-FDG. 18F-RGD-K5 did not appreciably cross the blood–brain barrier in our imaging studies. The absorbed doses in urinary bladder, liver, and kidneys were higher for 18F-RGD-K5 than for 18F-FDG. A large fraction of 18F-RGD-K5 (∼44% in 2.5 h) and 18F-HX4 (∼45% in 3.5 h) was excreted through the urinary system, whereas 18F-fluromisonidazole had little urinary excretion (∼4% in 5 h). Hence, the urinary bladder doses for 18F-RGD-K5 (376 μGy/MBq) and 18F-HX4 (299 μGy/MBq) were much higher than that for 18F-fluromisonidazole (29 μGy/MBq) (for 4-h bladder-voiding model). However, steps can be taken to reduce the bladder dose. Patients can be encouraged to void frequently because the bladder dose reduced to approximately 103 ± 4 μGy/MBq in the 1-h bladder-voiding model.
Organ Doses in μGy/MBq for Several 18F-Based Imaging Agents
Table 6 compares WB radiation dose and effective dose from 18F-RGD-K5 with doses from a few 18F-based radiopharmaceuticals (14,16,17). As shown in these tables, the radiation dose from 18F-RGD-K5 is comparable to that from other 18F-based imaging agents.
Comparison of Dose per Unit Administered Activity Between 18F-RGD-K5 and Other 18F-Based Imaging Agents
CONCLUSION
The biodistribution profile of 18F-RGD-K5 was similar for monkeys and humans. For a typical 555-MBq injected dose of 18F-RGD-K5, the effective dose for the 4.8- and 1-h bladder-voiding models was 17.2 ± 0.6 and 8.3 ± 0.6 mSv, respectively. The urinary bladder wall had the highest dose among all the organs and is deemed to be the critical organ. With frequent bladder voiding, doses to the bladder and the WB can be reduced. 18F-RGD-K5 can be used safely in humans for imaging integrin αvβ3 expression.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We thank Donna Mosley for her help with patient data acquisition. We thank Mary Benetz and the staff from the Protocol Management Office, Clinical Research Unit, and Protocol Support Laboratory for their help with the research protocol. In addition, we thank Stephen M. Krause, Merck and Co., for the rhesus monkey data acquisition. The study was supported by Siemens Molecular Imaging Inc. The human part of the study was conducted at Fox Chase Cancer Center under the ClinicalTrials.gov Identifier NCT00743353. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 12, 2012.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- Received for publication July 25, 2011.
- Accepted for publication January 10, 2012.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- PET-Based Human Dosimetry of the Dimeric {alpha}v{beta}3 Integrin Ligand 68Ga-DOTA-E-[c(RGDfK)]2, a Potential Tracer for Imaging Tumor Angiogenesis
- Internal Dose Assessment of (-)-18F-Flubatine, Comparing Animal Model Datasets of Mice and Piglets with First-in-Human Results
- Interrogating Tumor Metabolism and Tumor Microenvironments Using Molecular Positron Emission Tomography Imaging. Theranostic Approaches to Improve Therapeutics
- The Growing Impact of Bioorthogonal Click Chemistry on the Development of Radiopharmaceuticals