


Abstract
PET allows absolute measurements of myocardial blood flow (MBF). The aim of the present study was to evaluate the feasibility and repeatability of supine bicycle exercise stress, compared with standard adenosine stress, in PET. Methods: In 11 healthy volunteers, MBF was assessed at rest, during adenosine-induced (140 μg/kg/min over 7 min) hyperemia, and immediately after supine bicycle exercise (mean workload, 130 W, which is 70% of the predicted value) using PET and 15O-H2O. The assessment was then repeated after 20 min. Coronary flow reserve (CFR) was calculated as hyperemic/resting MBF for adenosine stress and exercise stress. Repeatability was evaluated according to the method of Bland and Altman. Results: No significant differences were found between the paired resting MBF (1.22 ± 0.16 vs. 1.26 ± 0.21 mL/min/g; mean difference, 3% ± 11%) and the hyperemic MBF with adenosine stress (5.13 ± 0.74 vs. 4.97 ± 1.05; mean difference, −4% ± 14%) or exercise stress (2.35 ± 0.66 vs. 2.25 ± 0.61; mean difference, −4% ± 19%). CFR was reproducible with adenosine stress (4.23 ± 0.62 vs. 4.05 ± 1.06, P = not statistically significant; mean difference, −5% ± 19%) and exercise stress (1.91 ± 0.46 vs. 1.80 ± 0.44, P = not statistically significant; mean difference, −5% ± 15%). Repeatability coefficients for MBF were 0.26 (rest), 1.34 (adenosine stress), and 0.82 (exercise stress) mL/min/g. Conclusion: Assessment of CFR with 15O-H2O and PET using bicycle exercise in the PET scanner is feasible and at least as repeatable as using adenosine stress.
Quantitative regional myocardial blood flow (MBF) can be measured noninvasively and accurately using PET. 15O-water is metabolically inert and freely diffuses across all capillary membranes, including the capillary membrane of the myocardium, rapidly equilibrating between the vascular and extravascular spaces. The 2-min half-life of the 15O-isotope allows repetitive MBF measurements at 10-min intervals. A traditional shortcoming of the 15O-water technique used to be its need for additional 15O-carbon monoxide blood pool scans to define the regions of interest and correct for the high 15O activity in the blood pool. Recently, a new technique has been proposed for generating myocardial images directly from dynamic 15O-water scans, eliminating the need for additional C15O blood pool scans (1) while allowing for serial 15O-water PET measurements of MBF. This technique has recently been validated against microspheres in experimental animals (2,3), and its repeatability has been documented in humans (4).
Baseline and hyperemic MBF measurements allow the assessment of coronary flow reserve (CFR), or hyperemic/baseline MBF, an integrated parameter of endothelial function and vascular smooth muscle relaxation. PET has been widely used to assess CFR in healthy volunteers and in patients with coronary artery disease, cardiovascular risk factors, and other cardiac diseases (5). Similarly, measurement of CFR with PET has been used to assess the effects of cardiovascular conditioning, coronary angioplasty (6), and pharmacologic interventions (7). Adenosine or dipyridamole are commonly used as a hyperemic stimulus, although little is known about their interaction with drugs studied in pharmacologic interventions. Furthermore, the use of a pharmacologic stimulus may be of limited value in the assessment of the physiologic importance of any cardiovascular disease. Physical exercise is a physiologic stimulus that reflects the natural response of the coronary arteries to physical activities better than can any isolated pharmacologic stimulation (8–11).
However, very few reports in the literature deal with physical exercise in PET (12–15), and to our knowledge, neither the feasibility nor the repeatability of exercise stress in PET has ever been studied. Thus, the present study was designed to evaluate the feasibility and repeatability of inducing hyperemic MBF by supine bicycle exercise stress in the PET scanner and to compare the resulting MBF with adenosine-induced hyperemic MBF.
MATERIALS AND METHODS
The study protocol was approved by the local ethics committee. All subjects gave informed and written consent before the study.
Study Population
Eleven healthy male volunteers (mean age, 27 ± 8 y) were studied. None had a history of cardiovascular disease or smoking. Entrance criteria included normal heart rate, normal blood pressure, normal resting electrocardiogram (ECG), and low clinical probability of coronary artery disease (16). In addition, all volunteers were carefully instructed to refrain from caffeine intake during the 24 h before the study.
Study Protocol
Figure 1 summarizes the study protocol. With the patient’s feet attached to a bicycle ergometer (model 380 B; Siemens-Elema AG, Zurich, Switzerland), MBF was measured at rest. After 10 min had been allowed for decay of 15O radioactivity in the body, MBF was measured again during adenosine-induced hyperemia. Adenosine has a very short half-life of <10–20 s and is therefore suitable for repetitive use within the same session. It was infused for 7 min at 140 μg per kilogram of body weight per minute, according to standard practice (17). Three minutes after the start of the adenosine infusion, the hyperemic MBF measurement was started. After 10 min, exercise was begun at 50–75 W, and workload was increased in increments of 25–50 W until 70% of the predicted value for upright bicycle exercise was reached (mean workload, 130 W). MBF was measured immediately after the end of exercise. A 20-min transmission scan was then acquired for attenuation correction of all emission scans and to allow time for the volunteer to recover after the physical exercise. Measurement was repeated using the same protocol at rest, during adenosine stress, and immediately after supine bicycle exercise.
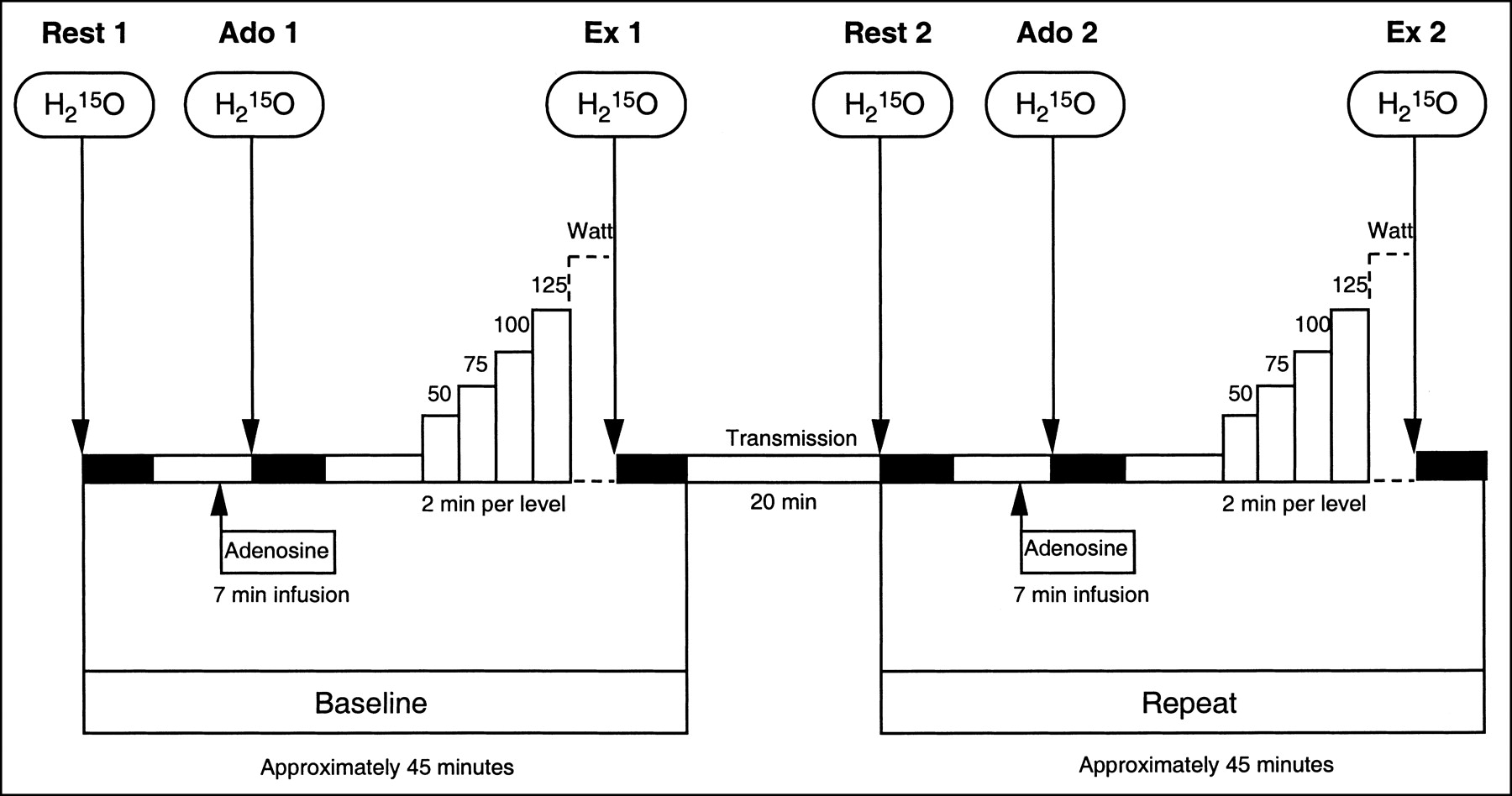
MBF was assessed with H215O and PET at rest (Rest 1), during adenosine-induced hyperemia (Ado 1; intravenous adenosine infusion at 140 μg/min/kg over 7 min), and immediately after supine bicycle exercise (Ex 1) in scanner (workload is indicated in watts). All measurements were repeated (Rest 2, Ado 2, and Ex 2) after 20-min transmission scan.
Blood pressure was continuously monitored (Finapress; BOC Inc., Englewood, CO) and was recorded at 1-min intervals. The ECG was monitored continuously throughout the procedure, and a 12-lead ECG was recorded at baseline, at 1-min intervals during adenosine administration, at each exercise level, and during 10 min of recovery.
Image Acquisition
PET was performed on an Advance scanner (General Electric Medical Systems, Milwaukee, WI). This device records 35 image planes simultaneously. The axial field of view is 14.5 cm. A 30-min blank scan was recorded as part of the daily routine. The optimal imaging position was determined by a 2-min rectilinear scan after exposure of an external 68Ge ring source. Starting after the background frame, 15O-water (500–700 MBq) was injected as an intravenous bolus over 20 s at an infusion rate of 10 mL/min to assess MBF. The line was then flushed for another 2 min. The dynamic image sequences were 14 × 5 s, 3 × 10 s, 3 × 20 s, and 4 × 30 s.
Image Processing
The sinograms obtained were corrected for attenuation and were reconstructed on a workstation (SUN Microsystems, Mountain View, CA) using standard reconstruction algorithms. Images were transferred to a personal computer (model 2200; transtec Computer AG, Bulach, Switzerland) and were analyzed with pixelwise modeling software (PMOD; University Hospital Zurich, Zurich, Switzerland). Myocardial images were then generated directly from the dynamic 15O-water study, avoiding the need for additional 15O-carbon monoxide blood pool scans to define regions of interest as previously reported (1–4). Briefly, the factor sinograms were generated by linear dimension reduction of the dynamic sinograms, on which the required variate and covariate factors (the myocardial and blood time-activity curves) were modeled from the lung time-activity curve. The general theory for optimal linear-dimension reduction of sequences of medical images has recently been reported (18,19). Factor images were generated by iterative reconstruction (1). Regions of interest were drawn within the left ventricle on 4–6 consecutive image planes and were projected both onto the dynamic 15O-water images, to generate blood time-activity curves (input function), and onto the right ventricle, to correct for spillover in the septum. Similarly, myocardial regions of interest were drawn within the left ventricular myocardium on at least 12 consecutive image planes and were projected onto the dynamic 15O-water images to obtain tissue activity curves. The regions were drawn semiautomatically using a centerline within the myocardium. The junctions of right and left ventricle were marked to indicate the septum. The left ventricular free wall was then subdivided geometrically into 3 segments of the same size. In accord with the recommendations of the American Society of Echocardiography (20), the left ventricle was subdivided into a total of 16 segments. However, for the present analysis the subsegments were grouped to obtain a mean value for septal, anterior, lateral, and inferior wall segments. Arterial and tissue activity curves were fitted to a single-tissue-compartment tracer kinetic model to give values of regional and global MBF (mL/min/g), as has previously been described (7,21).
MBF, CFR, and Coronary Resistance
Because MBF at rest is determined mainly by cardiac workload (22), we corrected MBF at rest for rate-pressure product (RPP) using the following equation: Corrected MBF = (MBF/RPP) × 104 (3). To account for the variability of coronary driving pressure, the ratio of mean arterial pressure to MBF was calculated as an index of coronary resistance as previously described (23,24).
CFR was defined as the ratio of MBF during hyperemia (induced by either adenosine or exercise) to MBF at rest and was calculated for baseline and repeated measurements.
Statistical Analysis
Statistical comparison of hemodynamic data, MBF, and CFR was performed by 1-way ANOVA for repeated measurements. Data are reported as mean ± SD. To test the repeatability of each measurement, we analyzed the difference between the 2 measurements according to the method of Bland and Altman (25). The repeatability coefficient was calculated as 1.96 times the SD of the differences, following the definition adopted by the British Standards Institution (26). For better comparison, the repeatability coefficient is also given as a percentage of the average value of the 2 measurements.
RESULTS
The procedure was well tolerated, apart from the common side effects caused by adenosine. None of the subjects experienced any ECG changes during the procedure.
Hemodynamics
During the 2 resting measurements, systolic blood pressure, diastolic blood pressure, mean aortic blood pressure, and RPP were comparable (Table 1). However, heart rate was slightly higher during the repeated resting measurements, possibly because recovery time after bicycle exercise was too short for some volunteers. For the RPP values at the initial and repeated rest tests, we found a repeatability coefficient of 2,573, that is, 32% of the mean RPP. The same comparison during the 2 adenosine infusions revealed no significant difference between the mean values (Table 1). The repeatability coefficient of RPP was comparable, namely 3,826, or 32% of the mean RPP. The value for the comparison of baseline and repeated exercise was 5,020, that is, 26% of the mean RPP.
Hemodynamics
MBF and CFR
The first and second resting mean MBF values were 1.22 ± 0.16 and 1.26 ± 0.21 mL/min/g, respectively (Table 2), with a mean difference of 3% ± 11% (P = not statistically significant [NS]). The individual MBF values and the Bland-Altman plot are shown in Figure 2. The agreement of both measurements is shown in Figure 3. The repeatability coefficient for resting MBF was 0.26 mL/min/g, equaling 21% of the mean (Table 2). The respective values for the corrected MBF were 1.75 ± 0.37 and 1.46 ± 0.29 mL/min/g (P = NS), resulting in a slightly higher mean difference of −12% ± 16% and a repeatability coefficient of 0.58 mL/min/g (37% of the mean).

(A) Repeated resting and hyperemic MBF measurements. Paired values are given for each participant. Mean values (large circles) are given as mean ± 1 SD. (B) Differences in paired values are plotted against their average value (Bland-Altman plot). Repeatability is best at rest but comparable during adenosine and bicycle exercise. Rest 1 and 2, Ado 1 and 2, and Ex 1 and 2 are defined as in Figure 1.
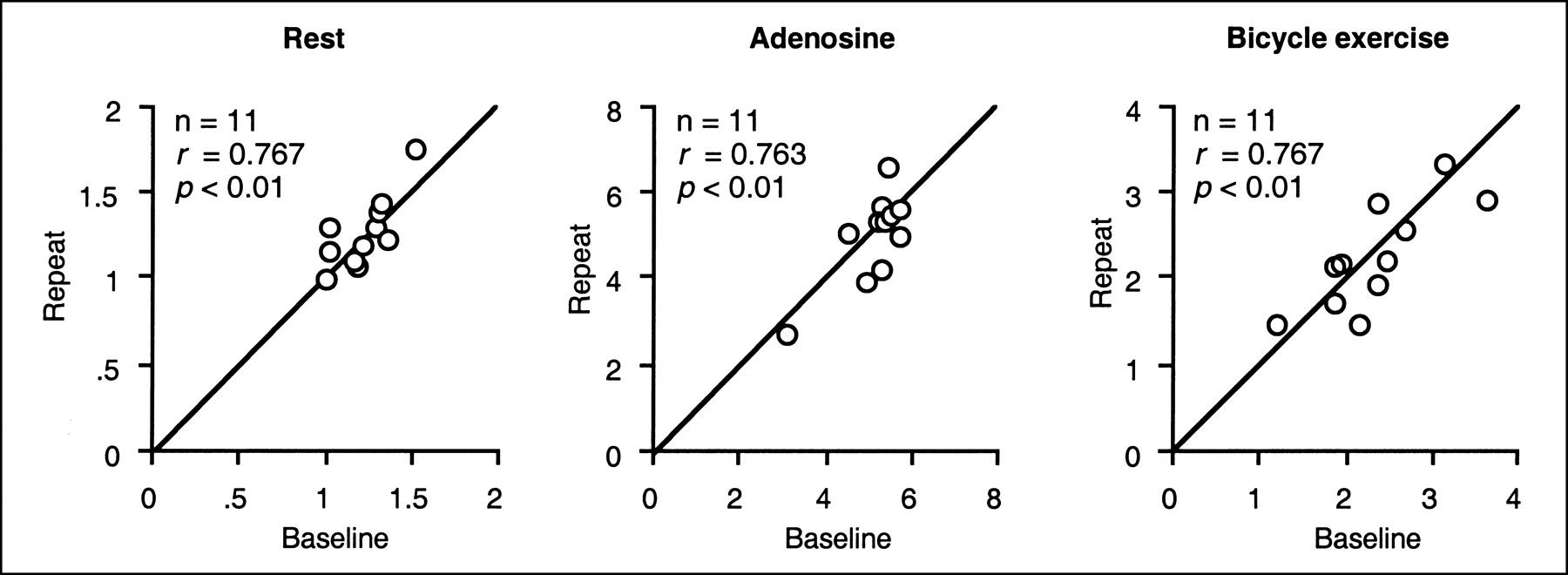
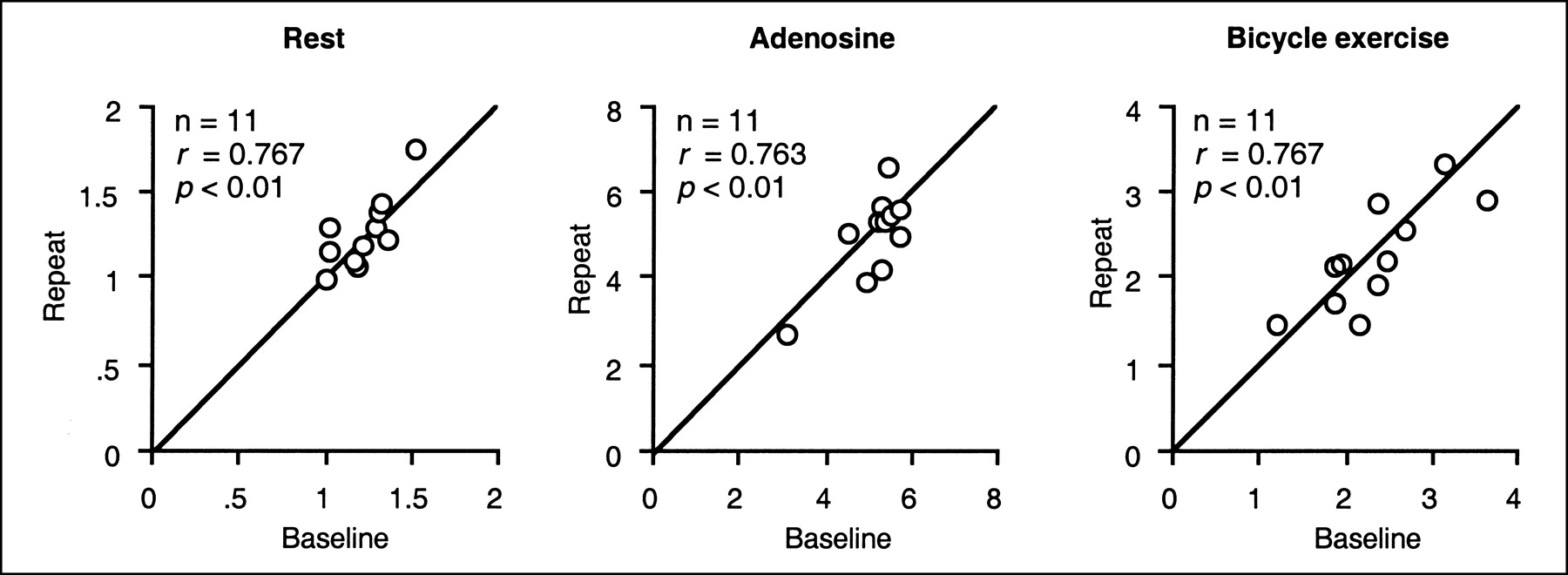
Scattergram of repeated MBF measurements (mL/min/g). Line of equality, along which points would lie if agreement were perfect, is shown.
Myocardial Blood Flow
Adenosine induced a significant increase in mean MBF—to 5.13 ± 0.74 mL/min/g (initial adenosine test; P = 0.0001 vs. initial rest test) and 4.97 ± 1.05 mL/min/g (repeated adenosine test; P = 0.0001 vs. repeated rest test), with no significant difference (−4% ± 14%) between the 2 hyperemic measurements (Fig. 2). The repeatability coefficient for the 2 hyperemic MBF values (Table 2) was 1.34 mL/min/g (27% of the mean).
Bicycle exercise also induced a significant increase in mean MBF—to 2.35 ± 0.66 mL/min/g (initial exercise test; P < 0.001 vs. initial rest test) and 2.25 ± 0.61 mL/min/g (repeated adenosine test; P < 0.001 vs. repeated rest test), with no significant difference (−4% ± 19%) between the 2 hyperemic measurements. The agreement of both measurements is shown in Figures 2 and 3. The repeatability coefficient for the 2 MBF values after exercise was 0.82 mL/min/g (36% of the mean) (Table 2). The MBF values were significantly lower after exercise than during adenosine stress (P < 0.001). The values of the regional MBF are given in Table 2. The best (lowest) repeatability coefficient was that for the inferior wall at rest.
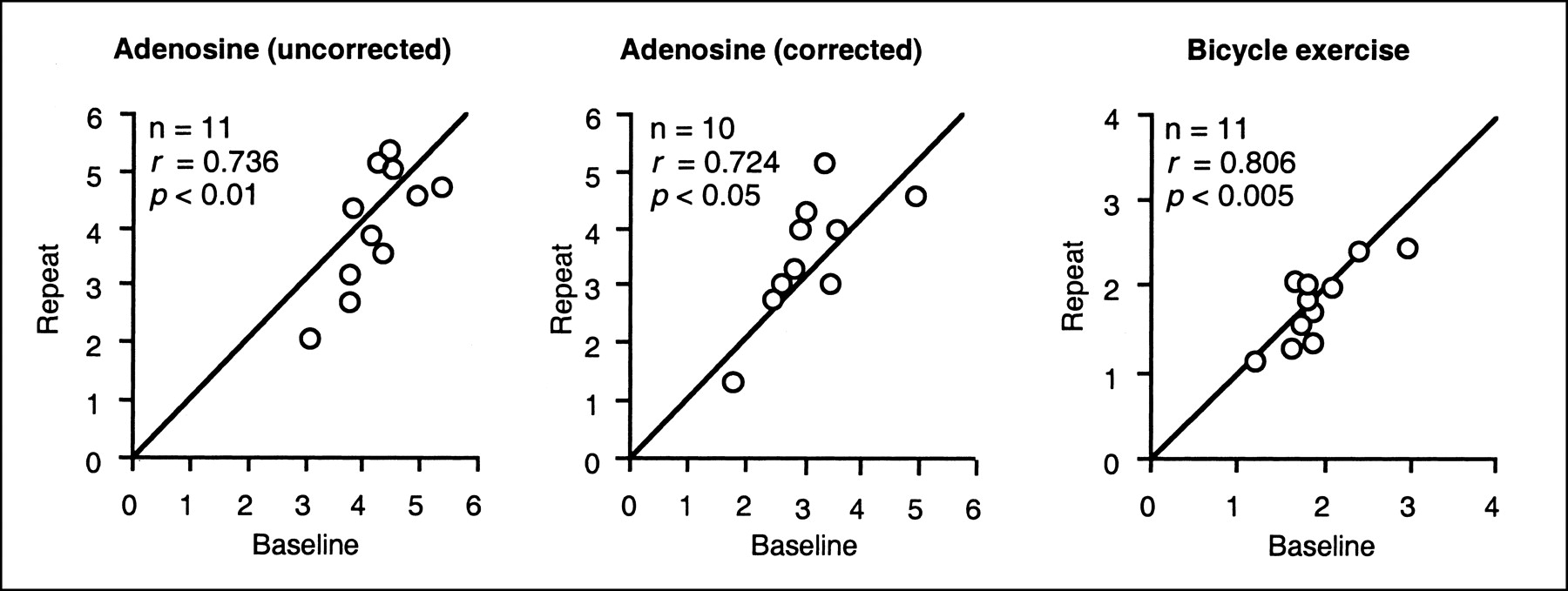
CFR values are summarized in Table 3 and shown in Figures 4 and 5. CFR at the initial adenosine test (MBF for initial adenosine test divided by MBF for initial rest test; relative values) was 4.23 ± 0.62, and CFR at the repeated adenosine test (MBF for repeated adenosine test divided by MBF for repeated rest test) was 4.05 ± 1.06 (mean difference, −5% ± 19%; P = NS). After the resting MBF was corrected for RPP, the respective CFR values were 3.06 ± 0.84 and 3.54 ± 1.09 (mean difference, 13% ± 24%; P = NS). The repeatability coefficient was 1.44 (35%) for CFR and 1.48 (44%) for corrected CFR (Table 3). The values for CFR using bicycle exercise stress were 1.91 ± 0.46 and 1.80 ± 0.44 (mean difference, −5% ± 15%; P = NS), which were significantly lower than the values using adenosine (P < 0.0001). The repeatability coefficient was 0.56 (30%). Generally, the regional CFR values showed considerably lower repeatability than did the global values.
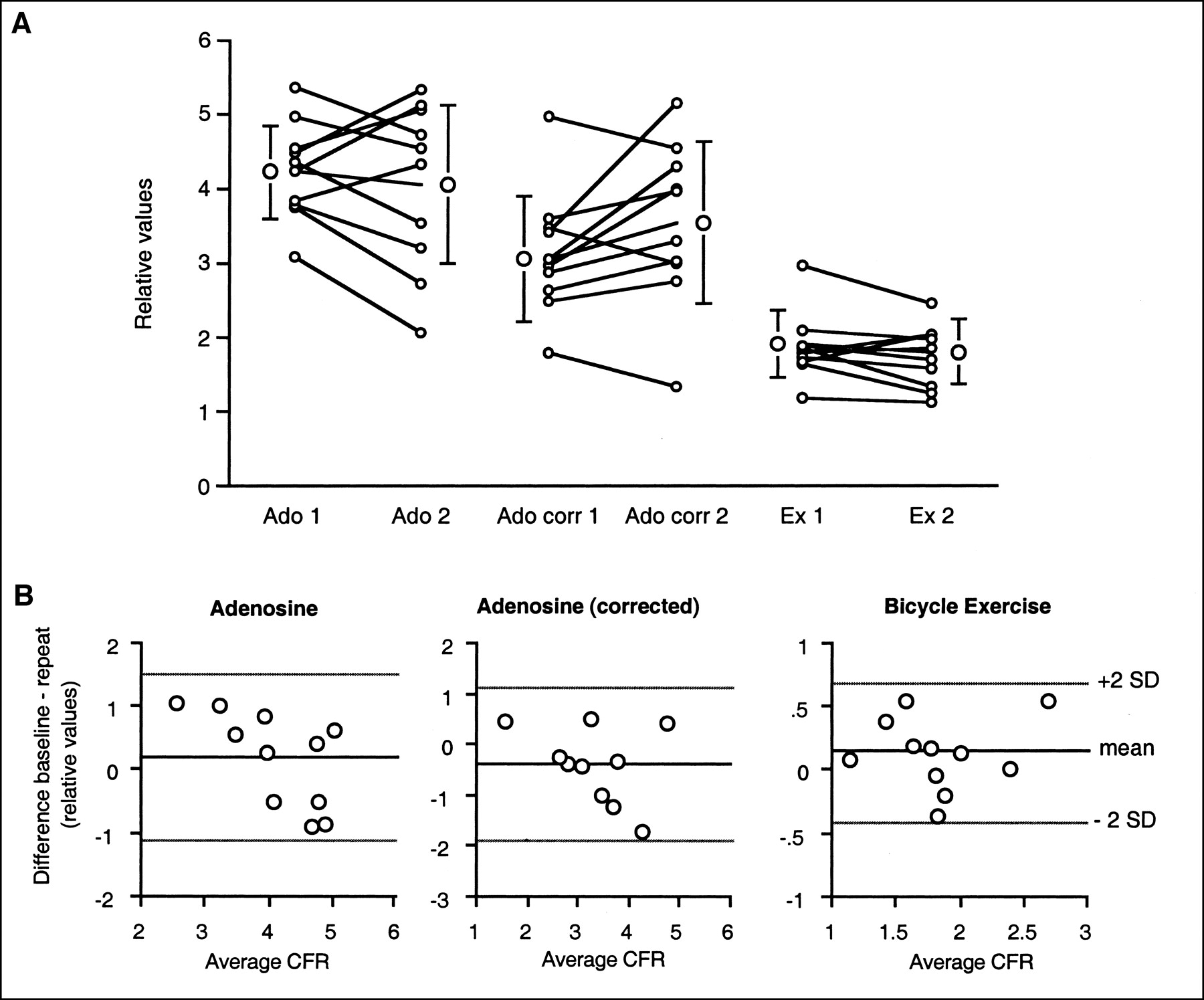
(A) Repeated assessment of CFR with and without correction of baseline MBF for RPP. Paired values are given for each participant. Mean values (large circles) are given as mean ± 1 SD. (B) Differences in paired values are plotted against their average value (Bland-Altman plot). Ado 1 and 2 and Ex 1 and 2 are defined as in Figure 1; corr = corrected.

Scattergram of repeated CFR measurements (relative values). Line of equality, along which points would lie if agreement were perfect, is shown.
Coronary Flow Reserve
Coronary Resistance
Coronary resistance did not differ significantly between the 2 resting measurements (67 ± 10 vs. 69 ± 11 mm Hg/mL/min/g; P = NS) and the 2 respective hyperemic measurements, that is, adenosine stress (17 ± 4 vs. 19 ± 5, P = NS) and bicycle stress (45 ± 13 vs. 50 ± 12). Thus, coronary resistance dropped significantly during bicycle exercise compared with the value during rest (P < 0.001 vs. rest), and showed a further decrease during adenosine stress (P < 0.01 vs. exercise).
DISCUSSION
PET is used increasingly in studies comparing the effect of various pharmacologic interventions on myocardial perfusion. At the same time, little is known about potential interactions between most of the study drugs and adenosine or dipyridamole, both of which are commonly used as pharmacologic hyperemic stressors. The use of physical exercise as a hyperemic stimulus avoids these problems. In addition, bicycle exercise—although performed with the patient supine in the scanner—represents a physiologic stimulus and thus reflects the natural response of MBF to physical activities better than can any isolated pharmacologic stimulation (8–11). Therefore, assessment of the feasibility and repeatability of hyperemic MBF using supine bicycle exercise stress in the PET scanner, and comparison with adenosine-induced hyperemic MBF, are important issues.
For the measurement of global MBF at rest, we found a repeatability coefficient of 0.26 mL/min/g (21% of the average value between the initial and repeated rest measurements), indicating good repeatability for the method and comparing well with our previous data (3). It remains difficult, however, to assign the small difference between the 2 measurements either to an intrinsic error in the measurement (methodologic error) or to real changes in MBF (physiologic variability). Because MBF at rest depends largely on cardiac work, that is, myocardial oxygen consumption, MBF at rest is expected to vary with RPP. To allow comparable interpretation of the quantitative data, some investigators have proposed that MBF be corrected for RPP, an index of external cardiac work (27). This correction did not improve agreement between the 2 measurements in our study, probably because RPP varied only slightly between the initial and repeated rest measurements, underlining the rapid recovery of hemodynamic conditions after adenosine and bicycle exercise stress. However, the recovery time after physical exercise might have been slightly too short in some of the volunteers, although for the sake of the repeatability of our data, we did not aim for the maximal workload.
Regional resting MBF was similar in the 4 left ventricular segments, with a comparable coefficient of variance in all regions. Agreement between repeated measurements in each segment was considerably inferior to agreement between repeated global MBF values. This inferiority could be due partly to methodologic issues, because regions of interest of smaller size have poorer count statistics than do larger regions of interest. In addition, however, the spatial heterogeneity of myocardial perfusion is well accepted (28) and may have influenced our results. Regional variability in perfusion has been observed in the hearts of all species studied thus far (29–31). King et al. (30), for example, found that even after correcting for methodologic error and temporal variability, flow to small regions of the left ventricle of conscious baboons ranged almost 6-fold at the largest extreme. Recently, the issue of heterogeneity of MBF in healthy humans has been extensively discussed (31). Briefly, differences in local metabolic needs, perhaps secondary to differences in regional function, have been suggested. Temporal heterogeneity may cause changing variations within regions (32). Spatial heterogeneity in regional MBF seems to be linked to arteriolar or tissue oxygen partial pressure over a broad range, from 40 to 200 mm Hg in dogs (33). Furthermore, a linear relationship between coronary flow distribution and tissue norepinephrine content may exist (34). Thus, physiologic heterogeneity may considerably contribute to the larger variability in segmental MBF, and temporal variations may at least partly explain the inferior repeatability of regional MBF measurements, compared with global MBF.
The 2 adenosine measurements of global MBF revealed a repeatability coefficient of 1.34 mL/min/g (27% of the mean value), only slightly higher than that observed for resting MBF (21%) and comparing well with previous results (3). Similarly, hyperemic regional MBF showed a higher repeatability coefficient for all left ventricular segments, indicating reduced agreement, compared with rest.
The repeatability coefficient for the 2 exercise measurements was 0.82 mL/min/g (36% of the mean) and, thus, comparable to adenosine stress, although exercise-induced hyperemia was significantly lower than adenosine-induced hyperemia. Several factors may have contributed. First, the volunteers were not asked to perform to their maximal level of effort, in order to allow for (hemodynamic) recovery within a reasonable time as requested by the repeatability study protocol. Second, data were acquired not during exercise (to avoid excessive motion artifacts during scanning) but immediately after exercise, when the workload on the heart and the heart rate rapidly decrease and when flow is also expected to rapidly fall. Thus, the exercise-induced MBF should be considered the MBF after submaximal exercise stress, possibly limiting clinical usefulness. However, the MBF values are quite comparable or even slightly higher than those achieved during dobutamine stress (35,36). In perfusion imaging, dobutamine stress has been shown to provide results that are clinically equivalent to those of adenosine stress (37).
Because MBF during maximal vasodilation depends mainly on coronary driving pressure (i.e., mean coronary artery pressure), we estimated the coronary resistance during hyperemia to account for changes in hemodynamic conditions. In fact, resistance was almost identical during both adenosine-induced hyperemic measurements. Resistance during bicycle exercise was significantly higher but almost identical in the 2 bicycle stress measurements. This finding is in line with previous reports, in which exercise stress in addition to pharmacologic stress was shown to increase coronary vascular resistance, thus significantly decreasing hyperemic MBF and CFR (15). This decrease most likely results from an increase in extravascular compressive forces caused by higher ventricular pressures and contractility during physical stress. In view of the fact that repeated measurements revealed almost identical results after calculation of coronary resistance, it seems appropriate to assume that physiologic heterogeneity may be more important in accounting for the differences in repeated MBF measurements and that methodologic issues are less important.
As a reflection of the repeatability of global MBF measurements at rest and during adenosine stress, the baseline (4.23 ± 0.62) and repeated (4.05 ± 1.06) CFR values were similar (P = NS). However, the repeatability coefficient was 1.48 (36%), indicating variability in the hemodynamic response to adenosine. Correction of resting MBF did not improve the repeatability of CFR, confirming that such correction is not mandatory for intragroup comparisons when hemodynamic parameters such as RPP remain stable (3). The repeatability coefficient for global exercise-induced CFR was 0.56 (30%), indicating that the repeatability of CFR is at least as good with exercise stress as with adenosine.
Studies of regional MBF have demonstrated that the distribution of maximal MBF is extremely heterogeneous (29), resulting in a wide dispersion of CFR (27). Thus, the modest repeatability of regional CFR in our study may be explained mainly by physiologic heterogeneity rather than solely by methodologic issues.
We have previously reported, for a larger number of subjects, that resting MBF was slightly higher in women than in men but that no sex differences existed during hyperemia (31). Thus, although we have not included female volunteers in the present study, one can reasonably anticipate that sex differences would not have significantly changed our results with regard to stress perfusion measurement.
Repetitive MBF measurements in the same patients have been reported by others, albeit usually to compare MBF measurements with different approaches (38,39). In addition, the repeatability of MBF measurements for PET with pharmacologic stress has been reported using water (3) and ammonia (27) as flow tracers.
To our knowledge, the present study is the first to report the feasibility and range of repeatability of bicycle exercise stress for inducing hyperemic MBF in PET with 15O-labeled water. How far apart measurements can be without causing a problem remains a question of judgment for each individual study and clinical setting. Our data also provide information helpful for choosing the sample size of clinical PET studies. The repeatability of PET in patients with heart disease remains to be determined.
CONCLUSION
Assessment of CFR with 15O-H2O and PET using bicycle exercise stress in the PET scanner is feasible and at least as repeatable as using adenosine stress. Our results support the use of bicycle exercise stress in PET as a physiologic stimulus to induce hyperemic flow.
Acknowledgments
We are grateful to Thomas Berthold, head radiographer, for his excellent technical assistance. This study was supported by grant SCORE B 32-55002.98 from the Swiss National Science Foundation, by the EMDO Stiftung Zurich, and by the Radiumfonds für Krebsforschung.
Footnotes
Received May 6, 2002; revision accepted Aug. 28, 2002.
For correspondence or reprints contact: Philipp A. Kaufmann, MD, Nuclear Cardiology, Cardiovascular Center, University Hospital C NUK 32, Raemistrasse 100, CH-8091 Zurich, Switzerland.
E-mail: Philipp.Kaufmann{at}dmr.usz.ch
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- FDA Approval of 18F-Flurpiridaz for PET: Stepping into a New Era of Myocardial Perfusion Imaging?
- Quantitatively Predicting Effects of Exercise on Pharmacokinetics of Drugs Using a Physiologically Based Pharmacokinetic Model
- Effects of Hypercapnia on Myocardial Blood Flow in Healthy Human Subjects
- Absolute Myocardial Blood Flow and Flow Reserve Assessed by Gated SPECT with Cadmium-Zinc-Telluride Detectors Using 99mTc-Tetrofosmin: Head-to-Head Comparison with 13N-Ammonia PET
- Diagnostic Value of 13N-Ammonia Myocardial Perfusion PET: Added Value of Myocardial Flow Reserve
- Quantitative PET Measurements of Myocardial Blood Flow in Young, Healthy Volunteers: What Should We Expect?
- Cardiac PET Imaging for the Detection and Monitoring of Coronary Artery Disease and Microvascular Health
- Long-Term Prognostic Value of 13N-Ammonia Myocardial Perfusion Positron Emission Tomography: Added Value of Coronary Flow Reserve
- The Clinical Value of Myocardial Blood Flow Measurement
- Absolute Quantification of Myocardial Blood Flow with 13N-Ammonia and 3-Dimensional PET
- Repeatability of Cold Pressor Test-Induced Flow Increase Assessed with H215O and PET
- Comparison of 64-Slice CT with Gated SPECT for Evaluation of Left Ventricular Function
- Reproducibility of Measurements of Regional Myocardial Blood Flow in a Model of Coronary Artery Disease: Comparison of H215O and 13NH3 PET Techniques
- Caffeine Decreases Exercise-Induced Myocardial Flow Reserve
- Novel Doppler Assessment of Intracoronary Volumetric Flow Reserve: Validation Against PET in Patients With or Without Flow-Dependent Vasodilation
- Positron Emission Tomography-Measured Abnormal Responses of Myocardial Blood Flow to Sympathetic Stimulation Are Associated With the Risk of Developing Cardiovascular Events
- Comparison of treadmill exercise versus dipyridamole stress with myocardial perfusion imaging using rubidium-82 positron emission tomography
- Assessment of the Long-Term Reproducibility of Baseline and Dobutamine-Induced Myocardial Blood Flow in Patients with Stable Coronary Artery Disease
- Myocardial Blood Flow Measurement by PET: Technical Aspects and Clinical Applications
- Systemic Inhibition of Nitric Oxide Synthase Unmasks Neural Constraint of Maximal Myocardial Blood Flow in Humans
- CT Attenuation Correction for Myocardial Perfusion Quantification Using a PET/CT Hybrid Scanner
- Comparison of Regional Myocardial Blood Flow and Perfusion in Dilated Cardiomyopathy and Left Bundle Branch Block: Role of Wall Thickening
- Influence of Altitude Exposure on Coronary Flow Reserve