


Abstract
The aim of this study was to evaluate the repeatability of endothelium-related myocardial blood flow (MBF) responses to cold pressor testing (CPT) as assessed by PET. Methods: In 10 age-matched control subjects (26.6 ± 3.4 y) and 10 tobacco smokers (24.9 ± 3.3 y) MBF was assessed at rest and after repeated CPT (CPT1 and CPT2, 40 min apart) using PET with H215O. CPT was performed by a 2-min immersion of the subject's foot in ice water. MBF values were corrected for cardiac workload (rate·pressure product), and the repeatability of CPT-related MBF values was assessed according to Bland and Altman. Results: Corrected MBF at CPT1 and CPT2 were comparable in control subjects (1.79 ± 0.37 vs. 1.70 ± 0.35 mL/min/g; P = not significant [NS]) and in smokers (1.97 ± 0.42 vs. 1.80 ± 0.41 mL/min/g; P = NS). Repeatability coefficients in control subjects and smokers were 0.46 mL/min/g (27% of the mean MBF) and 0.51 mL/min/g (27%), respectively. MBF increased significantly after CPT in both groups but tended to be lower in smokers (P = 0.08). Conclusion: PET measured MBF combined with CPT is a feasible and repeatable method for the evaluation of endothelium-related changes of MBF.
Since the first report by Hines and Brown in 1933 (1), cold pressor testing (CPT) has been evaluated in several physiologic, pharmacologic, and clinical studies as a powerful stimulus of sympathetic activity and has been used to examine the sympathetic neural influence on peripheral and coronary circulation (2). It is well established that increased sympathetic activity produces dilatation of coronary resistance vessels and, thus, increases myocardial blood flow (MBF) in healthy volunteers (3,4). Modulation of coronary vascular resistance by the sympathetic neural system is achieved not only by metabolically mediated vasomotor response and circulating neurohormones released in response to sympathetic activation but also by direct innervation through cardiac postganglionic neural axons (3,5,6). The coronary vascular response to sympathetic activation is strongly dependent on the functional integrity of the endothelium and nitric oxide (NO)-regulated vasodilatation. This response can be altered to produce reduced coronary vasodilation or even vasoconstriction in patients with coronary artery disease (4,7–11). Thus, CPT is a useful technique to assess coronary endothelial dysfunction.
Quantitative regional MBF can be measured noninvasively and accurately using PET with H215O (12–15). This allows assessment of hyperemic MBF response to various stimuli as an integrated parameter of coronary vasodilation and vascular smooth muscle relaxation (16–18). Adenosine and dipyridamole are commonly used as pharmacologic hyperemic stimuli, leading mainly to endothelium-independent vasodilation of the coronary circulation. In contrast to these vasodilators, the coronary vascular response to CPT most likely reflects endothelium-dependent coronary vasodilation (19–21). Several reports have been published using CPT as a sympathetic stimulus in healthy volunteers and patients with cardiovascular risk factors, yielding a good correlation of angiographically established flow-dependent dilation and MBF measured by PET (22–24). However, the repeatability of CPT for the evaluation of endothelial function using PET still remains to be established. The aim of the present study was to evaluate the repeatability of endothelium-related MBF responses to CPT as assessed by PET.
MATERIALS AND METHODS
Study Population
Ten healthy volunteers (mean age, 26.6 ± 3.4 y) and 10 tobacco smokers (mean age, 24.9 ± 3.3 y) were consecutively enrolled in our study within 3 mo. Three subjects in the control group and 4 in the smoker group were female. None of the study participants had a history of cardiovascular or peripheral neural disease. Inclusion criteria were a normal resting electrocardiogram (ECG), normal heart rate and normal blood pressure, and an unremarkable excursive cardiopulmonary examination. Study participants reported a cumulative exposure to tobacco smoke of 4.8 ± 2.2 packyears (number of packs smoked per day × duration of smoking status in years) and were asked to refrain from smoking for 4 h before the study as previously suggested (25,26). Validation of self-reported smoking status was achieved by measurement of urine cotinin levels (averaging 1,620 μg/L in smokers, with a cutoff at <499 μg/L) and fractions of CO-hemoglobin (FCOHb) in a venous blood sample as previously reported (27,28). All female study participants had a negative urine pregnancy test. The study protocol was approved by the local institutional review board and all subjects gave written informed consent before enrollment in the study.
Study Protocol
First, MBF was measured at rest. After allowing for decay of H215O, MBF was measured during immersion of the left foot in ice water (CPT1). The subject's foot was submerged in a container filled with 4°C ice water up to the level of the ankle for 2 min and, thereafter, was withdrawn from the ice water container. The infusion of H215O and the PET sequence were initiated 1 min into the foot immersion (29).
Repeated exposure to severe cold can activate adaptive mechanisms characterized by a diminution of the sympathetic response and, therefore, substantially compromise repeatability of the vascular response to CPT (30). Therefore, after a deconditioning period of 40 min, measurement was repeated with immersion of the opposite (right) foot in ice water (CPT2) with the identical protocol.
Image Acquisition
PET image acquisition was performed in the PET Center of the University Hospital of Zurich on an Advance scanner (GE Healthcare). This device records 35 image planes simultaneously in 2-dimensional mode. The axial field of view is 14.5 cm. A 30-min blank scan was recorded as part of the daily routine. In the 40-min interval between CPT1 and CPT2, a 20-min transmission scan using an external 68Ge source was performed for attenuation correction. Starting after the background frame, a dose of 500–700 MBq of H215O was injected as an intravenous bolus over 20 s at an infusion rate of 24 mL/min to assess MBF. The dynamic image sequences obtained were 14 × 5 s, 3 × 10 s, 3 × 20 s, and 4 × 30 s.
Image Processing
The sinograms obtained were corrected for attenuation and were reconstructed on a dedicated workstation (Sun Microsystems) using standard reconstruction algorithms. Images were analyzed with a pixel-wise modeling software developed at our institution (PMOD Technologies Ltd.). Myocardial images were then generated directly from the dynamic H215O study, avoiding the need for additional C15O blood-pool scans to define regions of interest as previously reported (12,31). Factor images were generated by iterative reconstruction. After reorienting the factor images along the heart axis to form vertical long-axis, horizontal long-axis, and short-axis-slices, regions of interest were drawn within the left ventricle on 4–6 consecutive image planes and were projected both onto the dynamic H215O images, to generate blood time–activity curves (input function), and onto the right ventricle, to correct for spillover in the septum. Similarly, myocardial regions of interest were drawn on the short-axis slices within the left ventricular myocardium on at least 12 consecutive image planes and were projected onto the dynamic H215O images to obtain tissue activity curves. The junctions of right and let ventricle were marked to indicate the septum. The left ventricular free wall was then subdivided geometrically into 3 segments of the same size. In accord with the recommendations of the American Heart Association (32), the left ventricle was further subdivided into a total of 16 segments. However, for the present analysis, the subsegments were grouped to obtain a mean value of global wall perfusion. Arterial and tissue activity curves were fitted to a single-tissue-compartment tracer kinetic model to give values of regional and global MBF (mL/min/g), as previously described (33).
Data Interpretation
Mean values of global MBF are given in mL/min/g myocardium. Because MBF at rest and after sympathetic stimulation is strongly determined by cardiac workload, we corrected MBF values for its corresponding rate·pressure product (RPP) using the following equation: Corrected MBF = (MBF/RPP) × 104. To compare the increase in MBF after both CPTs, the respective differences of MBF at CPT and at rest were calculated and expressed as the percentage of the MBF at rest, both for uncorrected and RPP-corrected values.
Statistical Analysis
Numeric values are given as mean ± SD. Statistical comparison of MBF values was performed using the Student t test. P values < 0.05 were considered statistically significant. Comparison of MBF values was performed using linear regression analysis. To evaluate the repeatability of each measurement, the repeatability coefficient was calculated as 1.96 times the SD of the differences as proposed by Bland and Altman (34) and adopted by the British Standards Institution.
RESULTS
All CPT procedures were well tolerated and no subjects were withdrawn from the analysis. None of the subjects experienced any significant ECG changes or intolerable alterations of blood pressure.
Pooled Hemodynamic Data
Pooled hemodynamic data are shown in Table 1. The RPP increased significantly after CPT1 and CPT2 and both RPP values were comparable (P = not significant [NS]). A good correlation of pooled RPP values was found (r = 0. 95, P < 0.0001, standard error of the estimates (SEE) = 444 mm Hg × bpm). Bland–Altman analysis yielded a repeatability coefficient of 1,051 mm Hg × bpm (13% of the mean RPP).
Hemodynamics
Hemodynamics in Control Subjects and Smokers
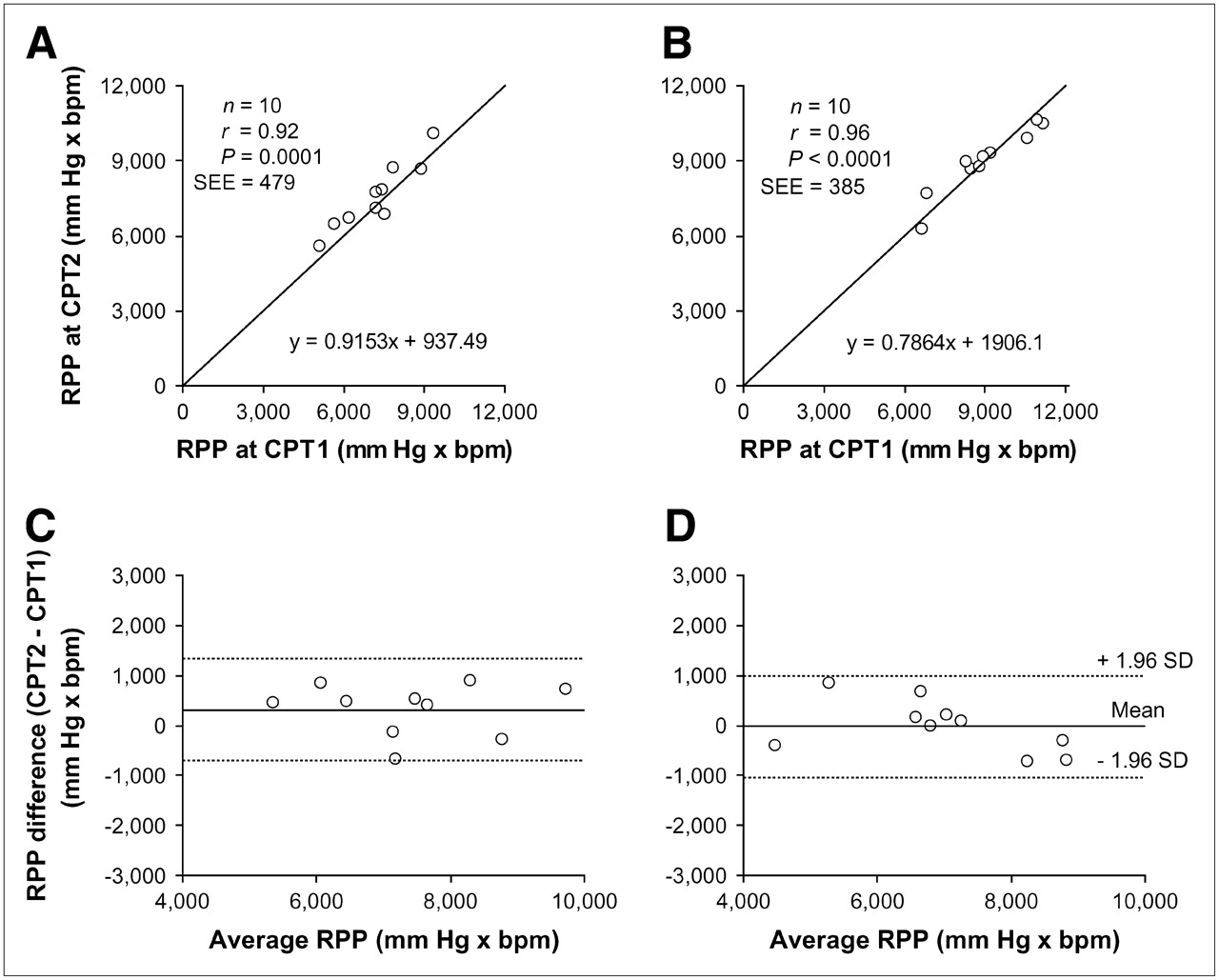
Hemodynamic variables in control subjects and smokers are provided in Table 1. The RPP increased significantly at CPT1 and CPT2 compared with rest in control subjects and smokers. Furthermore, the CPT-induced increase in RPP was similar at CPT1 and CPT2 in both groups (P = NS), although there was a trend toward a lower RPP increase after CPT2 in smokers. At rest, RPP values were comparable in both groups. After CPT, however, when data from both CPTs was averaged, we found higher RPP values in smokers compared with control subjects (11,089 ± 2,663 vs. 9,247 ± 1,287 mm Hg × bpm; P = 0.008). The correlation between RPP values at CPT1 and CPT2 was excellent in control subjects (r = 0.92, P = 0.0001, SEE = 479 mm Hg × bpm) and in smokers (r = 0.96, P < 0.0001, SEE = 385 mm Hg × bpm) (Fig. 1). The repeatability of RPP values was excellent (repeatability coefficient: 1,014 mm Hg × bpm [14% of mean RPP] in control subjects and 1,029 mm Hg × bpm [11%] in smokers) (Fig. 1).

Linear regression analysis of RPP values at CPT1 and CPT2 in control subjects (A) and smokers (B). Line of identity is given in both graphs. Differences in RPP in control subjects (C) and smokers (D) after repeated CPT are plotted against their average values (Bland–Altman-plot). 1.96 SD denotes repeatability coefficient. Mean denotes mean of differences.
Pooled MBF Data
Global MBF increased significantly after CPT1 and CPT2 with and without correction, reaching comparable values (Table 2). Accordingly, a good correlation among repeated measurements for uncorrected MBF values (r = 0.81, P < 0.0001, SEE = 0.18 mL/min/g) and corrected MBF values (r = 0.80, P < 0.0001, SEE = 0.22 mL/min/g) was found (Fig. 2). The regression line intercepts did not differ from zero (P = NS). The repeatability coefficients were 0.41 mL/min/g (28% of mean MBF) and 0.48 mL/min/g (26%), respectively, for uncorrected and corrected MBF (Fig. 2).
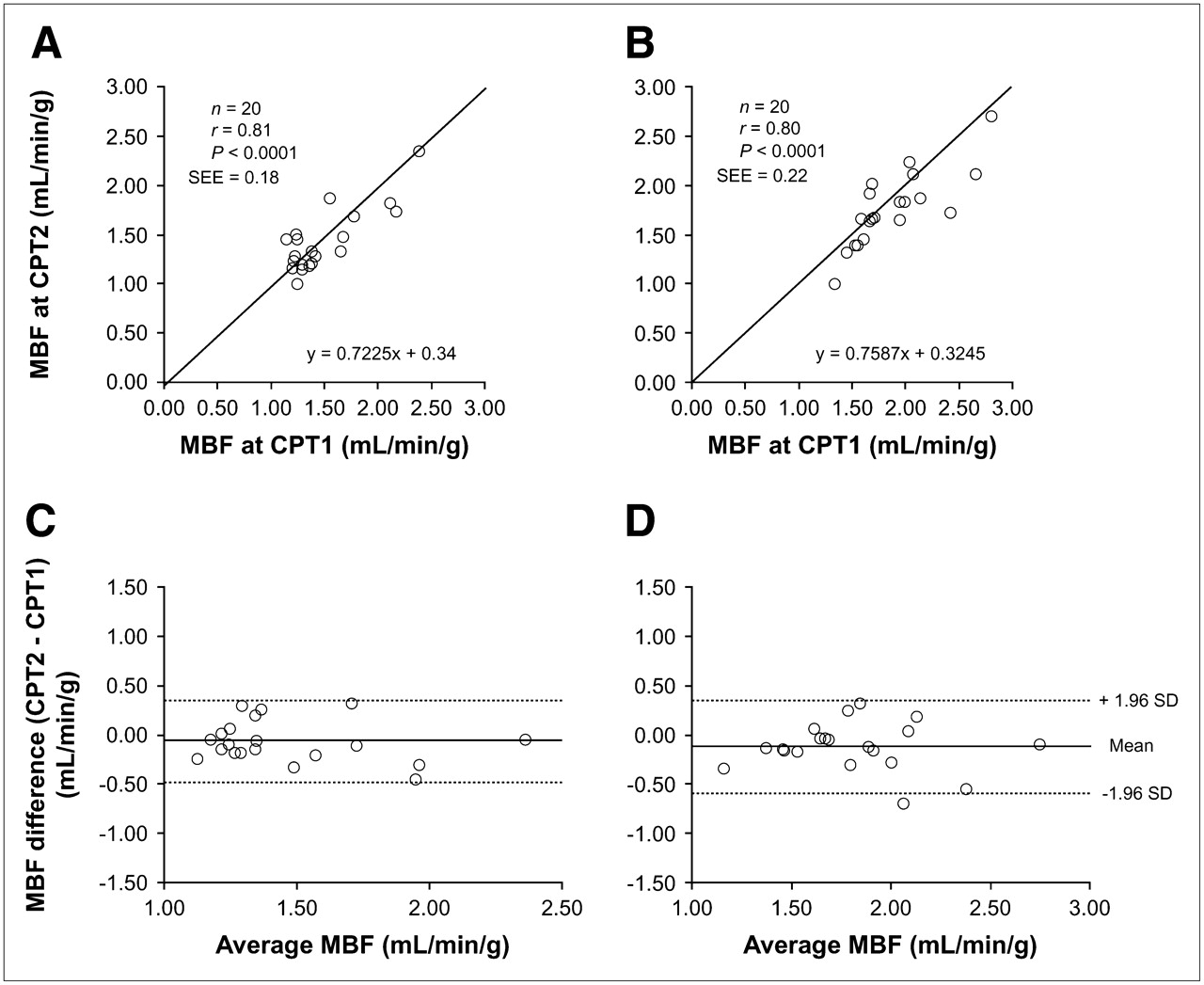
Linear regression analysis of pooled global uncorrected MBF (A) and RPP-corrected MBF (B) at CPT1 and CPT2. Line of identity is given in both graphs. Differences in pooled global uncorrected MBF (C) and RPP-corrected MBF (D) after repeated CPT are plotted against their average values (Bland–Altman-plot). Mean denotes mean of differences; 1.96 SD denotes repeatability coefficient.
Global MBF values
MBF in Control Subjects and Smokers
Global MBF values are shown in Table 2. Uncorrected MBF increased significantly after both CPTs in control subjects and in smokers. Similarly, corrected MBF was elevated after CPT1 and CPT2 compared with rest, although the increase in MBF after CPT2 in smokers fell short of statistical significance (P = 0.08). The absolute and relative increase in MBF (ΔCPT) was comparable after CPT1 versus CPT2 within both groups (P = NS). For corrected values the averaged relative increase after both CPTs tended to be lower in smokers versus control subjects (P = 0.08). Bland–Altman plots revealed a repeatability coefficient of 0.39 mL/min/g (31% of mean MBF) for control subjects and 0.41 mL/min/g (24%) for smokers for uncorrected values. After correction for cardiac workload, the respective values were comparable—that is, 0.46 mL/min/g (27%) for control subjects and 0.51 mL/min/g (27%) for smokers. Correlation coefficients are given in Figure 3. The regression line intercepts did not differ from zero (P = NS).
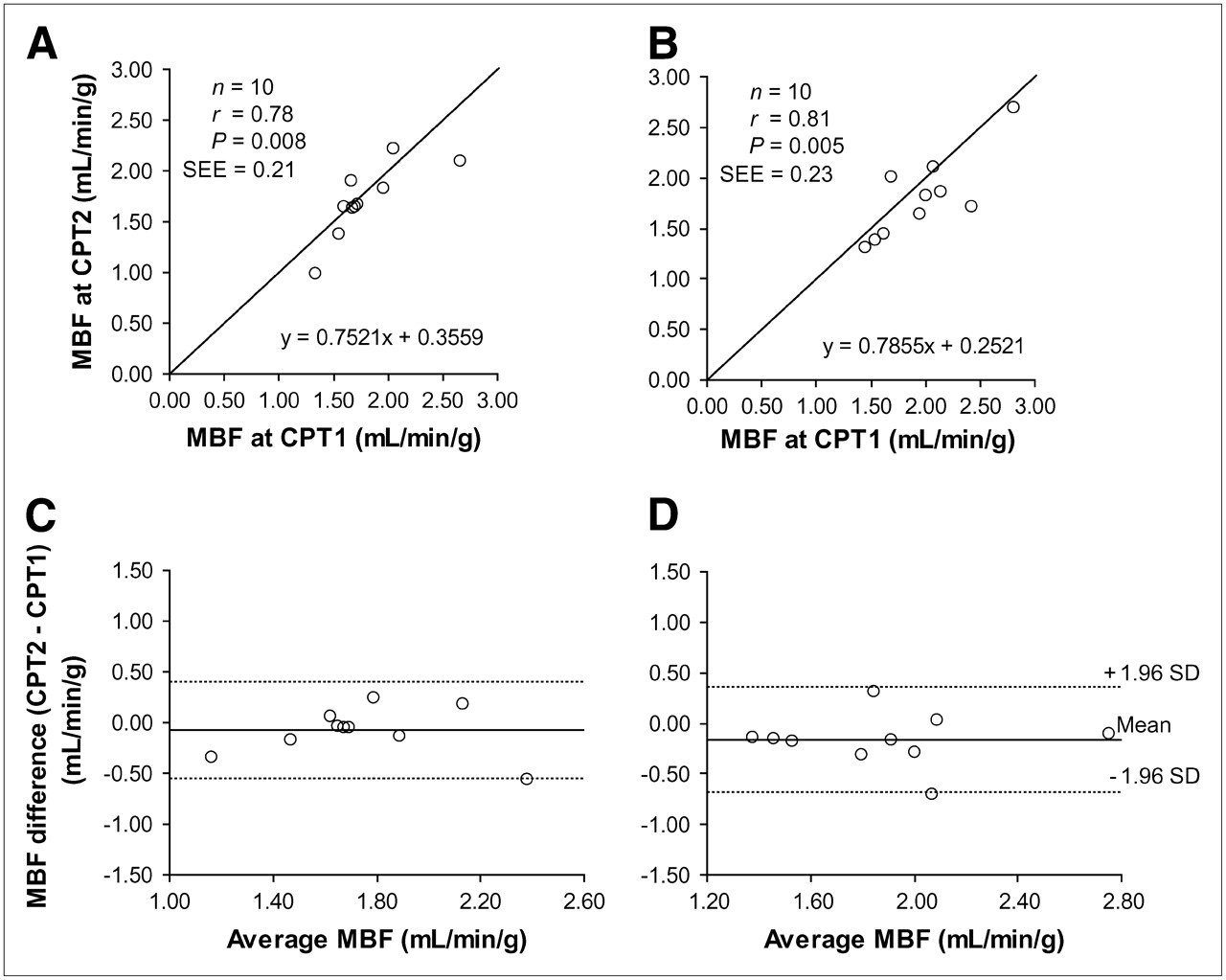
Linear regression analysis of global RPP-corrected MBF at CPT1 and CPT2 in control subjects (A) and smokers (B). Line of identity is given in both graphs. Differences in global RPP-corrected MBF in control subjects (C) and smokers (D) after repeated CPT are plotted against their average values (Bland–Altman-plot). Mean denotes mean of differences; 1.96 SD denotes repeatability coefficient.
DISCUSSION
The results of the present study show a good repeatability of CPT-induced changes in hemodynamics and MBF in healthy young individuals and in young tobacco smokers. The increase in absolute MBF induced by CPT in control subjects (0.35 mL/min/g) compares very well with the values reported by Campisi et al. (26) (0.28 mL/min/g) and Schindler et al. (35) (0.32 mL/min/g), although we used radiolabeled water while the latter used ammonia as tracer. The flow increase induced by CPT in smokers proved as reproducible as that in healthy volunteers, whereas the observed MBF increase in smokers was slightly higher than that observed in the literature (25,26), most likely due to the younger age of smokers in our study and their relatively lower total exposure to smoking. Nevertheless, the percentage increase in RPP-corrected MBF tended to be lower in smokers, although this finding fell short of statistical significance (Fig. 4).

Average percentage increase in MBF at CPT1 and CPT2 in control subjects and smokers.
Interestingly, smokers started with higher resting MBF values and reached higher CPT-related MBF values, most likely indicating a substantially higher baseline sympathetic activity in smokers, as substantiated by the higher RPP in the latter group. Our observation of a higher resting RPP is in line with previous reports (25,26) and might be explained by the fact that discontinuation of smoking for 4 h before inclusion in the study—as suggested by previous studies (25,26)—might have been an insufficient interval. In fact, nicotine evokes the release of catecholamines with subsequent adrenergically mediated increase in cardiac work and MBF (36).
Although not yet completely understood, several mechanisms appear to contribute to the coronary vasomotor response associated with CPT. The metabolically mediated flow increase after CPT is an important determinant of coronary vasomotor response to sympathetic activation. It is the result of increased myocardial oxygen demand secondary to elevated heart rate and contractility. This notion is supported by our data showing a significantly lower MBF response when correcting for RPP. Nevertheless, repeatability was preserved after correction, underlining the repeatability of the test. In the normal coronary circulation the metabolically mediated flow increase is associated with flow-mediated endothelium-dependent vasodilation of the coronary arteries (4,10,22). Several observations support the validitiy of noninvasively measured changes in MBF after CPT as indicators of endothelium-dependent coronary vasomotion. For example, CPT-induced changes in coronary blood flow correlate with changes in invasive flow measurements in response to intracoronary acetylcholine administration (10), an endothelium-dependent vasodilator. Furthermore, changes in the diameter of epicardial conduit vessels after CPT correlate with cold-induced changes in MBF assessed with PET, underlining the validity of the test (22). Finally, intravenous administration of l-arginine, the substrate of NO synthase, increases the bioavailability of NO and restores the myocardial flow response after CPT in long-term smokers (26). In addition to the metabolically mediated flow response to CPT, there is substantial evidence of a direct involvement of adrenergic neurons in coronary vasomotor tone (3). During sympathetic activation after acute cold exposure, the α-adrenergically mediated coronary vasoconstriction is, in a healthy individual, offset by flow-mediated endothelium-dependent vasodilator response, whereas this vasoconstrictor effect is largely unopposed in the presence of endothelial dysfunction (22).
Independent of the exact mechanisms in the pathogenesis of abnormal endothelium-dependent vasomotion, the prognostic implications associated with this condition have prompted a search for clinically practicable diagnostic methods for the evaluation of endothelial function (37). Unfortunately, most diagnostic procedures published in experimental or clinical trials—such as direct intracoronary administration of acetylcholine, quantitative coronary angiography, or intracoronary Doppler flow measurements (38)—are not suitable for wide clinical application because of their invasive nature and the substantial risk of procedure-related morbidity. PET using H215O is a widely established method for the noninvasive evaluation of MBF avoiding the risks inherent with invasive testing. Our study shows that assessment of endothelium-dependent coronary vasomotion using CPT as the sympathetic stimulus and PET-measured MBF as the diagnostic tool provide consistent results comparing well with the repeatability previously reported for pharmacologic (12,15,39) and bicycle exercise stress (13). This confirms the important role of CPT in the diagnostic algorithms applied to patients with suspected endothelial dysfunction. In addition, our results now may provide a ground on which sample size calculations for future studies can be based. It remains a question of judgment for each clinical and individual setting which repeatability limits are required to provide acceptable and meaningful results. However, our data are confined to short-term repeatability. Although long-term repeatability may be affected by day-to-day variability of biologic and hemodynamic parameters, this was beyond the scope of this study and remains to be determined.
We do not report on the repeatability of regional values. However, CPT is a test most commonly used for assessing endothelial dysfunction in patients who have presumably not yet developed stenotic lesions. Accordingly, segmental analysis may not be the primary aim of this technique and, thus, the present study was powered to assess global and not segmental analysis. Another limitation was the relatively low cumulative exposure to tobacco smoke in the smoker group. Part of the study design was to test the reproducibility of CPT-induced MBF response using PET in individuals with suspected pathologic endothelium-dependent vasoreactivity. For this purpose, subjects with an ongoing history of tobacco smoking were chosen. However, to obtain data from age-matched smokers, a young population was chosen and therefore the burden of exposure to smoking was limited. This short duration may have contributed to the fact that only a modest impairment of endothelium-dependent vasoreactivity was found, which fell short of statistical significance, and therefore the study was not designed to detect very small differences in MBF as this was not the aim of the present study.
Furthermore, validation of self-reported smoking status by measurements of urine cotinine levels and blood FCOHb was only performed in the smoker group and not in the control group. Therefore, the nonsmoking status in the control group could not be validated in an objective manner.
CONCLUSION
Our study documents the repeatability of hemodynamic and MBF changes to CPT. Thus, PET-measured MBF combined with CPT allows the noninvasive assessment of endothelium-related coronary vasomotor function.
Acknowledgments
This study was supported by a grant from the Swiss National Science Foundation (professorship grant PP00A-68835). We are grateful to Ratko Milovanovic for his excellent technical support as radiographer.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication February 25, 2006.
- Accepted for publication June 12, 2006.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prognostic Value of Quantitative Metrics From Positron Emission Tomography in Ischemic Heart Failure
- Myocardial Blood Flow and Coronary Flow Reserve During 3 Years Following Bioresorbable Vascular Scaffold Versus Metallic Drug-Eluting Stent Implantation: The VANISH Trial
- Absolute Myocardial Blood Flow and Flow Reserve Assessed by Gated SPECT with Cadmium-Zinc-Telluride Detectors Using 99mTc-Tetrofosmin: Head-to-Head Comparison with 13N-Ammonia PET
- Impairment of Coronary Flow Reserve Evaluated by Phase Contrast Cine-Magnetic Resonance Imaging in Patients With Heart Failure With Preserved Ejection Fraction
- The effects of cold and exercise on the cardiovascular system
- Diagnostic Value of 13N-Ammonia Myocardial Perfusion PET: Added Value of Myocardial Flow Reserve
- Endothelial Dysfunction in Systemic Lupus Erythematosus: Evaluation with 13N-Ammonia PET
- Cardiac PET Imaging for the Detection and Monitoring of Coronary Artery Disease and Microvascular Health
- Long-Term Prognostic Value of 13N-Ammonia Myocardial Perfusion Positron Emission Tomography: Added Value of Coronary Flow Reserve
- The Clinical Value of Myocardial Blood Flow Measurement
- Olmesartan, But Not Amlodipine, Improves Endothelium-Dependent Coronary Dilation in Hypertensive Patients
- Smoking Cessation Normalizes Coronary Endothelial Vasomotor Response Assessed with 15O-Water and PET in Healthy Young Smokers