


Abstract
Although physical exercise is the preferred stimulus for cardiac stress testing, pharmacologic agents are useful in patients who are unable to exercise. Previous studies have demonstrated short-term repeatability of exercise and adenosine stress, but little data exist regarding dobutamine (Dob) stress or the long-term reproducibility of pharmacologic stressors in coronary artery disease (CAD) patients. PET allows accurate, noninvasive quantification of myocardial blood flow (MBF) and coronary flow reserve (CFR). The aim of the study was to investigate the long-term reproducibility of Dob stress on MBF and CFR in CAD patients using PET. Methods: Fifteen patients with chronic stable angina and angiographically proven CAD (>70% stenosis in at least 1 major coronary artery) underwent PET with 15O-labeled water and Dob stress at baseline (time [t] = 0) and after 24 wk (t = 24). MBF at rest and MBF during Dob stress were calculated for the whole left ventricle, the region subtended by the most severe coronary artery stenosis (Isc), and remote myocardium subtended by arteries with minimal or no disease (Rem). Reproducibility was assessed using the Bland-Altman (BA) repeatability coefficient and was also expressed as a percentage of the mean value of the 2 measurements (%BA). Results: Dob dose (30 ± 11 vs. 031 ± 11 μg/kg/min; P = not significant [ns]) and peak Dob rate·pressure product (20,738 ± 3,947 vs. 20,047 ± 3,455 mm Hg × beats/min; P = ns) were comparable at t = 0 and t = 24. There was no significant difference in resting or Dob MBF (mL/min/g) between t = 0 and t = 24 for the whole left ventricle (1.03 ± 0.19 vs. 1.10 ± 0.20 and 2.02 ± 0.44 vs. 2.09 ± 0.57; P = ns for both), Isc (1.05 ± 0.24 vs. 1.10 ± 0.26 and 1.79 ± 0.53 vs. 1.84 ± 0.62; P = ns for both), or Rem (1.03 ± 0.23 vs. 1.10 ± 0.26 and 2.27 ± 0.63 vs. 2.26 ± 0.63; P = ns for both) territories. Global (1.98 ± 0.40 vs. 1.90 ± 0.46; P = ns) and regional CFR (Isc: 1.65 ± 0.40 vs. 1.67 ± 0.47, and Rem: 2.25 ± 0.57 vs. 2.06 ± 0.51; P = ns) were reproducible. The BA repeatability coefficients (and %BA) for MBF in ischemic and remote territories were 0.3 (28%) and 0.26 (24%) at rest and 0.49 (27%) and 0.58 (26%) during Dob stress. Conclusion: In patients with clinically stable CAD, Dob induces reproducible changes in both global and regional MBF and CFR over a time interval of 24 wk. The reproducibility of MBF and CFR with Dob was comparable with the short-term repeatability reported for adenosine and physical exercise in healthy subjects.
Evaluation of regional myocardial blood flow (MBF) with radionuclide and echocardiographic techniques plays an important role in the diagnosis and management of coronary artery disease (CAD). Physical exercise serves as the optimal physiologic stimulus for myocardial hyperemia, but in patients who are unable to exercise, pharmacologic stressors such as dobutamine (Dob) or adenosine offer an alternative. Dob is a synthetic sympathomimetic amine that acts via cardiac adrenergic receptors to stimulate positive inotropic and chronotropic effects, thereby increasing cardiac work and myocardial oxygen demand to effect a corresponding increase in MBF (1,2). In contrast, adenosine induces near-maximal coronary vasodilatation primarily via activation of specific adenosine A2A receptors in vascular smooth muscle and, thus, hyperemia is independent of metabolic demand (3).
In assessing ischemic heart disease, studies have used several surrogate markers for therapeutic efficacy, including ST segment shift, coronary collateral density, left ventricular function, and semiquantitative assessment of regional MBF. With the advent of more novel therapies, including angiogenic gene therapy, a more physiologically robust endpoint is needed to discriminate between small changes in regional myocardial perfusion (4). Several techniques have been advocated to measure this effect, but all suffer from fundamental limitations. Doppler flow wires only assess epicardial artery flow velocity, coronary angiography cannot visualize vessels <0.5 mm, myocardial contrast echocardiography is operator dependent, and conventional nuclear perfusion scintigraphy is limited by semiquantitative data.
Coronary microcirculatory function can only be tested indirectly by measuring parameters such as MBF and the coronary flow reserve (CFR) (5). PET is the only noninvasive technique that has been validated to provide accurate measurements of absolute regional MBF in humans in vivo (6). CFR, the ratio of hyperemic to baseline MBF, is an integrated parameter of whole coronary circulation. In patients with CAD, CFR provides insight into the functional significance of a coronary stenosis and, in the absence of angiographically detectable CAD, is an index of the integrity of the coronary microcirculation. PET has been widely used to assess CFR in healthy volunteers (7,8) and in patients with CAD (9) and to assess the effect of pharmacologic interventions such as α- (10) and β-blockade (11) and coronary angioplasty (12).
Vasodilator agents are comparatively short acting and have been shown to have good short-term reproducibility, a property useful in serial consecutive measurements of MBF before and after pharmacologic or therapeutic interventions during the same study session (13). In contrast, the reproducibility of Dob stress has not been extensively studied. In the short-term, this measure is influenced by the comparatively long half-life of the drug as compared with adenosine, but this property will not affect assessment of long-term reproducibility. Little data exist regarding the long-term reproducibility of any pharmacologic stress agents.
Although vasodilators are probably more efficient stressors, the mechanism of Dob hyperemia better mimics physical exercise and arguably provides more relevant insight into the effects of CAD on the coronary circulation. Therefore, we proposed to quantify the long-term reproducibility of resting and Dob-induced hyperemic MBF and CFR measured by PET in patients with stable CAD.
MATERIALS AND METHODS
Patient Population
Fifteen patients were recruited from St. Mary’s and Hammersmith Hospitals in London and followed for 24 wk for the study. The patients represented part of a placebo control arm of a randomized clinical study assessing pharmacologic intervention in chronic stable angina. Baseline demographics are provided in Table 1. All patients described at least a 3-mo history of chronic stable angina and demonstrated electrocardiographic (ECG) evidence of exercise-induced myocardial ischemia defined as ≥1 mm of horizontal or downsloping ST segment depression. The presence of significant CAD, defined as luminal stenosis of >50% in at least 1 major coronary artery, was confirmed by coronary angiography. Four patients had multivessel disease, but no patient with significant disease in all 3 major vessels was included in this study. Exclusion criteria included a recent history (<3 mo) of myocardial infarction or unstable angina, inability to undergo exercise tolerance testing (ETT), or resting ECG patterns that would interfere with interpretation of ST changes during exercise.
Characteristics of Patient Population Enrolled in Study
The study protocol was approved by the Research Ethics Committee of Hammersmith and St. Mary’s Hospitals, and radiation exposure was licensed by the U.K. Administration of Radioactive Substances Advisory Committee. All subjects gave informed and written consent before the study
Study Design
MBF by PET was measured under resting conditions and during peak Dob stress on 2 occasions: at baseline (time [t] = 0) and at study completion, after 24 wk (t = 24). Angina class (Canadian Cardiovascular Society [CCS]) was scored and ETT was performed following a standard Bruce protocol both at baseline and at study completion. All PET scans were standardized for time of day and fasting state and all antianginal medication was omitted on the day of study.
PET Study Protocol
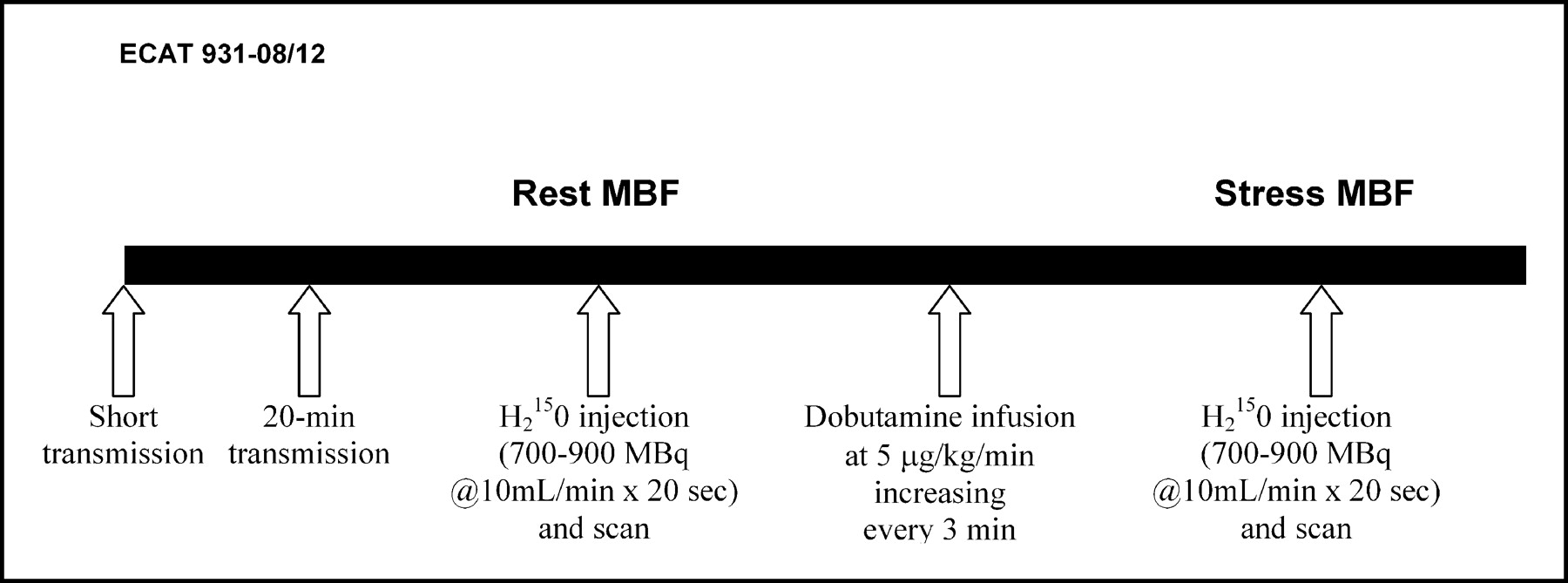
Scanning (Fig. 1) was performed at the Medical Research Council Clinical Sciences Centre, Hammersmith Hospital, London, with an ECAT 931-08/12 fifteen-slice tomograph (CTI/Siemens) giving a 10.5-cm axial field of view. All emission and transmission data were reconstructed using a Hanning filter with a cutoff frequency of 0.5 unit of the reciprocal of the sampling interval of the projection data, resulting in an axial resolution of 6.6 mm and a transaxial image resolution of 8.5-mm full width at half maximum.
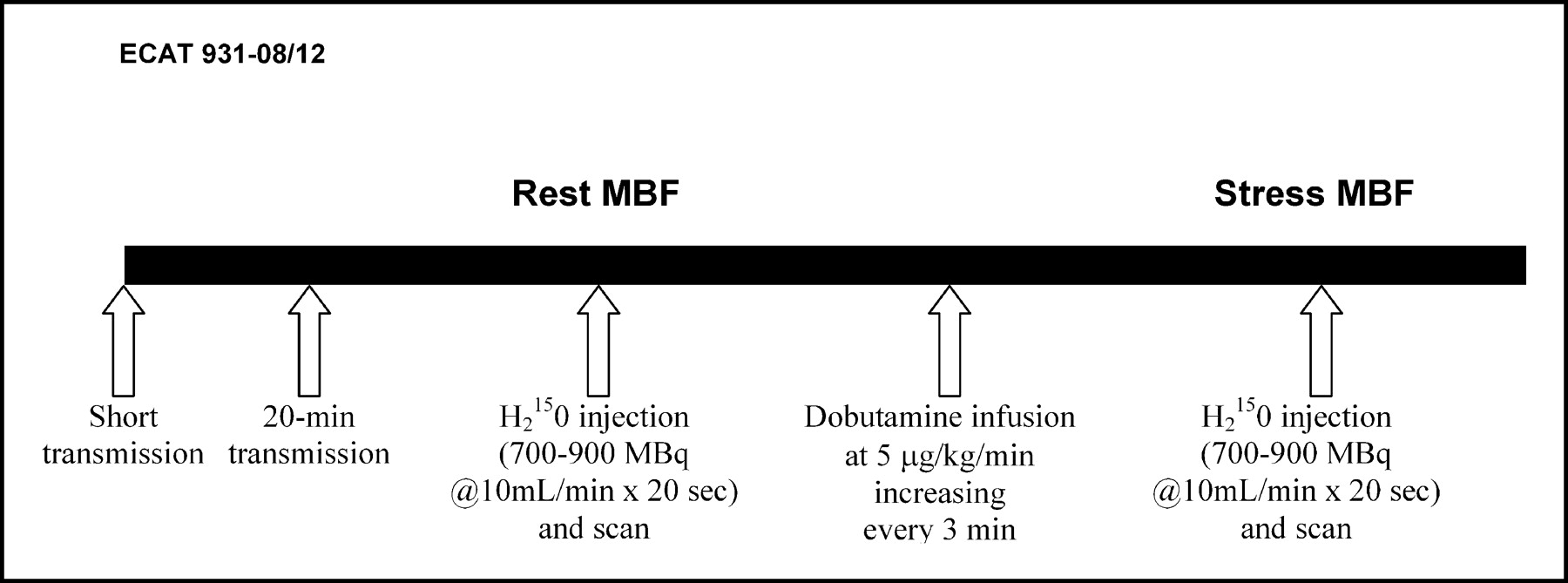
Study protocol used for measurement of MBF using H215O and PET (ECAT 931-08/12 scanner) at rest and during Dob hyperemia, performed at baseline (t = 0) and repeated after 24 wk (t = 24).
Subjects lay supine in the scanner and the optimal imaging position was determined by a 5-min rectilinear scan after the exposure of an external 68Ge ring source. A 20-min transmission scan was then acquired for the purpose of attenuation correction of all subsequent emission scans. 15O-Labeled water ([H215O]; 700–900 MBq) was injected as an intravenous bolus over 20 s at an infusion rate of 10 mL/min for measurement of MBF. Ten minutes after measurement of baseline MBF, to allow for decay of 15O radioactivity, another scan was carried out during Dob stress, which was administered using a standard clinical protocol of incremental dosing. Infusion commenced at 5 mg/kg/min, increasing every 3 min to 10, 15, 20, 30, and 40 mg/kg/min or until the onset of chest pain or ischemic ECG signs or if a fall in systolic pressure >20 mm Hg occurred. A single dose of intravenous atropine (600 mg) was administered to those subjects in whom heart rate did not increase >100 bpm at 40 mg/kg/min. PET acquisition was timed to commence when a steady state was achieved at the maximal tolerated Dob dose. Cardiac rhythm was monitored continuously throughout the procedure. Blood pressure was recorded by an automatic cuff sphygmomanometer (Dynamap) at 1-min intervals, and a 12-lead ECG was recorded at baseline and every 2 min during Dob administration.
PET Data Analysis
PET data analysis was performed by a single operator before disclosure of blinded angiographic findings. The sinograms obtained were corrected for attenuation and reconstructed on a MicroVax II computer (Digital Equipment Corp.) using dedicated array processors and standard reconstruction algorithms. Images were transferred to a SUN SPARC 2 workstation (Sun Microsystems) and analyzed with dedicated software (MATLAB; the MathWorks Inc.). Myocardial images, for the definition of regions of interest (ROIs), were generated directly from the dynamic H215O, as previously reported (14). Briefly, the creation of factor sinograms requires estimates of vascular (right and left heart) and myocardial tissue time-activity curves (14). Factor images describing tissue and blood distributions were generated by iterative reconstruction as previously described (15,16). Factor images were resliced into short-axis images in an orientation perpendicular to the long axis of the left ventricle. Sixteen ROIs, corresponding to the territories of distribution of the 3 major coronary arteries, were drawn within the left ventricular myocardium on 12 consecutive image planes, according to the recommendations of the American Society of Echocardiography (17). The regions were drawn semiautomatically using a center line within the myocardium. The ROIs drawn at baseline and at 24 wk were comparable in size and position. For the present analysis, however, the original 16 left ventricular ROIs were regrouped into 4 larger segments representing septal, anterior, lateral, and inferior walls. A separate set of ROIs was defined for the right ventricular cavity and the left atrium. Myocardial and blood time-activity curves were then generated from the dynamic image and fitted to a single-tissue compartment tracer kinetic model to give values of MBF (mL/min/g) (18). Subsequently, in each patient the myocardial ROI subtended by the most severe coronary stenosis was labeled as Isc, whereas the ROI subtended by an artery with minimal (<50% diameter stenosis) or no disease was labeled as Rem.
Since resting MBF is determined by cardiac work load (19), we corrected resting MBF for the rate·pressure product (RPP), an index of myocardial oxygen consumption: MBF = (MBF/RPP) × 104 (9). CFR was calculated as the ratio of MBF during Dob-induced hyperemia to MBF at rest corrected for RPP. Minimal coronary resistance (arbitrary units) was calculated as the mean pressure divided by MBF (whole left ventricle) during peak Dob infusion.
Statistical Analysis
Comparisons of the hemodynamic, exercise, and PET parameters at t = 0 and t = 24 data were performed by paired Student t tests. A P value < 0.05 was considered statistically significant. The coefficient of variance was calculated as SD/mean. To measure the reproducibility of resting and Dob MBF and CFR, we calculated the repeatability coefficient defined as 1.96 × SD, as proposed by Bland and Altman (20,21) and recommended by the British Standards Institution. Assuming that the data are normally distributed, in 95% of the cases, the difference between the 2 measures will be less than the repeatability coefficient. In addition, the repeatability is given as a percentage of the average value of the 2 measurements, although the results show that the error does not change with the absolute value of the measurement.
RESULTS
Clinical Status and Exercise Tolerance
All 15 patients reported stable symptoms over the 24-wk study period with no change in CCS functional class (2.3 ± 0.5) and, therefore, were included in the analysis. No patient required modification of antianginal therapy or procedural intervention during the study.
In our study population, both total treadmill exercise time (425 ± 95 s vs. 499 ± 106 s; P < 0.001) and maximum ST depression during exercise (2.4 ± 1.0 vs. 2.8 ± 1.2 mm; P < 0.02) increased at study completion compared with baseline. These findings probably reflect an effect of training and a greater tolerability of ischemia as described previously (22). To correct for this effect, we calculated the ratio of time achieved to ST depression (s/mm ST depression), which was comparable at baseline and at study completion (206 vs. 211 s/mm; P = not significant [ns])
PET Data
Hemodynamic measurements were similar for rest and Dob stress at baseline and after 24 wk (Table 2). For the values of RPP at rest, we found good repeatability with a coefficient of 2,340—that is, 24% of the mean RPP. The absolute repeatability coefficient of RPP during Dob stress was greater at 4,285 mm Hg × beats/min, but this represented a similar proportion (21%) of the mean peak RPP. Dob dose was not different between the 2 studies (30 ± 11 vs. 31 ± 11 μg/kg/min; P = ns).
Main Hemodynamic Parameters at Rest and Peak Dob Measured at Baseline (t = 0) and After 24 Weeks (t = 24)
Global MBF.
The baseline (t = 0) and 24 wk (t = 24) resting and Dob stress measurements were comparable (Table 3). Coefficient of variance data are presented in Table 4. The repeatability coefficient of global resting MBF was 0.25 mL/min/g, representing 23% of the mean and of Dob MBF was 0.58 mL/min/g—that is, 28% of the mean.
Values of MBF (mL/min/g) and CFR Measured at Baseline (t = 0) and After 24 Weeks (t = 24)
Coefficient of Variance of Global and Regional MBF Measurements at Baseline (t = 0) and After 24 Weeks (t = 24)
Regional MBF.
MBF measurements in Isc regions at rest and during Dob stress were comparable at t = 0 and t = 24 (Table 3). Individual values illustrating between-subject variability are shown in Figure 2. Bland-Altman analysis for both measures demonstrated good reproducibility with proportionally similar repeatability coefficients for resting Isc MBF (0.30 mL/min/g, 28% of the mean) and Isc MBF during peak Dob (0.49 mL/min/g, 27% of the mean) (Figs. 3A and 3B). Repeatability coefficients for Rem territories were similar to Isc territories and comparable at rest (0.26 mL/min/g equivalent to 24% of the mean) and during Dob hyperemia (0.58 mL/min/g equivalent to 26% of the mean) (Figs. 3C and 3D).

Individual resting and Dob MBF measured at baseline (1) and after 24 wk (2) in ischemic (Isc, A and B) and remote (Rem, C and D) myocardium. Paired values are given for each participant.

Repeatability of regional MBF measurements in ischemic (Isc, A and B) and remote (Rem, C and D) myocardial territories. Difference of 2 MBF measurements at rest (A and C) and during Dob hyperemia (B and D) is plotted against their average value (Bland-Altman plot).
CFR.
Global CFRs at baseline and at 24 wk were comparable (Table 3) with a repeatability coefficient of 0.64, representing variation of 33% from the mean. Regional CFRs demonstrated similar limits of agreement with a repeatability coefficient of 0.46 (28%) and of 0.65 (30%) for Isc and Rem CFR, respectively (Figs. 4A and 4B).

Repeatability of CFR measured at baseline (1) and after 24 wk (2) in ischemic (Isc, A) and remote (Rem, B) myocardial territories. Differences of values are plotted against their average value (Bland-Altman plot).
DISCUSSION
Although physical exercise has been shown to be feasible as a stressor with nuclear scintigraphy and echocardiography, pharmacologic agents are often preferred for technical and logistic reasons (23). The mechanism of Dob stress more closely mimics the physiologic stimulus of exercise than vasodilator agents and thus may provide greater insight into the functional limitations of myocardial and coronary disease. The present study was designed to determine the long-term reproducibility of Dob hyperemic MBF in patients with stable CAD. PET methodology was used because it provides accurate noninvasive assessment of absolute MBF in vivo and is increasingly used in studies comparing the effects of various interventions on myocardial perfusion. The short-term reproducibility of MBF measurements using PET has been previously demonstrated in healthy volunteers with both physical exercise and adenosine stress (13,24). The present study demonstrates that reproducibility of MBF can be extended to include both Dob stress and patients with stable CAD. In addition, our data provide insight into the time-related variability of resting MBF in patients with heart disease.
Reproducibility of MBF at Rest
The long-term reproducibility of MBF under resting conditions was good, with 95% limits of agreement measured within 23% of the mean for global MBF and 27% for regional MBF. Although a significant interindividual heterogeneity of resting MBF has been previously demonstrated (25), a good short-term repeatability in the same healthy individuals has been reported using PET (13). In healthy volunteers, global left ventricular MBF during a single session demonstrated a repeatability coefficient representing 18% of the mean value. However, this was higher for regional MBF—that is, between 22% and 46% of the mean value. Despite the effort made in the present study to standardize some parameters known to affect reproducibility—including time of day, smoking, caffeine consumption, and fasting state—the long-term repeatability of resting MBF was inferior to that previously reported in short-term studies. Numerous physiologic variables affect resting MBF, and this difference probably reflects the difficulty to correct for all of these factors if the time interval between the studies is longer.
Previous studies have suggested that repeatability of regional MBF may be more susceptible to variability, specifically due to methodologic reasons, because ROIs with smaller size have poorer counting statistics compared with ROIs with larger size. However, spatial heterogeneity of myocardial perfusion is well accepted (26) and may have influenced our results. Regional variability of perfusion has been observed in the hearts of all species studied thus far (27–29) to the extent of 6-fold (30), but the basis for such heterogeneity still lacks a definite explanation. Differences in local metabolic needs, perhaps secondary to differences in regional function, have been suggested (25). Temporal heterogeneities may cause changing variations between regions (31). Spatial heterogeneity in regional MBF has been linked to arteriolar or intratissue oxygen partial pressure over a broad range, from 40 to 200 mm Hg in dogs (32). Furthermore, a linear relationship between coronary flow distribution and tissue norepinephrine content may exist (33). Thus, physiologic heterogeneity may account for the larger variability in segmental MBF and temporal variations may explain, at least in part, the fact that regional MBF measurements are less reproducible than global MBF.
Reproducibility of Hyperemic Blood Flow
The 2 hyperemic measurements of global MBF revealed a repeatability coefficient of 0.58 (28% of the mean value) that indicated worse agreement than that observed for resting MBF. Regional hyperemic MBF for both Isc and Rem territories also demonstrated repeatability coefficients reflecting 27%–28% of the mean value. These findings are similar to short-term reproducibility results with adenosine-induced hyperemia. Since MBF during Dob stress is dependent on both RPP and coronary vasodilatation, we estimated the variability of cardiac work and coronary resistance. The latter was considered to reflect indirectly coronary driving pressure during Dob stress. RPP calculated under resting conditions (mean difference, −637) and during Dob hyperemia (mean difference, −691) was comparable (P = ns). Minimal coronary resistance at baseline was similar to that measured at 24 wk (56 ± 15 vs. 54 ± 16 arbitrary units; P = ns). As a result of the reproducibility of MBF measurements, we found similar values for global CFR at baseline and after 24 wk (1.95 ± 0.5 and 1.88 ± 0.45, respectively). However, the repeatability coefficient was 0.64, proportionally representing >33% of the mean. This likely reflects the combination of variability of resting MBF and the hemodynamic response to Dob. Regional CFR measurements also demonstrated higher repeatability coefficients (28%–30%) when compared with regional MBF.
Studies of regional blood flow have demonstrated that the distribution of both resting and hyperemic flow is extremely heterogeneous (27), resulting in a wide dispersion of coronary reserve (26). Seemingly, intrinsic properties, such as maximal regional blood flow, vary significantly throughout the heart and over time. Thus, the more modest reproducibility seen with regional CFR may be explained. Repetitive MBF measurements in the same patients have been reported by others, albeit usually to compare estimates of flow using 2 different approaches (34). Previous studies assessing repeatability of regional MBF in healthy volunteers have demonstrated comparatively modest reproducibility (13,24). Explanations include physiologic variability of hyperemic flow and methodologic issues. Our data for regional MBF in ischemic and remote territories in patients with CAD demonstrates much better reproducibility than that seen in control subjects (13,24). Therefore, PET methodologic issues are unlikely to be the main determinant for regional variability. The consistency of regional peak MBF measurements in patients with heart disease suggests that, with peak Dob stress and symptomatic myocardial ischemia, variability in peak MBF is driven by the metabolic demands of myocardium subtended by flow-limiting stenoses. In addition, we found that heterogeneity of peak MBF in remote territories also demonstrated reduced variability compared with previous published regional data in healthy volunteers (13,24). This is in line with previous reports demonstrating alteration of flow reserve in remote territories during severe regional ischemia (35). Values of hyperemic MBF measured in our study are similar to data published in the current literature using Dob stress and PET (36,37). These values are comparable with those attained by bicycle exercise (24) but are significantly lower than the hyperemia achieved with adenosine (13).
How far apart measurements can be made without causing a problem remains a question of judgment for each clinical and individual setting. Nagamachi et al. (38) have reported significant reproducibility of their MBF measurements with PET using 13NH3 and dipyridamole, performed on different days due to the long half-life of the drugs, but they did not provide a repeatability coefficient for their data. Dob has a half-life of ∼2 min, but its effect on the metabolic demands of myocardial tissue persists well beyond this time, limiting the assessment of reproducibility during a single session. Furthermore, in patients with coronary disease, ischemic insult alters regional myocardial function by a combination of stunning and preconditioning. These physiologic responses to myocardial ischemia remain beyond the pharmacokinetic clearance of Dob and have been shown to persist for a variable length of time (39,40). To obviate these confounding factors we assessed our patients over the long term and chose a time interval that would provide useful information on the variability of resting and Dob-induced MBF for clinical studies assessing the effect of various interventions.
CONCLUSION
The use of Dob as a stressor is increasing in clinical cardiology, and in the present study we report on the repeatability of MBF and CFR obtained during a conventional Dob stress protocol. We have also demonstrated the long-term reproducibility of noninvasively derived quantitative MBF measurements with PET and H215O in patients with stable CAD. The results support the use of PET as a reproducible technique for the determination of MBF after pharmacologic or mechanical intervention on the coronary circulation and could provide useful information for choosing the sample size of future clinical studies using Dob stress.
Footnotes
Received Jun. 11, 2004; revision accepted Sep. 10, 2004.
For correspondence or reprints contact: Paolo G. Camici, MD, Medical Research Council Clinical Sciences Centre, Imperial College of Science Technology and Medicine, Hammersmith Hospital, Du Cane Rd., London W12 0NN, United Kingdom.
E-mail: paolo.camici{at}csc.mrc.ac.uk
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cardiac PET Imaging for the Detection and Monitoring of Coronary Artery Disease and Microvascular Health
- The Clinical Value of Myocardial Blood Flow Measurement
- Hemodialysis-Induced Cardiac Dysfunction Is Associated with an Acute Reduction in Global and Segmental Myocardial Blood Flow
- Repeatability of Cold Pressor Test-Induced Flow Increase Assessed with H215O and PET
- Reproducibility of Measurements of Regional Myocardial Blood Flow in a Model of Coronary Artery Disease: Comparison of H215O and 13NH3 PET Techniques
- Novel Doppler Assessment of Intracoronary Volumetric Flow Reserve: Validation Against PET in Patients With or Without Flow-Dependent Vasodilation