


Abstract
PET absolute myocardial blood flow (MBF) with H215O and 13NH3 are widely used in clinical and research settings. However, their reproducibility with a 16-myocardial segment model has not been examined in chronic coronary artery disease (CAD). We examined the short-term reproducibility of PET H215O MBF and PET 13NH3 MBF in an animal model of chronic CAD. Methods: Twelve swine (mean weight ± SD, 38 ± 5 kg) underwent percutaneous placement of a copper stent in the mid circumflex coronary artery, resulting in an intense inflammatory fibrotic reaction with luminal stenosis at 4 wk. Each animal underwent repeated resting MBF measurements by PET H215O and PET 13NH3. Attenuation-corrected images were analyzed using commercial software to yield absolute MBF (mL/min/g) in 16 myocardial segments. MBF was also normalized to the rate·pressure product (RPP). Results: By Bland–Altman reproducibility plots, the mean difference was 0.01 ± 0.18 mL/min/g and 0.01 ± 0.11 mL/min/g, with confidence limits of ±0.36 and ±0.22 mL/min/g for uncorrected regional PET H215O MBF and for uncorrected regional PET 13NH3 MBF, respectively. The repeatability coefficient ranged from 0.09 to 0.43 mL/min/g for H215O and from 0.09 to 0.18 mL/min/g for 13NH3 regional MBF. RPP correction did not improve reproducibility for either PET H215O or PET 13NH3 MBF. The mean difference in PET H215O MBF was 0.03 ± 0.14 mL/min/g and 0.02 ± 0.19 mL/min/g for infarcted and remote regions, respectively, and in PET 13NH3 MBF was 0.03 ± 0.11 mL/min/g and 0.00 ± 0.09 mL/min/g for infarcted and remote regions, respectively. Conclusion: PET H215O and PET 13NH3 resting MBF showed excellent reproducibility in a closed-chest animal model of chronic CAD. Resting PET 13NH3 MBF was more reproducible than resting PET H215O MBF. A high level of reproducibility was maintained in areas of lower flow with infarction for both isotopes.
Several therapeutic advances have been developed for the treatment of chronic coronary artery disease (CAD) in patients otherwise not candidates for conventional revascularization. A common goal of these techniques, including laser revascularization, angiogenesis, and enhanced external counterpulsation, is to improve myocardial perfusion (1–3). However, demonstration of improved myocardial perfusion after these therapies has been challenging, in part due to limited knowledge on the reproducibility of serial blood flow measurements.
PET has distinct advantages for evaluating serial changes in myocardial blood flow (MBF). The noninvasive nature, along with the high spatial and temporal resolution, scatter and attenuation correction, high-energy tracers, and radiolabeling of naturally occurring compounds permit tracer kinetic modeling and accurate quantification of absolute MBF in mL/min/g. The short physical half-lives of PET tracers also allow repeated measurements of MBF in a single session. The PET perfusion tracers H215O and 13NH3 are increasingly used in clinical and research settings for assessment of absolute MBF. Although absolute MBF with both isotopes has been validated under normal, ischemic, and nonreperfused infarction conditions (4–11), their short-term reproducibility is not well established for conditions of chronic CAD. In particular, reproducibility of PET MBF has been reported only for models with 3 or 4 myocardial segments, not for the standard 16-segment model. Detailed knowledge of the variability associated with these measurements is required for sensitivity and sample-size calculations. Therefore, the aim of the study was to compare the short-term reproducibility of PET H215O MBF and PET 13NH3 MBF in 16 standard myocardial segments in a closed-chest swine model of chronic CAD.
MATERIALS AND METHODS
Animal Experimental Preparation
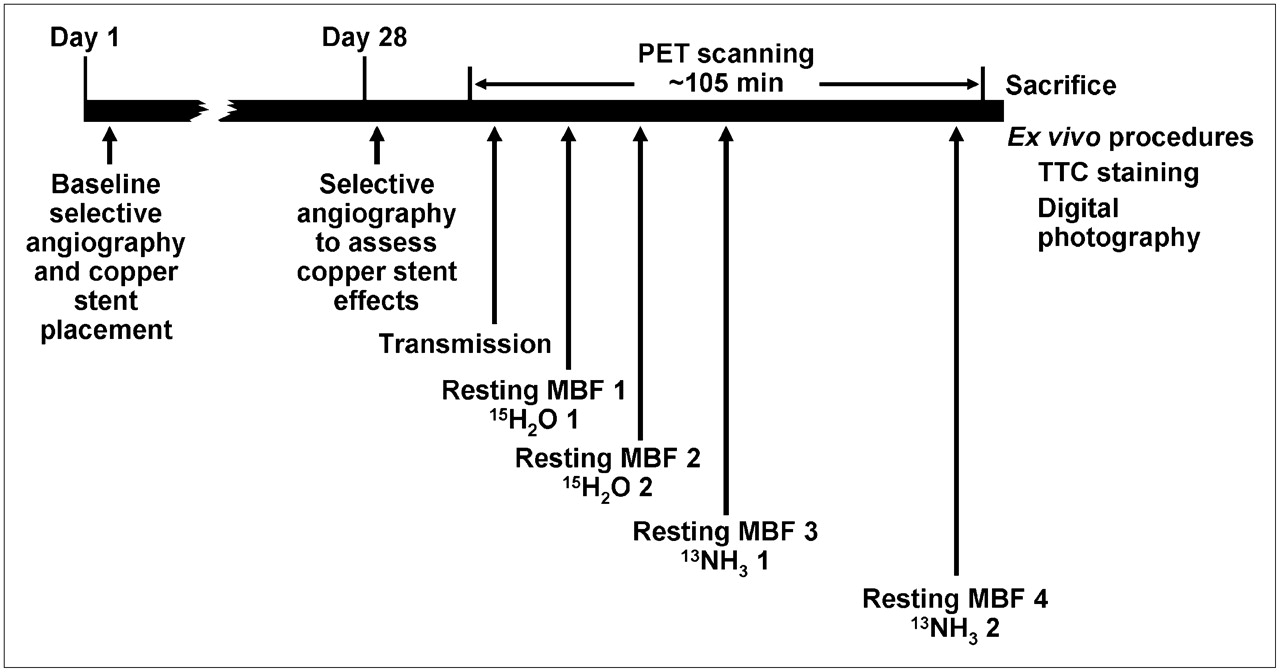
The Institutional Animal Care and Use Committee approved these studies. The investigation conforms with the Guide for the Care and Use of Laboratory Animals (12). Figure 1 illustrates the protocol sequence. On day 1, each Sus scrofa swine (mean weight ± SD, 38 ± 5 kg) underwent general anesthesia, mechanical ventilation, and arterial hemodynamic monitoring. Each animal received an intravenous bolus (10,000 units) of unfractionated heparin before undergoing selective baseline coronary angiography via the left carotid artery. Under fluoroscopic guidance and sterile conditions, a copper stent was placed percutaneously in the mid left circumflex coronary artery. The copper stent produces an intense inflammatory fibrotic reaction and vessel remodeling linearly related to the period of exposure (13,14). The result is progressive coronary artery luminal narrowing, subtotal and total coronary occlusion, with collateral development to an area of nonviable myocardium, confirmed postmortem by staining with triphenyltetrazolium chloride (TTC). After stent placement, the wound was closed and the animal was allowed to recover. Analgesics and penicillin (900,000 units intramuscularly) were administered through day 3 and oral aspirin (325 mg/d) and oral amiodarone (5 mg/kg/d) through day 28 after the procedure.

Protocol sequence. MBF = myocardial blood flow; TTC = triphenyltetrazolium chloride.
On day 28, each animal again underwent general anesthesia, mechanical ventilation, and arterial hemodynamic monitoring before returning to the fluoroscopy suite. Selective coronary angiography was performed to confirm the reactive inflammatory fibrotic effect of the copper stent before PET scanning.
PET Scanning Protocol
Scans were performed with an Advance PET scanner (GE Healthcare). Animals were positioned in the scanner, and after exposure from 68Ge rod sources, a 2-min transmission scan was acquired to determine the optimal positioning of the left ventricle (LV). A low-power laser beam was then superimposed on a cross-shaped ink mark on the animal to maintain the position. A 6-min transmission scan was performed for attenuation correction of the emission images. Emission images were acquired in the sequence shown in Figure 1. For the first resting H215O (H215O 1), an H215O bolus (711 ± 129 MBq) was injected intravenously over 20 s at a rate of 10 mL/min. The venous line was flushed for another 2 min. The following acquisition was used: 5 × 2, 20 × 3, 6 × 10, 6 × 30 frames × seconds. Hemodynamic measurements were obtained at the peak H215O activity. The second resting H215O bolus (691 ± 126 MBq) was administered 14 ± 2 min after the first H215O bolus and the image acquisition was repeated. After a period of 55 ± 4 min for 13NH3 production, the first 13NH3 slow bolus (709 ± 28 MBq) was injected intravenously over 20 s followed by a saline flush. The following acquisition parameters were used: 5 × 2, 20 × 3, 9 × 10, 4 × 20, 3 × 300 frames × seconds. Hemodynamic measurements were obtained at peak 13NH3. After radioactive decay and additional 13NH3 production (56 ± 5 min), the second 13NH3 slow bolus (670 ± 46 MBq) was administered and the above 13NH3 acquisition repeated.
After the PET scans, the animal was sacrificed and ex vivo procedures were performed. The heart was removed and divided into 5 or 6 short-axis slices of equal thickness. Heart slices were subsequently stained with 1% TTC and digitally photographed (Fig. 2).

Pig pathologic specimen after processing with TTC.
PET Data Analysis
Sinograms were corrected for attenuation, scatter, randoms, dead time, and radioactive decay and reconstructed using filtered backprojection with a ramp filter (cutoff, 4 mm) into a 22-cm field of view. Images were transferred to a personal computer workstation and analyzed with commercial software (version 2.4; PMOD Technologies). Using a combination of long- and short-axis images, the operator defined the apex and the base of the LV myocardium: apex = the short-axis slice after visualization of the LV cavity and base = the slice at 2-slice thicknesses before visualization of the septal dropout (Fig. 3A). Each short-axis slice thickness was 4.25 mm. On short-axis H215O and 13NH3 images, the center of the LV cavity and the septum were manually defined (Fig. 3A). The software then automatically defined 4 myocardial regions of interest (ROIs) in the apical planes and 6 myocardial ROIs in both mid and basal LV planes to produce a total of 16 myocardial segments (Fig. 3B). The left and right ventricular blood-pool ROIs were also defined manually on 3 short-axis planes to obtain the arterial and venous input functions, respectively (Fig. 3C). Factor analysis was applied to the H215O data to generate myocardial and blood-pool images (Fig. 4A) to guide H215O ROI placement (15). Time–activity curves were generated for the arterial, venous, and myocardial ROIs (Fig. 4B). The H215O arterial, venous and tissue input functions were fit to a 1-compartment model that includes left and right ventricle spillover corrections to yield values of regional and global MBF in mL/min/mL (16). Calculation of the tissue fraction (TF) was performed as previously described (17). The 13NH3 input functions were fit to a 1-compartment model that includes metabolite and left and right ventricle spillover corrections to yield values of regional and global MBF in mL/min/mL (18). Only the first 4 min of the 13NH3 time–activity curves were used in the modeling. For comparison with previously reported values, MBF values were divided by the density of myocardial tissue (1.04 g/mL) to express MBF values in mL/min/g (19).

(A) Using a combination of long-axis and short-axis images, the operator defined the apex and the base of LV myocardium: the short-axis slice after visualization of LV cavity was chosen as apex and the slice at 2-slice thicknesses before visualization of the septal dropout was chosen as base. On a short-axis image, center of LV cavity and septum were manually defined. (B) Software subsequently automatically defined 4 myocardial ROIs in the apical planes, and 6 ROIs in both mid and basal LV planes to produce a total of 16 myocardial segments. Ant-sep = anteroseptal; Inf-sep = inferoseptal. (C) Left and right ventricular blood-pool ROIs were also defined manually on at least 3 short-axis planes to obtain the arterial and venous input functions, respectively

H215O (A) and 13NH3 (B) short-axis images corresponding to pig pathologic specimen in Figure 2. Factor analysis was applied to H215O data to generate images for H215O ROI placement.
To account for changes produced by cardiac workload, MBF was corrected for the rate·pressure product (RPP) (20), using the formula MBFcorr = (MBF/RPP) × 104.
Statistical Analysis
Values are expressed as mean ± SD. Comparisons of the hemodynamic and MBF measurements were performed by paired Student t test. To determine the reproducibility of PET MBF, the repeatability coefficient (1.96 × SD) and limits of agreement were calculated as proposed by Bland and Altman (21). Absolute and percent mean differences were also calculated. ANOVA and post hoc analyses were used to determine the differences between MBF and TF values in infarcted versus remote regions.
RESULTS
Sixteen animals were included. Four animals died suddenly after copper stent placement, leaving 12 animals to undergo PET. The mean luminal coronary artery stenosis for the 12 animals was 91% ± 7%. All animals had evidence of myocardial infarction by TTC staining, exemplified by the processed short-axis slices of an animal from the study (Fig. 2).
Hemodynamic Measurements
During the first and second MBF measurements for each PET perfusion tracer, the heart rate and the systolic and diastolic blood pressures were nearly identical (Table 1). There were no significant differences in the hemodynamic parameters between H215O 1 versus H215O 2 or between 13NH3 1 versus 13NH3 2. The RPP mean difference was 438 mm Hg × bpm (5.3% ± 9.6%) for H215O and 382 mm Hg × bpm (5.4% ± 15.5%) for 13NH3.
Hemodynamic Measurements
Global MBF
Resting global MBF (i.e., mean flow in the whole LV) was 0.75 ± 0.26 mL/min/g for H215O 1, 0.76 ± 0.28 mL/min/g for H215O 2, 0.66 ± 0.19 mL/min/g for 13NH3 1, and 0.64 ± 0.22 mL/min/g for 13NH3 2. The mean difference was 0.01 ± 0.11 mL/min/g (1.4% ± 14.1%) for H215O MBF and 0.02 ± 0.09 mL/min/g (3.0% ± 13.0%) for 13NH3 MBF. The repeatability coefficient was 0.21 mL/min/g (26.6% of the mean) and 0.18 mL/min/g (26.6% of the mean) for uncorrected global H215O and 13NH3 MBF, respectively.
Corrected global MBF was higher than uncorrected MBF, with mean values of 1.14 ± 0.18 mL/min/g for H215O 1, 1.24 ± 0.24 mL/min/g for H215O 2, 1.03 ± 0.38 mL/min/g for 13NH3 1, and 1.18 ± 0.48 mL/min/g for 13NH3 2. The mean difference was 0.10 ± 0.18 mL/min/g (9.6% ± 15.7%) for corrected H215O global MBF and 0.15 ± 0.37 mL/min/g (18.6% ± 45.6%) for corrected 13NH3 global MBF. The repeatability coefficient was 0.38 mL/min/g (30.7% of the mean) and 0.78 mL/min/g (67.8% of the mean) for corrected global H215O and 13NH3 MBF, respectively.
Regional MBF
Resting uncorrected PET MBF values in 16 segments are shown in Table 2 with their mean differences and repeatability coefficients. Bland–Altman plots for resting regional uncorrected PET H215O MBF and PET 13NH3 MBF are shown in Figure 5. The mean difference was 0.01 ± 0.18 mL/min/g and 0.01 ± 0.11 mL/min/g, with confidence limits of ± 0.36 and ± 0.22 mL/min/g for uncorrected regional PET H215O MBF and for uncorrected regional PET 13NH3 MBF, respectively. The repeatability coefficient ranged from 0.20 to 0.60 mL/min/g (28.7%–72.1% of the mean) for uncorrected regional PET H215O MBF and from 0.17 to 0.32 mL/min/g (27.2%–51.1% of the mean) for uncorrected regional PET 13NH3 MBF. The agreement in regional uncorrected MBF by each isotope is also shown in the scatter plots (Fig. 6).

Bland–Altman plots for resting regional uncorrected MBF for H215O (A) and 13NH3 (B). Mean difference was 0.01 mL/min/g and 0.01 mL/min/g, with confidence limits of ±0.37 and ±0.23 mL/min/g for H215O and for 13NH3, respectively.

Scatter plots for H215O (A) and 13NH3 (B) uncorrected PET MBF. Line of identity is shown.
Resting Regional Uncorrected MBF (mL/min/g)
Because animals underwent copper stent placement with its attendant progressive coronary artery narrowing in the proximal to mid left circumflex coronary artery, the posterior region of the LV contained infarcted tissue by TTC staining (Fig. 2). Resting uncorrected MBF measurements in these segments were significantly lower than those in remote regions. For H215O 1, mean infarcted MBF was 0.69 ± 0.28 mL/min/g versus mean remote MBF of 0.81 ± 0.30 mL/min/g (P = 0.039). For H215O 2, mean infarcted MBF was 0.68 ± 0.30 mL/min/g versus mean remote MBF of 0.82 ± 0.30 mL/min/g (P = 0.019). For 13NH3 1, mean infarcted MBF was 0.58 ± 0.20 mL/min/g versus mean remote MBF of 0.72 ± 0.22 mL/min/g (P = 0.001). For 13NH3 2, mean infarcted MBF was 0.58 ± 0.23 mL/min/g versus mean remote MBF of 0.71 ± 0.24 mL/min/g (P = 0.005). The mean difference in PET H215O MBF was 0.03 ± 0.14 mL/min/g and 0.02 ± 0.19 mL/min/g for infarcted and remote regions, respectively, and in PET 13NH3 MBF was 0.03 ± 0.11 mL/min/g and 0.00 ± 0.09 mL/min/g for infarcted and remote regions, respectively.
The repeatability coefficients were similar between infarcted versus remote H215O MBF and similar between infarcted versus remote 13NH3 MBF.
After RPP correction, the mean difference in regional corrected MBF ranged from 0.02 ± 0.27 mL/min/g (0.4% ± 30.2%) to 0.26 ± 0.60 mL/min/g (22.8% ± 47.8%) for H215O and from 0.08 ± 0.38 mL/min/g (14.9% ± 48.9%) to 0.22 ± 0.43 (26.1% ± 49.2%) for 13NH3 corrected MBF (Table 3). Repeatability coefficients ranged from 0.38 to 1.19 mL/min/g (29.3%–76.1% of the mean) for H215O and from 0.70 to 0.98 mL/min/g (62.3%–83.4% of the mean) for 13NH3. RPP correction appeared to worsen the reproducibility of regional MBF to a greater extent for 13NH3 than for H215O, shown by the Bland–Altman and scatter plots (Figs. 7 and 8).

Bland–Altman plots for resting regional corrected MBF values for H215O (A) and 13NH3 (B). Mean difference was 0.11 mL/min/g and 0.16 mL/min/g, with confidence limits of ±0.66 and ±0.80 mL/min/g for H215O and for 13NH3, respectively. corr = corrected.

Regression plots for H215O (A) and 13NH3 (B) corrected PET MBF. Line of identity is shown.
Resting Regional RPP-Corrected MBF (mL/min/g)
TF
TF in regions subtended by the stented artery was significantly lower than that in remote regions (0.536 ± 0.134 g/mL vs. 0.782 ± 0.073 g/mL, P < 0.0001) for H215O 1. The range of H215O 1 TF was 0.287–0.773 g/mL in segments containing TTC-negative tissue and 0.556–0.950 g/mL in remote myocardium. For H215O 2, TF was 0.574 ± 0.127 (range, 0.325–0.679) g/mL in stented vs. 0.792 ± 0.081 (range, 0.593–0.894) g/mL in remote regions.
DISCUSSION
Our results indicate that MBF measurements in absolute terms obtained noninvasively with PET H215O and PET 13NH3 in a single session were highly reproducible in a swine model of chronic CAD. The high level of reproducibility was found in both normal- and low-flow states, the latter containing infarcted myocardium, and was present for global and regional MBF measurements by both isotopes. However, 13NH3 MBF was more reproducible than H215O MBF.
Reproducibility of PET H215O MBF
The reproducibility of PET H215O resting MBF has been reported in 3 publications to date. Two studies were from the same institution, and all 3 studies had small numbers of human subjects (11 and 21 healthy volunteers, and 15 patients with CAD) (10,22,23). The studies found very good reproducibility of resting PET H215O MBF but all 3 in effect reported values in a 4-segment model of the LV (septal, anterior, lateral, inferior). To our knowledge, the reproducibility of the clinically used 16-segment model has not been reported previously. Using the 16-segment model, we observed very good reproducibility of regional resting uncorrected PET H215O MBF, with a mean difference of 0.01 mL/min/g and absolute repeatability coefficients in the range of 0.24–0.60 mL/min/g or 28.7%–72.1% of the mean. Despite the 16-segment model, our values are similar to the previously reported reproducibility coefficients of 0.20–0.66 mL/min/g for resting PET H215O MBF using the 4-segment model (10,22).
Reproducibility of regional uncorrected resting PET H215O MBF in infarcted myocardium has not previously been reported. In our study, resting uncorrected PET H215O MBF in regions subtended by the copper-stented coronary artery and containing TTC-negative myocardium (repeatability coefficient, 0.24 mL/min/g) showed reproducibility similar to that of remote areas (repeatability coefficient, 0.39 mL/min/g). Flow values in these regions were higher than expected, likely from a contribution of residual antegrade and collateral flows and the admixture of scar tissue and viable myocardium. This was confirmed by a mean TF of 0.536 ± 0.134 g/mL in the same regions. Reproducibility of regional resting PET H215O MBF in ischemic territories has previously been reported to be 0.26 mL/min/g, or 24% of the mean; however, in that study, repeat measurements were obtained at 24 wk and a 4-segment model was used (23).
Global resting PET H215O MBF showed excellent reproducibility in our study, with an absolute repeatability coefficient of 0.21 mL/min/g (27% of the mean), comparable to prior reports of 0.17 mL/min/g (18% of the mean) (10), 0.26 mL/min/g (21% of the mean) (22), and 0.25 mL/min/g (23% of the mean) (23).
A wide range of uncorrected resting global and regional PET H215O MBF in remote myocardium has been reported in healthy humans and animals (10,24–27). The mean global and regional resting PET H215O MBF values in the current study are in agreement with prior studies. RPP correction has not consistently reduced the variability associated with these measurements in our study or others (10,25,28), suggesting the contribution of other factors. Heterogeneity of resting MBF has been described within and between individuals (25). Both temporal and spatial heterogeneity have been observed in healthy humans and animals and may relate to “twinkling” of capillary flows, time-dependent changes in regional metabolic requirements, local autoregulatory changes, and the fractal nature of regional flow distribution (25,29).
Reproducibility of PET 13NH3 MBF
Three prior publications have addressed the reproducibility of resting PET 13NH3 MBF measurements (11,18,28). These studies included 6, 8, and 30 healthy volunteers, and 6 humans with stable CAD (28). Important differences between these reports and the current study include their use of human subjects, their longer time interval between scans, their fewer myocardial regions (3–4), and the 3-compartment kinetic modeling in 2 earlier studies. Despite smaller ROIs, our mean difference (0.00–0.04 mL/min/g) between the 2 resting regional PET 13NH3 MBF was similar to the mean difference in the earlier study (0.04 ± 0.04 mL/min/g) (28). Use of anesthetized animals likely contributed in part to our observed reproducibility by minimizing subject motion, allowing more stringent hemodynamic regulation and reducing other effects of consciousness on blood flow and autoregulatory mechanisms. RPP correction did not improve the reproducibility of resting regional PET 13NH3 MBF in their study or our study. The mean difference of 15.8% ± 15.8% between the 2 resting PET 13NH3 MBF values in the second study (11) is higher than the mean difference in our study (0.3%–6.0%), despite our smaller ROIs. That study was among the few in which RPP correction improved reproducibility of resting PET 13NH3 MBF. In the study examining 1- and 2-compartmental modeling techniques in healthy humans, the relative change between the 2 resting MBF indices for all techniques was 0.03–0.04 mL/min/g but that study reported MBF values in only 3 myocardial segments (18).
In the current study, the repeatability coefficient of resting PET 13NH3 MBF in regions containing TTC-negative myocardium (0.22 mL/min/g) was similar to that of remote areas (0.18 mL/min/g), suggesting stable reproducibility in areas of low flow with infarction.
Resting PET 13NH3 MBF in remote or normal regions is in agreement with prior measurements (11,28). Interestingly, PET 13NH3 MBF estimates appear to be consistently lower than PET H215O MBF estimates in this study. In the single prior publication comparing PET H215O MBF and PET 13NH3 MBF, this systematic difference was not present in the 15 healthy volunteers (9). The reasons for the difference in our study are likely both physiologic and methodologic. First, in all animals, PET image acquisition was first performed with the 2 serial H215O administrations, followed almost 1 h later by the first 13NH3 acquisition. With prolonged instrumentation and sedation, a trend toward lower blood pressure was observed over the course of our PET, which might have contributed to lower resting MBF. Second, metabolite correction was applied to the 13NH3 data and might systematically affect MBF estimates. However, only the first 4 min of data were used in the kinetic modeling, and at 4 min there remains ∼75% of the 13N-labeled radioactivity as 13NH3 in the arterial blood of human volunteers (30). Third, if the tissue composition is highly heterogeneous, with a mixture of viable and fibrotic myocardium, PET 13NH3 MBF may be lower than PET H215O MBF because the former reflects the average uptake and therefore average flow in the admixture, whereas H215O uptake is negligible in scar and mainly reflects activity in the better perfused segments (31). Though this might explain the lower PET 13NH3 MBF estimates in regions with this admixture, it does not account for the difference in MBF in normal regions. Whereas equivalence in performance of H215O and 13NH3 as perfusion tracers may be demonstrated, the 2 tracers are not congruent. Myocardial H215O uptake does not vary despite wide variations on flow rate because it is metabolically inert and freely diffusible across capillary and sarcolemmal membranes (32). On the other hand, myocardial 13NH3 uptake depends on blood flow, myocardial metabolic trapping, and whole-body metabolism of 13NH3. Despite accounting for these differences in kinetic modeling, these tracers may still provide measurements of different parameters, even in normal myocardium.
Reproducibility of PET H215O MBF Versus PET 13NH3 MBF
Although reproducibility was excellent for both PET H215O and PET 13NH3 uncorrected resting MBF in the current study, reproducibility was higher for PET 13NH3 than for PET H215O regional MBF (Fig. 5; Table 2). The short physical half-life of H215O (2.1 min vs. 9.8 min for 13NH3) results in a rapid decline in counting rates, creating considerable statistical noise and affecting tracer quantification (33). The smaller ROIs in the current study compound the existing problem of statistical noise with H215O. Subtraction for spillover between myocardium and blood pool also augments statistical noise and is sensitive to subject movement (5). The latter poses more challenges for ROI placement on H215O images than on 13NH3 images because of the poorer myocardial definition of the former. Lastly, the partition coefficient of water may not be constant around infarcted tissue and may affect PET H215O MBF in such regions (17).
In areas of low flow with infarction (TTC-negative regions; Fig. 2), reproducibility remained excellent for both H215O and 13NH3. Lower counting statistics associated with lower flow is a potential contributing factor to differences in reproducibility between remote and infarcted regions, particularly with the higher statistical noise of H215O. With 13NH3, differences in trapping and metabolism in areas of lower flow with infarction could alter the flow–extraction relationship. In particular, the cell-integrity dependence of 13NH3 extraction may affect its reproducibility in TTC-negative regions. Lastly, partial-volume correction was not applied to our H215O or 13NH3 studies; partial-volume effects can result in <100% recovery of tissue activity in structures measuring less than about twice the full width at half maximum spatial resolution and can amount to 30% activity loss (34). This may be a particular issue for regions containing infarcted myocardium.
Limitations
Because of practical considerations, the order of 2 tracers could not be randomized. Further, we did not assess reproducibility of hyperemic MBF in part due to practical considerations but also because the response of swine to vasodilator stress is highly variable in our experience. Even in humans, up to 16% of patients receiving adenosine at a dose of 140 μg/kg/min have failed to achieve maximal coronary vasodilation (35).
Because all animals underwent copper stent placement in only the mid left circumflex coronary artery, results may not be applicable to other regions of low flow with infarction or to the setting of multivessel disease.
CONCLUSION
PET H215O and PET 13NH3 resting global and regional MBF showed excellent reproducibility in a closed-chest animal model of chronic CAD, despite small ROIs. Resting PET 13NH3 MBF was more reproducible than resting PET H215O MBF, likely in large part due to higher counting statistics with 13NH3. A high level of reproducibility was maintained in areas of low flow with infarction with both 13NH3 and H215O. RPP correction did not improve short-term reproducibility of either resting PET 13NH3 MBF or resting PET H215O MBF, suggesting the role of other factors.
Acknowledgments
The authors thank the Mayo Cyclotron personnel for isotope production, Mayo PET technologists for late-night acquisitions, and Teresa Decklever for her contribution to PET data analysis. We are also indebted to Drs. Alejandro R. Chade and Lilach O. Lerman for their support. The study was supported by a grant from the Mayo Foundation. This study was presented in part at the 9th Annual Symposium and Scientific Session of the American Society of Nuclear Cardiology, New York, NY, September 30 to October 2, 2004. The authors have no conflicts of interest to disclose.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication January 6, 2006.
- Accepted for publication March 20, 2006.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Quantitative Assessment of Myocardial Blood Flow in Cardiac Sarcoidosis: A Potential Next Step in the Further Integration of FDG-PET in Imaging Management?
- Impact of Unexpected Factors on Quantitative Myocardial Perfusion and Coronary Flow Reserve in Young, Asymptomatic Volunteers
- Single-Phase CT Aligned to Gated PET for Respiratory Motion Correction in Cardiac PET/CT
- Quantification of Absolute Myocardial Blood Flow by Magnetic Resonance Perfusion Imaging