


Abstract
Preclinical studies have indicated that somatostatin receptor (sst)–expressing tumors demonstrate higher uptake of radiolabeled sst antagonists than of sst agonists. In this study, we evaluated whether imaging with sst antagonists was feasible in patients. Methods: Biodistribution and tumor uptake of the sst antagonist 111In-DOTA-pNO2-Phe-c(DCys-Tyr-DTrp-Lys-Thr-Cys)DTyrNH2 (111In-DOTA-BASS) were studied in 5 patients with metastatic thyroid carcinoma or neuroendocrine tumors. Findings were compared with 111In-pentetreotid (111In-DTPA-octreotide) scan. Results: No adverse effects of 111In-DOTA-BASS (20 μg) were observed. 111In-DOTA-BASS detected 25 of 28 lesions, whereas 111In-DTPA-octreotide detected only 17 of 28 lesions. In the same patient, 111In-DOTA-BASS showed higher tumor and lower renal uptake than 111In-DTPA-octreotide (3.5 ± 2.8 percentage injected activity [%IA] vs. 1.0 ± 0.99%IA and 1.5 ± 0.3 %IA vs. 2.3 ± 0.7 %IA) at 4 h after injection. Conclusion: Imaging of neuroendocrine tumors with sst antagonists is clinically feasible. The favorable human biodistribution data suggest that sst antagonists could significantly affect peptide receptor–mediated imaging and therapy.
Targeting of G-protein–coupled receptors with radiolabeled receptor agonists is a promising diagnostic and therapeutic approach in oncology (1). Radiolabeled somatostatin receptor (sst) agonists have become an integral part of diagnostic and therapeutic management of patients with neuroendocrine tumors (2,3). Although agonists readily internalize into tumor cells, permitting accumulation of radioactivity, radiolabeled antagonists do not and have therefore not been used clinically for tumor targeting.
Ginj et al., however, showed in animal studies that radiolabeled sst antagonists are superior to agonists for the in vivo targeting of tumors expressing sst subtypes 2 (sst2) and 3 (sst3) (4). The in vivo uptake in sst2-positive tumors was twice as high with the antagonist 111In-DOTA-pNO2-Phe-c(DCys-Tyr-DTrp-Lys-Thr-Cys)DTyrNH2 (111In-DOTA-BASS) as with the highly potent agonist [111In-DTPA0,Tyr3,Thr8]-octreotide (111In-DTPA-TATE) (DTPA is diethylenetriaminepentaacetic acid). Scatchard analysis in human embryonic kidney (HEK)-sst2 cells showed more than 10 times the number of binding sites for 111In-DOTA-BASS (maximum number of sst2 binding sites, 354 ± 14 pM) as for 111In-DTPA-TATE (maximum number of sst2 binding sites, 23 ± 1.0 pM) (4). The same observation has been made for 5-HT2A receptors and corticotrophin-releasing factor receptors (5,6). Comparison of radiolabeled agonists and antagonists in a gastrin-releasing peptide receptor–positive prostate cancer animal model also showed the superiority of antagonists in an additional receptor system (7,8). If confirmed clinically, these observations could lead to a paradigm shift in the development of radiolabeled G-protein–coupled receptor ligands for diagnostic and therapeutic purposes.
The purpose of this pilot study was to evaluate the feasibility of imaging sst-expressing tumors in patients with the novel receptor antagonist 111In-DOTA-BASS. Tumor detection rate and tracer uptake by tumors and normal organs were determined at various times and compared with recent 111In-DTPA-octreotide scans. On the basis of the biodistribution of 111In-DOTA-BASS, estimates were made for the expected radiation dosimetry of the therapeutic radioligand 90Y-DOTA-BASS.
MATERIALS AND METHODS
Patients
Five consecutive patients with progressive disease after standard therapy were prospectively recruited. Their tumors demonstrated low or moderate uptake of 111In-DTPA-octreotide (tumor uptake less than or slightly above liver uptake) limiting the efficacy of radionuclide therapy with sst agonists. Patient characteristics are summarized in Table 1. Exclusion criteria were renal insufficiency, treatment with short-acting somatostatin analogs less than 3 d, and sandostatin depot injection less than 4 wk before scanning. The use of 111In-DOTA-BASS in this setting was approved by the local institutional review board, and written informed consent was obtained in accordance with the Declaration of Helsinki.
Patient Characteristics
Radiochemistry
The peptide-chelator conjugate DOTA-pNO2-Phe-c(DCys-Tyr-DTrp-Lys-Thr-Cys)DTyrNH2 (DOTA-BASS) (Fig. 1) was synthesized under good manufacturing practice conditions by standard 9-fluorenylmethoxycarbonyl solid-phase synthesis as previously described (9). The pure compound was characterized by electrospray ionization mass spectrometry and analytic reversed-phase high-performance liquid chromatography.

Structural formula of sst antagonist DOTA-BASS.
For the preparation of 111In-DOTA-BASS, 500 μL of ammonium acetate buffer (0.4 M, pH 5.0) were added to the vial containing 25 μg of DOTA-BASS and incubated with approximately 200 MBq of 111InCl3 (Mallinckrodt) for 30 min at 95°C. Quality control of the final product was performed by analytic reversed-phase high-performance liquid chromatography and instant thin-layer chromatography. 111In-DTPA-octreotide was prepared with the commercially available kit Octreoscan (Covidien). The labeling yield of 111In-DOTA-BASS and 111In-DTPA-octreotide was 95% or greater at a specific activity of 12 GBq/μmol and 26 GBq/μmol, respectively. The radiochemical purity of 111In-DOTA-BASS was greater than 95%.
Imaging
Total-body and SPECT 111In-DOTA-BASS scans were obtained 11–13 d after 111In-DTPA-octreotide scans. All studies were done with the same dual-head γ-camera (Skylight; Phillips) equipped with medium-energy, parallel-hole collimators. 111In-DTPA-octreotide planar scans were obtained at 4 and 24 h after injection of approximately 10 μg (167–192 MBq) of 111In-DTPA-octreotide (European Association of Nuclear Medicine guidelines (10)), and sst antagonist total-body scans were obtained at 0.5, 1, 4, 24, 48, and 72 h after injection of 20 μg (145–176 MBq) of 111In-DOTA-BASS. For both tracers, SPECT images of the abdomen and thorax were acquired at 5 h after injection (2 × 180° rotation; 64 projections; 128 × 128 matrix; 30-s acquisition time per projection). Patients’ vital parameters such as blood pressure, pulse rate, oxygen saturation, and electrocardiogram were monitored for at least 2 h after injection of 111In-DOTA-BASS.
111In-DOTA-BASS and 111In-DTPA-octreotide scans were assessed independently by 2 experienced nuclear medicine physicians. The physicians were unaware of patients’ identity, type of scan, and results of other imaging modalities. Afterward, the image findings were compared lesion by lesion with each other and with contrast-enhanced CT studies of the chest and abdomen. These scans had been acquired less than 5 wk before the 111In-DTPA-octreotide scans using various multislice CT scanners.
Pharmacokinetics
For all imaging time points, regions of interest were manually drawn around the whole body and each organ with visible uptake (kidneys, spleen, liver, bladder, and tumor lesions), on both the anterior and the posterior scans. Background regions were placed close to the regions of interest for background correction. The geometric mean value, between anterior and posterior, was taken and corrected for attenuation using the conjugate-view method (11). Whole-body activity acquired 30 min after injection of 111In-DOTA-BASS was set as 100 percentage injected activity (%IA). Blood samples were taken at 1, 2, 3, 4, 5, 10, 20, 30, and 60 min and 1.5, 4, and 24 h after injection.
Dosimetry
Time–activity curves derived from the whole-body studies were analyzed with the OLINDA/EXM 1.0 software (Vanderbilt University) (12) to calculate the radiation dose after administration of 111In-DOTA-BASS. For the latter calculation, it was assumed that 111In-DOTA-BASS and 90Y-DOTA-BASS demonstrate an identical biodistribution. Organ doses were calculated for the whole-body male phantom. Blood marrow doses were determined by the blood-based red marrow dose methodology, which assumes a linear relation between the blood residence time and the red marrow residence time (13).
RESULTS
Pharmacokinetics and Dosimetry
None of the patients experienced adverse reactions after intravenous injection of 20 μg of 111In-DOTA-BASS. Blood sampling revealed a biexponential blood clearance of 111In-DOTA-BASS: α-half-life, 12.5 ± 1.9 min and β-half-life, 6.1 ± 1.1 h; approximately 65% of the administered activity was cleared in the α-phase. The clearance occurred predominantly via the kidneys. The longest residence times of 111In-DOTA-BASS were observed in the tumor and kidneys (Figs. 2 and 3).

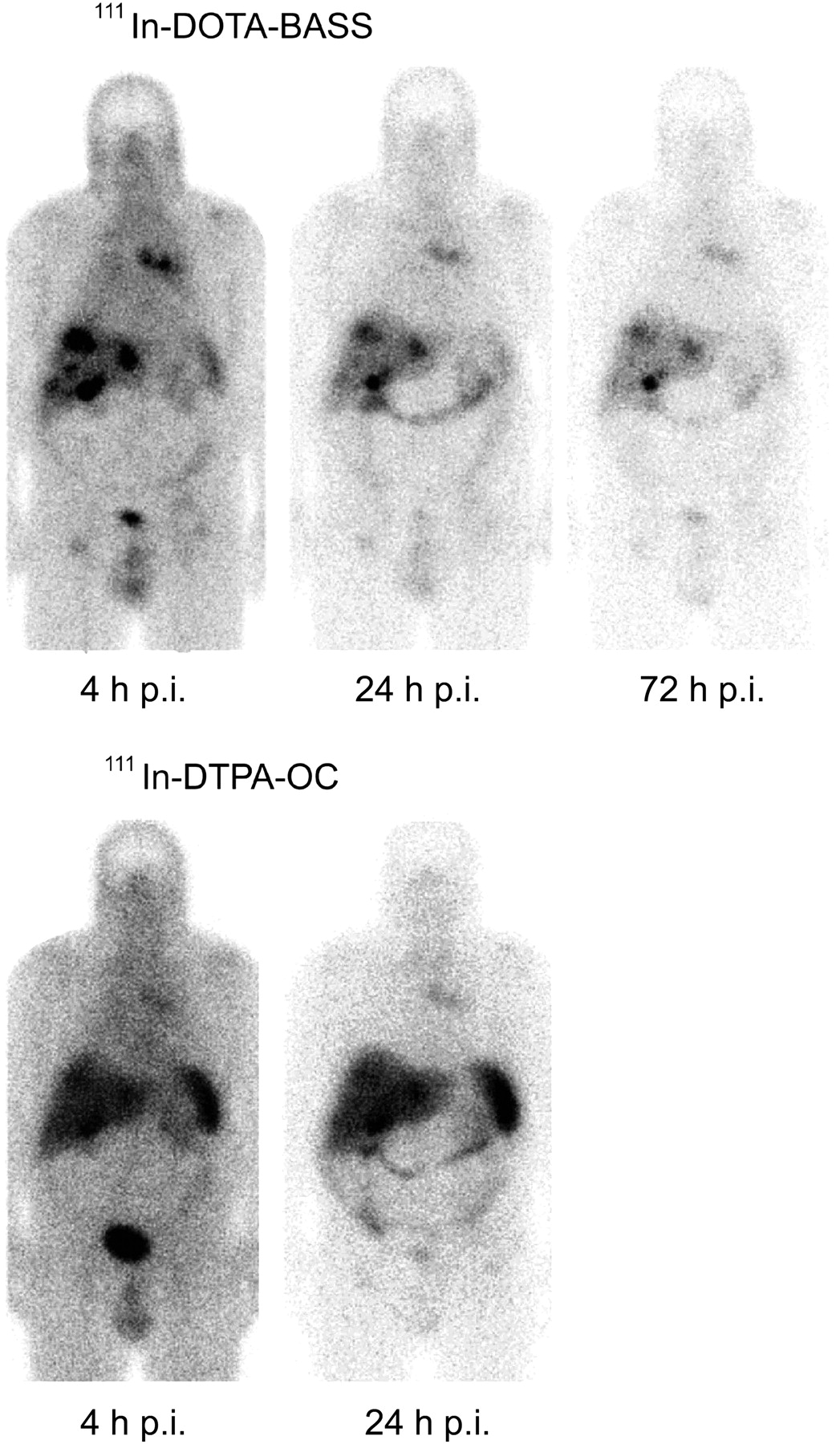
111In-DOTA-BASS (4, 24, and 72 h after injection) and 111In-DTPA-octreotide (4 and 24 h after injection) planar posterior whole-body scans from patient 4. Large arrow shows increased uptake of 111In-DOTA-BASS and 111In-DTPA-octreotide in liver, corresponding to multiple liver metastases. Tumor-to-kidney uptake ratio was several times higher for 111In-DOTA-BASS (6.1 at 4 h after injection and 3.3 at 24 h after injection) than for 111In-DTPA-octreotide (1.18 at 4 h after injection and 0.88 at 24 h after injection). Small arrow shows spleen. OC = octreotide; p.i. = after injection.

111In-DOTA-BASS (4, 24, and 72 h after injection) and 111In-DTPA-octreotide (4 and 24 h after injection) planar anterior whole-body scans from patient 2. Images illustrate better tumor-to-background uptake ratio of 111In-DOTA-BASS (e.g., tumor-to-liver uptake ratio of 6.7 at 4 h after injection and 3.5 at 24 h after injection) than of 111In-DTPA-octreotide (1.2 at both time points). In this patient, 111In-DOTA-BASS detected 16 metastases, whereas 111In-DTPA-octreotide detected only 11 metastases. OC = octreotide; p.i. = after injection.
In the quantitative analysis, there were relevant differences in the biodistribution between the sst antagonist 111In-DOTA-BASS and sst agonist 111In-DTPA-octreotide (Fig. 4). The antagonist showed up to 4.1 times higher uptake in the tumor (111In-DOTA-BASS, 3.5 ± 2.8 %IA, and 111In-DTPA-octreotide, 1.0 ± 0.99 %IA) 4 h after injection. At the same time, the uptake in the kidneys was lower (111In-DOTA-BASS, 1.5 ± 0.3 %IA, and 111In-DTPA-octreotide, 2.3 ± 0.7 %IA), resulting in up to 5.2 times higher tumor-to-kidney uptake ratio in favor of the antagonist (Supplemental Table 1 [supplemental materials are available online only at http://jnm.snmjournals.org]; Figs. 2 and 4). The antagonist also showed lower uptake in organs such as liver (111In-DOTA-BASS, 1.4 ± 0.2 %IA, and 111In-DTPA-octreotide, 1.7 ± 0.6 %IA) and spleen (111In-DOTA-BASS, 1.0 ± 0.2 %IA, and 111In-DTPA-octreotide, 2.3 ± 1.0 %IA) 4 h after injection.
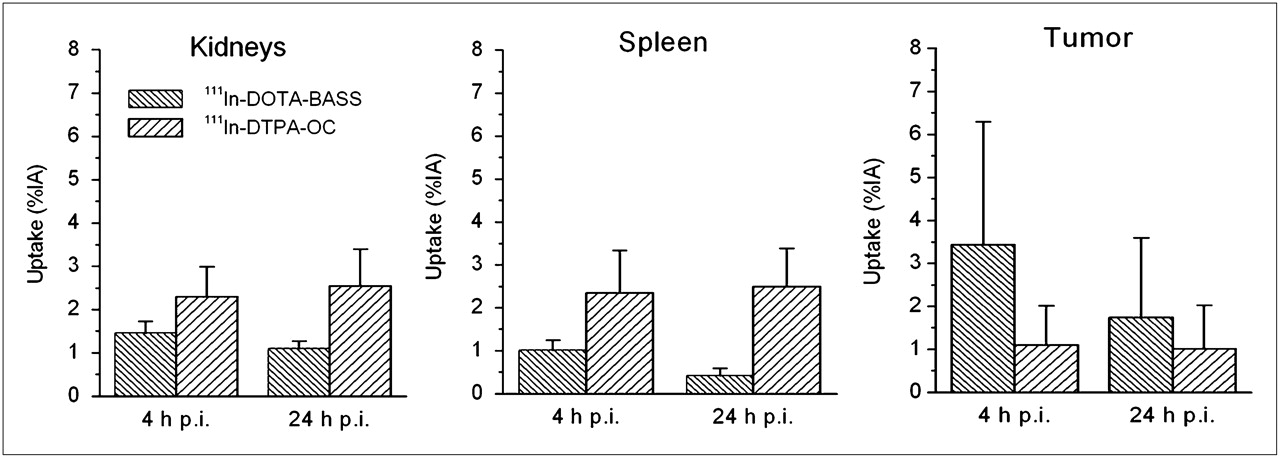
Comparison of 111In-DOTA-BASS and 111In-DTPA-octreotide uptake in kidneys, spleen, and tumors. Values are expressed as mean ± SD of 5 patients. OC = octreotide; p.i. = after injection.
The calculated effective radiation dose was 0.049 ± 0.0076 mSv/MBq for 111In-DOTA-BASS and 0.25 ± 0.031 mSv/MBq for 90Y-DOTA-BASS (Table 2). The critical normal organs receiving the highest radiation dose were kidneys, spleen, and urinary bladder wall.
Absorbed Radiation Dose of 111In-DOTA-BASS and 90Y-DOTA-BASS
Detection of Tumor Lesions
111In-DOTA-BASS, 111In-DTPA-octreotide, and CT scans detected a total of 28 lesions; 25 were positive with 111In-DOTA-BASS and 17 with 111In-DTPA-octreotide (Supplemental Table 2). All lesions visible on 111In-DTPA-octreotide scans were also detected by 111In-DOTA-BASS, whereas there were 8 lesions on 111In-DOTA-BASS that were not visible on 111In-DTPA-octreotide. There were 3 bone lesions that were negative on both 111In-DOTA-BASS and 111In-DTPA-octreotide scans, but bone metastases were confirmed by serial CT.
DISCUSSION
Our pilot study provides the first clinical evidence that radiolabeled sst antagonists not only detect sst2-expressing neuroendocrine tumors but also may even be superior to sst agonists for imaging and therapy of neuroendocrine tumors. The studied receptor antagonist 111In-DOTA-BASS had a favorable biodistribution profile (higher tumor uptake and lower organ uptake) than the agonist 111In-DTPA-octreotide, resulting in a higher tumor detection rate. The higher tumor uptake of 111In-DOTA-BASS is consistent with preclinical studies that have indicated that 111In-DOTA-BASS can bind to a larger number of sst2 conformations than sst agonists (4). The slightly better receptor affinity of 111In-DOTA-BASS than of 111In-DTPA-octreotide (inhibitory concentration of 50%, 9.4 ± 0.4 nM (4) vs. 22 ± 3.6 nM (14)) may also have contributed to the higher tumor uptake of 111In-DOTA-BASS.
With respect to radionuclide therapy, it is particularly encouraging that tumor-to-kidney ratios were up to 5.2 times higher for the antagonist than for the agonist. The kidneys are the major dose-limiting organ in peptide receptor radionuclide therapy, especially for 90Y-labeled receptor agonists (3,15). On one hand, the severalfold higher tumor-to-kidney uptake ratio could significantly improve the efficacy and toxicity profile of radionuclide therapy with 90Y-labeled sst ligands, especially in patients with moderate 111In-DTPA-octreotide–avid tumor tissue (e.g., our patient collective). On the other hand, sst antagonists may have a negative effect on tumor growth. In vivo studies in rats showed a dose-dependent release of growth hormone growth hormone (GH) after injection of sst antagonists (16). The minimum effective dose necessary to achieve growth hormone release was 0.02 mg/kg (17.4 nmol/kg). The GH-releasing effect lasted about 15 min. It is therefore unlikely that 20–200 μg (14–140 nmol) of DOTA-BASS have any effects on tumor growth. To further evaluate the potential of somatostatin receptor antagonists for radionuclide therapy, we estimated the organ doses of 90Y-DOTA-BASS. For these calculations, we assumed that 90Y-DOTA-BASS shows the same biodistribution as 111In-DOTA-BASS. 111In has been used extensively as surrogate for the pure β-emitter 90Y because it has similar coordination chemistry, a similar physical half-life, and a similar metabolic handling (1,17). Compared with literature data for 90Y-DOTATOC (18,19), 90Y-DOTA-BASS showed lower renal, hepatic, and splenic radiation doses (Table 2).
The lower renal and liver doses can be explained by a charge difference between the 2 compounds. Negatively charged compounds such as 111In-DTPA-octreotide show often higher renal and liver doses than neutral compounds such as 111In- or 90Y-DOTA-BASS (20). The reasons for the low splenic uptake of 111In-DOTA-BASS are currently not clear.
The following limitations of the study should be noted. We have chosen the only Food and Drug Administration– and European Medicines Agency–approved sst imaging agent (111In-DTPA-octreotide) for comparison with our sst2 antagonist 111In-DOTA-BASS. Comparison with unlicensed second-generation sst analogs—for example, 111In-DOTATOC—was not possible because of legal reasons. However, choosing 111In-DTPA-octreotide is feasible because 111In-DTPA-octreotide and 111In-DOTATOC show similar biodistribution in humans, without significantly different tumor and kidney uptake (21).
Only 5 patients were included in this pilot study because the aim of the study was to obtain first clinical data on the potential usefulness of imaging sst-positive tumors with sst antagonists and not to determine the sensitivity and specificity of 111In-DOTA-BASS SPECT in a specific population.
CONCLUSION
This is the first proof of concept showing that imaging of neuroendocrine tumors with sst antagonists is feasible in patients. As suggested by preclinical studies, 111In-DOTA-BASS provided a higher tumor uptake and better visualization of metastatic neuroendocrine tumors than 111In-DTPA-octreotide. We anticipate that the antagonist approach will have significant impact on peptide receptor–mediated imaging and therapy.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
We thank Ulrike Buchegger-Podbielski and Christof Rottenburger at the University Hospital Freiburg for their support of the patient studies. This work was supported by the Swiss National Science Foundation (320000-118333). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Aug. 18, 2011.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication February 7, 2011.
- Accepted for publication May 20, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Somatostatin Receptor Antagonists as a Theranostic Option in Iodine-Refractory Thyroid Carcinoma
- Head-to-Head Comparison of 68Ga-NODAGA-JR11 and 68Ga-DOTATATE PET/CT in Patients with Metastatic, Well-Differentiated Neuroendocrine Tumors: Interim Analysis of a Prospective Bicenter Study
- Somatostatin Receptor Antagonists as a Theranostic Option in Iodine-Refractory Thyroid Carcinoma
- A Randomized, Factorial Phase II Study to Determine the Optimal Dosing Regimen for 68Ga-Satoreotide Trizoxetan as an Imaging Agent in Patients with Gastroenteropancreatic Neuroendocrine Tumors
- First-in-Humans Study of the SSTR Antagonist 177Lu-DOTA-LM3 for Peptide Receptor Radionuclide Therapy in Patients with Metastatic Neuroendocrine Neoplasms: Dosimetry, Safety, and Efficacy
- A Prospective, Randomized, Double-Blind Study to Evaluate the Safety, Biodistribution, and Dosimetry of 68Ga-NODAGA-LM3 and 68Ga-DOTA-LM3 in Patients with Well-Differentiated Neuroendocrine Tumors
- Multimodal Imaging of 2-Cycle PRRT with 177Lu-DOTA-JR11 and 177Lu-DOTATOC in an Orthotopic Neuroendocrine Xenograft Tumor Mouse Model
- Head-to-Head Comparison of 68Ga-DOTA-JR11 and 68Ga-DOTATATE PET/CT in Patients with Metastatic, Well-Differentiated Neuroendocrine Tumors: A Prospective Study
- Phase I Trial of Well-Differentiated Neuroendocrine Tumors (NETs) with Radiolabeled Somatostatin Antagonist 177Lu-Satoreotide Tetraxetan
- Future of Theranostics: An Outlook on Precision Oncology in Nuclear Medicine
- International Union of Basic and Clinical Pharmacology. CV. Somatostatin Receptors: Structure, Function, Ligands, and New Nomenclature
- Safety, Biodistribution, and Radiation Dosimetry of 68Ga-OPS202 in Patients with Gastroenteropancreatic Neuroendocrine Tumors: A Prospective Phase I Imaging Study
- Somatostatin Receptor Imaging of Neuroendocrine Tumors: From Agonists to Antagonists
- Sensitivity Comparison of 68Ga-OPS202 and 68Ga-DOTATOC PET/CT in Patients with Gastroenteropancreatic Neuroendocrine Tumors: A Prospective Phase II Imaging Study
- SSTR-Mediated Imaging in Breast Cancer: Is There a Role for Radiolabeled Somatostatin Receptor Antagonists?
- Somatostatin Receptor Antagonists for Imaging and Therapy
- Biodistribution, Pharmacokinetics, and Dosimetry of 177Lu-, 90Y-, and 111In-Labeled Somatostatin Receptor Antagonist OPS201 in Comparison to the Agonist 177Lu-DOTATATE: The Mass Effect
- Proof of Therapeutic Efficacy of a 177Lu-Labeled Neurotensin Receptor 1 Antagonist in a Colon Carcinoma Xenograft Model
- Citius, Altius, Fortius: An Olympian Dream for Theranostics
- Highly Increased 125I-JR11 Antagonist Binding In Vitro Reveals Novel Indications for sst2 Targeting in Human Cancers
- Molecular Imaging of Gastroenteropancreatic Neuroendocrine Tumors: Current Status and Future Directions
- Comparative Evaluation of the Biodistribution Profiles of a Series of Nonpeptidic Neurotensin Receptor-1 Antagonists Reveals a Promising Candidate for Theranostic Applications
- Comparison of the Therapeutic Response to Treatment with a 177Lu-Labeled Somatostatin Receptor Agonist and Antagonist in Preclinical Models
- Radiopeptides for Imaging and Therapy: A Radiant Future
- Development of 68Ga- and 89Zr-Labeled Exendin-4 as Potential Radiotracers for the Imaging of Insulinomas by PET
- N-Terminal Modifications Improve the Receptor Affinity and Pharmacokinetics of Radiolabeled Peptidic Gastrin-Releasing Peptide Receptor Antagonists: Examples of 68Ga- and 64Cu-Labeled Peptides for PET Imaging
- Comparison of Somatostatin Receptor Agonist and Antagonist for Peptide Receptor Radionuclide Therapy: A Pilot Study
- Targeted Radionuclide Therapy: Proceedings of a Joint Workshop Hosted by the National Cancer Institute and the Society of Nuclear Medicine and Molecular Imaging
- PulmoBind, an Adrenomedullin-Based Molecular Lung Imaging Tool
- Evaluation of 177Lu-DOTA-sst2 Antagonist Versus 177Lu-DOTA-sst2 Agonist Binding in Human Cancers In Vitro