


Abstract
Preclinical and clinical studies have indicated that somatostatin receptor (sst)–expressing tumors demonstrate higher uptake of radiolabeled sst antagonists than of sst agonists. In 4 consecutive patients with advanced neuroendocrine tumors, we evaluated whether treatment with 177Lu-labeled sst antagonists is feasible. Methods: After injection of approximately 1 GBq of 177Lu-DOTA-[Cpa-c(DCys-Aph(Hor)-DAph(Cbm)-Lys-Thr-Cys)-DTyr-NH2] (177Lu-DOTA-JR11) and 177Lu-DOTATATE, 3-dimensional voxel dosimetry analysis based on SPECT/CT was performed. A higher tumor-to-organ dose ratio for 177Lu-DOTA-JR11 than for 177Lu-DOTATATE was the prerequisite for treatment with 177Lu-DOTA-JR11. Results: Reversible minor adverse effects of 177Lu-DOTA-JR11 were observed. 177Lu-DOTA-JR11 showed a 1.7–10.6 times higher tumor dose than 177Lu-DOTATATE. At the same time, the tumor-to-kidney and tumor–to–bone marrow dose ratio was 1.1–7.2 times higher. All 4 patients were treated with 177Lu-DOTA-JR11, resulting in partial remission in 2 patients, stable disease in 1 patient, and mixed response in the other patient. Conclusion: Treatment of neuroendocrine tumors with radiolabeled sst antagonists is clinically feasible and may have a significant impact on peptide receptor radionuclide therapy.
Radiolabeled somatostatin receptor (sst) agonists, for example, 177Lu-DOTATATE, have become an integral part of therapeutic management in patients with neuroendocrine tumors (1). Radiolabeled sst antagonists are not established for tumor targeting, mainly because they do not internalize into tumor cells. Ginj et al., however, were the first to show in animal studies that radiolabeled sst antagonists are superior to agonists for targeting of tumors (2). A possible explanation may be that antagonists bind to a larger population of binding sites than agonists (2). Scatchard analysis in sst subtype 2 (sst2)–transfected HEK293 cells showed more than 10 times the number of binding sites for the sst antagonist 111In-DOTA-[p-NO2-Phe-c(DCys-Tyr-DTrp-Lys-Thr-Cys)-DTyr-NH2] (111In-DOTA-BASS) than for the sst agonist [111In-DTPA0,Tyr3,Thr8]-octreotide. Furthermore, in vitro receptor autoradiography showed about 4 times higher accumulation of 177Lu-DOTA-BASS in sst2-expressing human tumor samples than did the sst agonist (3). These results were confirmed clinically in a pilot imaging study with 111In-DOTA-BASS and 111In-pentetreotide (111In-DTPA-octreotide) (4). Unfortunately, 111In-DOTA-BASS has a relatively low sst2 affinity (2). To overcome this problem, the next generation of sst antagonists was synthesized to improve the receptor affinity. From a small library, 177Lu-DOTA-[Cpa-c(DCys-Aph(Hor)-DAph(Cbm)-Lys-Thr-Cys)-DTyr-NH2] (177Lu-DOTA-JR11) showed the highest sst2 affinity (5).
The purpose of this pilot study was to evaluate the feasibility of peptide receptor radionuclide therapy with the novel sst antagonist 177Lu-DOTA-JR11. Before treatment, tumor and organ doses of 177Lu-DOTATATE and 177Lu-DOTA-JR11 were compared in the same patient after injection of a nontherapeutic test dose. A higher tumor-to-organ dose ratio for 177Lu-DOTA-JR11 than for 177Lu-DOTATATE was the prerequisite for treatment with 177Lu-DOTA-JR11.
MATERIALS AND METHODS
Patients
Four consecutive patients with progressive neuroendocrine tumors and limited treatment options due to chronic grade 2 or 3 kidney disease were prospectively recruited. Patient characteristics are summarized in Table 1. Exclusion criteria were concurrent antitumor treatment (octreotide [Sandostatin; Novartis Pharmaceuticals] depot less than 4 wk before test injection and treatment), preexisting grade 3 and 4 hematologic toxicity, and pregnancy or breastfeeding. The institutional review board approved this study, and all subjects gave written informed consent in accordance with the Declaration of Helsinki.
Characteristics of Patients with Neuroendocrine Tumors and Chronic Kidney Insufficiency
Radiochemistry
DOTA-JR11 was synthesized as previously described (5). DOTATATE was received from piChem (Austria). For the preparation of 177Lu-DOTA-JR11 and 177Lu-DOTATATE, the corresponding peptide conjugate was dissolved in 500 μL of ascorbate buffer, pH 5.0, and 177LuCl3 was added. The solution was incubated at 95°C for 30 min. Quality control was performed by analytic reverse-phase high-performance liquid chromatography on a Phenomenex Jupiter C18 4-μm, 250 × 4.6 mm column (eluents, A = 0.1% trifluoroacetic acid in water and B = acetonitrile; gradient, 0–25 min, 95%–50% A; flow, 0.75 mL/min). The labeling yield of 177Lu-DOTATATE and 177Lu-DOTA-JR11 was more than 99% and the radiochemical purity of 177Lu-DOTA-JR11 was at least 93%. Sterile filtration of the final product was performed before application to the patient.
Test Injection: Pharmacokinetics and Dosimetry
Tumor and organ doses of 177Lu-DOTA-JR11 and 177Lu-DOTATATE were compared in the same patient using a cross-over design in an interval of 3 wk. Blood sampling, whole-body imaging studies, and SPECT/CT of the abdomen were used to generate pharmacokinetic data. All studies were done with the same SPECT/CT scanner (BrightView XCT; Philips) equipped with medium-energy, parallel-hole collimators. Whole-body scanning and low-dose SPECT/CT were performed at 1, 3, 24, and 72 h after injection of a mean dose (±SD) of 175 ± 15 μg (range, 160–200 μg) (1,060 ± 75 MBq [range, 990–1,130 MBq]) of 177Lu-DOTATATE and 150 ± 20 μg (range, 130–165 μg) (975 ± 115 MBq [range, 850–1,085 MBq]) of 177Lu-DOTA-JR11. One hour before injection of both radiopeptides, an infusion of 1,000 mL of physiologic NaCl solution containing 20.7 mg of arginine per milliliter and 20.0 mg of lysine per milliliter was started and continued for 5 h to inhibit tubular reabsorption of radiopeptides. The patient’s vital parameters such as blood pressure, pulse rate, oxygen saturation, and electrocardiogram were monitored for at least 50 min after injection of 177Lu-DOTA-JR11.
To avoid organ- and tumor-activity overlap, a 3-dimensional quantification technique using SPECT/CT information was used for the calculation of tumor and kidney doses (IMALYTICS workstation and STRATOS software; Philips) (6). SPECT images were corrected for scatter and attenuation. A calibration factor was determined using a water-filled cylinder phantom with three 177Lu-filled spheres. Voxelwise residence time maps were calculated by integrating the time–activity curves using a monoexponential tail-fitting, and the mean absorbed tumor and kidney doses were calculated (7). Bone marrow doses were determined by blood-based red-marrow dose methodology (4). Blood samples were taken at 13 time points up to 22.5 h after injection. Urine samples were collected at 1.5, 3, 5, 8, and 21 h after injection to study the stability of 177Lu-DOTA-JR11. Two-dimensional dosimetry technique was used for the calculation of all remaining organs (OLINDA/EXAM 1.0 software; Microsoft) as described before (4).
Treatment: Response and Adverse Events
Patients received 2–3 cycles of 177Lu-DOTA-JR11 (105 ± 35 μg [range, 55–160 μg] [4,120 ± 1,260 MBq (range, 1,870–5,890 MBq)] per treatment cycle) in an interval of 8 wk. The amount of activity and number of treatment cycles was chosen on the basis of kidney dosimetry calculations. None of the patients received a kidney dose of more than 23 Gy. Kidney protection was performed in the same way as described above. The imaging and blood-sampling protocol were the same as for the test injections, with the same imaging and blood-sampling time points. As for the test injections, 3-dimensional voxel-based technique was used for the calculation of tumor and kidney doses. The doses of the remaining organs were calculated with 2-dimensional dosimetry technique as described above (4).
Initial staging, eligibility, and follow-up measurements were based on 68Ga-DOTATATE PET/CT imaging, 99mTc-mercaptoacetyltriglycine renography, and laboratory and clinical results. Initial staging was performed less than 2 wk before the first test-injection. Blood tests were performed every 3 wk between treatment cycles and every 3–4 mo thereafter. Morphologic response and tubular kidney function were evaluated 3 and 12 mo after treatment by 68Ga-DOTATATE PET/CT and 99mTc-mercaptoacetyltriglycine renography using a standard protocol (8,9). The CT scans were performed without contrast medium to avoid further kidney toxicity. 68Ga-DOTATATE PET/CT scans were assessed independently by 1 experienced nuclear medicine physician and 1 experienced radiologist unaware of the date of the scan and patients’ identity. Any discrepant readings were resolved by consensus.
RESULTS
Pharmacokinetics, Dosimetry, and Response
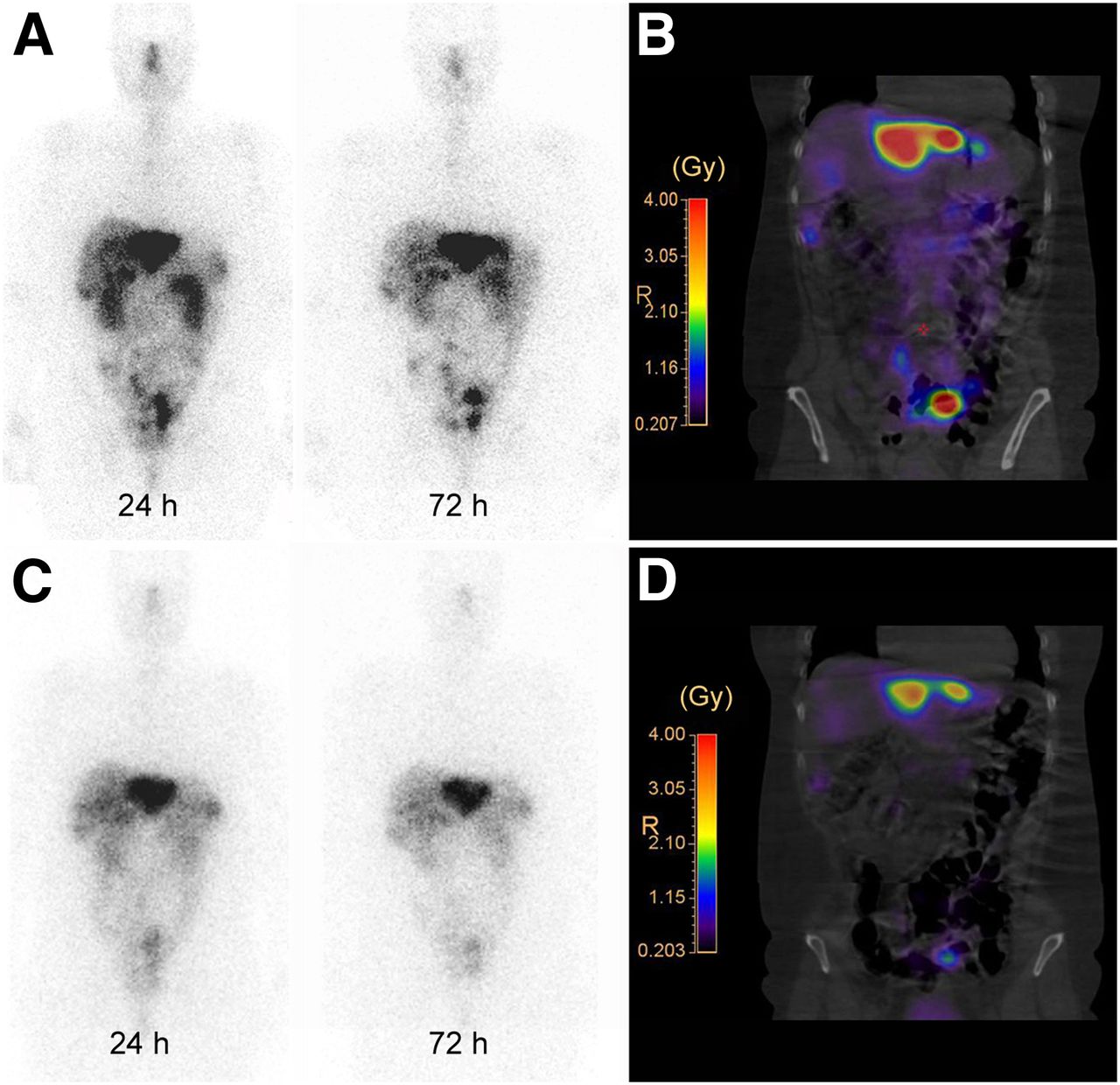
The blood clearance was similar for 177Lu-DOTA-JR11 and 177Lu-DOTATATE: α half-life, 8 ± 6 min versus 10 ± 6 min, and β half-life, 8.8 ± 1.4 h versus 7.8 ± 2.5 h; approximately 65% of the administered activity was cleared in the α phase. Excretion was predominantly renal and no metabolites were found in the urine, indicating a high metabolic stability of 177Lu-DOTA-JR11. 177Lu-DOTA-JR11 showed a longer intratumoral residence time and higher tumor uptake than 177Lu-DOTATATE in all 4 patients (between 1.3 and 2.8 times longer residence time and between 1.1 and 2.6 times higher tumor uptake), resulting in a 1.7–10.6 times higher tumor dose (Figs. 1 and 2). 177Lu-DOTA-JR11 has 1.1–7.2 times higher tumor-to-kidney and tumor–to–bone marrow dose ratios than 177Lu-DOTATATE. As a result, all 4 patients were treated with 2–3 treatment cycles of 177Lu-DOTA-JR11. Table 2 shows the results of tumor dose calculations, tumor-to-kidney dose ratios, tumor–to–bone marrow dose ratios, and 3-mo follow-up. Table 1 and Figure 3 show the remission status before our treatment, after 3-mo of follow-up, and after maximum follow-up. Organ and effective doses of 177Lu-DOTA-JR11 and 177Lu-DOTATATE are given in Table 3.

177Lu-DOTA-JR11 planar scans (A) and isodose curves (B) of patient 2 after injection of 1,065 MBq of 177Lu-DOTA-JR11 and corresponding 177Lu-DOTATATE planar scans (C) and isodose curves (D) after injection of 1,115 MBq of 177Lu-DOTATATE. Planar scans (A and C) show results 24 and 72 h after injection of 177Lu-DOTA-JR11 and 177Lu-DOTATATE.
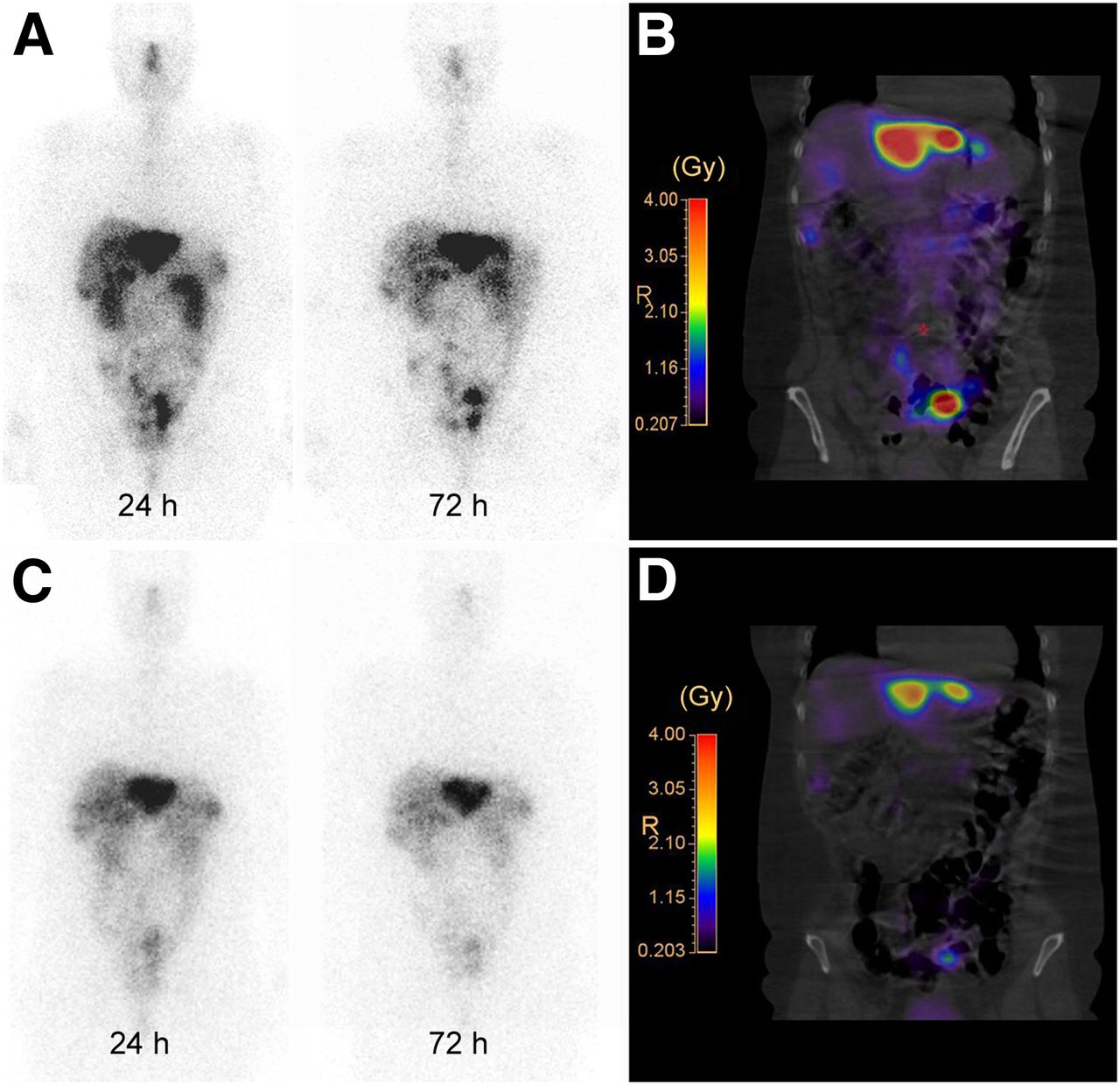
177Lu-DOTA-JR11 planar scans (A) and isodose curves (B) of patient 3 after injection of 850 MBq of 177Lu-DOTA-JR11 and corresponding 177Lu-DOTATATE planar scans (C) and isodose curves (D) after injection of 990 MBq of 177Lu-DOTATATE. Planar scans (A and C) show results 24 and 72 h after injection of 177Lu-DOTA-JR11 and 177Lu-DOTATATE.
Summary of Tumor Dose Calculations and Treatment Response of Delineable Tumors
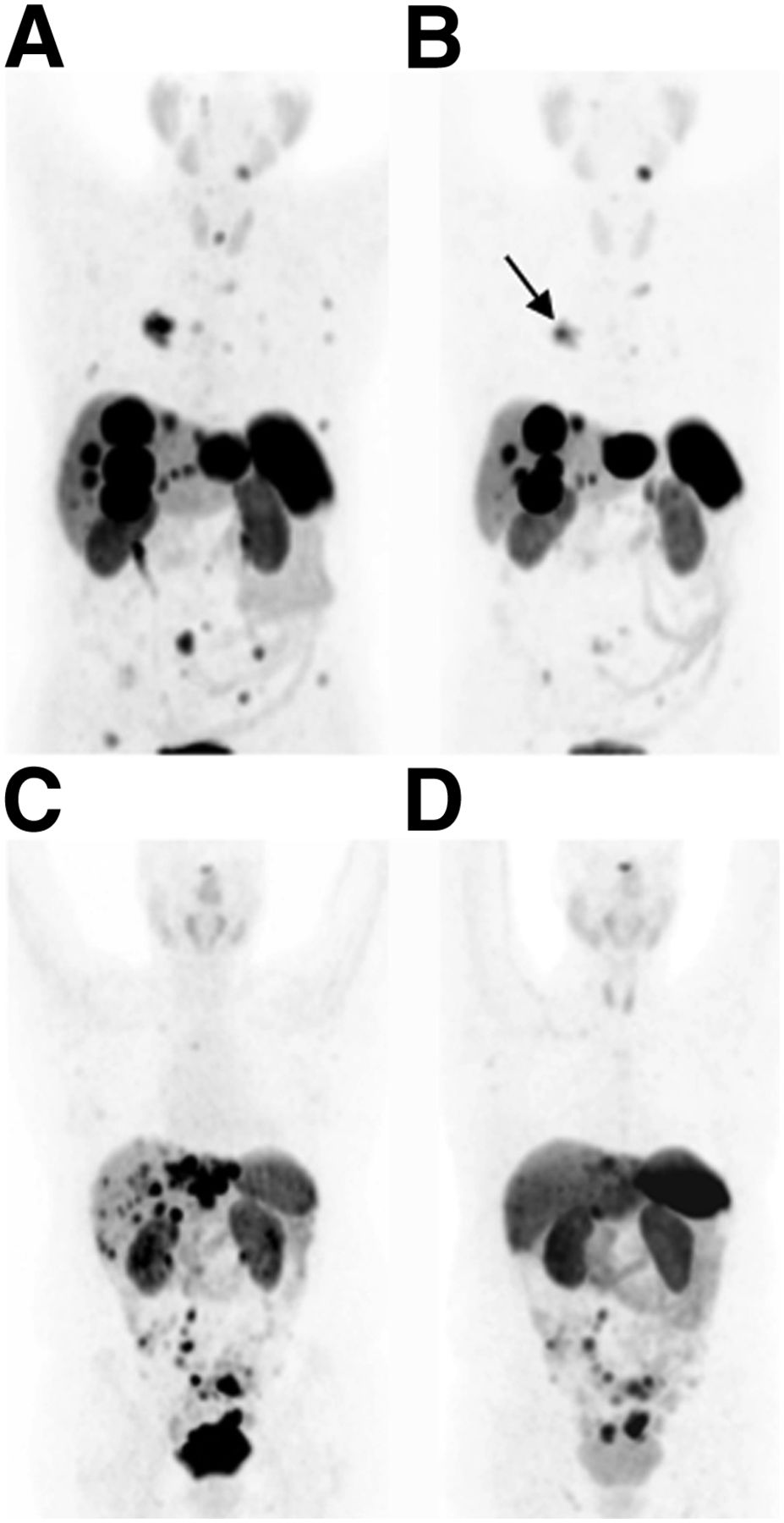
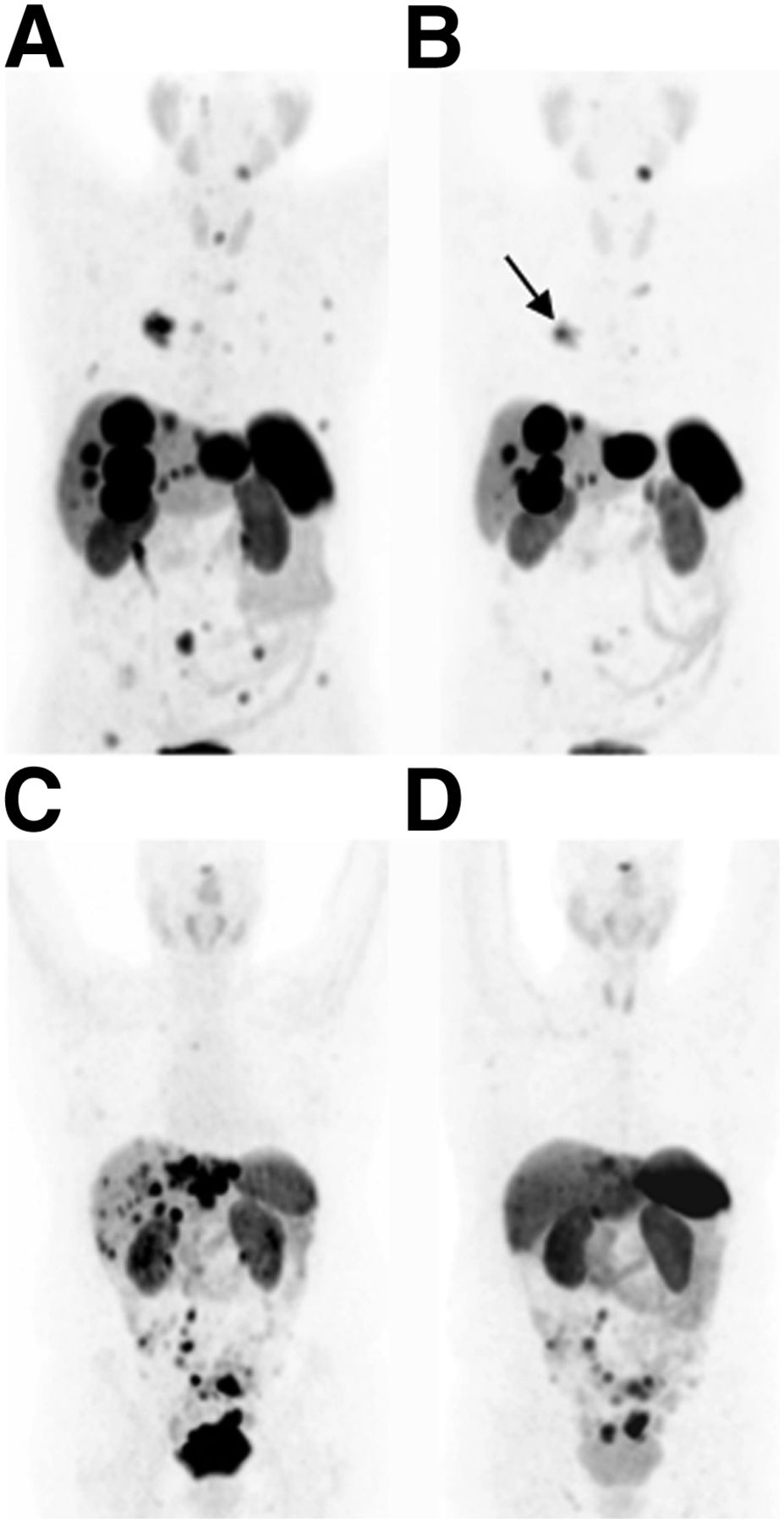
68Ga-DOTATATE PET images of patient 2 before (A) and 3 mo after (B) treatment with 15.2 GBq of 177Lu-DOTA-JR11 and 68Ga-DOTATATE PET images of patient 3 before (C) and 12 mo after (D) treatment with 5.9 GBq of 177Lu-DOTA-JR11. Three-month follow-up scan of patient 2 (B) shows decreased uptake by metastatic liver and bone disease and by primary tumor in right lung (arrow). Twelve-month follow-up scan of patient 3 (D) shows decreased uptake by metastatic liver disease.
Comparison of 177Lu-DOTATATE and 177Lu-DOTA-JR11 Organ and Effective Doses of 4 Patients with Neuroendocrine Tumors or Carcinomas
Adverse Events
One patient experienced a short episode of flush just after injection of 177Lu-DOTA-JR11. Another patient developed grade 3 thrombocytopenia (41,000/mm3), which completely recovered within 8 wk after injection of 177Lu-DOTA-JR11 (Table 1). There was no relevant decrease of tubular kidney function within 12 mo of follow-up (mercaptoacetyltriglycine clearance, 135 ± 11 mL/min/1.73 m2 vs. 126 ± 13 mL/min/1.73 m2). Also, creatinine levels did not much change before and approximately 12 mo after treatment (1.32 ± 0.13 mg/dL vs. 1.39 ± 0.10 mg/dL).
DISCUSSION
Our pilot study provided the first clinical evidence that radiolabeled sst antagonists may be superior to sst agonists for the treatment of neuroendocrine tumors. The sst2-receptor antagonist 177Lu-DOTA-JR11 had a favorable pharmacokinetic and biodistribution profile (longer intratumoral residence time and higher tumor uptake) compared with the agonist 177Lu-DOTATATE, resulting in 1.7–10.6 times higher tumor doses.
It is particularly encouraging that tumor-to-kidney and tumor–to–bone marrow dose ratios were up to 6.2 and 7.2 times higher for the antagonist than for the agonist. The kidneys and the bone marrow are the major dose-limiting organs in peptide receptor radionuclide therapy (1). Therefore, severalfold higher tumor-to-kidney and tumor–to–bone marrow dose ratios of 177Lu-DOTA-JR11 could significantly improve the efficacy and toxicity profile of radionuclide therapy when using only 50% of the cumulative activity of 177Lu-DOTATATE. According to our study results, the cumulative standard activity of 29.6 GBq of 177Lu-DOTATATE (10) will result in a median tumor dose of 59 Gy, a mean bone marrow dose of 2.3 Gy, and a mean kidney dose of 36 Gy. When treating patients with 177Lu-DOTA-JR11, the median tumor dose will be 104 Gy, the mean bone marrow dose will be 1.5 Gy, and the mean kidney dose will be 27 Gy if using only 50% of the standard dose (14.8 GBq) of 177Lu-DOTATATE. Actually, efficacy (2 patients with a partial response, 1 with stable disease, and 1 with a mixed response) and toxicity profiles (no grade 4 toxicity) are encouraging in our first 4 patients after treatment with 177Lu-DOTA-JR11.
The small number of patients is the most relevant limitation of this study. Nevertheless, the 3-dimensional voxel-based dosimetry approach together with the low-activity treatment approach in the same patient using a cross-over design allowed the direct comparison of 177Lu-DOTA-JR11 and 177Lu-DOTATATE dosimetry in 13 tumor lesions.
CONCLUSION
This pilot study provided the first clinical evidence, to our knowledge, that treatment of neuroendocrine tumors with radiolabeled sst antagonists is clinically feasible. If the favorable tumor-to-organ dose ratios are confirmed in larger studies, radiopeptide treatment with sst antagonists may improve peptide receptor radionuclide therapy in neuroendocrine tumors. Systematic clinical studies with radiolabeled DOTA-JR11 for imaging and therapy of neuroendocrine tumors are in preparation.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Jean E.F. Rivier, Jean Claude Reubi, and Helmut R. Maecke, who are coinventors of somatostatin-based antagonistic radiopeptides, assigned all their patent rights to their respective academic institutions. This work was supported by the Swiss National Science Foundation (320000-118333) and the German Cancer Consortium (DKTK). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the University Hospital Freiburg staff, in particular Christian Lohrmann, for reading the 68Ga-DOTATATE PET/CT scans and R. Tönnesmann for technical support. Jean E. F. Rivier is “The Dr. Frederik Paulsen Chair in Neurosciences Professor.”
Footnotes
Published online Jun. 24, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication February 10, 2014.
- Accepted for publication May 9, 2014.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Side-by-Side Comparison of the In Vivo Performance of [212Pb]Pb-DOTAMTATE and Other SSTR2-Targeting Compounds
- Limitations of the radiotheranostic concept in neuroendocrine tumors due to lineage-dependent somatostatin receptor expression on hematopoietic stem and progenitor cells
- Radiolabeled Somatostatin Receptor Antagonist Versus Agonist for Peptide Receptor Radionuclide Therapy in Patients with Therapy-Resistant Meningioma: PROMENADE Phase 0 Study
- Somatostatin Receptor Antagonists as a Theranostic Option in Iodine-Refractory Thyroid Carcinoma
- 68Ga-SSO-120 PET for Initial Staging of Small Cell Lung Cancer Patients: A Single-Center Retrospective Study
- Somatostatin Receptor Antagonists as a Theranostic Option in Iodine-Refractory Thyroid Carcinoma
- The Emergence of Somatostatin Antagonist-Based Theranostics: Paving the Road Toward Another Success?
- First-in-Humans Study of the SSTR Antagonist 177Lu-DOTA-LM3 for Peptide Receptor Radionuclide Therapy in Patients with Metastatic Neuroendocrine Neoplasms: Dosimetry, Safety, and Efficacy
- Treatment of advanced gastroenteropancreatic neuroendocrine neoplasia, are we on the way to personalised medicine?
- 177Lu-DOTA-EB-TATE, a Radiolabeled Analogue of Somatostatin Receptor Type 2, for the Imaging and Treatment of Thyroid Cancer
- Multimodal Imaging of 2-Cycle PRRT with 177Lu-DOTA-JR11 and 177Lu-DOTATOC in an Orthotopic Neuroendocrine Xenograft Tumor Mouse Model
- Head-to-Head Comparison of 68Ga-DOTA-JR11 and 68Ga-DOTATATE PET/CT in Patients with Metastatic, Well-Differentiated Neuroendocrine Tumors: A Prospective Study
- Cholecystokinin 2 Receptor Agonist 177Lu-PP-F11N for Radionuclide Therapy of Medullary Thyroid Carcinoma: Results of the Lumed Phase 0a Study
- NANETS/SNMMI Consensus Statement on Patient Selection and Appropriate Use of 177Lu-DOTATATE Peptide Receptor Radionuclide Therapy
- Phase I Trial of Well-Differentiated Neuroendocrine Tumors (NETs) with Radiolabeled Somatostatin Antagonist 177Lu-Satoreotide Tetraxetan
- Future of Theranostics: An Outlook on Precision Oncology in Nuclear Medicine
- Medical Management of Gastroenteropancreatic Neuroendocrine Tumors: Current Strategies and Future Advances
- New Developments in Peptide Receptor Radionuclide Therapy
- The Relevance of Dosimetry in Precision Medicine
- Somatostatin Receptor Imaging of Neuroendocrine Tumors: From Agonists to Antagonists
- Sensitivity Comparison of 68Ga-OPS202 and 68Ga-DOTATOC PET/CT in Patients with Gastroenteropancreatic Neuroendocrine Tumors: A Prospective Phase II Imaging Study
- 177Lu-3BP-227 for Neurotensin Receptor 1-Targeted Therapy of Metastatic Pancreatic Adenocarcinoma: First Clinical Results
- Somatostatin Antagonists for Radioligand Therapy of Nonendocrine Tumors
- Repeated 177Lu-Labeled PSMA-617 Radioligand Therapy Using Treatment Activities of Up to 9.3 GBq
- Advantages and Limits of Targeted Radionuclide Therapy with Somatostatin Antagonists
- SSTR-Mediated Imaging in Breast Cancer: Is There a Role for Radiolabeled Somatostatin Receptor Antagonists?
- Clinical History of the Theranostic Radionuclide Approach to Neuroendocrine Tumors and Other Types of Cancer: Historical Review Based on an Interview of Eric P. Krenning by Rachel Levine
- Somatostatin Receptor 2-Targeting Compounds
- Biodistribution, Pharmacokinetics, and Dosimetry of 177Lu-, 90Y-, and 111In-Labeled Somatostatin Receptor Antagonist OPS201 in Comparison to the Agonist 177Lu-DOTATATE: The Mass Effect
- Glu-Ureido-Based Inhibitors of Prostate-Specific Membrane Antigen: Lessons Learned During the Development of a Novel Class of Low-Molecular-Weight Theranostic Radiotracers
- Somatostatin Receptor Antagonists for Imaging and Therapy
- Clinical Trial with Sodium 99mTc-Pertechnetate Produced by a Medium-Energy Cyclotron: Biodistribution and Safety Assessment in Patients with Abnormal Thyroid Function
- Highly Increased 125I-JR11 Antagonist Binding In Vitro Reveals Novel Indications for sst2 Targeting in Human Cancers
- Citius, Altius, Fortius: An Olympian Dream for Theranostics
- Comparison of the Therapeutic Response to Treatment with a 177Lu-Labeled Somatostatin Receptor Agonist and Antagonist in Preclinical Models
- Radiopeptides for Imaging and Therapy: A Radiant Future
- Radioisotopic Purity of Sodium Pertechnetate 99mTc Produced with a Medium-Energy Cyclotron: Implications for Internal Radiation Dose, Image Quality, and Release Specifications
- Carcinoid and Neuroendocrine Tumors: Building on Success
- In Vitro and In Vivo Application of Radiolabeled Gastrin-Releasing Peptide Receptor Ligands in Breast Cancer
- Triple-Peptide Receptor Targeting In Vitro Allows Detection of All Tested Gut and Bronchial NETs
- Targeting Neuropeptide Receptors for Cancer Imaging and Therapy: Perspectives with Bombesin, Neurotensin, and Neuropeptide-Y Receptors