


Abstract
Neurotensin receptor 1 (NTR1) is overexpressed in ductal pancreatic adenocarcinoma, which is still one of the deadliest cancers, with a very poor prognosis. Eligible patients were offered salvage radiopharmaceutical therapy with the novel NTR1 antagonist 177Lu-3BP-227. Methods: Six patients with confirmed ductal pancreatic adenocarcinoma who had exhausted all other treatment options received 177Lu-3BP-227 for evaluation of NTR1 expression in vivo. Three patients received treatment activities of 5.1–7.5 GBq. Results: Administration of 177Lu-3BP-227 was well tolerated by all patients. The kidneys were identified as the dose-limiting organ. The most severe adverse event was reversible grade 2 anemia. One patient achieved a partial response and experienced significant improvement of symptoms and quality of life. This patient survived 13 mo from diagnosis and 11 mo from the start of 177Lu-3BP-227 therapy. Conclusion: This initial report provides clinical evidence of the feasibility of treatment of ductal pancreatic adenocarcinoma using 177Lu-3BP-227.
- pancreatic adenocarcinoma
- neurotensin receptor 1 antagonist
- targeted radioligand therapy
- TRLT
- dosimetry
- 177Lu
Pancreatic adenocarcinoma has an extremely poor prognosis. Mortality virtually equals incidence, and the 5-y survival rate of metastatic pancreatic adenocarcinoma is less than 5% (1). In particular, patients with new-onset ascites have a life expectancy of approximately 2 mo only, and death is typically due to inanition rather than to a large tumor burden. At the time of diagnosis, most patients are ineligible for surgery because of metastatic spread or local tumor invasion (2). For metastatic disease, current treatment options are limited to cytotoxic chemotherapy (1).
Neurotensin receptor 1 (NTR1) is highly expressed in ductal pancreatic adenocarcinoma but not in normal pancreatic tissue or chronic pancreatitis (3). Furthermore, the incidence of NTR1 expression and receptor density increases with higher malignancy of the pancreatic lesion, and hepatic metastases express NTR1 at an intensity similar to that of the primary tumor (4). The restricted expression in normal tissues—limited to the central nervous system and the intestinal tract (5)—makes NTR1 a promising target for targeted radioligand therapy (TRLT) of ductal pancreatic adenocarcinoma.
3BP-227 is a DOTA-conjugated NTR1 antagonist that has been developed on the basis of the previously described SR142948A (6). In a NTR1-positive HT29 xenograft model, 177Lu-labeled 3BP-227 significantly inhibited tumor growth and resulted in a 9-fold increase in tumor doubling time, as well as a tumor growth delay of more than 5 wk (7).
Here, we report our initial experience with TRLT using 177Lu-3BP-227 in patients with metastatic pancreatic adenocarcinoma after exhaustion of all other treatment options.
MATERIALS AND METHODS
Patients and Regulatory Issues
177Lu-3BP-227 was administered as salvage therapy to 6 pancreatic adenocarcinoma patients (whose condition allowed doing so) in accordance with paragraph 37 of the updated Declaration of Helsinki, “Unproven Interventions in Clinical Practice,” and in accordance with the German Medical Products Act (AMG §13 2b). Each therapy was approved individually by a certified institutional tumor board. Because this is a retrospective report on findings for regular clinical care and not a systematic clinical trial, the need for additional approval by an ethics committee was waived. All patients signed a detailed informed consent form before undergoing the treatment, as well as consenting to the use of their anonymized clinical data for scientific purposes. Patient characteristics are given in Table 1.
Patient Demographic and Clinical Characteristics
Radiopharmaceuticals
Good-manufacturing-practice–grade 3BP-227 was manufactured by Soneas Research Ltd. A 25-μg (22.1 nmol) quantity of 3BP-227 per 1 GBq of 177Lu (non–carrier-added; ITG) was dissolved in 0.4 mL of buffer (0.4 M acetate, 0.325 M gentisic acid, pH 5.5). 3BP-227 dissolved in buffer was mixed with 177Lu and heated to 85°C for 30 min. The compound-to-radioactivity ratio was chosen to yield a specific activity of approximately 45 MBq/nmol for the final preparation—an activity that is routinely achieved and clinically accepted for DOTA-conjugated compounds (8,9)
Quality control was performed using thin-layer chromatography and high-performance liquid chromatography. For the latter, the labeling solution was analyzed with an Aeris 3.6-μm peptide XB-C18 column (100 × 4.6 mm; Phenomenex). Solvent A was 0.1% trifluoroacetic acid in MeCN, and solvent B was 0.1% trifluoroacetic acid in H2O. The gradient was 100% B to 100% A within 20 min, at a flow rate of 0.8 mL/min, using a NaI detector (Raytest) and a 254-nm diode array detector. The retention time of the labeled product was 9.9 min. For thin-layer chromatography analysis, 2 μL of the labeling solution were analyzed using an instant thin-layer chromatography salicylic acid system (10 × 1 cm; Varian) in citrate buffer (0.1 M, pH 5) and a Raytest miniGITA. The radiochemical yield and radiochemical purity were at least 95%.
Formulation for Intravenous Injection
If the high-performance liquid chromatography result conformed to the specifications (radiochemical yield and purity ≥ 95%), the reaction mixture was diluted with 0.9% NaCl solution to a volume of 2 mL. After retrieval of reference samples and samples for sterility testing, 0.9% NaCl solution was added to a final volume of 10 mL using a μ DDS-A unit (Tema Sinergie). This step included sterile filtration and dispensing into a shielded syringe.
Sterility and Pyrogen Tests
The limulus amebocyte lysate test for pyrogen concentration was performed on-site using a nonradioactive solution of 3BP-227 in 0.4 M sodium acetate buffer. The result was available before administration of 177Lu-3BP-227. Sterility of the radiolabeled product was determined on-site at the Zentralklinik Bad Berka according to chapter 2.6.1 of the European Pharmacopoeia. All master batches during setup of the radiolabeling procedure were tested for sterility; thus, it was established that the product of the radiolabeling procedure generally conforms to sterility specifications (no growth). The test results for individual batches became available after administration.
Scintigraphy and SPECT/CT Imaging
The kinetics of 177Lu-3BP-227 were determined on the basis of 5 planar whole-body scintigraphy studies in defined time order after administration of the radiopharmaceutical. Acquisition of scans for dosimetry studies began immediately after infusion and continued for up to 119 h using a Spirit DH-V dual-head γ-camera (Mediso), medium-energy general-purpose collimator, 15% energy window, 208-keV peak, and 15 cm/min speed. Scintigrams were analyzed using regions of interest. After geometric mean and background correction, time-dependent time–activity curves were obtained and fitted to mono- or biexponential functions using OriginPro software (version 8.1G; OriginLab Corp.).
Dosimetry Calculations
The dosimetric approach was based on the MIRD scheme. The residence time, cumulated activity, uptake, and effective half-life were calculated, and the mean absorbed doses were estimated using the OLINDA/EXM software. Uptake values were calculated as percentage injected activity, and effective half-lives, residence times, and mean absorbed organ and tumor doses were obtained for whole body, normal tissues, and organs, as well as for tumor lesions that were large enough and sufficiently distinguishable from the surrounding tissue to allow the definition of a region of interest. For lesions that were too small to allow clear demarcation, dosimetry was not calculated. The regions of interest for normal tissue and background were placed over those regions showing no tumor involvement.
Treatment Procedure
To prevent nausea and emesis, 8 mg of ondansetron and 8 mg of dexamethasone were injected before therapy. 177Lu-3BP-227 was administered intravenously over 10–15 min using a dedicated infusion system. 177Lu-3BP-227 was administered intraperitoneally under ultrasound guidance. Dexamethasone (4 mg) was given orally for 3 consecutive days after 177Lu-3BP-227 therapy.
The administered activity was individually chosen on the basis of uptake in the tumor lesions after infusion of 1.2–1.5 GBq of 177Lu-3BP-227, thus applying a scheme similar to that used by Wild et al. for the evaluation of 177Lu-DOTA-JR11 (10). Treatment planning was based on the clinical condition of the patient, the patient’s hematologic and renal function, and the practical guidance on peptide receptor radionuclide therapy (8).
All patients received 177Lu-3BP-227 intravenously. However, patient 3 received the second, third, and fourth TRLT intraperitoneally because of the presence of extensive peritoneal carcinomatosis (11,12).
Clinical, Radiologic, and Laboratory Follow-up
The records of the patients were reviewed for any incidence of hematologic, gastrointestinal, or other adverse events. Circumstances that resulted in cessation or delay in treatment were documented. Alterations in carbohydrate antigen 19-9 serum levels were also evaluated.
The referring physicians or oncologists systematically followed up all patients after therapy by determining relevant laboratory parameters every 2 wk. If the patient’s general condition allowed, an 18F-FDG PET/CT study was performed 8–12 wk after therapy and was used to determine treatment efficacy.
RESULTS
Patients 1 and 2
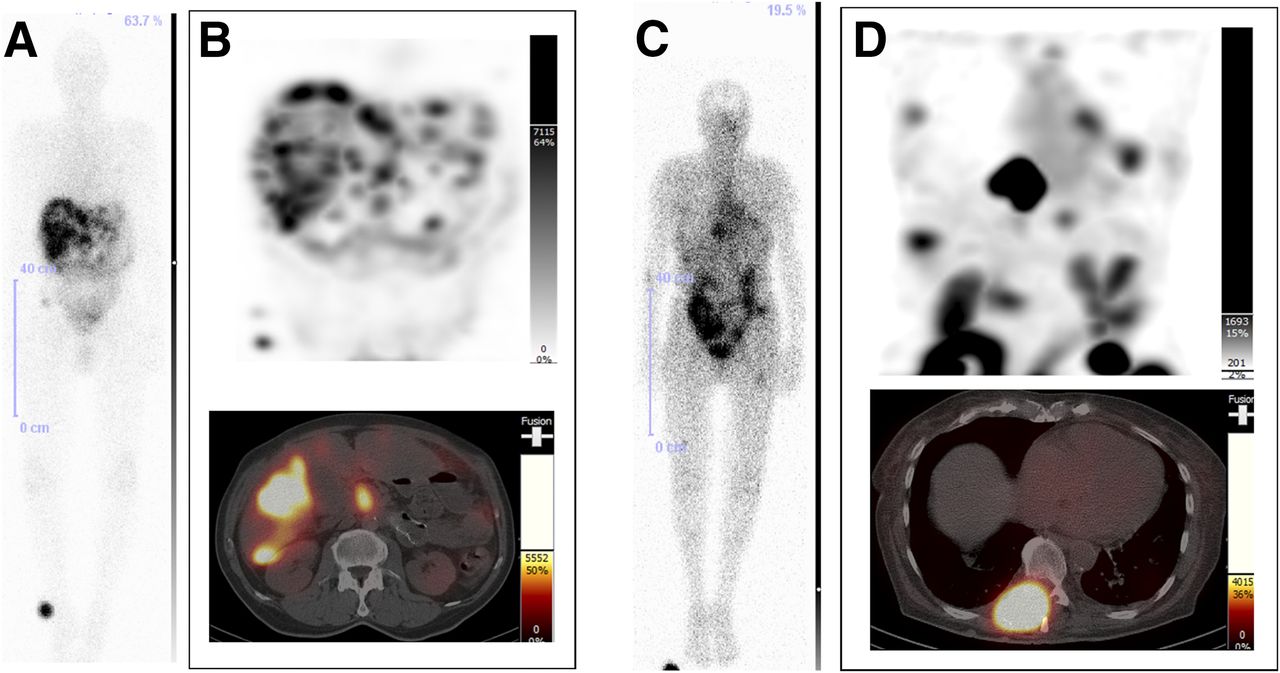
Patients 1 and 2 presented with very advanced pancreatic adenocarcinoma with extensive metastases. Patient 1 had unresectable disease (Supplemental Fig. 1 shows an 18F-FDG PET scan for this patient; supplemental materials are available at http://jnm.snmjournals.org) and categorically refused chemotherapy. Patient 2 had a treatment history of 56 mo with several different chemotherapeutic regimens, including oxaliplatin, gemcitabine, FOLFIRI (folinic acid/fluorouracil/irinotecan), and nab-paclitaxel. Both patients received an intravenous application of 177Lu-3BP-227 (1.2 GBq in patient 1 and 1.5 GBq in patient 2), which was tolerated without any side effects. In both patients, there was excellent uptake of 177Lu-3BP-227 in the primary tumors and metastases (Fig. 1; Table 2). However, further treatment and follow-up were prevented by death within 2 wk after dosimetry in patient 1 and by the identification of a previously unknown brain metastasis in patient 2.
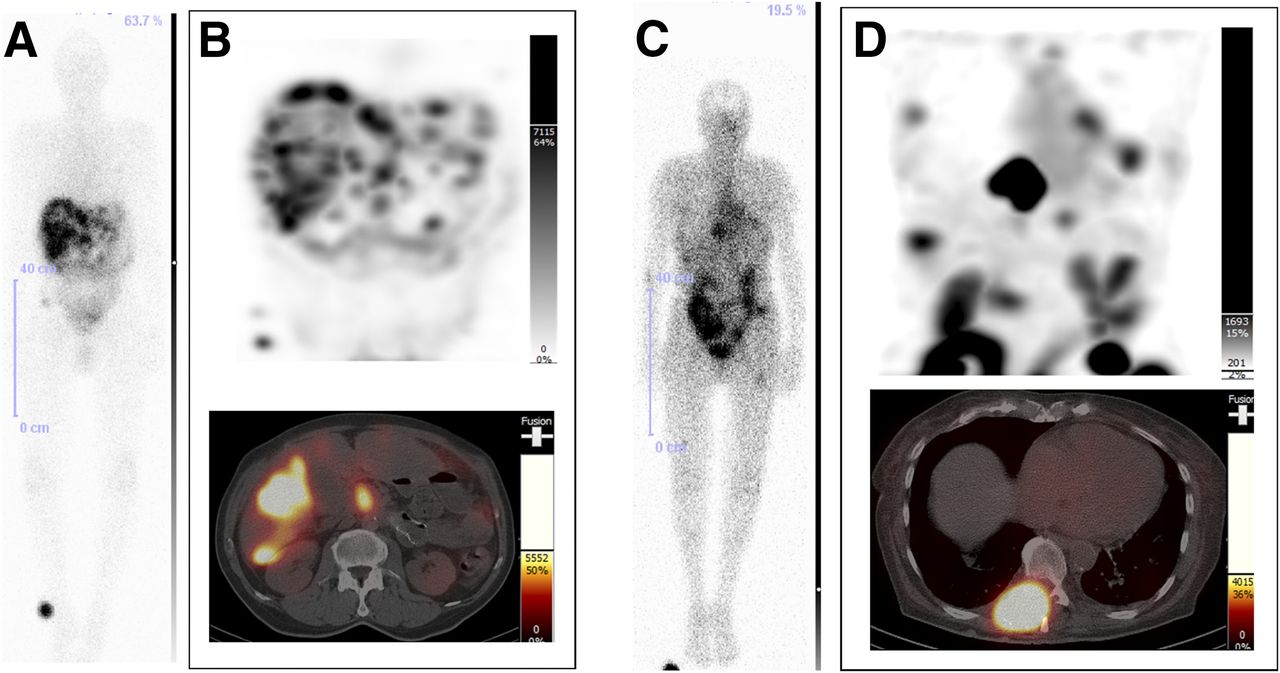
177Lu-3BP-227 planar and SPECT/CT scans of patient 1 (A and B) and patient 2 (C and D). (A) Planar scintigraphy 24 h after injection. (B) SPECT maximum-intensity projection 45 h after injection (top) and axial section, liver lesions and primary tumor, 45 h after injection (bottom). (C) Planar scintigraphy 48 h after injection. (D) SPECT maximum-intensity projection 44 h after injection (top) and axial section, large spinal lesion, 44 h after injection (bottom).
Absorbed Doses to Organs
Patient 3
Seven months after experiencing back pain, diarrhea, and weight loss, patient 3 was diagnosed with ductal adenocarcinoma of the pancreatic body. Hepatic, pulmonary, and lymph node metastases were present at the time of diagnosis, as well as infiltration of the visceral blood vessels and peritoneal carcinomatosis with massive ascites production. Additional medical conditions included severe cachexia due to malnutrition (hypoalbuminemia and hypoproteinemia), a nonfunctioning left kidney, and diabetes mellitus. After diagnosis, the patient received palliative chemotherapy with FOLFIRINOX (folinic acid/fluorouracil/irinotecan/oxaliplatin) and FOLFOX (folinic acid/fluorouracil/oxaliplatin) but presented with progressive disease after initiation of chemotherapy during the scheduled restaging. All conventional treatment options had thus been exhausted, and the prognosis was extremely poor.
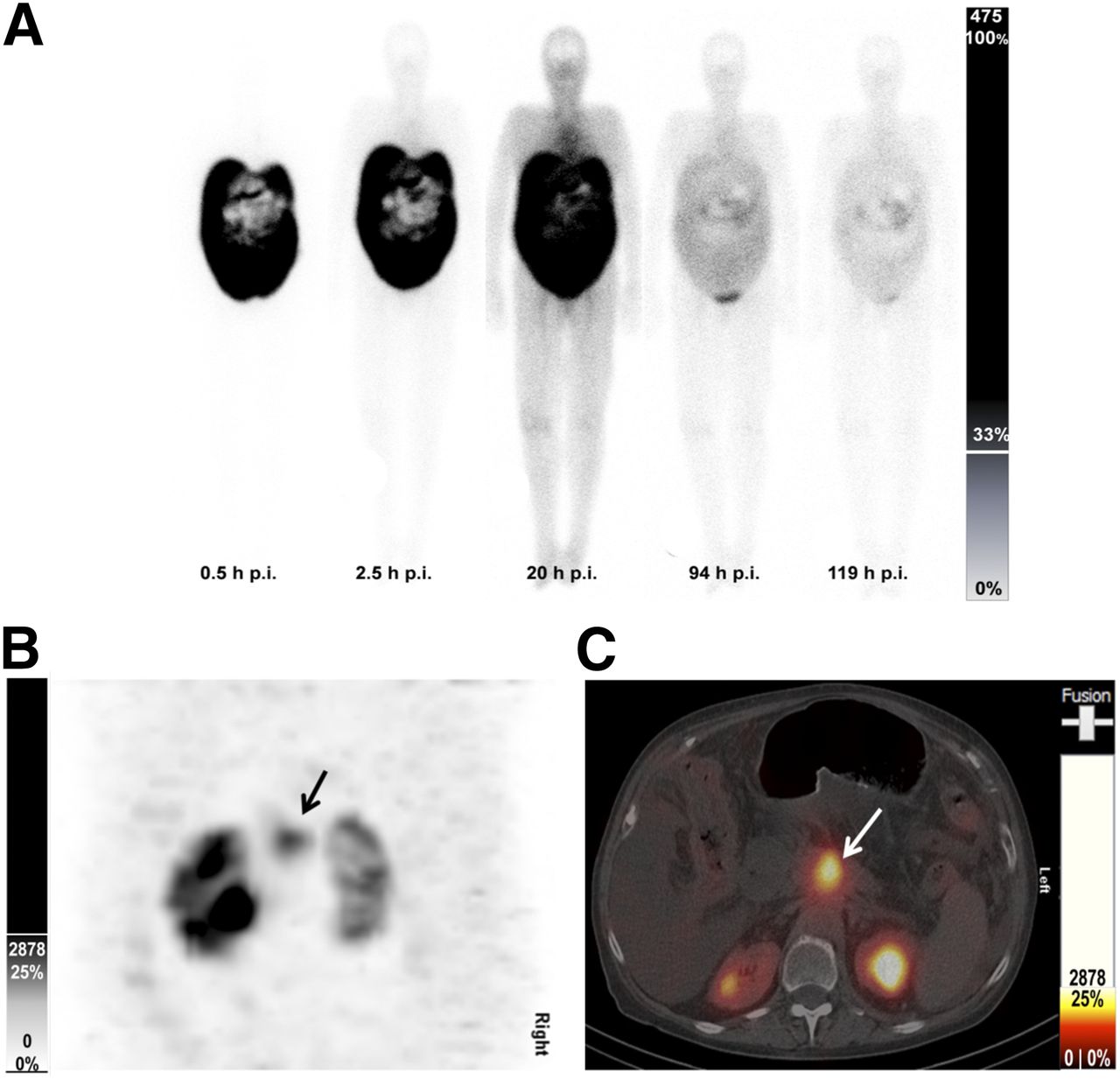
After an initial intravenous application of 1.5 GBq of 177Lu-3BP-227 to assess tumor uptake and organ dosimetry, the patient first received 2 further cycles (4 wk) of FOLFOX and then started a series of 3 intraperitoneal administrations (6.4, 7.5, and 5.5 GBq) at intervals of 8–10 wk (Supplemental Table 1). The application of 177Lu-3BP-227 was tolerated without any side effects (e.g., no nausea or vomiting) and without significant changes in pulse or blood pressure. SPECT/CT imaging 96 h after the application showed uptake in the primary tumor in the pancreas body and diffuse accumulation in the peritoneal carcinomatosis (Fig. 2). Dosimetry calculations identified the single functioning kidney as the dose-limiting organ (Table 2). The administered cumulative activity, 20.8 GBq, delivered a total dose of 22 Gy to the kidney. Serum creatinine levels and glomerular filtration rate remained normal during the treatment and follow-up (Supplemental Table 2).
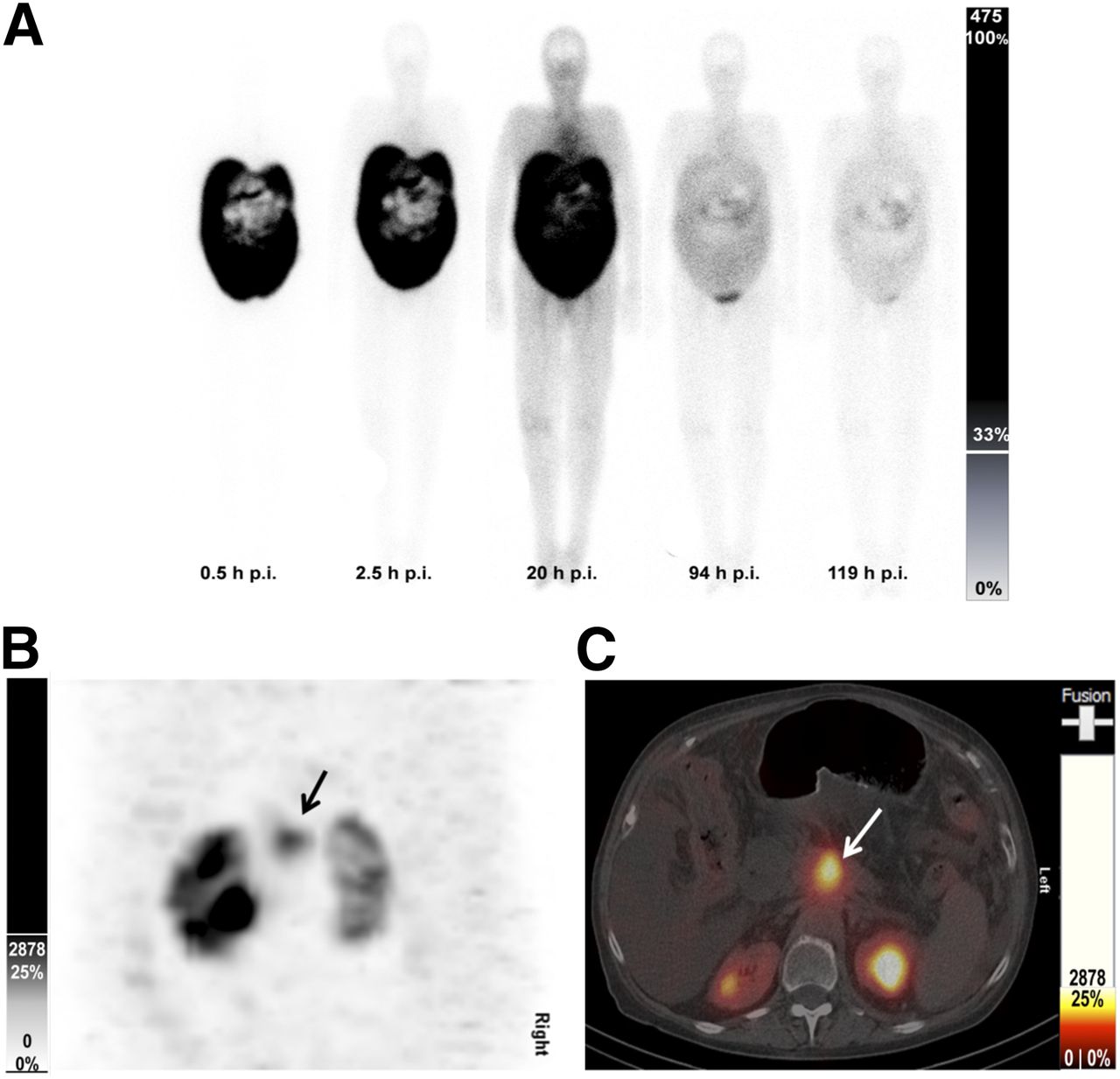
177Lu-3BP-227 planar and SPECT/CT scans of patient 3. (A) Series of whole-body images with corresponding count scale. (B) Maximum-intensity projection 96 h after administration. Arrow indicates primary tumor in pancreatic body. (C) Axial section, primary tumor, 96 h after injection.
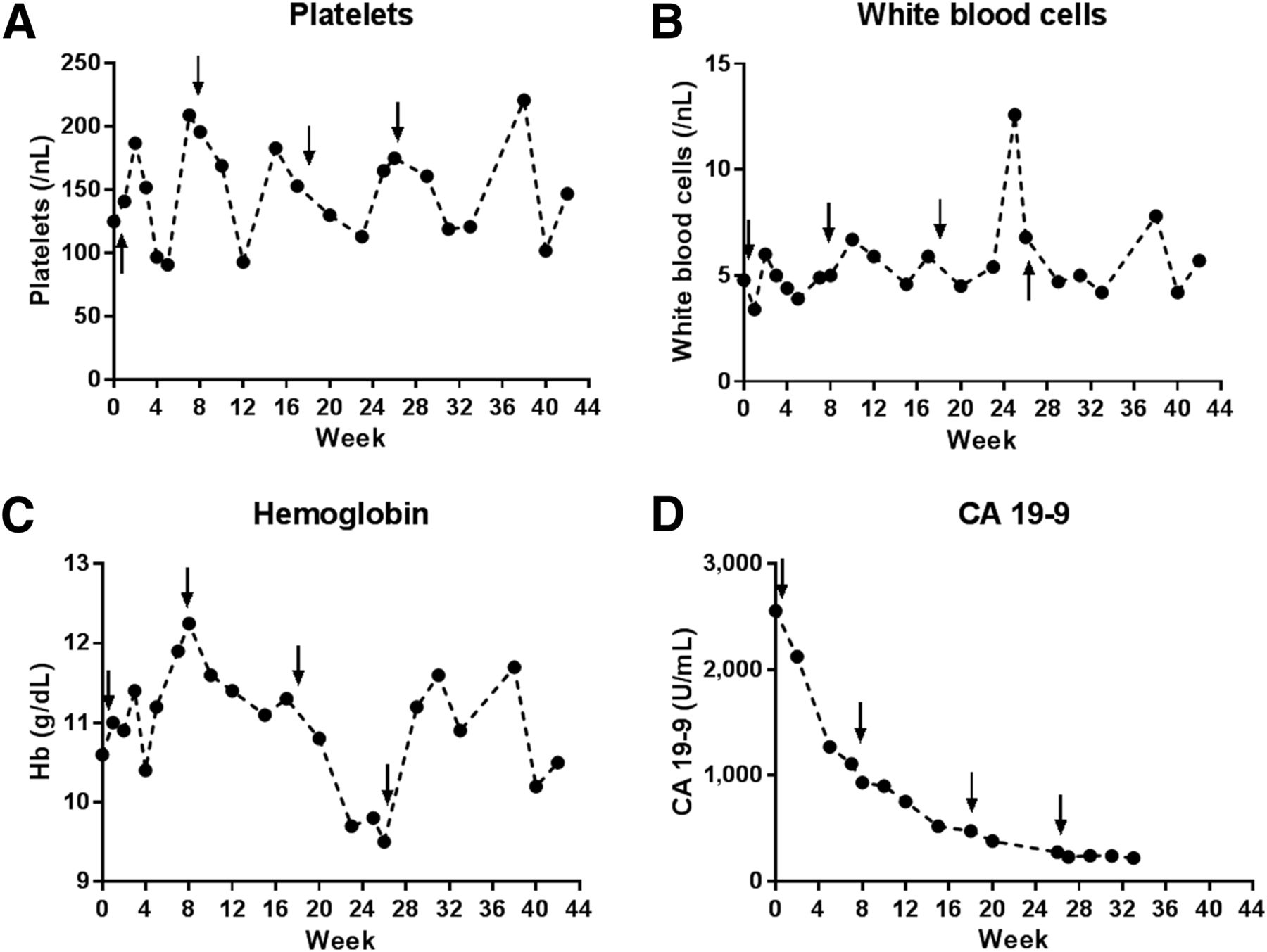
At baseline, the patient presented with a functional status of less than 70% according to the Karnofsky performance scale, grade 1 anemia (hemoglobin level, 6.6 mmol/L), grade 1 thrombocytopenia (platelets, 125 gigaparticles/L), and strongly increased serum carbohydrate antigen 19-9 (2,555 U/mL). During treatment, there was thrombocytopenia between grades 0 and 1, with recovery between administrations, and temporary grade 1 leukopenia (Figs. 3A–3C; Supplemental Table 1). There was a short and reversible episode of grade 2 anemia before the last treatment. Carbohydrate antigen 19-9 levels decreased during treatment from 2,555 to 220 U/mL and remained at this level during follow-up (Fig. 3D).
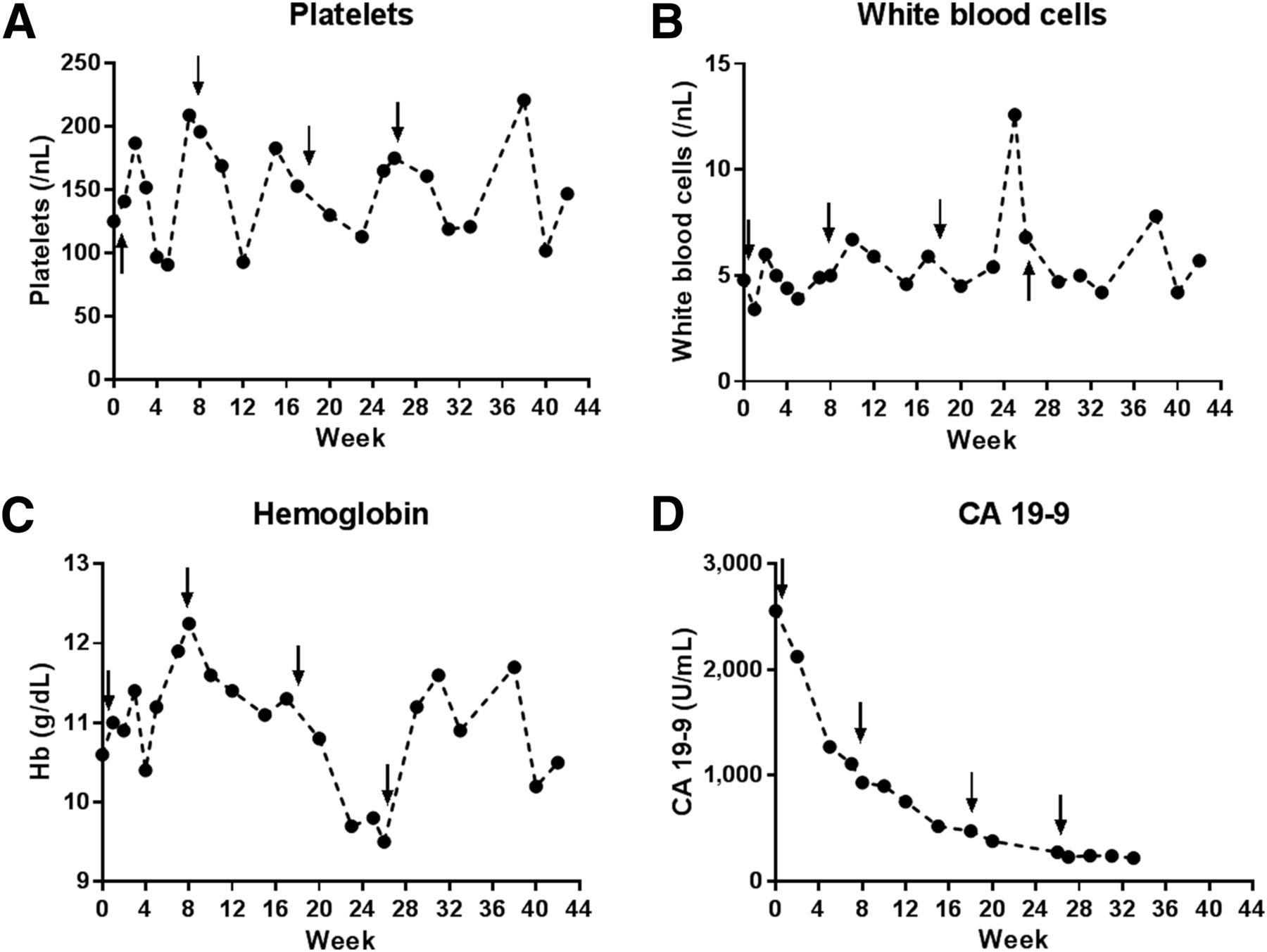
Laboratory parameters for patient 3 during 177Lu-3BP-227 treatment and follow-up. (A) Number of platelets. (B) Number of white blood cells. (C) Hemoglobin concentration. (D) Serum carbohydrate antigen (CA) 19-9 levels. Arrows indicate TRLT cycles.
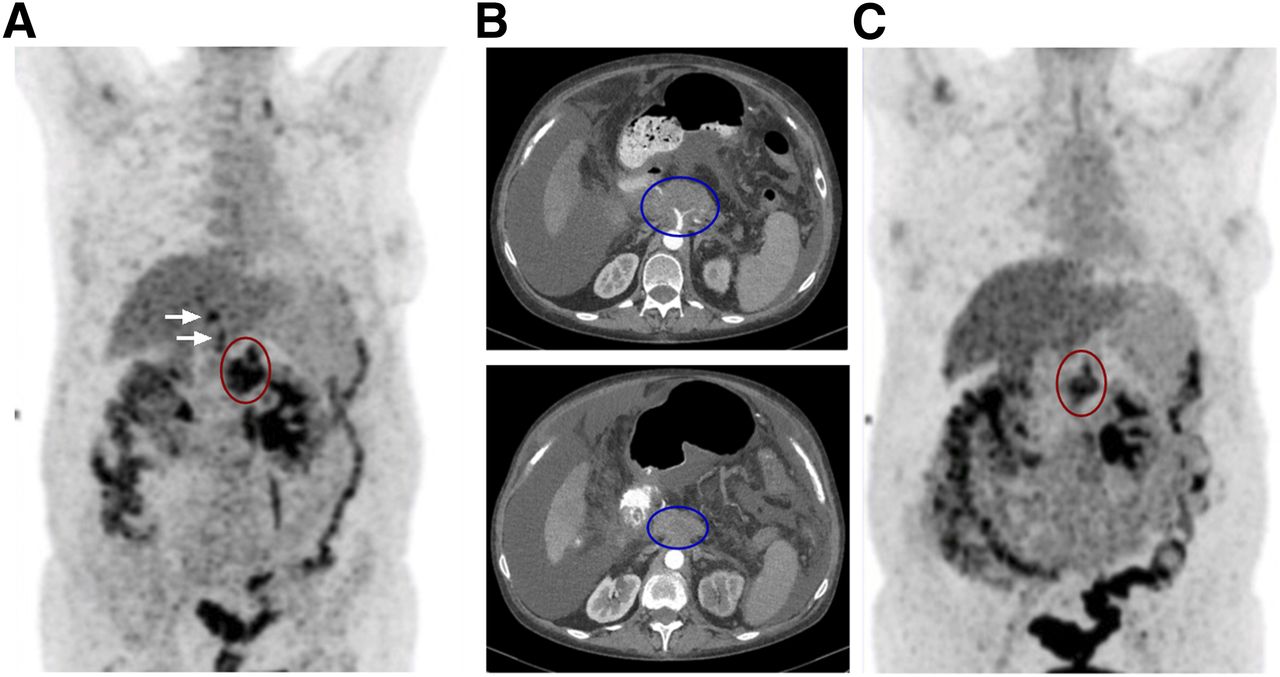
The size and metabolic activity of the pancreatic primary tumor decreased significantly during 177Lu-3BP-227 treatment as shown by 18F-FDG PET (Fig. 4). Metabolic activity decreased in the supra- and retroclavicular lymph nodes and in the pulmonary metastases, and liver metastases were no longer detectable. According to PERCIST and RECIST, the patient achieved a partial remission of the disease. Ascites production decreased, allowing drainage to be reduced from twice daily to twice weekly. The general status and quality of life of the patient improved considerably during treatment. The patient lived for 11 mo from the start of 177Lu-3BP-227 treatment (13 mo from diagnosis, when ascites was already present). The patient reported significant improvement in her quality of life during this period. However, death occurred after bacteremia and septic shock as a complication of central venous catheter placement.
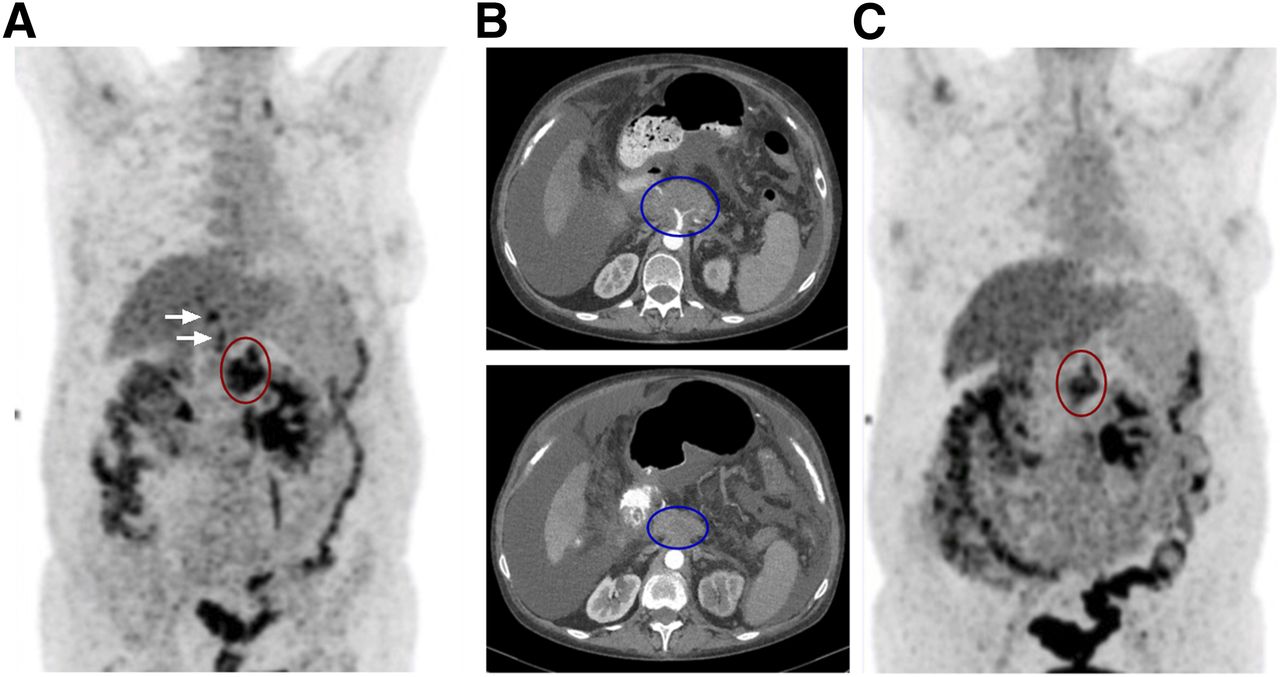
18F-FDG PET and CT scans of patient 3 before (A, B upper panel) and after (B lower panel, C) 177Lu-3BP-227 therapy. (A) 18FDG PET before 177Lu-3BP-227 therapy. Red oval: primary tumor; arrows: liver metastases. (B, upper panel) Axial CT section; primary tumor (blue oval) before 177Lu-3BP-227 therapy. (B, lower panel) Axial CT section; primary tumor (blue oval) after 3 cycles of 177Lu-3BP-227 therapy. (C) 18FDG PET after 3 cycles of 177Lu-3BP-227 therapy. Red oval: primary tumor.
Patients 4–6
In patient 4, no uptake was detected in the tumor lesions after the intravenous application of 1.5 GBq of 177Lu-3BP-227, and therefore, therapy was not indicated.
The pancreatic primary tumors of patients 5 and 6 had been surgically removed, and both patients had received several cycles of chemotherapy with gemcitabine and FOLFIRINOX. Nevertheless, both patients presented with progressive disease. Intravenous application of 1.5 GBq of 177Lu-3BP-227 showed substantial uptake in the tumor lesions, and patients 5 and 6 received TRLT with 5.5 and 5.1 GBq of 177Lu-3BP-227, respectively. Both patients tolerated the therapy without any side effects, and no adverse events occurred during the immediate follow-up. However, both patients died within weeks because of rapid disease progression.
Dosimetry and Adverse Events
Dosimetry identified the kidneys as the dose-limiting organ in all patients. The absorbed organ doses ranged from 0.7 to 1.4 mSv/MBq. The dose to bone marrow, liver, and gastrointestinal tract was consistently low (Table 2). Whole-body planar images of all patients are shown in Supplemental Figure 2, and detailed pharmacokinetic data of the patients who underwent dosimetry are shown in Supplemental Figure 3.
All patients presented with grade 1 anemia, and 2 patients (patients 3 and 4) also had grade 1 thrombocytopenia before commencing treatment with 177Lu-3BP-227. The administration of 177Lu-3BP-227 was tolerated without any acute side effects by all patients. The most severe adverse event that was considered to be potentially related to 177Lu-3BP-227 treatment was reversible grade 2 anemia (patient 3). A detailed account of adverse events and laboratory follow-up is presented in Supplemental Tables 1–3.
DISCUSSION
This retrospective report provides the first evidence for the feasibility of pancreatic adenocarcinoma treatment with the novel NTR1-targeted radiopharmaceutical 177Lu-3BP-227. Tumor uptake was demonstrated in 5 of the 6 patients reported here (∼75% of pancreatic adenocarcinoma tumors express NTR1 (3)). One patient with an extremely poor prognosis due to ascites formation achieved a partial remission of the disease and survived for 11 mo after treatment initiation.
The kidneys were identified as the dose-limiting organ. However, none of the reported patients received a dose to the kidney that exceeded 23 Gy; the highest renal dose (22 Gy) was received by the patient obtaining a partial response. Considering that most pancreatic adenocarcinoma patients have a life expectancy shorter than the time it takes for radiation-induced kidney toxicity to develop (∼12–18 mo), the dosimetric analysis of the patients in this report justifies prospective clinical trials to establish a safe and effective cumulative dose of 177Lu-3BP-227, as well as risk factors to be considered in pancreatic adenocarcinoma patients.
One end-stage patient with massive ascites and a prognosis (given by the treating oncologist) of only a few weeks survival had an impressive response to intraperitoneal 177Lu-3BP-227 TRLT, with significant improvement in quality of life, general physical status, and emotional well-being. This patient survived for 13 mo from the time of diagnosis, when ascites formation was already present, and for 11 mo after the start of 177Lu-3BP-227 TRLT. Compared with the median survival of just 2 mo for pancreatic adenocarcinoma patients with new-onset ascites (2), this result constitutes a major improvement in survival, particularly because of the absence of any significant adverse effects. Although there was a short overlap with palliative chemotherapy, this overlap pertained only to the initial dose of 177Lu-3BP-227, given to assess tumor uptake and dosimetry, and even in this setting, the administration of 177Lu-3BP-227 did not elicit any acute side effects. The good tolerability of 177Lu-3BP-227 TRLT was also demonstrated by the lack of any toxicity worse than reversible grade 2 anemia, which occurred in only one instance.
The major limitation of this study was the small and inhomogeneous patient population, which was due to the fact that, instead of being a systematic clinical trial, this was a retrospective analysis of patients undergoing TRLT with 177Lu-3BP-227 as the last line of treatment after exhaustion of all conventional options.
CONCLUSION
This report provided clinical evidence of the feasibility of treatment of ductal pancreatic adenocarcinoma with the 177Lu-labeled NTR1 antagonist 3BP-227. High uptake in metastatic tumor lesions and a promising toxicity profile warrant further investigation of 177Lu-3BP-227 TLRT in prospective clinical studies to systematically evaluate its safety and efficacy and to define the patient population it will most benefit.
DISCLOSURE
Christiane Smerling, Frank Osterkamp, and Ulrich Reineke are shareholders and employees of 3B Pharmaceuticals GmbH. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the nursing staff and the nuclear medicine technologists of the Theranostics Center for Molecular Radiotherapy and Molecular Imaging for managing the patients mentioned in this report and assisting with preparation of the manuscript.
Footnotes
↵* Contributed equally to this work.
Published online Oct. 12, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 24, 2017.
- Accepted for publication September 27, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Synthesis of 64Cu-, 55Co-, and 68Ga-Labeled Radiopharmaceuticals Targeting Neurotensin Receptor-1 for Theranostics: Adjusting In Vivo Distribution Using Multiamine Macrocycles
- Complexes of the neurotensin receptor 1 with small-molecule ligands reveal structural determinants of full, partial, and inverse agonism
- Theranostics: Leveraging Molecular Imaging and Therapy to Impact Patient Management and Secure the Future of Nuclear Medicine
- Future of Theranostics: An Outlook on Precision Oncology in Nuclear Medicine
- Fibroblast-Activating Protein: Targeting the Roots of the Tumor Microenvironment